

Abstract
Ingrown toenails account for roughly 20% of all foot problems in primary care. It is most common in young men, with nail care habits and footwear being major contributors. Onychocryptosis is typically caused by self-treatment attempts to cure the condition in its early stages. Its clinical features are frequently confused with other osseous and soft tissue abnormalities. The goal of this study was to provide perspectives on the management of pain and inflammation in Onychocryptosis using an Ozoile-based hydrogel formulation in a semi-occlusive bandage for 14 days, while incorporating natural pharmacological solutions into established protocols. The primary outcomes measured were pain reduction on NRS and stadiation according to the Al Kline Classification. The reduction was statistically significant, with a mean decrease in VA S score from 10 to 4 (p <0.05), and Al Kline classification decreased by an average of 1.6 stages. 42% of patients recovered within the first 15 days of treatment, and 93% by the end of the scheduled treatment.
Key Words: : onychocryptosis, Ozoile, podiatry, pain, inflammation
Ingrown toenails account for approximately 20% of foot problems in primary care and occur most commonly in young men, while among adolescents and young adults, a higher susceptibility has been noticed in males compared to females, with a ratio of nearly 2:1.1
Although an ingrown toenail can occur at any age, this pathology is more commonly observed in the population between the ages of 10 and 30, as well as in older individuals.2 In approximately 80% of cases involving the foot, the ingrown toenail affects the big toe, and in over half of the patients, the damage involves the lateral skin fold;3 this hypothesis correlates with the fact that ingrown nails commonly form at the distal-lateral margin of the nail, which often bears the brunt of weight-bearing.4 Multiple risk factors for ingrown toenails have been reported including improper nail trimming technique, trichotillomania, trauma, history of nail surgery, constricting footwear, obesity, bone abnormalities, hyperhidrosis, and onychomycosis, most often there are multifactorial etiologies.5,6
Improper nail trimming technique is a well-known risk factor for ingrown toenails.7 While attempting to “round off” nail corners, patients may inadvertently create barbs and spicules. The compression can cause the distal nail bed to shrink and impede the re-growing nail. A spicule of the lateral or distal nail can anchor itself into the periungual tissue and penetrate deeply as the nail plate grows. Pain relief is often difficult to achieve because trimming the spicule necessitates cutting soft tissue as well. A vicious cycle of pain with unsuccessful attempts at relief often aggravates the condition.8 Trauma is also one of the most frequent risk factors.9
The constriction of the shoe and the weight borne more on a certain region of the foot, together with micro traumas perpetrated over time from different origins play a key role in the emergence of this condition. Nevertheless, certain systemic conditions can adversely affect this condition.
Obesity can potentially exacerbate onychocryptosis by contributing to greater soft tissue mass throughout the body, particularly in the lower extremities. This can mimic periungual hypertrophy and intensify constriction caused by footwear. Similarly, diabetes, as well as, thyroid, cardiac, and renal disorders can increase lower extremity edema mimicking the effect of obesity on the nail unit.9 Hyperhidrosis may contribute to the development of ingrowing toenails, as periungual skin integrity may be compromised via maceration. This is especially notable in adolescents in whom perspiration of the feet is more commonplace, increasing nail plate malleability and facilitating skin perforation.10 Finally, the lack of health education in the population may increase the risk of onychocryptosis for several reasons. Poor control of foot hygiene may lead to neglecting to cut toenails regularly or to do so properly, thus increasing the risk of onychocryptosis. The use of appropriate footwear can avoid continuous micro-trauma to the big toe. A key role is played by the lack of awareness of the signs of local inflammation, which may lead to not immediately recognizing the need for specialist support for this condition. Also, it is likely under-reported because patients are unlikely to seek medical care if they have mild symptoms.11 Its clinical presentation is often confused with several osseous and soft tissue abnormalities, some of which have great importance to a patient’s overall welfare.12
The management of onychocryptosis, both complex and non-complex, is a critical and evolving area as it involves not only the clinical aspects of the disease but also the management of intense pain and functional limitations in walking for those affected, regardless of age and lifestyle.
