

Abstract
The objective of our study was to reanalyse the Ethiopia STEPwise approach to Surveillance Noncommunicable Disease Risk Factors survey (NCD STEPS), using causal path diagrams constructed using expert subject matter knowledge in conjunction with graphical model theory to map the underlying causal network of modifiable factors associated with prediabetes/diabetes and hypertension. We used data from the 2015 Ethiopia NCD STEPS representative cross‐sectional survey (males; n = 3977 and females; n = 5823 aged 15–69 years) and performed directed acyclic graph‐informed logistic regression analyses. In both sexes, a 1‐unit higher in body mass index (BMI) and waist circumference (WC) were positively associated with prediabetes/diabetes (BMI: males: adjusted odds ratio [aOR]: 1.07 [95% confidence interval: 1.0, 1.1], females aOR: 1.03 [1.0, 1.1]; WC: males: aOR: 1.1 [0.9, 1.2], females: aOR: 1.2 [1.1, 1.3]) and hypertension (BMI: males: aOR: 1.2 [1.1, 1.2], females aOR: 1.1 [1.0, 1.1]; WC: males: aOR: 1.6 [1.4, 1.8], females: aOR: 1.3 [1.2, 1.5]). Although residing in urban settings was associated with higher odds of hypertension in both males (aOR: 1.79 [1.49, 2.16]) and females (aOR: 1.70 [1.49, 1.95]), it was only associated with prediabetes/diabetes in males (aOR: 1.56 [1.25, 1.96]). Males and females in pastoralist areas had lower odds of prediabetes/diabetes compared with their agrarian counterparts (males: aOR: 0.27 [0.14, 0.52], females: aOR: 0.31 [0.16, 0.58]). Physical activity was associated with lower odds of prediabetes/diabetes among females (aOR: 0.75 [0.58, 0.97]). Other diet‐related modifiable factors such as consumption of fruit and vegetable, alcohol or salt were not associated with either prediabetes/diabetes or hypertension. Our findings highlight the need to implement interventions that prevent overweight/obesity and nutrition‐related NCDs, particularly in urban areas.
Keywords: diabetes, Ethiopia, hypertension, noncommunicable diseases, prediabetes, risk factors
We provide empirical findings relating to the factors associated with hypertension and prediabetes/diabetes among Ethiopian males and females. Our findings highlight the need to implement interventions that promote healthy lifestyles to address the burden of overweight/obesity and Nutrition‐Related Noncommunicable Diseases, particularly in urban areas.
Key messages
Body mass index and waist circumference were positively associated with hypertension and prediabetes/diabetes for both sexes. Residing in urban settings was associated with increased odds of hypertension in both sexes, and with prediabetes/diabetes in males. Physical activity was associated with lower odds of prediabetes/diabetes among women.
Diet‐related factors (consumption of fruit and vegetables, alcohol, and salt) were not associated with either hypertension or prediabetes/diabetes.
There is a need for longitudinal, nationally representative dietary surveys, which enable the derivation of relevant indicators of the nutrition transition in Ethiopia.
1. INTRODUCTION
Noncommunicable diseases (NCDs) are the leading causes of mortality among adults globally and account for 70% of all global deaths annually (Institute for Health Metrics and Evaluation, 2019). The public health burden of NCDs is increasing in low‐ and middle‐income countries (LMICs), with individuals facing a substantially higher risk of premature NCD death compared with high‐income countries (Allen et al., 2017). Diabetes, defined as fasting blood glucose > 126 mg/dl (7.0 mmol/L; World Health Organization [WHO] & International Diabetes Federation, 2006), is one of the most prevalent nutrition‐related NCDs (NR‐NCDs) globally, with the incidence of diabetes increasing from 11.3 million in 1990 to 22.9 million in 2017 (Lin et al., 2020). The largest increase was seen in LMICs (Lin et al., 2020). Additionally, prediabetes (fasting blood glucose: 100–125 mg/dl; American Diabetes Association, 2021), increases predisposition to future progression into diabetes and is associated with higher risk of diabetic complications (Hostalek, 2019). Hypertension is another major contributor to the growing burden on NR‐NCDs globally; 1.13 billion people worldwide have hypertension (WHO, 2021a) with Africa displaying the highest prevalence (27%; WHO, 2021a).
In Ethiopia, the nutrition transition (i.e., the substitution of traditional plant‐based diets with increased intakes of animal products, saturated fats and processed foods, alongside reduced intake of fibres and increased time spent sedentary) has contributed to an increased prevalence of overweight, obesity and associated NR‐NCDs such as hypertension and diabetes in the past decade (Central Statistical Agency and ICF, 2016; Central Statistical Authority Ethiopia and ORC Macro, 2001; Ethiopian Public Health Institute (EPHI), Federal Ministry of Health, and WHO, 2016; Gebreyes et al., 2018; Misganaw et al., 2014). The diet transformation between 1996 and 2011 in Ethiopia has been documented recently (Worku et al., 2017). This shift has occurred alongside improvements in access to health services, which has seen NR‐NCDs replace communicable diseases as the leading causes of mortality in Ethiopia. For example, cardiovascular diseases were the second leading causes of mortality in Ethiopia in 2019 (Institute for Health Metrics and Evaluation, 2019). In response to the increasing burden of NR‐NCDs, the Ethiopian Government designed the national strategic action plan (NSAP) for the prevention and control of NCDs in 2014 (Federal Democratic Republic of Ethiopia: Ministry of Health, 2014). The main priority areas for action include health promotion and disease prevention to address behavioural risk factors and comprehensive NCD treatment, care and support (Federal Democratic Republic of Ethiopia: Ministry of Health, 2014). The importance of tackling NCDs for sustainable development was also emphasized in the Sustainable Development Goals (SDGs), which aim to reduce premature deaths from NCDs by a third by 2030 (SDG3; United Nations, n.d.). Accordingly, if progress is to be made in achieving the NCD‐related SDGs and the targets set out in the NSAP, then an understanding of the modifiable metabolic and behavioural factors associated with NR‐NCDs is critical so that priority interventions and target groups can be identified.
