

Abstract
The objective of this article is to characterize the value of centralized iodization facilities (CIFs) to advance Ethiopia's salt iodization programme and its impact on the population iodine status. The analysis is based on a review of publications relating to salt iodization and iodine deficiency control efforts in Ethiopia. The country has made remarkable progress in improving iodized salt coverage, leading to improved iodine intake across its population that would otherwise be at high risk of iodine deficiency disorders. Establishment of central processing facilities, more frequent monitoring and generation of data and encouraging private sector investment have been instrumental in this achievement. Ethiopia has thus achieved and sustained greater than 89% HH iodized salt coverage from its lowest point of 15% coverage and subsequently improved iodine intake across its population. Iodine intake sufficiency in a population is assessed by median urinary iodine concentration (MUIC). The lessons learned and the experience with CIFs have applicability in several other countries where fragmented salt production continues to create barriers to achieve higher iodized salt coverage.
Keywords: Ethiopia, iodine deficiency disorders, iodine status, salt iodization
The objective of this article is to characterize the value of centralized iodization facilities (CIFs) to advance Ethiopia's salt iodization programme and its impact on the population iodine status. The analysis is based on a review of publications relating to salt iodization and iodine deficiency control efforts in Ethiopia. The country has made remarkable progress in improving iodized salt coverage, leading to improved iodine intake across its population that would otherwise be at high risk of iodine deficiency disorders.
Key messages
Iodized salt access in Ethiopia has improved remarkably and correlates with improved iodine nutrition among the population.
The establishment of centralized iodization facilities (CIFs) have been instrumental in improving iodized salt coverage and access.
Development partner support and Government commitment and efforts on enforcement have created the right enabling environment to attract investments in salt processing.
1. INTRODUCTION
Iodine is an essential component of the hormones produced by the thyroid gland. Thyroid hormones, and therefore iodine, are essential for mammalian life. Most iodine (as iodide) is found in the oceans (≈50 μg/L), and iodide ions in seawater are oxidized to elemental iodine, which volatilizes into the atmosphere and is returned to the soil by rain, completing the cycle. However, iodine cycling in many regions is slow and incomplete, leaving soil and ground water deficient in iodine. Crops grown in these soils will be low in iodine, and humans and animals consuming food grown in these soils will become iodine deficient (World Health Organization/International Council for the Control of Iodine Deficiency/UNICEF (WHO/ICCIDD/UNICEF), 2007). Iodine deficient soils are most common in inland regions, mountainous areas and areas of frequent flooding, but can also occur in coastal regions. The topography of Ethiopia is mountainous, and the top layer of soil has been eroded for decades, leading to leaching away of nutrients including iodine‐making iodine deficiency disorders (IDD) endemic throughout the country (Businge et al., 2021).
Lack of iodine can cause endemic goitre, hypothyroidism, cretinism, decreased fertility rate, increased infant mortality and mental retardation. Salt iodization has been introduced in many countries around the world as a sustainable strategy to improve the population level iodine intake and prevent IDD. Ethiopia adopted this approach and launched its universal iodized salt (USI) programme in the 1990s. The Ethiopian Government was a signatory to the World Summit for Children held in 1990 and banned the production and sale of noniodized salt in 1996 (Chuko et al., 2015). Before the 1998–2000 Ethiopian–Eritrean conflict, nearly all edible salt in Ethiopia was produced in large, industrial‐scale plants in Eritrea along the Red Sea. Consolidated production and processing of salt across relatively sophisticated refineries enabled quick adoption of iodization policy and coverage of iodized salt of over 80% was achieved within 2 years (Adish et al., 2013). The 1998–2000 Ethiopian–Eritrean war interrupted Ethiopia's salt supply from Eritrea, as a result, Ethiopia started importing salt from neighbouring countries, particularly Djibouti. Seeking to avoid dependence on importation, the Ethiopian government explored domestic sources of salt. Although a small amount of salt is available in underground water in Dobi (Tigray) and from rock deposits in Godcusbo (Somali) regions, the largest potential for salt production in Ethiopia is at Lake Adfdera (Afar Region) that now produces and distributes over 70% of the total salt requirement. More so, the Ethiopian Government decided to lift the ban on noniodized salt to ease the pressure on salt scarcity caused by the conflict between 1998 and 2000.
Consequently, between 2000 and 2011, iodized salt coverage in Ethiopia began to fall. According to the Demographic Health Surveys (Ethiopia Public Health Institute (EPHI); ICF, 2000, 2005, 2011), the national average of households with iodized salt (HHIS) in 2000 was 28.4% (range 12%–47%), in 2005 was 54.3% (41%–92%) and by 2011 it has reached its lowest point of 15.4% (8%–40%). Correspondingly, the iodine status of the population assessed through median urinary iodine concentration (MUIC) across several National and subnational surveys of women of reproductive age (WRA), pregnant women (PW) and school age children (SAC) between 2009 and 2015 demonstrated alarming iodine insufficiency. MUIC is an accepted indicator to assess the sufficiency of population iodine intake. The trends in MUIC values compared against household iodized salt coverage are presented in Table 1 and Figure 1. A strong correlation is observed between MUIC and HHIS between 2009 and 2021.
Table 1.