Inconsistent conservative treatment and non-indicated surgical treatment often result in complications and the recurrence of the disease.13 Nonsurgical treatments are typically used for mild to moderate ingrown nails, whereas surgical approaches are used in moderate and severe cases. Simple nonsurgical palliative measures include correcting inappropriate footwear, managing hyperhidrosis and onychomycosis, soaking the affected toe followed by applying a mid- to a high-potency topical steroid and placing wisps of cotton or dental floss under the ingrown lateral nail edge.13
Patients are often exposed to several important risk factors that contribute to the development of this condition, including trauma, poor health and social education, incorrect nail cutting, and systemic diseases. Health education on the nail component of the foot is often absent among patients and a better understanding of this concept could lead to better compliance and adherence to therapy, as well as a decrease in recurrences. Nail injuries, initially common sources of pain, can have a significant impact on the quality of life and limit the ability to move, as well as negatively affect the psychological state of patients.
Although conventional treatments have made extensive use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and invasive surgery, podiatric research has opened up new perspectives through collaboration with pharmaceutical companies specializing in natural products. In this context, natural products such as ozonated oils can offer new complementary therapies. In particular, Ozoile represents a significant innovation in the therapeutic landscape.14
Ozoile is a pool of molecules obtained through a patented process by reaction of a defined mixture of oxygen-ozone with the olefinic fatty acids bonds of extra virgin olive oil +OIL®.
The process leads to the formation of stable Ozonides. Recent studies have shown that Ozoile possesses anti-inflammatory, antimicrobial, and regenerative properties, without showing overt toxicity and with several advantages over corticosteroids such as mometasone.15 This makes it an innovative approach to treat inflammatory pathological manifestations.16
Its unique formulation based on stable ozonides could revolutionize the management of onychocryptosis, offering an alternative to NSAIDs with presumed minimal side effects due to their natural nature.17 This study aims to evaluate the efficacy of Ozoile in hydrogel and cream (barrier effect) forms in the treatment of various manifestations of onychocryptosis and its different clinical forms, including inflammatory and infectious complications, as well as the impact on local function and posture.
The main objective was to provide new insights into the management of pain and inflammation in Onychocryptosis through the use of a combination of above mentioned Ozoile-based formulations, integrating natural pharmacological solutions into existing treatment protocols. The research not only evaluated the efficacy of Ozoile in the treatment of this specific podiatric condition but also its impact on patients’ quality of life during and after podiatric treatment.
Materials and Methods
Study population
This study was designed as a multicenter retrospective study and was approved by the ethics committee of the KORE University of Enna (Italy) Prot. N. 7520 11/04/2024 for the stated and proposed purposes. Seventy-five participants were recruited from different Italian regions, of both sexes, aged between 30 and 65 years (median age=48.2 years, SD=2.60 years). The study’s inclusion and exclusion criteria were evaluated by a group of podiatrists under the supervision of a physician, who enrolled all participants and assessed their characteristics. The inclusion criteria were as follows: onychocryptosis in progress, BMI between 18.5 and 24.9, absence of motor or neurological deficits, a recent history of nail trauma, and no orthopedic injury, or vestibular damage. Before the beginning of the study, each participant received a full explanation of the study procedures and signed a written consent form to participate. Confidentiality of the responses was also assured.
Regarding exclusions criteria these encompassed individuals with the absence of previous nail or other pathologies that could influence the results of this work, Al Kline stage 1, severe lesions on the affected foot, pre-existing medical conditions potentially affecting treatment response, or any history of allergy to the ingredients in the formulations utilized, diabetes, obesity and cardiopathies. As for the assessment that was used to stage the severity of nail disease, the classification according to Al Kline was chosen. As you can see from the image at the end of this section, the idea for a simple classification was based primarily on the severity and presentation of initial clinical findings and it was useful to quickly document the severity of the condition.18
Ozoile hydrogel and barrier cream: efficacy and use of the formulations
The patient was selected and followed from the beginning to the end of the treatment with the primary objective of evaluating the efficacy of Ozoile® Stable Ozonides in hydrogel and barrier cream forms in the context of nail pathology between stage 2 and 5 on the Al Kline scale.
