

Abstract
Introduction:
Pregnant women, postpartum women, and infants are at high risk for complications from influenza. From October to November 2012, Text4baby, a free national text service for pregnant women and mothers of infants aged <1 year, implemented a module of interactive messages encouraging maternal influenza vaccination. A program evaluation examined whether a text-based reminder or tailored education improved self-reported influenza vaccination or intent to be vaccinated later in the influenza season among Text4baby participants.
Methods:
Nearly one third (28,609/89,792) of enrollees responded to a text asking about their vaccination plans. Those planning to receive vaccination were randomly assigned to receive an encouragement message or an encouragement message plus the opportunity to schedule a reminder (n=3,021 at follow-up). Those not planning to be vaccinated were randomly assigned to receive general education or education tailored to their reason for non-vaccination (n=3,820 at follow-up). The effect of the enhanced messages was assessed using multinomial logistic regression in 2013–2014.
Results:
A reminder increased the odds of vaccination at follow-up among mothers (AOR=2.0, 95% CI=1.4, 2.9) and of continued intent to be vaccinated later in the season (pregnant, AOR=2.1, 95% CI=1.4, 3.1; mother, AOR=1.7, 95% CI=1.1, 2.5). Among mothers not planning to be vaccinated because of cost, those who received a tailored message about low-cost vaccination had higher odds of vaccination at follow-up (AOR=1.9, 95% CI=1.1, 3.5). Other tailored messages were not effective.
Conclusions:
Text reminders and tailored education may encourage influenza vaccination among this vulnerable population; both have now been incorporated into Text4baby.
Introduction
Seasonal influenza is more likely to cause severe illness in pregnant and newly postpartum women than in non-pregnant women.1–4 Pregnant women may be more susceptible to or more severely affected by certain viral pathogens, including influenza, because of pregnancy-related immunologic and anatomic/physiologic alterations.5 Pregnant women with influenza are also at increased risk of premature labor and delivery.6
Similarly, children aged below 5 years are at high risk of influenza-related complications, which may result in severe illness, hospitalization, and death.7 Pregnant women who receive influenza vaccine passively transfer influenza immunity to their newborns, which lasts for several months.8 The Advisory Committee on Immunization Practices and the American College of Obstetricians and Gynecologists (ACOG) recommend influenza vaccination for women who are or will be pregnant during influenza season (October–May in the U.S.).9 Postpartum women and other caregivers should also be vaccinated to protect their infants from influenza until they are age 6 months or older and can be vaccinated.
CDC reported that influenza vaccination increased among pregnant women following national efforts to vaccinate against the 2009 H1N1 pandemic influenza virus. Before the pandemic, less than 30% of pregnant women received the vaccine compared with 51% during the 2012–2013 influenza season.10
There is growing interest in using mobile phones to deliver public health interventions, given their ubiquitous nature and potential to reach underserved populations. As of January 2014, 90% of Americans owned mobile phones, and 81% of mobile phone owners sent or received text messages.11 Young adults, minorities, and people with lower levels of income and education text more often than their counterparts.12 Texting has been tested as a strategy to improve knowledge and change behavior.13 A 2010 review of text-based behavior change interventions concluded that most efforts showed evidence of improved behavioral or clinical outcomes, particularly weight loss, smoking cessation, and diabetes management.14 Two recent RCTs had mixed results; an intervention of up to five weekly texts was associated with improved influenza vaccination among low-income, urban children, adolescents, and pregnant women.15,16 However, a pilot study of 204 pregnant, low-income, urban women who had refused influenza vaccine found no increase in vaccination after they received 12 weekly texts.17
Launched in February 2010, Text4baby is the first free national mobile health (mHealth) service in the U.S.; more than 850,000 people have enrolled as of March 2015.18 Text4baby was designed based on health behavior theories, including social cognitive theory, the transtheoretical model, and the health belief model.19,20 The service aims to improve health knowledge and behavior by sending three weekly texts timed to a woman’s due date or her infant’s birthday. Text4baby was created by founding partners, the National Healthy Mothers, Healthy Babies Coalition, Voxiva, The Wireless Foundation, and Grey Healthcare Group, with support from the White House Office of Science and Technology Policy, and the USDHHS. Johnson & Johnson is the founding sponsor. All message content is developed in collaboration with and approved by the Text4baby Content Development Council.a
Early studies of Text4baby enrollees show the program is well received, facilitates interaction with health providers, reminds participants of appointments and immunizations, informs participants of medical warning signs, prepares enrollees for motherhood, and connects them with health services.21–23 Additional studies of Text4baby are ongoing.24
This evaluation of a program enhancement was conducted to assess participant response and inform future Text4baby influenza messaging. The evaluation examined whether the addition of a text-based reminder or tailored education improved
self-reported influenza vaccination; or
intent to be vaccinated later in influenza season (to determine whether there was movement along the continuum of behavior change).