Summary of national and subnational iodine status surveys conducted in Ethiopia between 2009 and 2021
| Authors | Location | Year of the study | Women of reproductive age (WRA) and pregnant women (PW) | School children (SAC) |
|---|---|---|---|---|
| MUIC (μg/L) | ||||
| Elias et al. (2021) | Sidama Zone, SNNPR Region, Southern Ethiopia | 2009 | 37.2 (WRA) | |
| Ersino et al. (2013) | Sidama Zone, SNNPR Region, Southern Ethiopia | 2009 | 15 (PW) | |
| Girma et al. (2021) | Sidama Zone, SNNPR Region, Southern Ethiopia | 2009 | 34.2 (SAC) | |
| Negeri et al. (2014) | Jimma Zone, Oromia Region, Southwest Ethiopia | 2011 | 48 (PW) | |
| Mezgebu et al. (2021) | Jimma Zone, Oromia Region, Southwest Ethiopia | 2011 | 56.4 (SAC) | |
| Kibatu et al. (2014) | Metekel Zone, Benishangul‐Gumuz Region, Northwest Ethiopia | 2012 | 39.9 (SAC) | |
| Haji et al. (2014) | East Haraghe Zone, Oromiya Region, Southwest Ethiopia | 2012 | 58.1 (PW) | |
| Keno et al. (2017) | West Welega Zone, Oromia Region, Southwest Ethiopia | 2014 | 88.6 (PW) | 70.5 (SAC) |
| Ethiopia Public Health Institute (EPHI), 2016—Ethiopianmicronutrient deficiencies survey | National survey | 2015 | 96.8 (WRA) | 104 (SAC) |
| Wassie et al. (2018) | Northwest Ethiopia | 2016 | 235 (SAC) | |
| Asfaw & Belachew, (2019) | Dawro Zone, SNNPR Region, Southwest Ethiopia | 2017 | 96.1 (SAC) | |
| Muktar et al. (2018) | West Hararghe Zone, Oromia Region, Southwest Ethiopia | 2017 | 146 (SAC) | |
| Ayalew et al. (2021) | South Wollo Zone, Amhara Region, Northern Ethiopia | 2019 | 158.5 (SAC) | |
Abbreviation: MUIC, median urinary iodine concentration.
Figure 1.
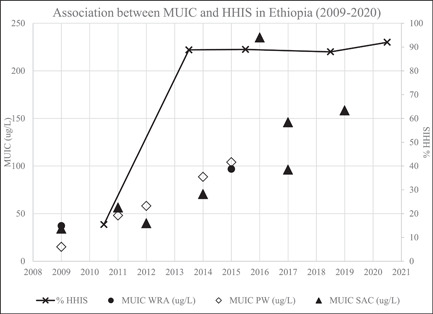
Association between median urinary iodine concentration (MUIC) and household iodized salt (HHIS) in Ethiopia
The 2005 Ethiopian National Iodine Deficiency Disorders survey exposed widespread iodine inadequacy among children and women measured through the prevalence of goitre and urinary iodine concentration (Abuye & Berhane, 2007). It was estimated that over 6 million (40%) children aged 6–12 years and four million (36%) women aged 15–49 years were affected by goitre. Furthermore, subclinical manifestations of IDD across the population were projected to be much higher with estimates of as many as three quarters of the population suffering from varying degrees of deficiency.
The data prompted the government to reassess its policy, which led to a renewed commitment and goal of achieving virtual elimination of IDD in 2005 (Girma et al., 2014). In early 2011, and after several years of promotion and advocacy, the Government of Ethiopia reintroduced a comprehensive legislation that mandated for all salt produced or imported into the country to be iodized by 2015 (Chuko et al., 2015; Wassie et al., 2018). While there are several challenges that need to be overcome, which are discussed within this paper, remarkable progress has been achieved where domestic salt supply is established to a point where Ethiopia does not need to rely on imports. Additionally, the aggregation of crude salt into central iodization facilities (CIFs) that facilitate consolidated processing and iodization is a prime contributing factor in the remarkable improvement in iodized salt coverage and access throughout the country. Very little information is documented or published on salt production and processing in Ethiopia, including CIF. This article, therefore, draws on a comprehensive study and mapping of salt production and processing undertaken by Segel Research & Training Consulting Plc and commissioned by UNICEF in 2021 to support the National Salt Iodization programme for the Government of Ethiopia.
The purpose of this article is to highlight the success Ethiopia has achieved and the key factors responsible, while discussing future directions for ensuring and sustaining optimum iodine nutrition. Salt production/producer in this article refers to crude salt or person or entity engaged in extracting salt in its natural state (usually from salt deposits or brines) while salt processing/processor refers to further treating or value‐addition (washing, refining, crushing, iodization, packaging) of salt for sale.
2. METHODS
2.1. Trends in key salt iodization programme indicators
The analysis is based on a comprehensive review of past and current publications relating to salt iodization and iodine deficiency control efforts in Ethiopia, including surveys, research papers, legislation, trade documents, policy statements, and national strategic plans. Data on key indicators from Demographic Health Surveys (Ethiopian Public Health Institute (EPHI); ICF, 2000, 2005, 2011, and 2016), National Micronutrient Surveys and other national or subnational published papers (Ethiopian Food and Drug Administration, UNICEF (2021); Ethiopian Public Health Institute, 2016) is characterized and analysed to present a trend analysis of critical changes in USI programme performance resulting from programmatic efforts including adjustments and refinements. For review of household coverage and iodine content in salt, iodization compliance was excluded where surveys used rapid test kits to estimate quantitative iodine levels in salt and these data are classified as salt being iodized at any level or not. Quantitative iodine values in household salt are presented for reports and papers that have utilized titration or other comparative assay methods.