Ozoile® Stable Ozonides is a pool of molecules obtained through a patented process by reaction of a defined oxygen-ozone mixture with the olefinic fatty acid bonds of organic olive oil. The process leads to the formation of stable Ozonides.14,15 Ozoile exerts its therapeutic efficacy mainly through the modulation of key biochemical pathways related to inflammation and pain perception.9 At the molecular level, its structure enables the selective inhibition of key enzymes in the inflammatory cascade, in particular Cyclooxygenase (COX) and lipoxygenase. Furthermore, stable Ozonides have been shown to possess healing biological activities.16
Measurement and treatment
After establishing a thorough medical, podiatric, and pharmacological history of the participants, they were clinically assessed and a form was created for each of them. The data entered included gender and age, motor activity performed (minimum 1 hour per week), BMI, staging of perceived pain level on the NRS scale, and current Al Kline classification (Figure 1). Subsequently, the lesion was cleansed and Ozoile Hydrogel was applied with a semi-occlusive dressing.
About topical therapy, after the application of the hydrogel, a semi-occlusive bandage was applied to the nail portion affected by Onychocryptosis with a gauze bandage, facilitating the absorption of the active ingredient while protecting the part from further trauma and/or external contamination. The patient played a key role in the treatment as he/she was educated on how to make this simple bandage so that he/she could change it independently every 24 hours by reapplying the hydrogel solution. After 7 days, the same procedure was repeated using Ozoile-barrier cream instead of hydrogel form, updating the patient’s file, and, where necessary, intervening with partial spiculectomy. As for the podiatric surgical approach using partial spiculectomy, this was only carried out if indicated according to the classification taken as reference for this work and never before treatment with hydrogel for at least 7 days, to reduce inflammation and pain locally and then to be able to proceed with the cruentation of the part. Having, at the third meeting, carried out the same protocol again (Ozoile barrier cream), the patient was invited to return after a further 7 days for a final evaluation during which the lesion was assessed and studied for the last time, and all data was recorded again to conclude the course with the participant. This work lasted a total of 21 days with follow-up every 7 days for three weeks: T0 initial time and application of Ozoile hydrogel, T1 T2 treatment with Ozoile barrier cream. A final global re-evaluation meeting (T3) was then held 7 days after the previous one (T2).
Results and statistical analysis
The main outcomes measured included pain reduction, assessed with the Numeric Rating Scale (NRS), the current Al Kline rating, and improvement in walking function.
Descriptive statistical techniques were used to characterize the evolution of the protocol. A p-value < 0.05 was considered statistically significant.
Throughout treatment, the entire study group showed gradual improvements in the reduction of periungual inflammation and pain, as well as in reported walking function. The reduction recorded was statistically significant with an average decrease in NRS score from 10±3.1 to 6±2.2 during the first 7 days, from 7±2.1 to 4±1.7 during the next encounter, and was approximately 3±1. (p<0.05) and an Al Kline classification that regressed an average of 1.6±0.5 stages.
From a percentage point of view, we calculated the comparison between the three encounters examined during this study. Between T0 and T1 the reduction in the pain scale was 26%, between T1 and T2 we saw a 37% decrease, and finally between T0 and T2 a 54% decrease.
42% of patients recovered within the first 10 days of treatment, the majority by the end of the planned course, with an overall treatment success of 93%.
The few subjects who did not recover were advised to change therapy and undergo further specialist investigation. Gender did not play a role in the healing rate, on the other hand, the footwear used can play an important role as a risk factor for the condition, as shoes can increase the likelihood of ingrown toenails by putting pressure on the toes or may delay healing if not changed in favor of a more appropriate shoe with a wider toe box that follows the anatomical shape of the foot. Shoes that are too tight can compress the toes, causing nails to grow into the surrounding skin.