Gebreyes et al. (2018) used data from the most recently conducted nationally representative survey (WHO NCD STEPwise approach to Surveillance [STEPS] survey) in Ethiopia, to identify risk factors for a number of NR‐NCDS, including dyslipidaemia, high blood pressure and hyperglycaemia. However, the identification of risk factors and covariates used to address confounding was based on the attainment of a prespecified level of significance (p < 0.05) in univariate analyses, with no consideration of the underlying causal network underpinning these associations. This approach is likely to have introduced bias into the estimates of the association between identified risk factors and the outcomes.
Accordingly, the aim of this study was to re‐analyse the WHO NCD STEPS survey using causal path diagrams derived using expert subject matter knowledge and graphical model theory to map the underlying causal network and thus identify a more conceptually appropriate set of modifiable factors associated with prediabetes/diabetes and hypertension among males and females in Ethiopia.
2. METHODS
2.1. Sample
We used data from 3977 males and 5823 females participating in the Ethiopian STEPS. The STEPS has been described elsewhere (WHO, 2021b), including details regarding the sample size determination, the sampling procedure, and data collection and management protocols. In brief, the Ethiopian STEPS survey was conducted in 2015 and followed the WHO STEPwise approach to surveillance for the identification of risk factors for NCDs in a nationally representative sample. The target population for the Ethiopian STEPS survey included all males and females aged 15–69 years, who had lived at their current place of residence for at least 6 months. A total of 513 Enumeration Areas (EAs) were covered nationwide, of which 404 were rural and 109 were urban. Twenty households (HHs) per EA were selected using systematic random sampling and one eligible individual from each HH was selected using the Kish method (a random selection of eligible individuals at HH level; Kish, 1949). The STEPS survey collected information on five main NCD risk factors, namely tobacco use, alcohol consumption, diet, physical activity and history of chronic disease. Additionally, blood pressure and body size measurements were taken. Blood pressure, in a sitting position, was measured three times on the right arm using an automatic digital sphygmomanometer (Boso‐Medicus Uno, BOSCH + SOHN). Systolic (SBP) and diastolic blood pressure (DBP) were recorded and the mean of the three measurements was used for analysis. Height and weight were measured with the electronic Growth Management Scale. Waist circumference (WC) was measured by placing a tape measure around the abdomen at the midpoint between the lower margin of the last rib and the top of iliac crest of the hip bone (further details can be found in Supporting Information 2). Venous blood sampling was conducted and cardiometabolic biomarkers were obtained (e.g., blood glucose and blood lipids). Fasting blood glucose, total cholesterol and high‐density lipoprotein cholesterol levels were measured using a CardioCheck PA Analyzer. Fasting triglyceride levels were measured using Cobas Integra 400 Plus (Roche Diagnostics GmbH) clinical chemistry analyzer.
The NCD STEP protocol was reviewed and approved by Institution Review Board of EPHI and National Ethics Review Committee of Ministry of Science and Technology. Informed consent was obtained from each participant and consent obtained from parents and guardians for those participants between age 15 and 17 years. For this secondary analysis of data, ethical approval was not required.
2.2. Outcomes
The outcome variables were prediabetes/diabetes and hypertension. Prediabetes/diabetes was defined as fasting blood glucose > 100 mg/dl (5.6 mmol/L; American Diabetes Association, 2021; WHO & International Diabetes Federation, 2006) or currently taking any medication, such as insulin, prescribed for diabetes. Hypertension was defined as SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg (Unger et al., 2020) or currently taking medication for raised blood pressure or hypertension.
2.3. Exposure
To identify nutritional, behavioural and socioeconomic factors previously associated with obesity, prediabetes/diabetes and hypertension in Sub‐Saharan Africa, we conducted a systematic literature review. We included studies that were conducted on adult males and females. The inclusion and exclusion criteria, search strategy and the search log are included in the Supporting Information 1. After screening, 750 studies were identified, from which we extracted data regarding variables associated with prediabetes/diabetes and hypertension (and relevant covariates). Modifiable factors included fruit and vegetable intake, urban residence, educational attainment, occupation: nonagricultural work, income, alcohol intake, khat chewing, smoking, salt intake, physical activity and livelihood (pastoralist). A description of the exposures and covariates included in the NCD STEPS analysis are included in Supporting Information 2.
2.4. Statistical analysis
Using these variables, a provisional causal path diagram was constructed to visualize the relationships between factors, outcomes and covariates. This preliminary causal path diagram was then used to facilitate discussion during a consultation with experts (n = 14) from the fields of nutrition, NCD epidemiology and public health. Using the expert knowledge, a formal causal path diagram was produced, which was used to inform the model‐building process of the statistical analysis. Our causal path diagrams, or ‘directed acyclic graphs’ (DAGs) were constructed using the open‐access software, DAGitty version 3.0 (Textor et al., 2016), which enables the creation of a DAG in a robust, systematic and reproducible manner. Briefly, DAGitty employs graphical model theory to search for covariate sets that qualify as ‘adjustment sets’, which, upon adjusting for, remove all confounding from the specified DAG. Using this overall DAG, a DAG was produced for each separate exposure of interest in relation to each of the outcome variables, resulting in the construction of a series of exposure‐outcome‐specific multivariable regression models. The overall DAG from which each specific exposure‐outcome DAG stemmed is shown in Supporting Information 3.