2.2. Analysis of salt production and processing
This article draws information from the study commissioned by UNICEF in 2021 designed to collect data on salt production and processing from different sources: (1) secondary data, (2) field survey, and (3) geospatial sources. The existing iodized salt production sites were identified and mapped through recent period images of Google Earth. The study included interviews with key informants including salt processors and salt producers.
3. RESULTS
This article analyses the advancement of Ethiopia's salt iodization programme from the perspective of salt production, salt processing, and ultimately iodized salt coverage and iodine nutrition trends.
3.1. Salt production
Camel caravans have carried blocks of salt mined by hand from Ethiopia's Danakil Depression to markets since the sixth century, however, modern day salt production in Ethiopia is rapidly changing. A large factor in the rapid development of salt production capacity was driven by the scarcity and price increases in salt following the Ethiopian–Eritrean conflict in early 2000 that led to disruption in salt supply from the Assab region, Eritrea. Rock salt or 'Amole’ was still being mined in Ethiopia at the time, but this salt was mainly being used for animal salt licks and continues to be mined for that purpose. Ethiopia started developing its domestic salt production capacity in response to the shortage as well as to move away from reliance on imports. At present, Ethiopia's primary salt production is concentrated at three zones, Lake Afdera, Dobi and Godcusbo. The requirement of salt for human consumption for Ethiopia's population is estimated at around 500,000 metric tonnes based on its current population and accounts for about 4.5 kg of salt per capita requirement. This estimate includes salt used by the food industry. Additionally, salt is used by other industries for leather tanning and other industrial applications as well as animal feed. The data on Ethiopia's salt usage in nonhuman consumption are not available. However, a rough estimate would be that 80% of Ethiopia's salt production would be for human consumption in the absence of heavy chlor‐alkali industries. Irrespective, Ethiopia's salt production potential is much higher than its requirement and it is estimated that Lake Afdera alone has a potential for 2.5 million metric tonne per annum of salt (Adish et al., 2013).
Around 70%–80% of the salt produced in Ethiopia comes from Lake Afdera. Lake Afdera is a natural saline lake located in the Danakil Depression. The salinity of the lake's water, high ambient temperatures, dry‐arid climate, and flat topography along the south and south west corners of the lake create almost ideal conditions for salt production. Most salt production units in Lake Afdera employ a conventional triple stage solar evaporation technique. Brine from the saline lake is pumped through consecutive pans concentrating along the stages through solar evaporation. As the brine saturates, calcium carbonate and calcium sulphate (gypsum) precipitates after which the brine is pumped into the final crystallizer ponds where sodium chloride (salt) is harvested. The residual brine liquor is usually discharged carrying off magnesium salts. This technique produces high‐quality salt with high sodium chloride content. Smaller artisanal producers in Lake Afdera apply a single‐stage technique, pumping water straight into crystallizer pans and allowing the brine to completely evaporate, leaving a salt deposit which is harvested. The single‐stage technique is predominantly used in Dobi and Godcusbo salt production zones as well. Dobi is located near Lake Afdera within the Afar region while Godcusbo is in the Somali Region in the south eastern part of the country close to the border with Somalia. Dobi and Godcusbo produce salt from underground brine that is mechanically pumped or at times manually raised through pulleys and buckets from wells. The production methods in Dobi and Godcusbo are relatively primitive and artisanal resulting in low yields of inferior quality salt. These regions account for less than 30% of Ethiopia's salt production.
3.2. Salt iodization
Between 2000 and 2011, most of the salt iodization efforts targeted iodization of salt at the primary production level. The primary method for salt iodization was to dissolve potassium iodate in water and spray the solution onto salt. Since the approach was to iodize salt at the point of production which at the time was dominated by small operations located in areas with poor infrastructure, manual knapsack sprayers were used. This potassium iodate was sprayed directly onto mounds of salt, manually mixed and subsequently packaged. There were attempts to mechanize this process to achieve better mixing and consistent iodization and several development partners provided mobile iodization machines. While these machines aided mixing and packaging of salt, they required additional labour to feed salt into the machines. These iodization machines were not suited for the environment and the prevailing infrastructure. Most of these machines have been abandoned, went into disrepair or broke down. Earlier iodization programmes also included training of salt producers and provision of potassium iodate and while small improvements were achieved, the efforts could not be sustained.
3.3. Introduction of CIFs in Ethiopia
Between 2011 and 2015, the programmatic approach to salt iodization changed, CIFs were considered. It was clear that iodization of salt at the primary production sites was not feasible and therefore the approach evolved to aggregating salt produced by smaller processors into central processing locations that would enable iodization, and this would also make monitoring of quality easier and enable more consistent iodization. Primary salt producers and traders had to be convinced to sell their salt to these central processing units instead of directly into the market. At the same time investors had to be identified who were willing to offtake the salt from producers and process and distribute this to consumers. Suspicion and doubt prevailed; however, these were eventually overcome through dialogue, assurances and producers eventually seeing the benefit of a consistent market.
