

Abstract
Background
Oocyte cryopreservation is a technique with considerable potential in reproductive medicine, including fertility preservation, as a way of delaying childbearing and as part of oocyte donation programs. Although the technique was relatively ineffective at first more recently numerous modifications have led to higher success rates.
Objectives
To compare the effectiveness and safety of vitrification and slow freezing as oocyte cryopreservation techniques for fertility outcomes in women undergoing assisted reproduction.
Search methods
We searched electronic databases, trial registers and websites, including the Cochrane Menstrual Disorders and Subfertility Group Specialised Register of controlled trials, Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE and PsycINFO (date of search 3 March 2014).
Selection criteria
Two review authors independently selected randomised controlled trials (RCTs) comparing vitrification and slow freezing for oocyte preservation in women undergoing assisted reproduction.
Data collection and analysis
Two review authors independently extracted the data from eligible studies and assessed their risk of bias. Any disagreements were resolved by discussion or by a third review author. Data extracted included study characteristics and outcome data. The overall quality of the evidence was assessed using GRADE methods.
Main results
Two RCTs were included in the review (106 participants). Neither study reported live birth rate. Vitrification was associated with an increased clinical pregnancy rate compared to slow freezing (RR 3.86, 95% CI 1.63 to 9.11, P = 0.002, 2 RCTs, 106 women, I2 = 8%, moderate quality evidence). The effect of vitrification compared to slow freezing on ongoing pregnancy rates was only reported in one small study, with inconclusive findings (RR 6.07, 95% CI 0.86 to 43.04, P = 0.07, one RCT, 28 women, low quality evidence).
No data were reported on adverse effects, nor were any other outcomes reported in the included trials. The evidence was limited by imprecision. We assessed the included studies as at low to unclear risk of bias as the methods were not well described.
Authors' conclusions
Oocyte vitrification compared to slow freezing probably increases clinical pregnancy rates in women undergoing assisted reproduction. However, the total number of women and pregnancies were low and the imprecision is high which limits applicability. The effect on ongoing pregnancy is uncertain as data were sparse. No data were available on live births or adverse effects.
Keywords: Female, Humans, Pregnancy, Freezing, Oocytes, Pregnancy Rate, Vitrification, Cryopreservation, Cryopreservation/methods, Randomized Controlled Trials as Topic
Plain language summary
Vitrification in comparison to slow freezing for egg cryopreservation in women undergoing assisted reproduction
Review question. What is the effectiveness and safety of vitrification in comparison to slow freezing as a method of preserving oocytes (eggs) in subfertile women undergoing assisted reproduction?
Background. Oocyte cryopreservation is a technique with considerable potential in reproductive medicine, including to preserve fertility, as a way of delaying childbearing, and as part of oocyte donation programs. Although the technique was relatively ineffective at first more recently numerous modifications have led to higher success rates. Cochrane review authors evaluated the evidence on two methods of freezing oocytes, vitrification and slow freezing. The most important difference between the techniques is the speed of freezing the eggs. Vitrification is a faster process which may potentially cause less damage to the eggs.
Characteristics of the included studies. The search of the medical literature was done in March 2014. We found two randomised controlled trials (RCTs) with 106 participants comparing oocyte vitrification versus slow freezing. Neither study reported live births or adverse events as outcomes. One reported ongoing pregnancy and both reported clinical pregnancy.
Key results. The clinical pregnancy rate was higher in the oocyte vitrification group than in the slow freezing group. The effect of vitrification compared to slow freezing on ongoing pregnancy rates was only reported in the one small study, with inconclusive findings.
Quality of the evidence. The quality of the evidence was rated as moderate for clinical pregnancy and low for ongoing pregnancy. The evidence was limited by imprecision.
Summary of findings
Summary of findings for the main comparison. Vitrification versus slow freezing for women undergoing oocyte cryopreservation.
| Vitrification versus slow freezing for women undergoing oocyte cryopreservation | |||||
| Population: subfertile women undergoing oocyte cryopreservation Settings: assisted reproduction Intervention: vitrification versus slow freezing | |||||
| Outcomes | Illustrative comparative risks (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | |
| Assumed risk | Corresponding risk | ||||
| Slow freezing | Vitrification slow | ||||
| Live birth | No studies reported live birth | ||||
| Ongoing pregnancy rate Follow‐up: median 9 months | 77 per 1000 | 467 per 1000 (66 to 1000) | RR 6.07 (0.86 to 43.04) | 28 (1 study) | ⊕⊕⊝⊝ low1,2 |
| Clinical pregnancy rate Follow‐up: mean 9 months | 116 per 1000 | 449 per 1000 (190 to 1000) | RR 3.86 (1.63 to 9.11) | 106 (2 studies) | ⊕⊕⊕⊝ moderate1,3 |
| Adverse events | No studies reported adverse events | ||||
| *The basis for the assumed risk is the median control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | |||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | |||||
1 Surrogate of live birth rate: downgraded due to indirectness. 2 RR 6.07 (95% CI 0.86 to 43.04): downgraded due to serious imprecision.
3 Although CI is wide, its lowest limit is still clinically relevant. Therefore, it was not downgraded due to imprecision.
Background
Description of the condition
Since the pioneering days of in vitro fertilisation (IVF), cryopreservation of human embryos has been a fundamental aspect of assisted reproductive technology (ART) by preventing wastage of valuable material and improving cumulative pregnancy rates (Friedler 1988). The first successful embryo cryopreservation was reported by Trounson and Mohr in 1983 (Trounson 1983), but subsequent modifications of the technique have allowed for a greater success rate and the standardisation of this valuable technique, with a high rate of embryo survival and implantation after transfer (Kader 2009).
More recently, the cryopreservation of human oocytes has been sought by young women undergoing oncology treatment as a method of fertility preservation (Friedler 2012; Kim 2006; Revel 2010). As survival rates in oncology patients of reproductive age improve, the issue of fertility preservation is becoming more important (Matthews 2012). Oocyte cryopreservation can also be used in women who are philosophically uncomfortable with embryo freezing, as well as by women who are conscious of the decline in ovarian reserve with advancing maternal age but are not ready to attempt pregnancy (Fahy 2007; Stoop 2011; Tucker 2004). There are other clinical situations that may benefit from oocyte cryopreservation, including the use of donor oocyte banking, which has been shown to be as effective as the use of fresh donated oocytes (Cobo 2011a). It may also be useful in those rare cases where the freshly aspirated oocytes cannot be inseminated due to the inability of the male partner to generate a semen sample and not having readily available semen aspiration techniques as a possible therapeutic option (Lockwood 2011). There are promising results in women with a risk of ovarian hyperstimulation syndrome (OHSS) who do not want to freeze embryos, to postpone embryo transfer using oocyte cryopreservation and so improve the rates of success in that cycle (Herrero 2011).
In summary, oocyte cryopreservation definitely has a place in reproductive medicine with very clear indications but whether slow freezing and vitrification are comparable is an issue that remains to be determined (Gook 2011; Gosden 2011; Smith 2010).
Description of the intervention
Oocyte cryopreservation is a newly developed technique for fertility preservation (Noyes 2009). The first successful pregnancy using frozen oocytes was reported by Chen et al in 1986 (Chen 1986). Although the technique was relatively ineffective at first, numerous modifications have led to a very satisfactory pregnancy rate that in some cases is similar to the success rates reported using fresh oocytes. Some IVF programmes today are leaning towards using vitrification instead of slow freezing for the cryopreservation of human oocytes (Rudick 2010). Vitrification offers a simple, rapid and inexpensive method with acceptable survival rates after thawing by diminishing ice crystal formation and with it the risk of injury to these large cells (Saragusty 2011).
Borini et al pioneered the systematic use of slow freezing for oocyte cryopreservation. Despite multiple modifications and improvements (including the use of intracytoplasmic sperm injection (ICSI) for attempted fertilisation) the overall pregnancy rates were initially somewhat disappointing. Vitrification builds its foundation in reducing the cooling time and increasing the amount of cryoprotectants in order to reduce the transitional stage and therefore the potential cooling damage (Borini 2010).