As it has been shown that associations between a number covariates and hypertension and prediabetes/diabetes may differ between the sexes (Choi et al., 2017; Everett & Zajacova, 2015; Ghosh et al., 2016; Kautzky‐Willer et al., 2016; McKenzie et al., 2020; Meisinger et al., 2002; Njølstad et al., 1998), an a priori decision was made to stratify the analysis by sex.
Estimates of prevalence were calculated with the appropriate sampling weights applied to account for the sampling procedure; however, for inferential statistics, no weighting was applied. Multivariable logistic regression models based on those with complete data for exposure, outcome and covariates (i.e., complete case analyses), were used to investigate the association between each modifiable factor and hypertension and separately, prediabetes/diabetes. Associations were reported as adjusted odds ratios (aOR) and their 95% confidence intervals (CIs). Adjustment sets for each modifiable factor were identified using the DAGs constructed for each of the outcomes, with adjustment sets being specific for each exposure‐outcome model. Data management and statistical analysis were conducted in Stata Version 16.1.
3. RESULTS
Descriptive characteristics of the sample included, stratified by sex, are shown in Table 1. The mean age of males and females included in the analysis was 31 years (SD: 13 and 12 years, respectively). The prevalence of prediabetes/diabetes and hypertension in males and females, respectively, was 11.2% and 11.3%, and 17.2% and 17.6%, respectively. The prevalence of overweight/obesity was twice as higher in females than in males, at 8.6% and 4.3%, respectively.
Table 1.
Sample characteristics (n = 9800) a
| Missing, n (%) | Males (n = 3977) | Females (n = 5823) | |
|---|---|---|---|
| Age (years) | – | 31.4 (13.4) | 30.6 (12.1) |
| Prediabetes and diabetes (yes) | 1011 (10.3) | 11.2 | 11.3 |
| Hypertension (yes) | 126 (1.3) | 17.2 | 17.6 |
| Overweight/obesity (yes) | 523 (5.3) | 4.3 | 8.6 |
| Urban residence (yes) | – | 15.6 | 23.3 |
| Fruit intake: five or more servings per day (yes) | – | 4.7 | 5.2 |
| Vegetable intake: five or more servings per day (yes) | – | 7.4 | 6.4 |
| Education (years) | 1 (0.01) | 5 (4) | 3 (4) |
| Occupation: nonagricultural worker (yes) | 6 (0.1) | 38.4 | 69.9 |
| Income >30,000 birr (yes) | 1683 (17.2) | 8.4 | 7.1 |
| Consumed alcohol in past 12 month (yes) | 23 (0.2) | 90.7 | 87.9 |
| Currently smoke (yes) | 4 (0.04) | 0.4 | 7.3 |
| Livelihood: pastoralist (yes) | – | 1.7 | 1.5 |
| Salt intake > 5 g/day (yes) | 1714 (17.5) | 97.1 | 96.3 |
| Physical activity > 150 min/week (yes) | – | 94.7 | 91.1 |
| Ever chewed Khat (yes) | 12 (0.1) | 25.5 | 11.2 |
| Average weekly meals prepared outside the home | 25 (0.3) | 0.7 (1.7) | 0.2 (1.0) |
| Triglycerides (mg/dl) | 1597 (16.3) | 124.6 (96.2) | 121.0 (92.1) |
| Total cholesterol (mg/dl) | 866 (8.8) | 124.4 (29.2) | 140.5 (36.5) |
| HDL (mg/dl) | 904 (9.2) | 37.9 (11.9) | 43.4 (13.4) |
| LDL (mg/dl) | 1597 (16.3) | 87.2 (34.9) | 102.1 (37.2) |
Note: Categorical variables are summarized as (n [%]) and continuous variables are summarized as mean (SD).
Abbreviations: HDL, high‐density lipoprotein; LDL, low‐density lipoprotein.
Weighted for survey design.
3.1. Associations between modifiable risk factors and prediabetes/diabetes
A 1 kg/m2 higher body mass index (BMI) was positively associated with prediabetes/diabetes in both males (aOR: 1.07 [95% CI: 1.0, 1.1]) and females (aOR: 1.03 [95% CI: 1.0, 1.1]; Figure 1). A 1 cm larger WC was associated with 10% (aOR: 1.1 [95% CI: 0.9, 1.2]) and 19% (aOR: 1.2 [95% CI: 1.1, 1.3]) higher odds of prediabetes/diabetes in males and females, respectively. Females who were engaged in nonagricultural work had higher odds of prediabetes/diabetes compared to agricultural workers (aOR: 1.4 [95% CI: 1.1, 1.8]). Residing in an urban setting (vs. rural) was positively associated with prediabetes/diabetes in males only (aOR: 1.6 [95% CI: 1.2, 2.0]). In contrast, pastoralist males (aOR: 0.3 [95% CI: 0.1, 0.5]) and females (aOR: 0.3 [95% CI: 0.2, 0.6]) had lower odds of prediabetes/diabetes compared with their agrarian counterparts. A 1‐year higher educational attainment level was associated with marginally lower odds of prediabetes/diabetes among females (aOR: 0.98 [95% CI: 0.95, 0.99]) and males (aOR: 0.96 [95% CI: 0.95, 0.99]). Females, but not males, who met WHO recommendations for physical activity (>150 min/week) had lower odds of prediabetes/diabetes (aOR: 0.8 [95% CI: 0.6, 1.0]).
Figure 1.