The subjects also reported good tolerability of the treatment. No side effects were recorded during treatment either Ozoile hydrogel or barrier cream on the skin or subcutaneous level (Figure 2, Table 1).
Discussion
General measures for ingrown toenails include proper footwear as well as correct nail trimming; this includes avoiding curved cutting off the lateral margins of the nail plate. General measures should also include management of the underlying factors (hyperhidrosis, onychomycosis). There have been few investigations of the epidemiology of ingrown toenails. Previous reports have noted that the prevalence was as high as 2.5 to 5%.19 It seems that the incidence and prevalence of ingrown toenails have increased these last years, probably due to increased health knowledge, and may also be related to lifestyle changes such as important physical activities. Ingrown toenail affects almost exclusively the hallux toenails. It can occur in one or both nail edges. Involvement of the lateral toe edge occurs twice as much as on the medial side.19,20
Although there is the limitation of the absence of a control group or comparison with another active ingredient, which we reserve the right to investigate at a later date as this was a preliminary study, the data from this study could open up a new frontier of complementary treatment of a pharmacological nature, in support of the therapies already in use in the protocols and guidelines, through the efficacy in topical therapy of Ozoile® in hydrogel and cream forms in the control of painful symptoms in Onychocryptosis, also leading to an improvement in joint function and quality of life in both study groups. The application of the bandage was simple and intuitive for the enrolled patients, who were also able to perform the task at home, with no difficulties arising and no self-care problems coming to our attention. The intervention of the podiatrist in educating the patient was crucial in this study, as almost all of the patients did not know or poorly knew the origin of their nail disease and were unable to find strategies to avoid recurrences. Many theories have been proposed to explain the onset of ingrown toenails. One assumption is that it is related to excess skin surrounding the nail, which is the real culprit. It is explained by wide lateral tissue tending to bulge up around the nail leading to pressure and necrosis.19 Reactive ground forces due to athletic activity, obesity, and/or constricting footwear aid this penetration.21 Given this, changing the wrong footwear, and changing incorrect walking and nail-cutting habits were all important risk factors on which patients need to be more educated to avoid risk. The hydrogel and barrier cream formulations were not described as oily or otherwise uncomfortable during bandaging and absorption was rapid, with no reported complications.
Figure 1.
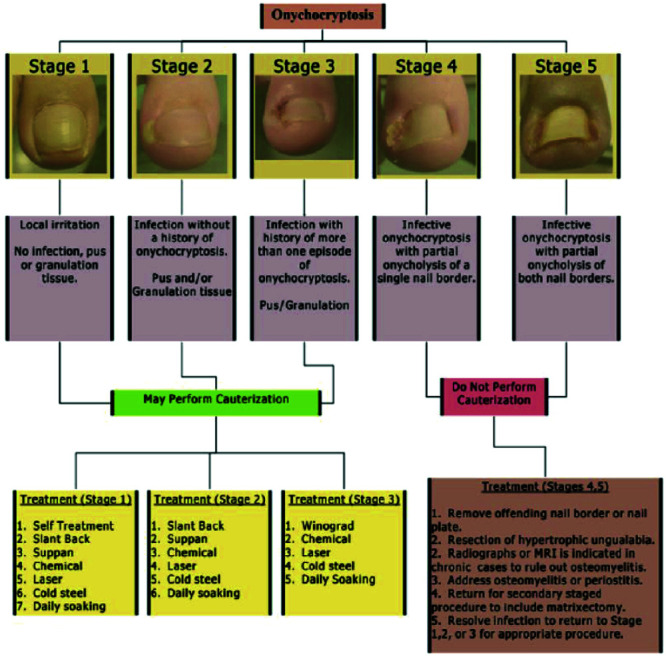
Al Kline classification and treatment algorithm.
Figure 2.