Initially vitrification was performed using open devices with low volume, such as capillary glasses, cooper devices, pulled straws and loops. More recently, closed devices (tubing systems) allow a decreased volume to be vitrified enabling the cryoprotectant concentration to be reduced and minimising the toxic effect of direct contact with liquid nitrogen (Bonetti 2011; Cobo 2012b; Saragusty 2011; Smith 2011). Overall, vitrification is perceived as a step forwards in cryopreservation and is rapidly replacing slow freezing in most programmes due to better oocyte survival after thawing and the fact that it can be easily replicated. With this method ice crystal formation is prevented by a high concentration of cryoprotectants and very high cooling rates (Leibo 2011).
How the intervention might work
The principle of oocyte cryopreservation implies cells brought into suspended animation for indefinite periods of time. During the process certain situations such as osmotic shock, crystal formation and the adverse effect of solute concentration (solution effect) should be prevented.
Currently two techniques are available. Both use cryoprotectants to avoid cell damage. The cooling rates must be controlled to allow dehydration while avoiding intracellular freezing and should be fast enough to avoid the toxic effects of the cryoprotectants. The first technique used is slow freezing. It requires a low concentration of cryoprotectants. The temperature decrease is slow (2 °C/minute) until the seeding temperature of ‐6 °C is reached. The oocytes remain at this temperature for 10 to 30 minutes then the temperature is dropped to ‐32 °C at a slower cooling rate before storage in liquid nitrogen. The second technique is vitrification, which uses higher amounts of cryoprotectants (generally combinations of propanediol (PROH), dimethyl sulphoxide (DMSO) and ethylene glycol (EG)), resulting in extreme shrinkage. To avoid toxicity, the exposure time must be reduced and the freezing rates reach ‐1500 °C/minute until the temperature reaches ‐20,000 °C. The thawing process implies rehydration; it is called warming in the case of vitrification and involves serial transfer through sucrose solutions. Vitrification may have advantages over slow freezing in particular technical aspects such as the ultra‐quick transition from liquid to solid state, thus avoiding the crystal formation that is thought to cause damage to cell structures or osmotic shock (Sansinena 2011). Using vitrification, the oocyte survival and fertilisation rates could be expected to be higher as structural damage at the cellular level is avoided (Gook 2007; Mullen 2004). Besides, no evidence of alterations in the meiotic spindle or in chromosome structures have been described in vitrification procedures (Chen 2003; Cobo 2010; Martinez‐Burgos 2011). However, success rates are still highly operator dependent.
Why it is important to do this review
Oocyte cryopreservation is a technique that potentially has several indications in reproductive medicine. These include for fertility preservation in cancer patients; as a method to delay childbearing in cases where embryo cryopreservation is not an option due to ethical issues or in countries in which this practice is not legal; to improve egg donation programmes by reducing waiting time; in ART procedures when there is an inability to obtain a semen sample on the day of oocyte retrieval; or to prevent OHSS. Some programmes have also included cryopreservation as a strategy to accumulate oocytes in low‐responder ART patients (Cobo 2012a; Jain 2006).
This review was conducted to provide objective information on the available data comparing vitrification to slow freezing for oocyte cryopreservation. Oocyte freezing became a more popular intervention after vitrification was introduced (Rudick 2010). Until recently vitrification was considered experimental so it is important to find solid evidence about the effectiveness and safety of oocyte cryopreservation by vitrification (Albertini 2011; Cobo 2011a; Cobo 2011b; Gook 2007).
Objectives
To compare the effectiveness and safety of vitrification and slow freezing as oocyte cryopreservation techniques for fertility outcomes in women undergoing assisted reproduction.
Methods
Criteria for considering studies for this review
Types of studies
Only randomised controlled trials (RCTs) were eligible for inclusion. Studies with evidence of inadequate sequence generation (for example alternate days, patient identification odd numbers) were excluded. Studies that divided the oocyte cohort from each woman into two experimental groups were not included.
Types of participants
Women who wanted to freeze oocytes for any reason.
Types of interventions
Trials comparing oocyte vitrification versus slow freezing.
Types of outcome measures
Primary outcomes
1. Live birth per woman undergoing an embryo transfer derived from thawed oocytes, defined as delivery of a live fetus after at least 24 completed weeks of gestation
Secondary outcomes
Ongoing pregnancy, defined as any pregnancy beyond 12 weeks
Clinical pregnancy, defined as evidence of one or more gestational sacs
Fertilisation rate, defined as the number of normal fertilised eggs over the total number of frozen‐thawed oocytes that were inseminated or injected (we planned not to pool these data)
Oocyte survival rate, defined as the number of oocytes that survived after thawing over the total number of oocytes thawed (we planned not to pool these data)
Miscarriage rate, defined as the number of miscarriages over the number of clinical pregnancies
Multiple pregnancy rate, defined as a pregnancy with more than one gestational sac over the number of clinical pregnancies
Chromosomes anomalies rate, defined as the number of fetuses or neonates with chromosomal abnormalities over the number of fetuses or neonates assessed for chromosomal abnormalities
Major congenital malformations, defined as the number of fetuses over 12 weeks or neonates with major congenital malformations over the total number of fetuses over 12 weeks or neonates
Search methods for identification of studies
We searched for all published and unpublished RCTs on oocyte freezing, without language restriction and in consultation with the Menstrual Disorders and Subfertility Group (MDSG) Trials Search Co‐ordinator, from inception of the database to present (date of search 3 March 2014).
Electronic searches
We searched the following electronic databases, trial registers and websites: the MDSG Specialised Register of controlled trials (Appendix 1), MEDLINE (Appendix 2), the Cochrane Central Register of Controlled Trials (CENTRAL) (Appendix 3), EMBASE (Appendix 4), PsycINFO (Appendix 5) and clinicaltrials.gov (Appendix 6).
Other electronic sources of trials included:
trial registers for ongoing and registered trials, Current Controlled Trials (www.controlled‐trials.com), ClinicalTrials.gov (clinicaltrials.gov/) and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int);
citation indexes, Science Citation Index (scientific.thomson.com/products/sci/);
conference abstracts in the Web of Knowledge (wokinfo.com/);
LILACS database, for trials from the Portuguese and Spanish‐speaking world (bases.bireme.br);
PubMed (www.ncbi.nlm.nih.gov/pubmed/);
OpenSIGLE database (opensigle.inist.fr/) and Google for grey literature.
Searching other resources
We handsearched reference lists of articles retrieved by the search and contacted experts in the field to obtain additional data. We also handsearched relevant journals and conference abstracts that are not covered in the MDSG Specialised Register, in liaison with the Trials Search Co‐ordinator.
Data collection and analysis
Selection of studies
Two review authors (DG and BR) independently reviewed studies for possible inclusion using Early Review Organizing Software (EROS) (Ciapponi 2011a; Ciapponi 2011b; Glujovsky 2010). After an initial screening of the titles and abstracts retrieved by the search, conducted by DG and BR, the full texts of all potentially eligible studies were retrieved. Two review authors (DG and BR) independently examined these full‐text articles for compliance with the inclusion criteria and selected the studies that were eligible for inclusion in the review. We planned to correspond with study investigators, as required, to clarify study eligibility. Disagreements as to study eligibility were resolved by discussion or by a third review author. The selection process was documented with a PRISMA flow chart.
Data extraction and management
Two review authors (DG and BR) independently extracted the data from eligible studies using a data extraction form designed and pilot‐tested by the authors. Any disagreement was resolved by discussion or by a third review author. The data extracted included study characteristics and outcome data. Where studies had multiple publications, the main trial report was used as the reference and additional details were derived from the secondary papers. We planned to correspond with study investigators for further data, as required.
Assessment of risk of bias in included studies
Two review authors (DG and BR) independently assessed the included studies for risk of bias using the Cochrane 'risk of bias' assessment tool (www.cochrane‐handbook.org). This tool assessed: allocation (random sequence generation and allocation concealment); blinding of participants and personnel, blinding of outcome assessors; incomplete outcome data; selective reporting; and other bias. Disagreements were resolved by discussion or by a third review author. We described all judgements fully and have presented the conclusions in the 'Risk of bias' table. The risks of bias were incorporated into the interpretation of the review findings by means of sensitivity analyses (see below).
