

Dear Editor,
Skin metastases from visceral cancer, excluding primary skin cancer and hematological malignancies are termed metastatic skin cancer.[1] Cutaneous metastasis from an internal malignancy is an uncommon phenomenon with incidence of 0.7–9%.[1] Cutaneous metastasis represents 2% of all cutaneous tumors.[2] It can be the manifestation of recurrence after the treatment of the primary tumor or rarely be the only manifestation of an underlying internal malignancy. Melanoma, lung cancer, and colorectal cancer are the most common sites of cutaneous metastases in males. Breast cancer, colorectal cancer, and melanoma frequently metastasize to the skin in women.[3] Cutaneous metastases from adenocarcinomas of the colon and rectum are extremely rare and typically signify widespread disease with poor prognosis.[1,4] Through this case report, we present a rare case suggestive of malignancy of carcinoma rectosigmoid whose initial presentation was with painless cutaneous umbilical nodule.
A 62-year-old male, a known case of chronic kidney disease stage-V, presented with complaints of a dark-colored raised lesion over the umbilicus of 1 year duration. There were no associated systemic manifestations like irregular bowel habits, blood in stools, or weight loss. He was clinically diagnosed as a case of umbilical hernia with a secondary infection 3 months back.
Dermatological examination revealed a well-defined hyperpigmented nodular mass with occasional ulceration over the umbilicus [Figure 1]. The histopathology was suggestive of metastatic adenocarcinoma [Figure 2a and 2b]. Immunohistochemistry (IHC) markers confirmed it to be an adenocarcinoma [Figures 3a and 3b].
Figure 1.

A well-defined hyperpigmented nodular mass with ulceration over the umbilicus
Figure 2.
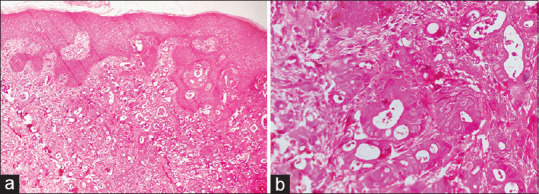
(a) Skin biopsy Showed an infiltrative lesion in the dermis composed of closely placed varying-sized and shaped tubules in a desmoplastic stroma (H & E, 10x). (b) These tubules are lined by cuboidal cells having large pleomorphic vesicular nuclei with prominent nucleoli and moderate amphophilic cytoplasm (H & E, 40x)
Figure 3.
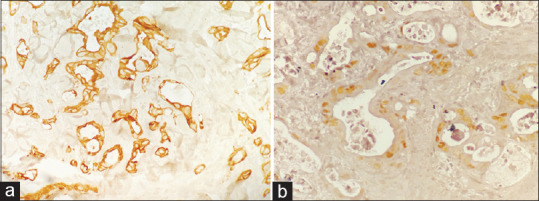
Immunohistochemistry with (a) CK20 (cytoplasmic) and (b) CDX2 (nuclei) highlight the tumor cells
Positron emission tomography-computed tomography was performed to know the primary and it was suggestive of carcinoma rectosigmoid with metastasis to the right breast, left axillary, retroperitoneal lymph node, omental deposits, Sister Joseph nodule, and ascites [Figure 4a and 4b]. The patient was referred to the oncology department for further management. The patient received treatment in the form of chemotherapy and radiotherapy but succumbed 3 months later owing to advanced stage at the time of presentation.
Figure 4.
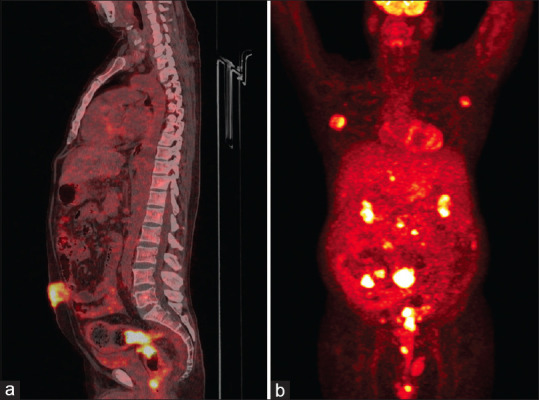
(a) Sagittal section showing metabolically active umbilical mass (Sister Mary Joseph nodule) along with the primary lesion involving the rectosigmoid. (b) 18F-FDG maximum intensity projection images depicting metastatic lesions in the right breast, left axillary lymph node, multiple omental nodules, mesenteric deposits along with primary lesion of the rectosigmoid lesion
Cutaneous metastases present clinically as rapidly growing painless dermal or subcutaneous nodules with intact overlying epidermis, or they can mimic inflammatory dermatosis.[3,4] Rectal carcinoma metastases to the skin have no distinctive features, presenting most often as small subcutaneous or intradermal nodules that measure 1–2 cm in diameter and tend to coalesce.[1] A common site for cutaneous metastasis in rectal carcinoma is the perineum followed by chest and axillae. The face and extremities are infrequently involved.[4,5,6]
Immunohistochemistry uses the CK7 and CK20 IHC algorithm for identifying carcinoma for unknown primary.[7] CK7–CK20+ is generally seen in colorectal carcinoma, gastric adenocarcinoma, and Merkel cell cancer.
Skin metastasis could be the first sign of an underlying advanced rectal cancer. Survival is poor and is generally around 6–7 months after diagnosis.[6] Therefore, recognition of suspicious skin lesions as possible harbingers of undiagnosed visceral malignancy is important in treating patients with or without a history of cancer.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Dehal A, Patel S, Kim S, Shapera E, Hussain F. Cutaneous metastasis of rectal cancer: A case report and literature review. Perm J. 2016;20:74–8. doi: 10.7812/TPP/15-078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chraiet N, Zenzri Y, Bouaziz H, Sassi I, Guebsi A, Kamoun S, et al. Generalized cutaneous metastases of breast cancer: An uncommon presentation. Clin Case Rep. 2020;8:667–71. doi: 10.1002/ccr3.2693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wang DY, Ye F, Lin JJ, Xu X. Cutaneous metastasis: A rare phenomenon of colorectal cancer. Ann Surg Treat Res. 2017;93:277–80. doi: 10.4174/astr.2017.93.5.277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hashimi Y, Dholakia S. Facial cutaneous metastasis of colorectal adenocarcinoma. BMJ Case Rep. 2013;2013:bcr2013009875. doi: 10.1136/bcr-2013-009875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chopra R, Chhabra S, Samra SG, Thami GP, Punia RPS, Mohan H. Cutaneous metastases of internal malignancies: A clinicopathologic study. Indian J Dermatol Venereol Leprol. 2010;76:125–31. doi: 10.4103/0378-6323.60548. [DOI] [PubMed] [Google Scholar]
- 6.Gazoni LM, Hedrick TL, Smith PW, Friel CM, Swenson BR, Adams JD, et al. Cutaneous metastases in patients with rectal cancer: A report of six cases. Am Surg. 2008;74:138–40. [PubMed] [Google Scholar]
- 7.Selves J, Long-Mira E, Mathieu MC, Rochaix P, Ilié M. Immunohistochemistry for diagnosis of metastatic carcinomas of unknown primary site. Cancers (Basel) 2018;10:108. doi: 10.3390/cancers10040108. [DOI] [PMC free article] [PubMed] [Google Scholar]