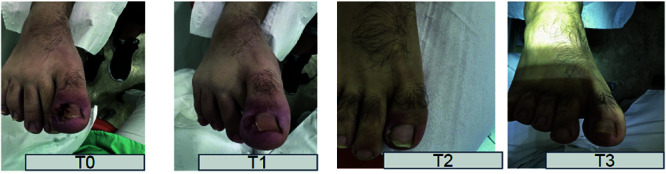
Effect of improvement at the end of the treatment on one of the patients involved.
Table 1.
Al Kline Classification evolution during the study.
| Stadiation Al Kline | T0 (first meeting) | T1 (+7days) | T2 (+7days) | T3 (+7days) |
|---|---|---|---|---|
| S5 | 19 | 5 | 1 | 1 |
| S4 | 0 | 8 | 4 | 0 |
| S3 | 0 | 5 | 5 | 3 |
| S2 | 0 | 1 | 9 | 15 |
The use of Ozoile hydrogel form also allowed a reduction in the degree of inflammation at T1, which was useful in the subsequent re-education of the nail plate, as well as in reducing the invasiveness of the spiculectomy by shortening the time required to restore the nail plate itself.
The same effects were confirmed also using Ozoile barrier cream.
Despite the safety data on the two products, Ozoile requires further studies regarding both efficacy and safety of use.
Conclusions
Ingrown toenails are a common issue that requires the attention of various healthcare professionals, including medical surgeons, dermatologists, and podiatrists. Additionally, specialized podiatry care plays a crucial role in the management of ingrown toenails. Podiatrists with expertise in foot and nail care play a key role in the management of this disease, both in patient follow-up and education. (e.g. on appropriate nail trimming techniques to prevent future issues).
By fostering an interprofessional team approach, we can ensure that patients receive comprehensive care tailored to their needs, leading to optimal outcomes and improved quality of life. In conclusion, these results indicate that the Ozoile-based hydrogel and barrier cream formulations are significantly effective in reducing pain and inflammation and improving function in patients with onychocryptosis in combination with podiatric treatment. This suggests that Ozoile, with its anti-inflammatory and analgesic properties, may be a viable alternative to conventional treatments or even better may be integrated into the most commonly used protocols to achieve a better overall result and patient adherence to the proposed therapy. Patient education was found to be lacking and needs to be worked on more.
These results confirm and correspond with the literature, albeit meager, which highlights the effectiveness of the new pharmacological formulations in treating these clinical pictures. Similar studies have shown that the combined use of innovative pharmacological therapies and early podiatric treatment can lead to better results than single pharmacological or podiatric therapies. Limitations to the study results were found to be the small sample size and poor follow-up period, so further investigation is required in this field.
List of abbreviations
- BMI
Body Mass Index
- COX
Cyclooxygenase
- NRS
Numerical Rating Scales
- NSAIDs
Non-steroidal anti-inflammatory drugs
- SD
Standard Deviation
Footnotes
Conflict of interest
The authors declare no potential conflict of interest, and all authors confirm accuracy.
Contributor Information
Vincenzo Francavilla, Email: vincenzo.francavilla@unikore.it.
Marianna D’Armetta, Email: darmetta.m@gmail.com.
Rosario Toscano, Email: dr.toscanorosario@icloud.com.
Angelo Campo, Email: podologia.campo@gmail.com.
Valentina Catanzaro, Email: valecata82@gmail.com.
Marina Manno, Email: mannomarina70@gmail.com.
Innocenzo Secolo, Email: studiosecolo1967@libero.it.