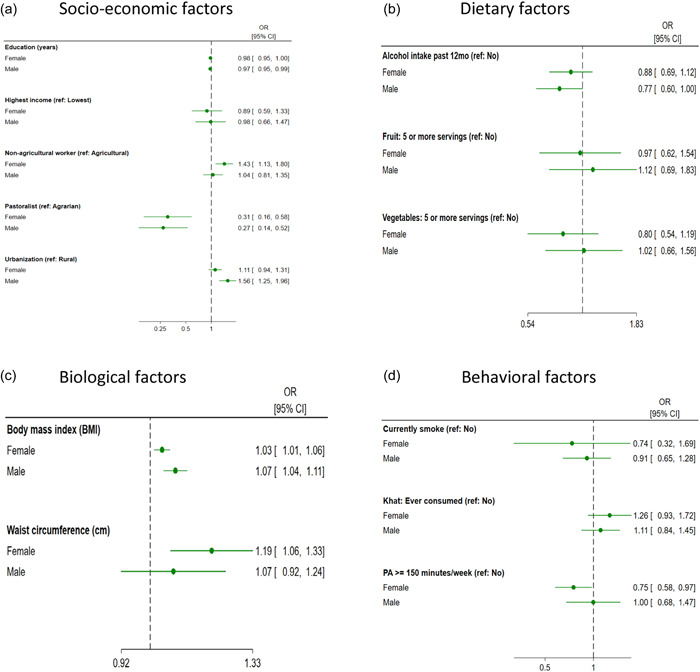
Modifiable (a) socioeconomic factors, (b) dietary factors, (c) biological factors and (d) behavioural factors associated with prediabetes/diabetes in males and females. Forest plots present odds ratios (ORs) and 95% confidene intervals (CIs)
3.2. Associations between modifiable risk factors and hypertension
BMI, WC and residing in an urban setting (vs. rural) were positively associated with hypertension in both males and females (Figure 2). A 1 kg/m2 higher BMI was associated with 20% and 10% higher odds of hypertension in males (aOR: 1.2 [95% CI: 1.1, 1.2]) and females (aOR: 1.1 [95% CI: 1.0, 1.1]), respectively. Similarly, a 1 cm larger WC was associated with 60% (aOR: 1.6 [95% CI: 1.4, 1.8]) and 30% (aOR: 1.3 [95% CI: 1.2, 1.5]) higher odds of hypertension in males and females, respectively. Males (aOR: 1.8 [95% CI: 1.5, 2.2]) and females (aOR: 1.7 [95% CI: 1.5, 1.9]) who resided in urban areas had higher odds of hypertension compared with their rural counterparts. Males who were engaged in nonagricultural work had higher odds of hypertension compared with agricultural workers (aOR: 1.3 [95% CI: 1.07, 1.64]). Pastoral females had higher odds of hypertension (aOR: 1.6 [95% CI: 1.1, 2.5]) compared with agrarian females. In contrast, a 1‐year higher educational attainment level was associated with lower odds of hypertension in females (aOR: 0.95 [95% CI: 0.9, 1.0]). Fruit and vegetable intake, daily salt intake >5 g/day, physical activity, and alcohol and khat intake were not associated with hypertension.
Figure 2.
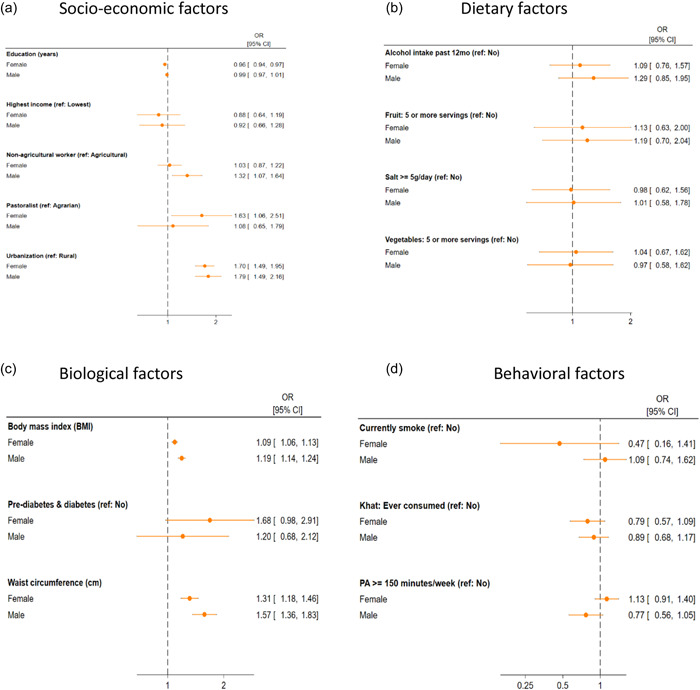
Modifiable (a) socioeconomic factors, (b) dietary factors, (c) biological factors and (d) behavioural factors associated with hypertension in males and females. Forest plots present odds ratios (ORs) and 95% confidence intervals (CIs)
4. DISCUSSION
4.1. Summary of findings
The objective of this study was to reanalyse data from the Ethiopia NCD STEP survey and use causal path diagrams based upon expert subject matter knowledge and graphical model theory, to identify a set of modifiable factors associated with prediabetes/diabetes and hypertension among males and females in Ethiopia. Nationally, the prevalence of prediabetes/diabetes and hypertension was ~11% and 17%, respectively, which was similar between the two sexes. Our analysis of modifiable factors showed that BMI and WC were positively associated with hypertension and prediabetes/diabetes for both males and females. An increase in WC was associated with increased odds of hypertension and prediabetes/diabetes in males and females. In contrast, an increase in educational attainment was associated with reduced odds of hypertension and prediabetes/diabetes in both males and females. Although residing in urban settings was associated with increased odds of hypertension in both males and females, it was only associated with prediabetes/diabetes in males. Males and females in pastoralist areas had lower odds of prediabetes/diabetes compared with their agrarian counterparts. In contrast, females in pastoralist areas had significantly higher odds of hypertension. Physical activity was associated with lower odds of prediabetes/diabetes among women only. Consumption of fruit and vegetables, alcohol, salt, smoking, khat consumption and income were not associated with either hypertension or prediabetes/diabetes.