We took care to search for within‐trial selective reporting, such as trials failing to report obvious outcomes or reporting them in insufficient detail to allow inclusion. We sought published protocols to compare the outcomes between the protocol and the final published study.
Where the identified studies failed to report the primary outcome of live birth but did report intermediate outcomes such as clinical pregnancy, we planned to undertake informal assessment as to whether the interim values (for example pregnancy rates) were similar to those reported in studies that also reported live birth.
Measures of treatment effect
For dichotomous data (for example live birth rates), we used the numbers of events in the control and intervention groups of each study to calculate and report risk ratios (RRs) and we also presented the Peto odds ratio (OR). We reversed the direction of effect of individual studies, if required, to ensure consistency across trials. We presented 95% confidence intervals (CIs) for all outcomes. Where data to calculate RRs were not available, we planned to utilise the most detailed numerical data available that might facilitate similar analyses of the included studies (for example test statistics, P values). We compared the magnitude and direction of effect reported by the studies with the way they are presented in the review, taking account of legitimate differences.
Numbers needed to treat to benefit (NNTB) were calculated as the inverse of the risk difference.
Unit of analysis issues
The primary analysis was per woman randomised. We planned to summarise in an additional table, and to not meta‐analyse, data that did not allow valid analysis (for example 'per cycle' data). Multiple live births (for example twins or triplets) were counted as one live birth event.
Dealing with missing data
Data were analysed on an intention‐to‐treat basis as far as possible and attempts were made to obtain missing data from the original trials. Where these were unobtainable, we planned to undertake imputation of individual values for the primary outcome only. Live births were assumed not to have occurred in participants without a reported outcome. For other outcomes, only the available data were analysed. Any imputation was planned to be subjected to a sensitivity analysis (see below).
Assessment of heterogeneity
We considered whether the clinical and methodological characteristics of the included studies were sufficiently similar for meta‐analysis to provide a clinically meaningful summary. We assessed statistical heterogeneity by the measure of the I2 statistic. An I2 value greater than 50% was taken to indicate substantial heterogeneity (Higgins 2003; Higgins 2011). If we detected substantial heterogeneity, we planned to explore possible explanations in sensitivity analyses (see below). We took any statistical heterogeneity into account when interpreting the results, especially if there was any variation in the direction of effect.
Assessment of reporting biases
In view of the difficulty of detecting and correcting for publication bias and other reporting biases, we aimed to minimise their potential impact by ensuring a comprehensive search for eligible studies and by being alert for duplication of data. If there were 10 or more studies in an analysis, we planned to use a funnel plot to explore the possibility of small study effects (a tendency for estimates of the intervention effect to be more beneficial in smaller studies).
Data synthesis
If the studies were judged to be sufficiently similar, we combined the data using fixed‐effect models in the comparisons between vitrification and slow freezing.
An increase in the odds of a particular outcome, which might be beneficial (for example live birth) or detrimental (for example adverse effects), was displayed graphically in the meta‐analyses to the right of the centre‐line and a decrease in the odds of an outcome to the left of the centre‐line.
Subgroup analysis and investigation of heterogeneity
Where data were available, we planned to conduct subgroup analyses to determine the separate evidence within the following subgroups:
studies where the average age for women was below 37 years and studies where the average age for women was 37 years and over;
studies where vitrification was performed in open devices and studies where vitrification was performed in closed devices;
studies where oocyte cryopreservation was performed with egg donors, studies where oocyte cryopreservation was performed for infertile non‐egg donors, and studies where oocyte cryopreservation was performed in women who sought to preserve their fertility.
Sensitivity analysis
We planned to conduct sensitivity analyses for the primary outcomes to determine whether the conclusions were robust to arbitrary decisions made regarding the eligibility and analysis of studies. These planned analyses included consideration of whether the review conclusions would have differed if:
eligibility was restricted to studies without high risk of bias;
alternative imputation strategies had been adopted;
a random‐effects model had been adopted.
Overall quality of the body of evidence
The overall quality of the body of evidence was assessed using GRADE criteria (study limitations, consistency of effect, imprecision, indirectness and publication bias). The judgements made were documented and justified. In future updates, the following outcomes should be included in the summary of findings table: live birth rate, ongoing pregnancy rate, clinical pregnancy rate, miscarriage rate and adverse effects.
Results
Description of studies
Results of the search
The search retrieved 197 articles and 35 were initially eliminated due to duplication. Twelve studies were potentially eligible and were retrieved as full‐text articles. Two studies (four articles) met our inclusion criteria. Eight studies were excluded. See the study tables Characteristics of included studies, Characteristics of excluded studies, Characteristics of studies awaiting classification and the flow chart (Figure 1).
1.
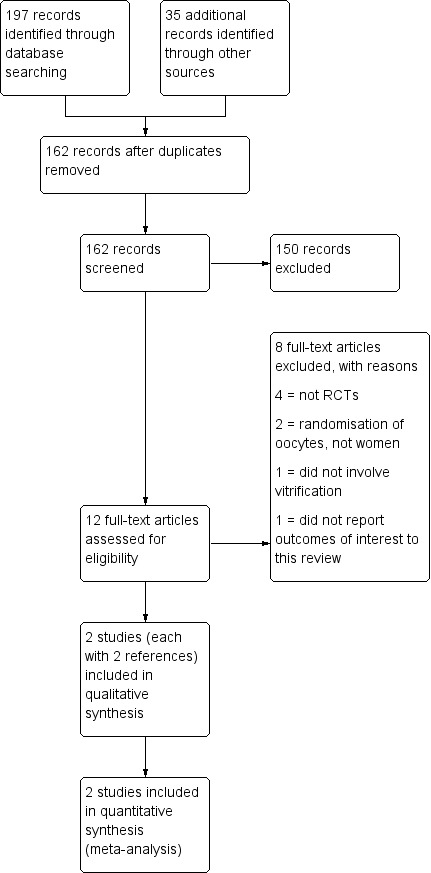
Study flow diagram.
Included studies
Study design and setting
Two parallel‐design randomised controlled trials (RCTs) were included in the review. Both were single‐centre studies, conducted in the USA and Brazil, respectively.
Participants
The studies included 63 women in the intervention groups and 43 in the control groups. All were women with infertility. In one study (Smith 2010) women participated if they had supernumerary mature oocytes (more than nine mature oocytes recovered after cumulus cell removal from the controlled ovarian stimulation IVF or ICSI cycle) and in the other study (Schiewe 2010) oocytes came from donors and the recipients were randomised to each of the interventions. Although the published abstract did not mention the number of participants, in a personal communication the author told us that there were 15 in the vitrification group and 13 in the slow freezing group.
Interventions
One out of two studies compared vitrification versus slow freezing
One out of two studies compared vitrification versus choline‐enriched CJ3 slow freezing
Outcomes
Neither of two studies reported live births
One of two studies reported ongoing pregnancy
Two of two studies reported clinical pregnancies
Neither of two studies reported miscarriage rate
Neither of two studies reported chromosomal abnormalities
Neither of two studies reported congenital malformations
Excluded studies
Eight studies were excluded from the review for the following reasons:
four of eight studies were not RCTs;
two of eight studies randomised oocytes (instead of women);
one of eight studies reported no comparisons of interest;
one of eight studies reported no outcomes of interest.
Studies awaiting classification
Two studies were found in the Clinicaltrials.gov database. One study (Greenblatt 2014) has been terminated and the other (Hershlag 2012) was completed but the results have not yet been published.
Risk of bias in included studies
None of the included studies had high risk of bias for any of the evaluated items. For blinding of participants and personnel, the risk of bias was unclear in both included studies. The rest of the risk of bias items were classified as low or unclear. See Characteristics of included studies, Figure 2 and Figure 3.
2.