Giuseppe Messina, Email: giuseppe.messina@uniroma5.it.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
References
- 1.Mayeaux EJ Jr, Carter C, Murphy TE. Ingrown toenail management. Am Fam Physician 2019;100:158-64. [PubMed] [Google Scholar]
- 2.Khunger N, Kandhari R. Ingrown toenails. Indian J Dermatol Venereol Leprol 2012;78:279-89. [DOI] [PubMed] [Google Scholar]
- 3.Arica IE, Bostanci S, Kocyigit P, Arica DA. Clinical and sociodemographic characteristics of patients with ingrown nails. J Am Podiatr Med Assoc 2019;109:201-6. [DOI] [PubMed] [Google Scholar]
- 4.Haneke E. Controversies in the treatment of ingrown nails. Dermatol Res Pract 2012;2012:783924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Erdogan FG, Guven M, Erdogan BD, Gurler A. Previous nail surgery is a risk factor for recurrence of ingrown nails. Dermatol Surg 2014;40:1152-4. [DOI] [PubMed] [Google Scholar]
- 6.Yang G, Yanchar NL, Lo AY, Jones SA. Treatment of ingrown toenails in the pediatric population. J Pediatr Surg 2008;43:931-5. [DOI] [PubMed] [Google Scholar]
- 7.Pico AM, Verjano E, Mayordomo R. Relation between nail consistency and incidence of ingrown toenails in young male runners. J Am Podiatr Med Assoc 2017; 107:137-43. [DOI] [PubMed] [Google Scholar]
- 8.Vural S, Bostanci S, Kocyigit P, et al. Risk factors and frequency of ingrown nails in adult diabetic patients. J Foot Ankle Surg 2018;57:289-95. [DOI] [PubMed] [Google Scholar]
- 9.Heidelbaugh JJ, Lee H. Management of the ingrown toenail. Am Fam Physician 2009;79:303-8. [PubMed] [Google Scholar]
- 10.Borges APP, Pelafsky VPC, Miot LDB, Miot HA. Quality of life with ingrown toenails: a cross-sectional study. Dermatol Surg 2017;43:751-3. [DOI] [PubMed] [Google Scholar]
- 11.Pawlik P, Zaroda P, Dąda P, et al. Onychocryptosis: a review of epidemiology, risk factors, classification, complications and effective therapeutic strategies. J Educ Health Sport 2024;55:199-216. [Google Scholar]
- 12.De Lauro NM, De Lauro TM. Onychocryptosis. Clin Podiatr Med Surg 2004;21:617-30, vii. [DOI] [PubMed] [Google Scholar]
- 13.Moellhoff N, Polzer H, Baumbach SF, et al. Unguis incarnatus – konservative oder operative Therapie? Ein praktischer Behandlungsalgorithmus [Unguis incarnatus-conservative or operative treatment? A practical treatment algorithm]. Unfallchirurg 2021;124:311-318. German. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Currò M, Russo T, Ferlazzo N, et al. Anti-infiammatory and tissue regenerative effects of topical treatment with ozonated olive oil/vitamin E acetate in balanitis xerotica obliterans. Molecules 2018;23:645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Russo T, Currò M, Ferlazzo N, et al. Stable ozonides with vitamin E acetate versus corticosteroid in the treatment of lichen sclerosus in foreskin: evaluation of effects on infiammation. Urol Int 2019;103:459-65. [DOI] [PubMed] [Google Scholar]
- 16.Di Maria D. New therapeutic approach with Ozoile® to the EAC eczema, a chronic and annoying pathology. J Otolaryngol ENT Res 2020;12:32-5. [Google Scholar]
- 17.Al Kline DPM. Onychocryptosis: a simple classification system. Foot Ankle J 2008;1:6. [Google Scholar]
- 18.Ricci E, Pittarello M, Giacinto F. Studio di valutazione del presidio Rigenoma con Ozoile® nel trattamento di lesioni cutanee croniche. Ital J Wound Care 2022;6:90. [Google Scholar]
- 19.Zagolin G, Loss G, Tasinato M, et al. Advantages of the topical application of ozoile® in the healing of venous ulcers of the lower limbs. A randomized clinical study. Biomed J Sci Tech Res 2022;47:7516. [Google Scholar]
- 20.Chabchoub I, Litaiem N. Ingrown toenails. 2022 Sep 18. In: StatPearls [Internet]. Treasure Island (FL): Stat-Pearls Publishing; 2024. Jan–. PMID: 31536303. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.