4.2. Interpretation of findings
Our study extends the work by Gebreyes et al. (2018) by employing a more nuanced approach to the identification of factors related to hypertension and prediabetes/diabetes in Ethiopia. While we confirm several of the associations previously observed, with such triangulation increasing the confidence we have in these findings, our approach also resulted in a number of novel and/or altered findings. For example, whereas Gebreyes et al. (2018) observed associations between urban residence and lack of physical activity with diabetes in their sex‐combined models, we only observed these associations in males and females, respectively. In terms of novel findings, for prediabetes/diabetes we observed a positive association between nonagricultural work and prediabetes/diabetes in females, while a pastoralist livelihood and higher educational attainment were associated with reduced odds of prediabetes/diabetes. With regard to hypertension, we did not find, unlike Gebreyes et al. (2018), evidence for a protective effect of physical activity, whereas we did observe a female‐specific protective effect of educational attainment and hypertension.
Our finding that hypertension prevalence was ~17% and distributed similarly across both sexes is in line with other studies in Ethiopia (Dereje et al., 2020; Kibret & Mesfin, 2015). Residing in urban settings (vs. rural) was a consistent risk factor increasing the risk of hypertension in both sexes. This is in accordance with previous findings from Ethiopia (Kibret & Mesfin, 2015) but also the wider Sub‐Saharan (Addo et al., 2007) and African regions (Addo et al., 2007). Another risk factor for hypertension in both sexes was a higher BMI and WC, with a 1 cm higher WC associated with higher odds of hypertension (57% and 31% in males and females, respectively). Given the much greater burden of overweight/obesity in urban settings in Ethiopia, our finding of urban/rural disparities in hypertension prevalence is unsurprising. It has been speculated that other contributors to this urban/rural dichotomy include a greater use of motorized transport, sedentary types of occupation such as office work and an increased consumption of the high‐salt and high‐fat containing processed foods (Tesfaye et al., 2009). Surprisingly, we did not find strong evidence for a relationship between hypertension and each of physical activity, salt intake or consumption of fruits, vegetables and alcohol. Reasons for this between‐study discrepancy may include differences related to the sample (e.g., age, sex, ethnic composition and so on), differences in the derivation of variables or different covariates used in multivariable models across studies, or may be a result of the lack of variation in these variables, particularly for salt intake and physical activity.
Around 1 in 10 adults were classified as prediabetic or diabetic in this sample, with no differences between the sexes. However, these estimates are likely to underestimate the burden of prediabetes/diabetes in Ethiopia, as it is estimated that ~68% of individuals with diabetes are undiagnosed (International Diabetes Federation, 2019). We are not aware of any national studies in the country, which have reported on the prevalence of prediabetes/diabetes. However, two recent studies in the North of Ethiopia observed prevalence rates of prediabetes, which were ~1.5–4 times higher than in our study (Endris et al., 2019; He et al., 2020). Reasons for this discrepancy could relate to the criteria used to classify prediabetes, differences in the sociodemographic profiles of the samples, and thus differential exposure to prediabetes risk factors or, given the recency of the studies, may reflect real increases in the burden of prediabetes in more recent years. For example, recent national data suggest a diabetes prevalence of 3.2%, with more than 1.7 million individuals reported to have the condition. In absolute numbers, Ethiopia thus has the fourth highest burden of diabetes in Africa. In line with this prevalence, a meta‐analysis estimated the prevalence of diabetes in Ethiopia at between 2% and 6.5%, with the higher prevalence rates observed in urban settings (Bishu et al., 2019). Unsurprisingly, we also observed that the risk of prediabetes or diabetes was greater in those in urban settings. However, this association was much stronger in males. Although previous studies have shown disparities in the prevalence of prediabetes/diabetes in Ethiopia across sexes (Bishu et al., 2019; Endris et al., 2019; Woldegebriel et al., 2020) and between urban/rural settings, we are not aware of any studies that have identified an interaction between the two. We observed a protective effect of a pastoralist livelihood on risk for prediabetes/diabetes. Although we are unaware of any literature supporting this association, it may be a reflection of a higher level of physical activity in this group. Previous studies have suggested a link between low socioeconomic position, poor education and poverty, and diabetes risk; however, we did not observe associations with income and only small effects for education. In Ethiopia, there are large urban–rural inequalities in the provision of education and educational attainment (Sanfo & Ogawa, 2021) and so in our multivariable models, which also included adjustment for urban/rural residence, the association between education and prediabetes/diabetes is likely to be attenuated.