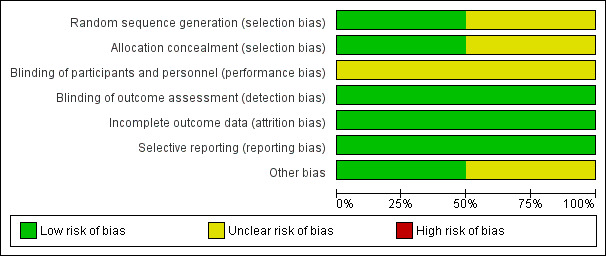
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
One study was at low risk of selection bias related to sequence generation, as they used computer randomisation. The other study did not describe the method used and was at unclear risk of this bias.
One study was at low risk of selection bias related to allocation concealment, as they sealed envelopes. The other study did not describe the method used and was at unclear risk of this bias.
Blinding
Blinding of participants and personnel (performance bias)
In one study, participants were blinded but personnel were not and the risk of bias was considered high. The other study did not describe whether blinding was used and was assessed to be at unclear risk of this bias.
Blinding of outcome assessment (detection bias)
Blinding of outcome assessment was not reported but the review authors judged that the outcome measurement was not likely to be influenced by lack of blinding.
Incomplete outcome data
All randomised women were adequately accounted for (due to the study design most were not included in the analysis (see Characteristics of included studies).
Selective reporting
In both studies, the protocols were not available but it was clear that the published reports included all expected outcomes and we considered the studies to be at low risk of bias.
Other potential sources of bias
In one study we found no potential sources of within‐study bias. In Smith 2010, only some of the randomised participants finally underwent the treatment and were included in the analysis, which could possibly create a bias in the selection of participants. This study was deemed as at unclear risk of other bias.
Effects of interventions
See: Table 1
Primary outcomes
1. Live birth
Neither of the two studies analysed this outcome.
Secondary outcomes
2. Ongoing pregnancy
The effect of vitrification compared to slow freezing on ongoing pregnancy rate was uncertain (RR 6.07, 95% CI 0.86 to 43.04, P = NS, 1 RCT, 28 women, I2 = not applicable, low quality evidence) (Analysis 1.1). The Peto OR was 6.31 (95% CI 1.26 to 31.69).
1.1. Analysis.

Comparison 1 Vitrification versus slow freezing, Outcome 1 Ongoing pregnancy rate.
3. Clinical pregnancy
Vitrification was associated with an increased pregnancy rate compared to slow freezing (RR 3.86, 95% CI 1.63 to 9.11, P = 0.002, 2 RCTs, 106 women, I2 = 8%, moderate quality evidence) (Analysis 1.2). The Peto OR was 4.74 (95% 2.05 to 10.92).
1.2. Analysis.
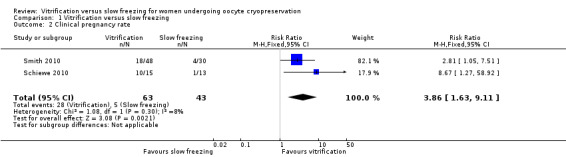
Comparison 1 Vitrification versus slow freezing, Outcome 2 Clinical pregnancy rate.
Both included studies reported increased oocyte survival rate (range 80% to 90% versus 45% to 67% in both studies) and fertilisation rate (range 76% to 83% versus 54% to 68% in both studies) in the vitrification groups (Table 2 and Table 3).
1. Survival rate.
| Study | Vitrification | Slow freezing |
| Smith 2010 | 281/349 (80.5%) | 159/238 (66.8%) |
| Schiewe 2010 | 141/158 (89.2%) | 59/129 (45.7%) |
2. Fertilisation rate.
| Study | Vitrification | Slow freezing |
| Smith 2010 | 200/260 (76.9%) | 104/155 (67.1%) |
| Schiewe 2010 | 117/141 (83%) | 32/59 (54.2%) |
Sensitivity, subgroup and any other planned analyses were not possible because only two studies were included.
Discussion
Summary of main results
Only two RCTs comparing oocyte vitrification versus slow freezing, where the primary outcomes were at least clinical pregnancy rates, were found. Oocyte vitrification compared to slow freezing increased the clinical pregnancy rate (RR 3.86, 95% CI 1.63 to 9.11). The effect of vitrification compared to slow freezing on ongoing pregnancy rates was only reported in one small study, with inconclusive findings (RR 6.07, 95% CI 0.86 to 43.04) (Table 1).
No study reporting live birth rates was found. Both survival rate and fertilisation rate (which were analysed in the additional tables) were higher in vitrified oocytes (Table 2; Table 3).
Overall completeness and applicability of evidence
The numbers of studies and participants were low and neither of the studies reported live births. Nevertheless, in the worst scenario determined by the confidence interval the intervention shows important improvements in terms of number needed to treat to benefit (NNTB): clinical pregnancy rate of 3 (95% CI 2 to 6) and probable increases in ongoing pregnancy rate of 3 (95% CI 1 to 10). As vitrification is operator‐dependent the learning curve should be considered and its effectiveness depends on the embryo laboratory experience with the technique. Lastly, there are several different kits for vitrification that should be evaluated to see if all have the same effectiveness. None of these issues have been addressed in the two included studies.
Quality of the evidence
The quality of the evidence was moderate for clinical pregnancy rate according to the GRADE rating and low for ongoing pregnancy rate (Table 1). Nevertheless, the number of studies and of participants in each study was low and we should be cautious. The main limitation of the evidence was imprecision. However, our findings were consistent. We assessed the included studies as at low to unclear risk of bias. The methods were not well described (Figure 2 and Figure 3).
Potential biases in the review process
We are not aware of any potential biases in the review process. Our search strategy was very comprehensive with no relevant limitations. We decided to exclude studies that randomised oocytes instead of randomising women because our primary outcome was live birth rate, which could not be assessed if oocytes were randomised. We did not exclude any study on the basis of reported outcomes.
Agreements and disagreements with other studies or reviews
Our systematic review has included two RCTs. We included one more study (Schiewe 2010) than the systematic review published by Cobo 2011b, which included only the trial published by Smith 2010. Although the comparator used in the study of Schiewe 2010 was not exactly the same as the one used in Smith 2010, both studies used slow freezing and showed similar outcomes and results. The main weakness of our systematic review is the small number of included studies and the absence of data about live birth rates. Nevertheless, it is likely that no new studies will be published in the future given that the currently published trials show favourable results, the proxy outcomes found in many other studies show benefits (Cao 2009; Cobo 2008; Cobo 2010; Cobo 2011b; Martinez‐Burgos 2011; Rienzi 2010; Zhang 2011), and that many of the worldwide IVF programmes have already included oocyte vitrification as a routine technique, as has been proposed by the American Society for Reproductive Medicine (ASRM 2013).
Oocyte vitrification is a technique that has been evaluated in several studies (Cao 2009; Cobo 2008; Cobo 2010; Cobo 2011b; Martinez‐Burgos 2011; Rienzi 2010; Zhang 2011) and which have shown that the survival rate was higher after thawing vitrified oocytes than on thawing oocytes that had been slow frozen. The fertilisation rate and embryo quality were analysed by the same investigators (Cao 2009; Cobo 2008; Cobo 2010; Cobo 2011b; Martinez‐Burgos 2011; Rienzi 2010; Zhang 2011) who compared a sibling cohort of oocytes coming from the same woman and found that both the fertilisation rate and embryo quality were better in the vitrification group. These results could partly explain the conclusions from this systematic review. Unfortunately, no studies evaluating adverse effects such as chromosomal abnormalities or congenital malformation were found.
In this review we did not evaluate studies that compared vitrified oocytes and fresh oocytes. Some authors have published information showing good results, encouraging doctors and patients to consider this technique as a good option when fresh oocytes are not available (Cobo 2010; Dominguez 2013; Paffoni 2008; Siano 2013; Sole 2013). That comparison is important to better understand the real scope that vitrification could achieve.
Authors' conclusions
Implications for practice.
No studies reporting live birth rates were found. The included studies reported that women whose oocytes were vitrified had higher clinical pregnancy rates than those whose oocytes underwent slow freezing. However, data were scanty and there is currently insufficient evidence to obtain definitive conclusions.