The location of CIFs must be strategically done with due consideration for the infrastructure, proximity to salt sources and markets and available road and utility infrastructure. Thus, 17 CIFs have been established in Ethiopia, 13 (76%) are located across three regions—Amhara, Afar and Tigray. Most of the CIFs have a recent history where 12 (70%) of them were established in the last 5 years. The oldest one was established 20 years ago. Only 12 out of the 17 CIFs are operational and the cumulative installed processing capacity of the CIFs is approaching 2 million metric tonnes although on aggregate less than 25% of this capacity is utilized given the salt requirement for Ethiopia. The installed processing capacity of the CIFs is presented in Table 2. Figure 2 provides an overview of the three main salt production zones—Lake Afdera, Dobi, and Godcusbo and 12 out of the 17 registered CIFs.
Table 2.
Registered salt processing companies (CIFs) in Ethiopia (as of 2021)
| Salt processor | Year Est. | Type of business | Installed capacity MT/annum | Actual est. production MT/annum | |
|---|---|---|---|---|---|
| Afder Walalaha Salt Production Plc | 2001 | Private limited | 112,500 | 20,000 | 4% |
| Ashale Salt | 2002 | Share company | 15,000 | 0 | 0% |
| Shewit Salt | 2002 | Private limited | 5000 | 0 | 0% |
| Guts Agro Industry Plc | 2010 | Private limited | 12,500 | 0 | 0% |
| Mesob Salt | 2012 | Sole proprietorship | 30,000 | 0 | 0% |
| Desta Alena Iodized Salt Producer | 2016 | Sole proprietorship | 21,500 | 5000 | 1% |
| SVS Plc | 2017 | Joint venture | 540,000 | 150,000 | 28% |
| Best Iodized Salt Factory (BIS) | 2018 | Sole proprietorship | 18,000 | 5000 | 1% |
| MTI Iodized Salt Plc | 2019 | Private limited | 20,000 | 5000 | 1% |
| Ella Trading Plc | 2020 | Private limited | 11,250 | 0 | 0% |
| SOM Iodized Salt | 2020 | Sole proprietorship | 1500 | 0 | 0% |
| Ekram Amiru Iodized Salt Producer | 2020 | Sole proprietorship | 3750 | 1500 | 0% |
| TTR Iodized Salt | 2020 | Joint venture | 725,000 | 150,000 | 28% |
| Danakil Ethiopia Plc | 2020 | Private limited | 300,000 | 180,000 | 34% |
| Family Iodized Salt | 2020 | Cooperative | 2500 | 0 | 0% |
| Green Star Trading Plc | 2020 | Private limited | 30,000 | 0 | 0% |
| Sadaking Salt Processing & Production | 2020 | Private limited | 36,000 | 10,000 | 2% |
| Total | 1,884,500 | 526,500 | 100% | ||
Figure 2.
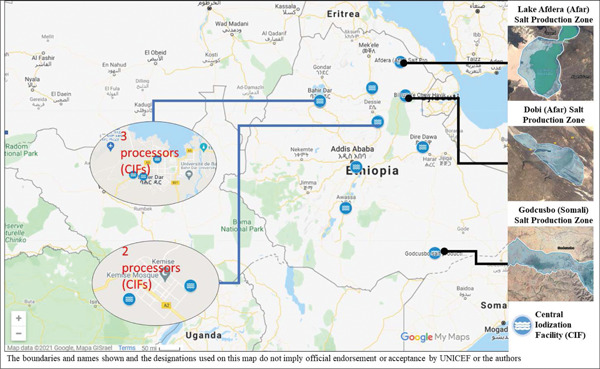
Location of Ethiopia's main salt production zones and processing facilities (central iodization facilities [CIFs])
Out of the 17 registered CIFs, 8 processing facilities did not report any production in 2020–2021. Three companies SVS, TTR and Danakil Plc reported production that accounted for almost 90% of Ethiopia's salt requirement. The reported actual production is not validated, and the survey commissioned by UNICEF relied on reported figures from the companies. The installed capacity of processing facilities exceeds the market for salt for human consumption resulting in underutilization of installed capacity which on average is below 30%. Given that salt use in industrial applications is less than 20% of the overall salt demand in Ethiopia, the underutilization of the processing capacity of CIFs pose business sustainability challenges and carries a risk of a few companies going out of business unless new markets such as exports are created for salt. An investment analysis for one of the major salt companies is presented in Box 1. This investment analysis applies to all CIFs and is thus intended to be an example. The processing companies dominating the market are either joint ventures or private limited companies and this is a testament to an effective business model for Ethiopia that combines local business acumen that leverages access to capital and finance.
Box 1. SVS example of well‐functioning CIFs over the last years.
SVS is an ‘iodized salt plant’ jointly built by Ethiopian and Turkish investors in August 2019 near the city of Semera, Afar region of Ethiopia. SVS salt plant, which cost around US$10 million, has a capacity of producing 540,000MT of iodized salt per year. The plant employs 463 permanent and 300 temporary workers. About 60% of the construction cost of the SVS salt plant was covered by Ethiopian investors while Turkish investors contributed the rest. The company procures unwashed raw salt to produce both noniodized (washed) and iodized salt from its two main sources: Lake Afdera and Dobi. SVS sources potassium iodate locally from the Drug Fund Institute with the permission of the Ministry of Health by check and balance method. The criteria to acquire potassium iodate are the production capacity, input and output ratio, legal license, and the iodized salt supply to the market. SVS is one of the largest clients for raw salt supply in the country.