4.3. Strengths and limitations
The major strength of this analysis is the use of DAGs and graphical model theory to guide multivariable model building and to ensure that the correct covariates are (and are not) adjusted for. This is the first study in Ethiopia that has adopted this approach to identify a comprehensive list of factors that affect hypertension and prediabetes/diabetes. We acknowledge a number of limitations. As a cross‐sectional survey, with exposures and outcomes measured at the same time, we are unable to rule out the possibility of reverse‐causality contributing to associations observed here. Furthermore, although the NCD STEPS survey provides data on a wide range of demographic and biomedical variables, residual confounding is still a possibility. For example, depression was not available in NCD‐STEPs but was identified as a relevant factor in both the systematic review and during the expert consultation, and was classified as ‘unmeasured’ in the DAG (Supporting Information 3). However, even if this variable had been available, it was not included in the adjustment sets of any of the exposures, suggesting that this was not actually a confounding variable. By employing a complete case analysis, we may have inadvertently introduced a selection bias into our analysis. Nonresponse is more extensive in those from lower socioeconomic positions and with poorer health status (Mostafa & Wiggins, 2015; Stafford et al., 2013) and thus we may have inadvertently selected a more socioeconomically advantaged and healthier sample which, in addition to a loss of power, may have introduced bias into the observed associations. Our definition of prediabetes/diabetes was based on fasting blood glucose, which is more susceptible to acute perturbations in blood glucose levels than HbA1c. HbA1c provides an indication of average blood glucose over the previous 2–3 months and has been recommended for diagnosing prediabetes/diabetes (International Expert Committee on Diabetes, 2009; WHO, 2011). However, HbA1c (and detection methods) can be affected by conditions such as sickle cell disease and malaria (International Expert Committee on Diabetes 2009), both of which are prevalent in various African regions, including Ethiopia. Future nutritional surveillance surveys should consider collecting both blood glucose concentrations and HbA1c, and the concordance between the two should be assessed. As the NCD STEPS survey was conducted in 2015 in Ethiopia, it is likely that the burden of hypertension and prediabetes/diabetes has increased and the demographic profile of these conditions changed, which may potentially result in a different set of factors being associated with these conditions. The lack of association between diet‐related factors and hypertension and prediabetes/diabetes could be explained by the lack of variability in these factors or potential misreporting biases, which are inherent in retrospective dietary assessment methods. The variables used may also lack the required sensitivity (e.g., recall period/units of measurement and type of dietary indicator) to assess the relationship between diet and NR‐NCDs. There is a need for longitudinal, nationally representative dietary surveys, which enable the derivation of relevant indicators of the nutrition transition (e.g., consumption of ultraprocessed foods, energy‐dense nutrient‐poor foods, sugar‐sweetened beverages), to assess their contribution to the burden of overweight, obesity and NCD risk in Ethiopia.
4.4. Implications for research and policy
This study allowed the identification of policy options that could help address the burden of NR‐NCDs in Ethiopia. The major modifiable risk factors for prediabetes/diabetes and hypertension were a higher BMI, WC and physical inactivity (in women only). Thus, it is critical to: (i) promote healthy eating, physical activity and reduce sedentary time; and (ii) strengthen NCD surveillance to generate evidence on the burden of NR‐NCDs and associated risk factors. The consumption of healthy diets (i.e., increased consumption of nutrient‐rich foods [e.g., fruits and vegetables] and reduced consumption of unhealthy foods) could be increased through the implementation of agricultural and food system policy measures (e.g., monitoring of the availability and marketing of unhealthy foods; targeted taxation on unhealthy foods; food price policies and programmes to increase access to healthy foods). Healthy physical activity behaviours could be achieved through increasing awareness of the health benefits associated with moderate‐to‐vigorous intensity activities; improving the availability of facilities to promote physical activity (e.g., green spaces); implementing workplace programmes to combat sedentary time; and developing national guidelines for physical activity for health. Dietary and physical interventions should target urban residents who suffer the greater burden of poor nutrition and health. Finally, besides the collection of fruit and vegetable intake, salt intake and alcohol intake, NCD surveillance surveys should also incorporate other dietary indicators relevant to NR‐NCDs such as the consumption of sugar‐sweetened beverages and energy‐dense nutrient‐poor foods (savoury/salty snacks, sweet food items/products) so their contribution to the burden of NR‐NCDs can be better understood.
5. CONCLUSION
We have provided empirical findings relating to the factors associated with hypertension and prediabetes/diabetes among Ethiopian males and females. BMI and WC were the main factors that were positively associated with hypertension and prediabetes/diabetes among males and females. In contrast, a higher educational attainment was associated with reduced odds of hypertension and prediabetes/diabetes in both males and females. Other modifiable factors such as fruit and vegetables intake, salt intake, alcohol consumption and smoking were not associated with either hypertension or prediabetes/diabetes. Our findings highlight the need to implement interventions that promote healthy lifestyles to address the burden of overweight/obesity and NR‐NCDs, particularly in urban areas.
AUTHOR CONTRIBUTIONS
Meron Girma and Tom Norris designed the study with help from Aregash Samuel, Tirsit Genye, Alemayehu Hussen, Zerihun Bekele, Cornelia van Zyl and Rebecca Pradeilles. Tirsit Genye, Alemayehu Hussen and Zerihun Bekele analysed the data with help from Tom Norris and Meron Girma. Tom Norris wrote the first draft of the paper. All authors took responsibility for the interpretation of the data and edited and approved the final manuscript.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
Supporting information
Supporting information.
ACKNOWLEDGEMENTS
The authors acknowledge Jemal Haider, Ferew Lemma, Kaleab Baye, Pierre‐Luc Vanhaeverbeke and Atkure Defar for their contribution during the development of the causal diagrams. Financial support for the National Information Platforms for Nutrition (NIPN), Ethiopia, is provided by the European Union Delegation for Ethiopia, the Foreign, Commonwealth and Development Office and the Bill and Melinda Gates Foundation.
Norris, T. , Girma, M. , Genye, T. , Hussen, A. , Pradeilles, R. , Bekele, Z. , van Zyl, C. , & Samuel, A. (2024). Predictors of prediabetes/diabetes and hypertension in Ethiopia: Reanalysis of the 2015 NCD STEPS survey using causal path diagrams. Maternal & Child Nutrition, 20(S5), e13365. 10.1111/mcn.13365
Tom Norris and Meron Girma are the joint first authors.