Implications for research.
Intermediate outcomes such as oocyte survival rate, fertilisation rate and embryo quality were shown to be higher with vitrification than with slow freezing, both in the two included studies and also in several excluded studies. However, more randomised controlled trials reporting live births, adverse effects and neonatal outcomes would be welcome to support the routine use of oocyte vitrification.
History
Protocol first published: Issue 8, 2012 Review first published: Issue 9, 2014
| Date | Event | Description |
|---|---|---|
| 14 April 2008 | Amended | converted to new review format |
| 8 June 2007 | New citation required and major changes | Substantive amendment |
Notes
Acknowledgements
Marian Showell, Trials Search Co‐ordinator of the Menstrual Disorders and Subfertility Group, who contributed to the search strategies.
Appendices
Appendix 1. MDSG Specialised Register search strategy
Keywords CONTAINS "slow cooling" or "slow freezing" or "slow rate freezing" or "slow cooling" or "slow freezing" or "slow rate freezing" or "cryopreservation" or "cryoprotectant" or "cryopreservation techniques‐oocytes" or "vitrification" or "rapid cooling" or "rapid freezing" or "rapid protocol" or "ultra‐rapid freezing" or "fast cooling" or "freezing method" or Title CONTAINS "slow cooling" or "slow freezing" or "slow rate freezing" or "slow cooling" or "slow freezing" or "slow rate freezing" or "cryopreservation" or "cryoprotectant" or "cryopreservation techniques‐oocytes" or "vitrification" or "rapid cooling" or "rapid freezing" or "rapid protocol" or "ultra‐rapid freezing" or "fast cooling" or "freezing method"
AND
Keywords CONTAINS "oocyte" or "oocyte chilling" or "oocyte cryo‐banking" or "oocyte cryopreservation" or "oocyte freezing" or "oocyte storage" or "oocyte vitrification" or "*Oocytes" or Title CONTAINS "oocyte" or "oocyte chilling" or "oocyte cryo‐banking" or "oocyte cryopreservation" or "oocyte freezing" or "oocyte storage" or "oocyte vitrification" or "*Oocytes"
Appendix 2. MEDLINE (Ovid) search strategy
Search run on 2 March 2011, and updated on 22 August 2011, 23 October 2012 and 3 March 2014.
1 exp cryopreservation/ or exp tissue preservation/ (52192) 2 (Cryopreserv$ adj2 oocyte$).tw. (543) 3 (Cryopreserv$ adj2 ov$).tw. (571) 4 (stor$ adj2 oocyte$).tw. (142) 5 (frozen adj2 oocyte$).tw. (224) 6 (freez$ adj2 oocyte$).tw. (126) 7 (cryofixation or cryonic suspension).tw. (326) 8 exp Freezing/ (18483) 9 or/1‐8 (66308) 10 slow‐freez$.tw. (476) 11 (slow$ adj2 freez$).tw. (579) 12 (slow$ adj2 cool$).tw. (875) 13 equilibrium freez$.tw. (47) 14 (slow$ adj2 froz$).tw. (169) 15 or/10‐14 (1551) 16 exp vitrification/ (28) 17 vitrifi$.tw. (2012) 18 (rapid adj2 freez$).tw. (1104) 19 (rapid adj2 cool$).tw. (874) 20 or/16‐19 (3852) 21 9 and 15 and 20 (381) 22 randomized controlled trial.pt. (300240) 23 controlled clinical trial.pt. (81772) 24 randomized.ab. (216510) 25 placebo.tw. (129349) 26 clinical trials as topic.sh. (152299) 27 randomly.ab. (159876) 28 trial.ti. (92676) 29 (crossover or cross‐over or cross over).tw. (49527) 30 or/22‐29 (734564) 31 exp animals/ not humans.sh. (3536040) 32 30 not 31 (678874) 33 21 and 32 (23)
Appendix 3. CENTRAL search strategy
1 exp cryopreservation/ or exp tissue preservation/ (618) 2 (Cryopreserv$ adj2 oocyte$).tw. (21) 3 (Cryopreserv$ adj2 ov$).tw. (3) 4 (stor$ adj2 oocyte$).tw. (5) 5 (frozen adj2 oocyte$).tw. (5) 6 (freez$ adj2 oocyte$).tw. (5) 7 (cryofixation or cryonic suspension).tw. (0) 8 exp Freezing/ (75) 9 or/1‐8 (691) 10 slow‐freez$.tw. (18) 11 (slow$ adj2 freez$).tw. (20) 12 (slow$ adj2 cool$).tw. (12) 13 equilibrium freez$.tw. (0) 14 (slow$ adj2 froz$).tw. (3) 15 or/10‐14 (34) 16 exp vitrification/ (2) 17 vitrifi$.tw. (55) 18 (rapid adj2 freez$).tw. (4) 19 (rapid adj2 cool$).tw. (22) 20 or/16‐19 (79) 21 9 and 15 and 20 (8)
Appendix 4. EMBASE search strategy
1 exp cryopreservation/ or exp low temperature procedures/ or exp "preservation and storage"/ (157730) 2 (Cryopreserv$ adj2 oocyte$).tw. (1262) 3 (Cryopreserv$ adj2 ov$).tw. (1175) 4 (stor$ adj2 oocyte$).tw. (203) 5 (frozen adj2 oocyte$).tw. (354) 6 (freez$ adj2 oocyte$).tw. (274) 7 (cryofixation or cryonic suspension).tw. (369) 8 exp FREEZING/ (24507) 9 exp oocyte/ (61617) 10 or/1‐9 (215670) 11 slow‐freez$.tw. (912) 12 (slow$ adj2 freez$).tw. (1058) 13 (slow$ adj2 cool$).tw. (1035) 14 equilibrium freez$.tw. (51) 15 (slow$ adj2 froz$).tw. (254) 16 or/11‐15 (2185) 17 exp vitrification/ (2561) 18 vitrifi$.tw. (4090) 19 (rapid adj2 freez$).tw. (1246) 20 (rapid adj2 cool$).tw. (1049) 21 or/17‐20 (6436) 22 10 and 16 and 21 (806) 23 Clinical Trial/ (893833) 24 Randomized Controlled Trial/ (368808) 25 exp randomization/ (65021) 26 Single Blind Procedure/ (19116) 27 Double Blind Procedure/ (120876) 28 Crossover Procedure/ (40108) 29 Placebo/ (236677) 30 Randomi?ed controlled trial$.tw. (101620) 31 Rct.tw. (13868) 32 random allocation.tw. (1346) 33 randomly allocated.tw. (20579) 34 allocated randomly.tw. (1963) 35 (allocated adj2 random).tw. (745) 36 Single blind$.tw. (14514) 37 Double blind$.tw. (145091) 38 ((treble or triple) adj blind$).tw. (362) 39 placebo$.tw. (203019) 40 prospective study/ (266200) 41 or/23‐40 (1422423) 42 case study/ (24405) 43 case report.tw. (263308) 44 abstract report/ or letter/ (907127) 45 or/42‐44 (1189158) 46 41 not 45 (1384398) 47 22 and 46 (68)
48 (2012$ or 2013$ or 2014$).em. (3172160) 49 (2012$ or 2013$ or 2014$).dp. (421881) 50 48 or 49 (3173054) 51 47 and 50 (14)
Appendix 5. PsycINFO search strategy
1 exp Reproductive Technology/ (1173) 2 oocyt$.tw. (489) 3 (ovum or ova$).tw. (6446) 4 or/1‐3 (7986) 5 slow‐freez$.tw. (0) 6 (slow$ adj2 freez$).tw. (3) 7 (slow$ adj2 cool$).tw. (18) 8 equilibrium freez$.tw. (0) 9 (slow$ adj2 froz$).tw. (0) 10 vitrifi$.tw. (4) 11 (rapid adj2 freez$).tw. (1) 12 (rapid adj2 cool$).tw. (17) 13 or/5‐12 (43) 14 4 and 13 (1)
Appendix 6. Clinicaltrials.gov
Keywords CONTAINS "slow freezing"
AND
Keywords CONTAINS "vitrification"
Data and analyses
Comparison 1. Vitrification versus slow freezing.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Ongoing pregnancy rate | 1 | 28 | Risk Ratio (M‐H, Fixed, 95% CI) | 6.07 [0.86, 43.04] |
| 2 Clinical pregnancy rate | 2 | 106 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.86 [1.63, 9.11] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Schiewe 2010.