The establishment of CIFs, establishment of iodization capacity and actual production and corresponding trends on household coverage of iodized salt is presented in Figure 3. We can observe from the graph that the first attempts at creation of CIFs did not have much impact on HHIS coverage. With a renewed approach and strategy, we can see that the cumulative installed capacity increased to meet the iodized salt requirement between 2016 to 2020 and correspondingly HHIS coverage has improved. This shows that the renewed CIF approach was more effective. Currently, the combined installed processing capacity exceeds the iodized salt requirement and therefore much of the installed processing capacity is not utilized which is also tabulated in Table 2 which also explains the parity between installed capacity and actual production.
Figure 3.
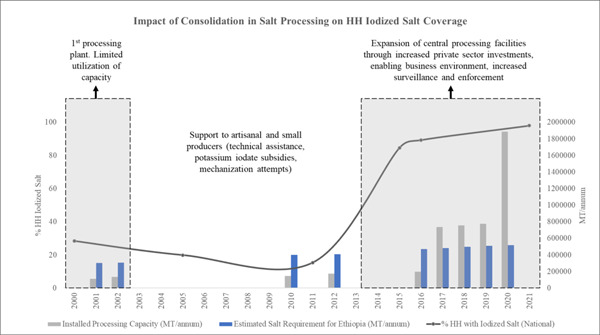
Trends in iodized salt coverage salt requirements and processing capacity
3.4. Iodized salt coverage trends
Overall, the proportion of households using iodized salt which was only 28% in 2000, and further fell to as low as 15% by 2011. Household coverage for iodized salt increased to 89% by 2016 (Ethiopia Public Health Institute (EPHI); ICF, 2016) and has remained steady as confirmed by the latest post market surveillance conducted by the Ethiopian Food and Drug Administration (EFDA) in 2021 (Figure 1). Furthermore, the post market surveillance conducted by the EFDA in 2021 which included quantitative analysis of iodine reported that iodine content of salt reported that 92% of salt samples collected from markets contained over 20 ppm I with the lowest coverage in Amhara Region where 13% of salt samples has iodine levels below 20 ppm I. In the same survey, nationally only about 1% of salt samples did not contain any iodine (<5 ppm). These data represent a dramatic progress for the salt iodization programme in Ethiopia.
3.5. Iodine intake trends
Clearly, improvements in iodized salt coverage have contributed to improved iodine intake. There is a positive trend in iodine intake, as reflected by the MUIC of the population since 2009 documented through various national and subnational studies which are presented in Table 1. According to WHO Guidelines (World Health Organization/International Council for the Control of Iodine Deficiency/UNICEF (WHO/ICCIDD/UNICEF), 2007) MUIC among school age children below 100 μg/L or WRA below 150 μg/L is indicative of iodine sufficiency. Low levels can be interpreted as iodine insufficiency given that pregnant women would have a higher requirement for iodine. The studies indicate a clear shift in iodine intake with a distinct rise in MUIC values between 2015 across all population subgroups which coincides with improved household coverage during the same period. This suggests that HHIS coverage and MUIC values correspond well in Ethiopia.
4. DISCUSSION
Reviewing trends in salt production, salt processing, household iodized salt coverage and ultimately iodine intake reveals important findings. First, salt production in Ethiopia has increased to a point where the country is self‐sufficient. While this production has improved, some aspects of salt production remain challenging, and the sector is still relatively fragmented and undermined by political, economic and social challenges which will need to be resolved. These include:
-
1.
Harsh climatic conditions, remoteness and lack of infrastructure in the Afar region that makes salt production operationally challenging and it is costly to get this salt to the central processing facilities and eventually into the market.
-
2.
The Afdera region continues to experience conflict and persistent political friction between the Regional and Federal Government which manifests into poor adoption of socioeconomic policies.
-
3.
Price controls and production quotas to protect the livelihoods of small‐scale salt producers frequently conflict with business dynamics and discourage investment into the salt sector and pose high business risk.
-
4.
The fragmented nature and small size of salt works restricts the potential for mechanization and adoption of modern salt production techniques.
-
5.
Surplus production and lack of markets for both food grade and industrial salt in the absence of export potential due to comparatively high production costs has led to a high turnover in salt production operations with many ceasing to operate.
Irrespective of these challenges, the Ethiopian Government has been successful with its vision to exploit the country's potential for salt production and establish independence from imports.
With salt production established, the next challenge for Ethiopia was to achieve salt iodization. Between 2000 and 2010, the thrust of the salt iodization programme was to iodize salt at the primary production level, and this did not yield big improvements and the small gains were difficult to sustain. Salt iodization largely flatlined over this period. At the nascent stages of the salt iodization programme, primary iodized salt production was dominated by small‐scale players that could not be regulated. In addition, earlier thrusts to support salt iodization through provision of subsidized potassium iodate, provision of equipment to mechanize salt iodization by small producers was counterproductive and not cost‐efficient. Salt iodization machines were placed and located at nonstrategic points and many went into a state of disrepair or nonuse. The Afari salt producers perceived support toward salt iodization as tactic to exclude them from participating in the salt economy due to their limited access to capital and the salt iodization programmed stalled for several years. The initial efforts in the early 2000 to establish CIF did not sufficiently engage the salt producers in negotiating terms for the sale of their salt to the CIF. There was mistrust and perceptions carried by salt producers who felt the profits from the distribution of salt disproportionately benefitted the CIF as there was a lack of appreciation for cost of processing and associated yield loss.