DATA AVAILABILITY STATEMENT
The data sets for most NCD STEPwise surveys are publicly available and can be obtained from the NCD Microdata Repository (https://extranet.who.int/ncdsmicrodata/index.php/home).
REFERENCES
- Addo, J. , Smeeth, L. , & Leon, D. (2007). Hypertension in sub‐Saharan Africa: A systematic review. Hypertension, 50(6), 1012–1018. 10.1161/HYPERTENSIONAHA.107.093336 [DOI] [PubMed] [Google Scholar]
- Allen, L. , Cobiac, L. , & Townsend, L. (2017). Quantifying the global distribution of premature mortality from non‐communicable diseases. Journal of Public Health, 39(4), 698–703. 10.1093/PUBMED/FDX008 [DOI] [PubMed] [Google Scholar]
- American Diabetes Association . (2021). Diagnosis. https://www.diabetes.org/a1c/diagnosis
- Bishu, K. G. , Jenkins, C. , Yebyo, H. G. , Atsbha, M. , Wubayehu, T. , & Gebregziabher, M. (2019). Diabetes in Ethiopia: A systematic review of prevalence, risk factors, complications, and cost. Obesity Medicine, 15, 100132. 10.1016/J.OBMED.2019.100132 [DOI] [Google Scholar]
- Central Statistical Agency and ICF . (2016). Ethiopia demographic and health survey 2016. [Google Scholar]
- Central Statistical Authority [Ethiopia] and ORC Macro . (2001). Ethiopia demographic and health survey 2000. [Google Scholar]
- Choi, H. , Kim, H. , & Kang, D. (2017). Sex differences in hypertension prevalence and control: Analysis of the 2010‐2014 Korea National Health and Nutrition Examination Survey. PLoS One, 12(5):e0178334. 10.1371/JOURNAL.PONE.0178334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dereje, N. , Earsido, A. , Temam, L. , & Abebe, A. (2020). Uncovering the high burden of hypertension and its predictors among adult population in Hosanna town, southern Ethiopia: A community‐based cross‐sectional study. BMJ Open, 10(10), e035823. 10.1136/BMJOPEN-2019-035823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Endris, T. , Worede, A. , & Asmelash, D. (2019). Prevalence of diabetes mellitus, prediabetes and its associated factors in Dessie Town, Northeast Ethiopia: A community‐based study. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 12, 2799–2809. 10.2147/DMSO.S225854 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ethiopian Public Health Institute, Federal Ministry of Health and World Health Organization . (2016). Ethiopia STEPS report on risk factors for non‐communicable diseases and prevalence of selected NCDs. [Google Scholar]
- Everett, B. , & Zajacova, A. (2015). Gender differences in hypertension and hypertension awareness among young adults. Biodemography and Social Biology, 61(1), 1–17. 10.1080/19485565.2014.929488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Federal Democratic Republic of Ethiopia: Ministry of Health . (2014). National Strategic Action Plan (NSAP) for prevention and control of non‐communicable diseases. [Google Scholar]
- Gebreyes, Y. , Goshu, D. , Geletew, T. , Argefa, T. , Zemedu, T. , Lemu, K. , & Belayneh, A. (2018). Prevalence of high bloodpressure, hyperglycemia, dyslipidemia, metabolic syndrome and their determinants in Ethiopia: Evidences from the National NCDs STEPS Survey, 2015. PLoS One, 13(5):e0194819. 10.1371/JOURNAL.PONE.0194819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghosh, S. , Mukhopadhyay, S. , & Barik, A. (2016). Sex differences in the risk profile of hypertension: a cross‐sectional study. BMJ Open, 6(7):e010085. 10.1136/BMJOPEN-2015-010085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- He, Y. , Chiang, C. , Gebremariam, L. W. , Hirakawa, Y. , Yatsuya, H. , & Aoyama, A. (2020). Factors associated with prediabetes and diabetes among public employees in Northern Ethiopia. Asia‐Pacific Journal of Public Health, 33(2–3), 242–250. 10.1177/1010539520974848 [DOI] [PubMed] [Google Scholar]
- Hostalek, U. (2019). Global epidemiology of prediabetes—present and future perspectives. Clinical Diabetes and Endocrinology, 5(1), 5. 10.1186/S40842-019-0080-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Institute for Health Metrics and Evaluation . (2019). GBD compare | Viz hub. Retrieved April 14, 2021, from https://vizhub.healthdata.org/gbd‐compare/
- International Expert Committee on Diabetes . (2009). International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care, 32, 1327–1334. 10.2337/dc09-9033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Diabetes Federation . (2019). IDF Diabetes Atlas, 9th edition. https://www.diabetesatlas.org/upload/resources/material/20191218_144539_afr_factsheet_en.pdf
- Kautzky‐Willer, A. , Harreiter, J. , & Pacini, G. (2016). Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocrine Reviews, 37(3), 278. 10.1210/ER.2015-1137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kibret, K. T. , & Mesfin, Y. M. (2015). Prevalence of hypertension in Ethiopia: A systematic meta‐analysis. Public Health Reviews, 36(1), 1–12. 10.1186/S40985-015-0014-Z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kish, L. (1949). A procedure for objective respondent selection within the household. Journal of the American Statistical Association, 44(247), 380–387. 10.1080/01621459.1949.10483314 [DOI] [Google Scholar]