| Methods | Not stated | |
| Participants | 28 recipients receiving oocytes from 15 consenting unproven egg donors (21‐27 y.o.) exposed to a standard COH protocol. 15 recipients received 158 vitrified eggs and 13 recipients received 129 eggs that had slow freezing | |
| Interventions | Oocytes were recovered, stripped and cryopreserved (3‐5 oocytes/container) within 37.5‐38 hr post‐hCG. The mS VTF‐treated oocytes were diluted in S3‐Oocyte solutions in 3 steps (5min, 2min, 1min) and maintained in shortened (cut: 2.0 cm) sterile flexipettes (300 mm ID, Cook), detached, sterile wiped, and sealed into CBSu0002 High Security straws. SF oocytes were treated in 2 steps of CJ3 solution loaded into CBSu0002 straws and cooled slowly (‐0.3u0003C/min from ‐7u0003C to ‐35u0003C then plunged). All oocytes were thawed at room temperature in a series of sucrose dilutions. ICSI was performed on surviving oocytes 2hr postthaw and cultured in LG medium 5%SS (tri‐gas, 37u0003C) | |
| Outcomes | Ongoing pregnancy rate: vitrification 47% versus slow freezing 10%. Clinical pregnancy rate: vitrification 67% and slow freezing 10% | |
| Notes | In a personal communication, the author detailed how participants were allocated to each intervention group and how many were in each group. Funded by EMD Serono, a subsidiary of Merck |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants were blinded but personnel were not |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding of outcome assessment was not stated, but the review authors judge that the outcome measurement is not likely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon) |
| Other bias | Low risk | No conflict of interest |
Smith 2010.
| Methods | Random allocation by random number generator | |
| Participants | Participants had 1) infertility attributable to tubal factor, severe male factor or unexplained factor; 2) regular, spontaneous menstrual cycles of 25 to 35 days; 3) acceptable follicular phase serum concentrations of follicle stimulating hormone (FSH;%10 IU/L), luteinizing hormone (LH;%13.5 IU/L), and estradiol (E2;%60 pg/mL); 4) body mass index% 30 kg/m2; 5) presence of both ovaries and normal uterine cavity. Patients with supernumerary mature oocytes (more than nine mature oocyte recovered after cumulus cell removal from the controlled ovarian stimulation IVF/ICSI cycle) were randomised (apparently n=230). All patients who failed to achieve a pregnancy in the fresh cycle were provided the option to transfer embryos derived from frozen/thawed or vitrified/warmed oocytes; n=78. This group of 78 received the intervention. | |
| Interventions | Oocyte slow freezing or vitrification | |
| Outcomes | Clinical pregnancies/thaw or warming cycle (%): SF 4/30 | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer random number generator |
| Allocation concealment (selection bias) | Unclear risk | It is not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | It is not mentioned |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding of outcome assessment was not stated, but the review authors judge that the outcome measurement is not likely to be influenced by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | The study protocol is not available but it is clear that the published reports include all expected outcomes |
| Other bias | Unclear risk | Conflict of interests: Irvine Scientific has provided the closed‐pulled straws and vitrification/warming solutions. Besides, only some of the randomised participants finally underwent the treatment and were analysed in the study, which could possibly create a bias in the selection of participants |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Behr 2005 | It is not about vitrification |
| Cao 2009 | Outcomes do not include live birth rate, ongoing pregnancy rate or clinical pregnancy rate |
| Cobo 2011b | It is not a randomised controlled trial |
| Cutting 2009 | It is not a randomised controlled trial |
| Edgar 2012 | It is not a randomised controlled trial |
| Fabbri 1998 | It is not a randomised controlled trial |
| Forman 2011 | Randomisation of oocytes from each woman, and not randomisation of women |
| Ragni 2007 | Randomisation of oocytes from each woman, and not randomisation of women |
Characteristics of studies awaiting assessment [ordered by study ID]
Greenblatt 2014.
| Methods | Randomised, parallel assignment, single‐blind |
| Participants | 14 or more oocytes at ovum pick‐up Age < 38 years BMI < 30 |
| Interventions | Slow freeze versus vitrification |
| Outcomes | Post‐thaw oocyte survival rate (time frame: 2 years) (designated as safety issue: no) Fertilisation rate Cleavage Embryo development Implantation rate Ongoing pregnancy |
| Notes |
NCT00777387 Study terminated: "studies emerged that demonstrated the superiority of vitrification" |
Hershlag 2012.
| Methods | Randomised, cross‐over asignment, open label |
| Participants | Donors: women ages 21‐32 years who wish to donate their eggs; must pass medical, physical and psychological screening Recipients: women under the age of 50 years who wish to have eggs donated to them through the Donor Egg Program and who also pass the medical, physical and psychological screening |
| Interventions | Slow freeze versus vitrification |
| Outcomes | Achievement of a pregnancy, as determined by a fetal heartbeat Percentage of eggs that result in blastocyst formation Oocyte survival ICSI fertilisation rate (percentage of eggs that fertilise) Incidence rate of embryo formation |
| Notes | NCT00852306 |
Differences between protocol and review
Outcomes such as survival rate (Table 2) and fertilisation rate (Table 3) were only included as additional tables because women were the unit of randomisation and performing a meta‐analysis of the above mentioned outcomes would not have been appropriate.
Considering that the intervention showed large effects, we used RR instead of the Peto OR as we had stated in the protocol. We based our decision on the Cochrane Handbook for Systematic Reviews of Interventions that states: 'The approximation used in the computation of the log odds ratio works well when intervention effects are small (odds ratios are close to one), events are not particularly common and the studies have similar numbers in experimental and control groups. In other situations it has been shown to give biased answers. As these criteria are not always fulfilled, Peto’s method is not recommended as a default approach for meta‐analysis'.
Contributions of authors
Demian Glujovsky: conceived the protocol of the review, co‐ordinated the whole process, did screening of studies, did data extraction and wrote the review.
Riestra Barbara: conceived the protocol of the review, did screening of studies, did data extraction and wrote the review.
Carlos Sueldo: provided general advice on the protocol and wrote the review.
Gabriel Fiszbajn: participated in the protocol development and wrote the review.
Sjoerd Repping: provided general advice on the protocol and wrote the review.
Florencia Nodar: participated in the protocol development and wrote the review.
Sergio Papier: participated in the protocol development and wrote the review.
Agustín Ciapponi: supervised the methods of the protocol, did screening of studies and wrote the review.
Sources of support
Internal sources
None, Other.
External sources
None, Other.
Declarations of interest
None
New
References
References to studies included in this review
Schiewe 2010 {published data only}
- Schiewe MC. Donor oocyte cryopreservation: A randomized clinical trial comparing microsecure vitrification (mS VTF) to choline‐enriched CJ3 slow‐freezing (SF). Personal communication.