A new approach to CIFs in the last 5–7 years has proven to be the breakthrough in improving iodization levels. A marked inflection point was observed between 2010 and 2015 where iodized salt coverage began to increase rapidly, and this is primarily attributed to CIFs. The contributing factors include:
-
1.
An enabling environment attracted private sector investment into salt processing and establishment of CIF was viewed as a lucrative business.
-
2.
The Ethiopian Government started applying more sanctions around the sale of noniodized salt. This encouraged investors to establish iodization facilities while discouraging the commercialization of weakly iodized and of inappropriate quality salt for human consumption, and which is produced by small producers and traders.
-
3.
The Afar Regional Government, which was initially fearful of salt iodization facilities, began to see these facilities as up‐takers for the salt produced by the Afari as opposed to a threat. Salt processing facilities supported by private sector investments were also able to negotiate and address the fears of primary salt producers. Salt processing facilities not opting to disrupt or foray into primary salt production enabled a more symbiotic relationship.
-
4.
Government and development partners sustained support and invested in data that strengthened advocacy efforts and better programme implementation.
Increased engagement with private investors has resulted in a better relationship between salt producers and processors. Primary salt producers have benefitted from secure markets for crude salt, while salt processors (through these CIFS) take this salt, refine, iodize, package and distribute it more effectively around the country. There is greater shared value between producers and processors and the consumer benefits from access to better quality salt. Another critical lesson is that Ethiopia has successfully navigated around ensuring the livelihoods of small‐scale salt producers are not threatened and there is a symbiotic relationship between salt producers and processors that ultimately benefits all participants in the salt value chain.
The DHS data show HHIS coverage at 28.4% in 2000, rising to 54.3% in 2005 and dropping back to 15.4% in 2011. The progress between 2011 and 2015 has been remarkable with iodization levels improving significantly. The 2016 DHS reported HHIS coverage at 89%. There were concerns whether this coverage could be sustained, especially since earlier efforts with salt iodization has resulted in an uptick but not maintained. These concerns stem from some risks and critical bottlenecks in the production and processing of salt which are summarized in Table 3. More recent data alleviate some concerns since the 2021 post market surveillance (Ethiopia Food and Drug Admnistration, UNICEF, 2021) undertaken by the Ethiopia Food and Drug Authority found 92% HHIS coverage.
Table 3.
Challenges to salt production and processing in Ethiopia
| Salt producers | Salt processors (CIFs) | |
|---|---|---|
| Policy |
|
|
| Environment |
|
|
| Operations |
|
|
The spatial orientation of CIFs in relation to the main salt production areas and major transport arteries is presented in Figure 2. Strategic positioning of CIFs to optimize the feasibility of aggregating salt from salt production zones takes into consideration where the major markets and infrastructure (such as roads and electricity) are located, is one of the main factors that has led to the success of CIFs. Another important factor has been the approach of the Government to create the opportunity and enabling an environment for private sector investment which attracts valuable capital influx and improves sustainability. In contrast, earlier efforts to establish CIFs were primarily Government or Donor funded and located in areas where the necessary infrastructure (roads and electricity) conditions were not favourable. Fewer processing facilities (CIFs) have also made it easier for the Government to monitor and regulate salt iodization which is a critical incentive to sustain iodization. This has also eased the complexity of distribution and access to potassium iodate. In the earlier period of re‐establishing salt iodization, development partners had supported the Government with free potassium iodate which had to be distributed to hundreds of small producers and the associated attempts at establishing the revolving fund were difficult to sustain. While the Government currently manages importation of potassium iodate and sells this through the revolving fund to CIFs, a consideration for the future may be to address these importation and foreign exchange restrictions as well as reduction or elimination of levies and duties. Such measures would create a greater incentive for salt processors to import potassium iodate directly.
As presented in Table 2, three companies, SVS Plc, TTR Iodized Salt and Denakil Plc account for 90% of the iodized salt supply. The other 14 registered CIFs are either dormant or producing very little. Underutilized production capacity poses a major business risk for these CIFs and even the three companies that are dominating have significant latent production capacity. This unfavourably affects the cost of production and will naturally force CIFs that cannot create competitive advantage to go out of business. Investors should therefore be cautioned to undertake extensive due diligence and have strong business plans before establishing new CIFs. Creating new markets for Ethiopia's salt industry particularly for exports could be a potential way to improve capacity utilization. This will require further transformation across the salt supply chain from production to distribution so that the Ethiopia's salt can compete with global market prices. Ethiopia is a landlocked country and already at a disadvantage. The country has tremendous raw salt potential, both rock salt and saline lakes. Accelerated growth in the salt sector and salt market is more likely to be achieved by promoting and growing the demand for industrial salt for the chlor‐alkali industry including fertilizer production which would be helpful for Ethiopia's predominantly agriculture‐based economy. In the absence of precise figures, it is estimated that 80% of Ethiopia's salt is for human consumption, both directly as household or kitchen salt and salt used by the food industry, while 20% is used for animal feed, leather tanning and other industrial applications. In comparison countries with highly developed salt sectors only use about 10% for human consumption.