- Lin, X. , Xu, Y. , Pan, X. , Xu, J. , Ding, Y. , Sun, X. , Song, X. , Ren, Y. , & Shan, P. F. (2020). Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Scientific Reports, 10(1), 1–11. 10.1038/s41598-020-71908-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKenzie, B. L. , Santos, J. A. , Geldsetzer, P. , Davies, J. , Manne‐Goehler, J. , Gurung, M. S. , & Webster, J. (2020). Evaluation of sex differences in dietary behaviours and their relationship with cardiovascular risk factors: a cross‐sectional study of nationally representative surveys in seven low‐ and middle‐income countries. Nutrition Journal, 19(1), 1–15. 10.1186/S12937-019-0517-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meisinger, C. , Thorand, B. , Schneider, A. , Stieber, J. , Döring, A. , & Löwel, H. (2002). Sex differences in risk factors for incident type 2 diabetes mellitus: The MONICA Augsburg Cohort Study. Archives of Internal Medicine, 162(1), 82–89. 10.1001/ARCHINTE.162.1.82 [DOI] [PubMed] [Google Scholar]
- Misganaw, A. , Mariam, D. H. , Ali, A. , & Araya, T. (2014). Epidemiology of major non‐communicable diseases in Ethiopia: A systematic review. Journal of Health, Population, and Nutrition, 32(1), 1–13. [PMC free article] [PubMed] [Google Scholar]
- Mostafa, T. , & Wiggins, R. D. (2015). The impact of attrition and non‐response in birth cohort studies: A need to incorporate missingness strategies. Longitudinal and Life Course Studies, 6(2), 131–146. 10.14301/llcs.v6i2.312 [DOI] [Google Scholar]
- Njølstad, I. , Arnesen, E. , & Lund‐Larsen, P. G. (1998). Sex differences in risk factors for clinical diabetes mellitus in a general population: a 12‐year follow‐up of the Finnmark Study. American Journal of Epidemiology, 147(1), 49–58. 10.1093/OXFORDJOURNALS.AJE.A009366 [DOI] [PubMed] [Google Scholar]
- Sanfo, J.‐B. M. B. , & Ogawa, K. (2021). Explaining the rural‐urban learning achievements gap in Ethiopian primary education: A re‐centered influence function decomposition using Young Lives data. Education Economics, 29(3), 269–297. 10.1080/09645292.2021.1872504 [DOI] [Google Scholar]
- Stafford, M. , Black, S. , Shah, I. , Hardy, R. , Pierce, M. , Richards, M. , Wong, A. , & Kuh, D. (2013). Using a birth cohort to study ageing: representativeness and response rates in the National Survey of Health and Development. European Journal of Ageing, 10(2), 145–157. 10.1007/s10433-013-0258-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tesfaye, F. , Byass, P. , & Wall, S. (2009). Population based prevalence of high blood pressure among adults in Addis Ababa: Uncovering a silent epidemic. BMC Cardiovascular Disorders, 9(1), 1–10. 10.1186/1471-2261-9-39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Textor, J. , van der Zander, B. , Gilthorpe, M. S. , Liskiewicz, M. , & Ellison, G. T. H. (2016). Robust causal inference using directed acyclic graphs: The R package “dagitty”. International Journal of Epidemiology, 45(6), 1887–1894. 10.1093/IJE/DYW341 [DOI] [PubMed] [Google Scholar]
- Unger, T. , Borghi, C. , Charchar, F. , Khan, N. A. , Poulter, N. R. , Prabhakaran, D. , Ramirez, A. , Schlaich, M. , Stergiou, G. S. , Tomaszewski, M. , Wainford, R. D. , Williams, B. , & Schutte, A. E. (2020). 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension, 75(6), 1334–1357. 10.1161/HYPERTENSIONAHA.120.15026 [DOI] [PubMed] [Google Scholar]
- United Nations . (n.d.). Transforming our world: The 2030 Agenda for Sustainable Development|Department of Economic and Social Affairs. Retrieved October 22, 2021, from https://sdgs.un.org/2030agenda
- Woldegebriel, A. G. , Fenta, K. A. , Aregay, A. B. , Aregay, A. D. , Mamo, N. B. , Wubayehu, T. W. , Bayray, A. , & Mulugeta, A. (2020). Effectiveness of anthropometric measurements for identifying diabetes and prediabetes among civil servants in a Regional City of Northern Ethiopia: A cross‐sectional study. Journal of Nutrition and Metabolism, 2020, 8425912. 10.1155/2020/8425912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Worku, I. H. , Dereje, M. , Minten, B. , & Hirvonen, K. (2017). Diet transformation in Africa: The case of Ethiopia. Agricultural Economics, 48(S1), 73–86. 10.1111/AGEC.12387 [DOI] [Google Scholar]
- World Health Organization . (2011). Use of glycated haemoglobin (HbA1c) in diagnosis of diabetes mellitus: Abbreviated report of a WHO consultation. https://apps.who.int/iris/bitstream/handle/10665/70523/WHO_NMH_CHP_CPM_11.1_eng.pdf [PubMed]
- World Health Organization . (2021a). Hypertension. Retrieved from www.who.int/news‐room/fact‐sheets/detail/hypertension
- World Health Organization . (2021b). STEPwise approach to NCD risk factor surveillance (STEPS). Retrieved October 22, 2021, from https://www.who.int/teams/noncommunicable‐diseases/surveillance/systems‐tools/steps
- World Health Organization & International Diabetes Federation . (2006). Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: Report of a WHO/IDF Consultation. https://www.who.int/diabetes/publications/Definition‐and‐diagnosis‐of‐diabetes_new.pdf
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Data Availability Statement
The data sets for most NCD STEPwise surveys are publicly available and can be obtained from the NCD Microdata Repository (https://extranet.who.int/ncdsmicrodata/index.php/home).