- Schiewe MC, Nugent N, Zozula S, Stachecki JJ, Anderson RE. Donor oocyte cryopreservation: A randomized clinical trial comparing microsecure vitrification (mS VTF) to choline‐enriched CJ3 slow‐freezing (SF). Fertility and Sterility 2010;94(4, Supplement):S117‐8. [Google Scholar]
Smith 2010 {published data only}
- Fioravanti J, Alegretti JR, Hassun PA, Motta ELA, Serafini PC, Smith GD. Prospective randomized comparison of human oocyte freezing and vitrification: an update. Fertility and Sterility 2007;88:S13. [DOI] [PubMed] [Google Scholar]
- Motta E, Serafini P, Fioravanti J, Alegretti JR, Hassun PA, Smith GD. Prospective randomized study of human oocyte cryopreservation by slow‐rate freezing or vitrification. Human Reproduction 2008;23:151. [DOI] [PubMed] [Google Scholar]
- Smith GD, Serafini PC, Fioravanti J, et al. Prospective randomized comparison of human oocyte cryopreservation with slow‐rate freezing or vitrification. Fertility and Sterility 2010;94(6):2088‐95. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Behr 2005 {published data only}
- Behr B, Le A, Khoury C, Boostanfar B, Feinman M, Frederick J. Comparison between two different human oocyte cryopreservation protocols on survival, fertilization and embryo development. Fertility and Sterility 2005;83(5):S19‐20. [Google Scholar]
Cao 2009 {published data only}
- Cao YX, Xing Q, Li L, Cong L, Zhang ZG, Wei ZL, et al. Comparison of survival and embryonic development in human oocytes cryopreserved by slow‐freezing and vitrification. Fertility and Sterility 2009;92(4):1306‐11. [DOI] [PubMed] [Google Scholar]
Cobo 2011b {published data only}
- Cobo A, Diaz C. Clinical application of oocyte vitrification: A systematic review and meta‐analysis of randomized controlled trials. Fertility and Sterility 2011;96(2):277‐85. [DOI] [PubMed] [Google Scholar]
Cutting 2009 {published data only}
- Cutting R, Barlow S, Anderson R. Human oocyte cryopreservation: Evidence for practice. Human Fertility 2009;12(3):125‐36. [DOI] [PubMed] [Google Scholar]
Edgar 2012 {published data only}
- Edgar DH, Gook DA. A critical appraisal of cryopreservation (slow cooling versus vitrification) of human oocytes and embryos. Human Reproduction Update 2012;18(5):536‐54. [DOI] [PubMed] [Google Scholar]
Fabbri 1998 {published data only}
- Fabbri R, Porcu E, Marsella T, Primavera MR, Seracchioli R, Ciotti PM, et al. Oocyte cryopreservation. Human Reproduction 1998;13 Suppl 4:98‐108. [DOI] [PubMed] [Google Scholar]
Forman 2011 {published data only}
- Forman EJ, Ferry KM, Benson MR, Campos J, Treff NR, Scott RT Jr. Embryos derived from vitrified oocytes are not at an increased risk of aneuploidy and demonstrate excellent implantation rates: a paired, randomised controlled trial (RCT) in an infertile population. Fertility and Sterility 2011;96(3):S44 O‐146. [Google Scholar]
Ragni 2007 {published data only}
- Ragni G, Paffoni A, Alagna F, Restelli L, Somigliana E. Reduced developmental potential of human oocytes after vitrification compared to slow freezing. Fertility and Sterility 2007;88(1):345. [Google Scholar]
References to studies awaiting assessment
Greenblatt 2014 {published data only}
- Greenblatt Ellen M. Randomized controlled trial comparing slow‐freezing to vitrification of oocytes. ClinicalTrials.gov. ClinicalTrials.gov, 2014.
Hershlag 2012 {published data only}
- Hershlag Avner, Cohen Matthew, Feng Huai L. A comparison of two freezing techniques. ClinicalTrials.gov. Clinical Trials.gov, 2012.
Additional references
Albertini 2011
- Albertini DF. The dawning of a new ice age for human oocyte cryopreservation. Journal of Assisted Reproduction and Genetics 2011; Vol. 28, issue 12:1141‐2. [PUBMED: 22167379] [DOI] [PMC free article] [PubMed]
ASRM 2013
- American Society for Reproductive Medicine (ASRM). Mature oocyte cryopreservation: a guideline. Fertility and Sterility 2013;99(1):37‐43. [DOI] [PubMed] [Google Scholar]
Bonetti 2011
- Bonetti A, Cervi M, Tomei F, Marchini M, Ortolani F, Manno M. Ultrastructural evaluation of human metaphase II oocytes after vitrification: closed versus open devices. Fertility and Sterility 2011;95(3):928‐35. [PUBMED: 20864096] [DOI] [PubMed] [Google Scholar]
Borini 2010
- Borini A, Levi Setti PE, Anserini P, Luca R, Santis L, Porcu E, et al. Multicenter observational study on slow‐cooling oocyte cryopreservation: clinical outcome. Fertility and Sterility 2010;94(5):1662‐8. [PUBMED: 20047739] [DOI] [PubMed] [Google Scholar]
Chen 1986
- Chen C. Pregnancy after human oocyte cryopreservation. Lancet 1986;1(8486):884‐6. [PUBMED: 2870356] [DOI] [PubMed] [Google Scholar]
Chen 2003
- Chen SU, Lien YR, Chao KH, Ho HN, Yang YS, Lee TY. Effects of cryopreservation on meiotic spindles of oocytes and its dynamics after thawing: clinical implications in oocyte freezing ‐ a review article. Molecular and Cellular Endocrinology 2003;202(1‐2):101‐7. [PUBMED: 12770738] [DOI] [PubMed] [Google Scholar]
Ciapponi 2011a
- Ciapponi A, Glujovsky D, Bardach A, García Martí S, Comande D. EROS: a new software for early stage of systematic reviews. HTAi 2011 Conference. Rio de Janeiro, Brazil, 2011, June 27‐29.
Ciapponi 2011b
- Ciapponi A, Glujovsky D, Bardach A, García Martí S, Comande D. EROS: a new software for early stage of systematic reviews. ISPOR 3rd Latin America Conference. Hilton Mexico City Reforma in Mexico City, Mexico, 2011 September 8‐10.
Cobo 2008
- Cobo A, Kuwayama M, Perez S, Ruiz A, Pellicer A, Remohi J. Comparison of concomitant outcome achieved with fresh and cryopreserved donor oocytes vitrified by the Cryotop method. Fertility and Sterility 2008;89(6):1657‐64. [PUBMED: 17889865] [DOI] [PubMed] [Google Scholar]
Cobo 2010
- Cobo A, Meseguer M, Remohi J, Pellicer A. Use of cryo‐banked oocytes in an ovum donation programme: a prospective, randomized, controlled, clinical trial. Human Reproduction 2010;25(9):2239‐46. [PUBMED: 20591872] [DOI] [PubMed] [Google Scholar]
Cobo 2011a
- Cobo A, Remohi J, Chang CC, Nagy ZP. Oocyte cryopreservation for donor egg banking. Reproductive Biomedicine Online 2011;23(3):341‐6. [PUBMED: 21767989] [DOI] [PubMed] [Google Scholar]
Cobo 2012a
- Cobo A, Garrido N, Crespo J, Jose R, Pellicer A. Accumulation of oocytes: a new strategy for managing low‐responder patients. Reproductive Biomedicine Online 2012;24(4):424‐32. [PUBMED: 22386762] [DOI] [PubMed] [Google Scholar]
Cobo 2012b
- Cobo A, Bellver J, Santos MJ, Remohi J. Viral screening of spent culture media and liquid nitrogen samples of oocytes and embryos from hepatitis B, hepatitis C, and human immunodeficiency virus chronically infected women undergoing in vitro fertilization cycles. Fertility and Sterility 2012;97(1):74‐8. [PUBMED: 22035968] [DOI] [PubMed] [Google Scholar]
Dominguez 2013
- Dominguez F, Castello D, Remohi J, Simon C, Cobo A. Effect of vitrification on human oocytes: a metabolic profiling study. Fertility and Sterility 2013;99(2):565‐72. [PUBMED: 23102858] [DOI] [PubMed] [Google Scholar]
Fahy 2007
- Fahy GM. Theoretical considerations for oocyte cryopreservation by freezing. Reproductive Biomedicine Online 2007;14(6):709‐14. [PUBMED: 17579984] [DOI] [PubMed] [Google Scholar]
Friedler 1988
- Friedler S, Giudice LC, Lamb EJ. Cryopreservation of embryos and ova. Fertility and Sterility 1988;49(5):743‐64. [PUBMED: 3282929] [DOI] [PubMed] [Google Scholar]
Friedler 2012
- Friedler S, Koc O, Gidoni Y, Raziel A, Ron‐El R. Ovarian response to stimulation for fertility preservation in women with malignant disease: a systematic review and meta‐analysis. Fertility and Sterility 2012;97(1):125‐33. [PUBMED: 22078784] [DOI] [PubMed] [Google Scholar]
Glujovsky 2010
- Glujovsky D, Bardach A, García Martí S, Comande D, Ciapponi A. New software for early stage of systematic reviews. XVIII Cochrane Colloquium. The Joint Colloquium of the Cochrane and Campbell Collaborations. Keystone Resort, Colorado, US, 2010 October 18‐22.