Table 3 outlines some of the challenges in salt production and salt processing in Ethiopia. The salt iodization progress is encouraging and to be celebrated although the country has much more potential to develop and grow its salt industry and with the right policies, enabling environment and support this can be achieved.
Several countries within the African continent such as Ghana and Senegal, and outside of the continent such as Philippines, Cambodia, Indonesia face similar challenges with improving salt iodization coverage. The lessons learned from Ethiopia's CIF model could be invaluable for other countries to adopt. These experiences and lessons therefore need to be studied and experiences widely disseminated so that they can benefit other salt iodization programmes.
5. CONCLUSION
Consolidation within the salt processing sector is clearly contributing to improved household access and coverage of iodized salt. As a result, iodine nutrition is also improving. However, a few challenges remain that need to be addressed to ensure sustainability of the salt iodization programme and protect the population from iodine deficiency.
-
1.
Ethiopia must prioritize a national assessment of population iodine status. Ethiopia's coverage has shifted but most recent data on population iodine status is not comprehensive. A national assessment would also identify subnational disparities in either insufficient or excessive iodine intake and enable programmatic actions that can ensure equitable protection from IDD.
-
2.
Salt production in Ethiopia remains fragmented and this sector needs to be uplifted to support centralized salt processing. Access to finance, land ownership, regulations and mining of salt, as well as issuance of salt licences, quotas on salt production, and technical knowledge of salt producers need to be improved. The cost of salt produced in Ethiopia remains higher than global averages which makes the sector noncompetitive and restricts growth.
-
3.
The processing capacity for salt is severely underutilized and on average less than 30%. This will pose commercial sustainability challenges for investors in salt processing and poses a business risk and delays return on investment. Several processing facilities also operate from nonstrategic locations (poor infrastructure, access to market or supply of crude salt).
-
4.
Ethiopia must sustain enforcement initiatives since this creates an incentive for salt processors to maintain iodization. Policies around access to finance and simplifying access to potassium iodate can also improve the commercial feasibility of salt processors and consequently protect investments, driving further development of the sector. The quality of salt produced is determined by the quality of crude salt and therefore better coordination between salt producers and processors also needs to be created.
-
5.
Sustained commitment and enabling a business environment benefits all value chain actors and ultimately creates access to more affordable, higher quality products for the consumers including low‐income households.
-
6.
Where the free salt market competitive situation is not the norm as it is in Ethiopia, large investments in raising consumer awareness and demand for quality iodized salt may not be effective in empowering the consumer.
The experience with CIFs in Ethiopia has applicability in several countries that continue to struggle with achieving adequate iodized salt coverage to prevent iodine deficiency disorders. The lessons learned from Ethiopia are therefore useful for other countries and offer a potential pathway to success.
AUTHOR CONTRIBUTIONS
Rizwan Yusufali and Arnaud Laillou designed the scope of the paper. Rizwan Yusufali, Tesfaye Chuko, and Arnaud Laillou conducted the analysis. Rizwan Yusufali wrote the first draft of the paper, Denise Frohmann supported with initial edits and review of references, Arnaud Laillou and Tesfaye Chuko reviewed the manuscript. All authors have read and approved the final manuscript.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGMENT
The authors would like to acknowledge the assistance in preparation of this article from the UNICEF nutrition team in Ethiopia, as well as other colleagues and peers that have contributed to Ethiopia's salt iodization programme over the years. The achievements of the USI programme are ultimately an outcome of the collective investments made by development partners, donors, the Ethiopian Government, and the private sector.
Yusufali, R. , Frohmann, D. , Chuko, T. , & Laillou, A. (2024). The advancement of Ethiopia's salt iodization program—The success story of the central iodized facilities. Maternal & Child Nutrition, 20(S5), e13427. 10.1111/mcn.13427
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
- Abuye, C. , & Berhane, Y. (2007). The goitre rate, its association with reproductive failure, and the knowledge of iodine deficiency disorders (IDD) among women in Ethiopia: Cross‐section community based study. BMC Public Health, 7, 316. 10.1186/1471-2458-7-316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adish, A. , Chucko, T. , Abay, A. , Assey, V. , & Desta, T. (2013). Ethiopia: Breaking through with a new iodized salt law. IDD Newsl. https://www.ign.org/cm_data/idd_nov13_ethiopia.pdf [Google Scholar]
- Asfaw, A. , & Belachew, T. (2019). Magnitude of iodine deficiency disorder and associated factors in dawro zone, southwest Ethiopia: The hidden hunger. Research Square, 1, 1–20. 10.21203/rs.2.13721/v1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ayalew, B. S. , Hassen, S. L. , Marefiyaw, T. A. , Yesuf, M. S. , Abebe, D. D. , & Temesgen, M. M. (2021). Prevalence of urinary iodine concentration among school children: In Dessie city, Ethiopia. BMC Pediatrics, 21, 423. 10.1186/s12887-021-02887-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Businge, C. B. , Longo‐Mbenza, B. , & Kengne, A. P. (2021). Iodine nutrition status in Africa: Potentially high prevalence of iodine deficiency in pregnancy even in countries classified as iodine sufficient. Public Health Nutrition, 24(12), 3581–3586. 10.1017/s1368980020002384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chuko, T. , Bagriansky, J. , & Brown, A. T. (2015). Ethiopia's long road to USI. In IDD Newsletter (Ed.) (vol. 43). Iodine Global Network. https://www.ign.org/cm_data/IDD_may15_ethiopia.pdf
- Elias, E. , Tsegaye, W. , Stoecker, B. J. , & Gebreegziabher, T. (2021). Excessive intake of iodine and low prevalence of goiter in school age children five years after implementation of national salt iodization in shebedino woreda, Southern Ethiopia. BMC Public Health, 21, 165. 10.1186/s12889-021-10215-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ersino, G. , Tadele, H. , Bogale, A. , Abuye, C. , & Stoecker, B. J. (2013). Clinical assessment of goiter and low urinary iodine concentration depict presence of severe iodine deficiency in pregnant Ethiopian women: A cross‐sectional study in rural Sidama, Southern Ethiopia. Ethiopian Medical Journal, 51(2), 133–141. [PubMed] [Google Scholar]
- Ethiopian Food and Drug Administration, UNICEF . (2021). Salt iodization market assessment. Addis Abeba, Ethiopia.