Gook 2007
- Gook DA, Edgar DH. Human oocyte cryopreservation. Human Reproduction Update 2007;13(6):591‐605. [PUBMED: 17846105] [DOI] [PubMed] [Google Scholar]
Gook 2011
- Gook DA. History of oocyte cryopreservation. Reproductive Biomedicine Online 2011;23(3):281‐9. [PUBMED: 21549640] [DOI] [PubMed] [Google Scholar]
Gosden 2011
- Gosden R. Cryopreservation: a cold look at technology for fertility preservation. Fertility and Sterility 2011;96(2):264‐8. [PUBMED: 21718989] [DOI] [PubMed] [Google Scholar]
Herrero 2011
- Herrero L, Pareja S, Losada C, Cobo AC, Pellicer A, Garcia‐Velasco JA. Avoiding the use of human chorionic gonadotropin combined with oocyte vitrification and GnRH agonist triggering versus coasting: a new strategy to avoid ovarian hyperstimulation syndrome. Fertility and Sterility 2011;95(3):1137‐40. [PUBMED: 21047635] [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jain 2006
- Jain JK, Paulson RJ. Oocyte cryopreservation. Fertility and Sterility 2006;86(4 Suppl):1037‐46. [PUBMED: 17008147] [DOI] [PubMed] [Google Scholar]
Kader 2009
- Kader AA, Choi A, Orief Y, Agarwal A. Factors affecting the outcome of human blastocyst vitrification. Reproductive Biology and Endocrinology 2009;7:99. [PUBMED: 19758458] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2006
- Kim SS. Fertility preservation in female cancer patients: current developments and future directions. Fertility and Sterility 2006;85(1):1‐11. [PUBMED: 16412718] [DOI] [PubMed] [Google Scholar]
Leibo 2011
- Leibo SP, Pool TB. The principal variables of cryopreservation: solutions, temperatures, and rate changes. Fertility and Sterility 2011;96(2):269‐76. [PUBMED: 21782053] [DOI] [PubMed] [Google Scholar]
Lockwood 2011
- Lockwood GM. Social egg freezing: the prospect of reproductive 'immortality' or a dangerous delusion?. Reproductive Biomedicine Online 2011;23(3):334‐40. [PUBMED: 21775211] [DOI] [PubMed] [Google Scholar]
Martinez‐Burgos 2011
- Martinez‐Burgos M, Herrero L, Megias D, Salvanes R, Montoya MC, Cobo AC, et al. Vitrification versus slow freezing of oocytes: effects on morphologic appearance, meiotic spindle configuration, and DNA damage. Fertility and Sterility 2011;95(1):374‐7. [PUBMED: 20828688] [DOI] [PubMed] [Google Scholar]
Matthews 2012
- Matthews ML, Hurst BS, Marshburn PB, Usadi RS, Papadakis MA, Sarantou T. Cancer, fertility preservation, and future pregnancy: a comprehensive review. Obstetrics and Gynecology International 2012;2012:953937. [PUBMED: 22529860] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mullen 2004
- Mullen SF, Agca Y, Broermann DC, Jenkins CL, Johnson CA, Critser JK. The effect of osmotic stress on the metaphase II spindle of human oocytes, and the relevance to cryopreservation. Human Reproduction 2004;19(5):1148‐54. [PUBMED: 15070883] [DOI] [PubMed] [Google Scholar]
Noyes 2009
- Noyes N, Porcu E, Borini A. Over 900 oocyte cryopreservation babies born with no apparent increase in congenital anomalies. Reproductive Biomedicine Online 2009;18(6):769‐76. [PUBMED: 19490780] [DOI] [PubMed] [Google Scholar]
Paffoni 2008
- Paffoni A, Alagna F, Somigliana E, Restelli L, Brevini TA, Gandolfi F, et al. Developmental potential of human oocytes after slow freezing or vitrification: a randomized in vitro study based on parthenogenesis. Reproductive Sciences 2008;15(10):1027‐33. [PUBMED: 19088372] [DOI] [PubMed] [Google Scholar]
Revel 2010
- Revel A, Revel‐Vilk S. Fertility preservation in young cancer patients. Journal of Human Reproductive Sciences 2010;3(1):2‐7. [PUBMED: 20607000] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rienzi 2010
- Rienzi L, Romano S, Albricci L, Maggiulli R, Capalbo A, Baroni E, et al. Embryo development of fresh 'versus' vitrified metaphase II oocytes after ICSI: a prospective randomized sibling‐oocyte study. Human Reproduction 2010;25(1):66‐73. [PUBMED: 19861328] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rudick 2010
- Rudick B, Opper N, Paulson R, Bendikson K, Chung K. The status of oocyte cryopreservation in the United States. Fertility and Sterility 2010;94(7):2642‐6. [PUBMED: 20723535] [DOI] [PubMed] [Google Scholar]
Sansinena 2011
- Sansinena M, Santos MV, Zaritzky N, Chirife J. 42 comparison of cooling rates in oocyte vitrification systems using a numerical simulation. Reproduction, Fertility and Development 2011;24(1):133‐4. [PUBMED: 22394764] [Google Scholar]
Saragusty 2011
- Saragusty J, Arav A. Current progress in oocyte and embryo cryopreservation by slow freezing and vitrification. Reproduction 2011;141(1):1‐19. [PUBMED: 20974741] [DOI] [PubMed] [Google Scholar]
Siano 2013
- Siano L, Engmann L, Nulsen J, Benadiva C. A prospective pilot study comparing fertilization and embryo development between fresh and vitrified sibling oocytes. Connecticut Medicine 2013;77(4):211‐7. [PUBMED: 23691734] [PubMed] [Google Scholar]
Smith 2011
- Smith GD, Motta EE, Serafini P. Theoretical and experimental basis of oocyte vitrification. Reproductive Biomedicine Online 2011;23(3):298‐306. [PUBMED: 21763203] [DOI] [PubMed] [Google Scholar]
Sole 2013
- Sole M, Santalo J, Boada M, Clua E, Rodriguez I, Martinez F, et al. How does vitrification affect oocyte viability in oocyte donation cycles? A prospective study to compare outcomes achieved with fresh versus vitrified sibling oocytes. Human Reproduction 2013;28(8):2087‐92. [PUBMED: 23744895] [DOI] [PubMed] [Google Scholar]
Stoop 2011
- Stoop D, Nekkebroeck J, Devroey P. A survey on the intentions and attitudes towards oocyte cryopreservation for non‐medical reasons among women of reproductive age. Human Reproduction 2011;26(3):655‐61. [PUBMED: 21212052] [DOI] [PubMed] [Google Scholar]
Trounson 1983
- Trounson A, Mohr L. Human pregnancy following cryopreservation, thawing and transfer of an eight‐cell embryo. Nature 1983;305(5936):707‐9. [PUBMED: 6633637] [DOI] [PubMed] [Google Scholar]
Tucker 2004
- Tucker M, Morton P, Liebermann J. Human oocyte cryopreservation: a valid alternative to embryo cryopreservation?. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2004;113 Suppl 1:S24‐7. [PUBMED: 15041126] [DOI] [PubMed] [Google Scholar]
Zhang 2011
- Zhang Z, Liu Y, Xing Q, Zhou P, Cao Y. Cryopreservation of human failed‐matured oocytes followed by in vitro maturation: vitrification is superior to the slow freezing method. Reproductive Biology and Endocrinology 2011;9:156. [PUBMED: 22151887] [DOI] [PMC free article] [PubMed] [Google Scholar]