- Ethiopian Public Health Institute (EPHI) . (2016). Ethiopia micronutrient deficiencies survey. Addis Abeba, Ethiopia.
- Ethiopian Public Health Institute (EPHI); ICF . (2000). Ethiopia Demographic and Health Survey 2000. Addis Ababa, Ethiopia and Claverton, Maryland, USA; Central Statistical Agency and ORC Macro.
- Ethiopian Public Health Institute (EPHI); ICF . (2005). Ethiopia Demographic and Health Survey 2005. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ORC Macro.
- Ethiopian Public Health Institute (EPHI); ICF . (2011). Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Claverton, Maryland, USA: Central Statistical Agency and ICF International.
- Ethiopian Public Health Institute (EPHI); ICF . (2016). Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia and Rockville, Maryland, USA: CSA and ICF.
- Girma, K. , Nibret, E. , & Gedefaw, M. (2014). The status of iodine nutrition and iodine deficiency disorders among school children in metekel zone, northwest Ethiopia. Ethiopian Journal of Health Sciences, 24(2), 109–116. 10.4314/ejhs.v24i2.2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girma, M. , Loha, E. , Bogale, A. , Teyikie, N. , Abuye, C. , & Stoecker, B. (2021). Iodine deficiency in primary school children and knowledge of iodine deficiency and iodized salt among caretakers in Hawassa Town: Southern Ethiopia. [online] Ajol.info. https://www.ajol.info/index.php/ejhd/article/view/83824
- Haji, K. , Berhane, Y. , & Worku, A. (2014). Subclinical iodine deficiency among pregnant women in Haramaya district, eastern Ethiopia: A community‐based study. Journal of Nutrition and Metabolism, 2014, 8. 10.1155/2014/878926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keno, T. , Ahrens, C. , Lauvai, J. , Kurabachew, H. , Biesalski, H. K. , & Scherbaum, V. (2017). Iodine status in pregnant women and school children of the Aira district in Ethiopia. NFS Journal. 7, 1–7. [Google Scholar]
- Kibatu, G. , Nibret, E. , & Gedefaw, M. (2014). The status of iodine nutrition and iodine deficiency disorders among school children in metekel zone, northwest Ethiopia. Ethiopian Journal of Health Sciences, 24(No. 2), 109. 10.4314/ejhs.v24i2.2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mezgebu, Y. , Mossie, A. , Rajesh, P. , & Beyene, G. (2021). Prevalence and serverity of Iodine deficiency disorder among children 6‐12 years of age in Shebe Senbo District, Jimma Zone, Southwest Ethiopia. [online] Ajol.info. https://www.ajol.info/index.php/ejhs/article/view/82978 [PMC free article] [PubMed]
- Muktar, M. , Roba, K. T. , Mengistie, B. , & Gebremichael, B. (2018). Iodine deficiency and its associated factors among primary school children in Anchar district, eastern Ethiopia. Pediatric Health, Medicine and Therapeutics, 9, 89–95. 10.2147/PHMT.S165933 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Negeri, Z. , Gobena, T. , Rajesh, P. , & Kassim, M. (2014). Determining the magnitude of iodine deficiency and its associated risk factors among pregnant women visiting Jimma university specialized hospital for antenatal care. World Journal of Medicine and Medical Science, 2, 1–16. [Google Scholar]
- Wassie, M. M. , Abebe, Z. , Tariku, A. , Gebeye, E. , Awoke, T. , Gete, A. A. , Yesuf, M. E. , Kebede, Y. , Biks, G. A. , & Zhou, S. J. (2018). Iodine status five years after the mandatory salt iodization legislation indicates above requirement: A cross sectional study in northwest Ethiopia. BMC Nutrition, 4, 52. 10.1186/s40795-018-0261-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization/International Council for the Control of the Iodine Deficiency Disorders/United Nations Childrens Fund (WHO/ICCIDD/UNICEF) . (2007). Assessment of the iodine deficiency disorders and monitoring their elimination. World Health Organization. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.