Methods
In October 2012, Text4baby launched an interactive influenza module developed in collaboration with CDC and ACOG.25,26
Study Design
Current enrollees received a baseline survey via text on October 16 or 17, 2012, that asked, Are you planning to get a flu shot this year? There were three response options: Yes, No, and I already got it. Enrollees responding Yes or No were eligible to participate in the evaluation.
Participants responding to the baseline survey that they were planning to be vaccinated (“planners”) were randomly assigned to two groups (simple randomization scheme using the sum of the digits of their phone number [even/odd]). The “usual message” group received one encouragement message advising them to put a reminder on their calendar. The “enhanced messages” group received one encouragement message plus the opportunity to set up a general reminder (sent 2 weeks after receiving their response) or a specific reminder (sent 1 day before their chosen date) (Figure 1).
Figure 1.
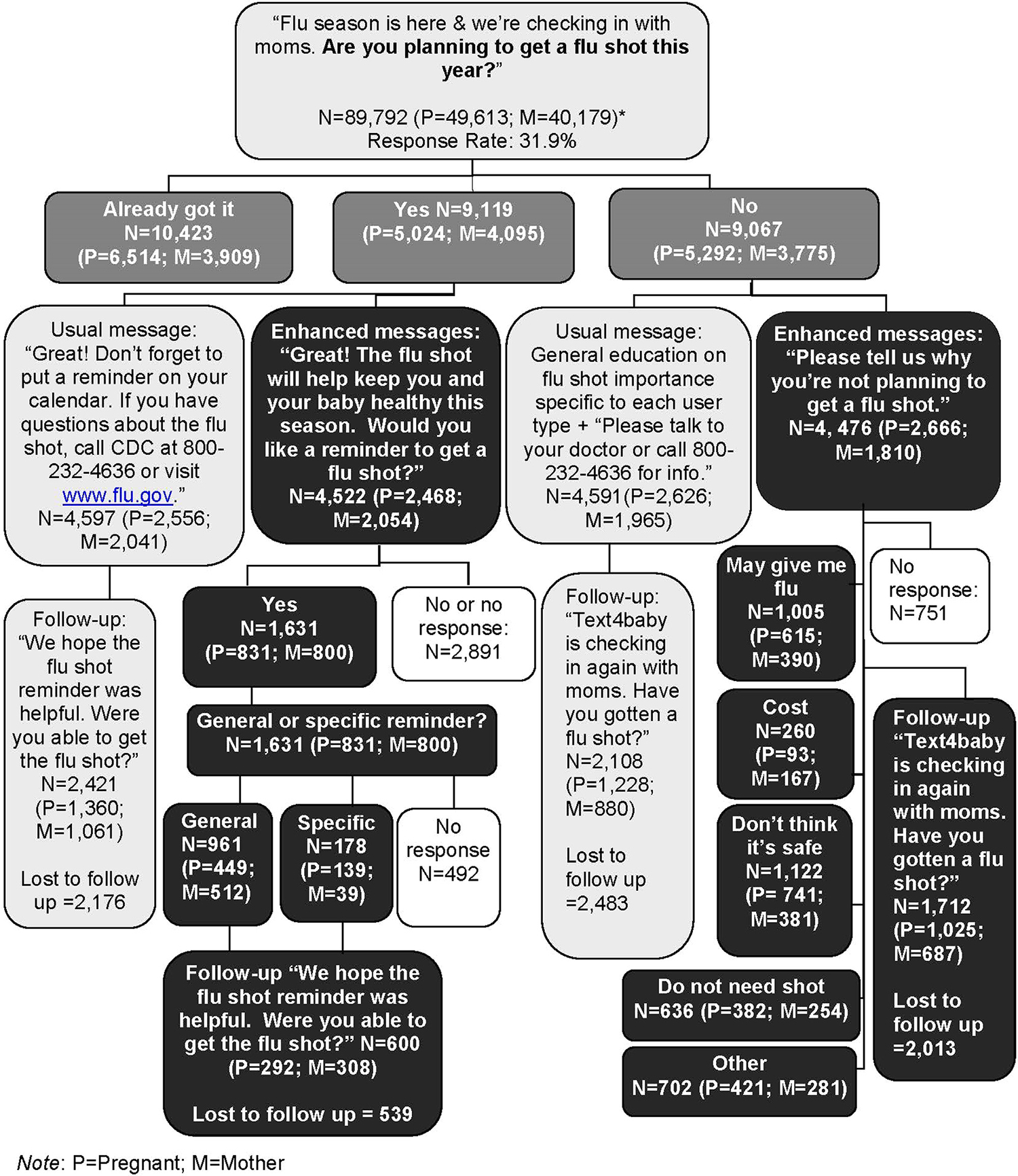
Overview of Text4baby influenza module flow, message content and participant response.
Participants responding at baseline that they were not planning to be vaccinated (“non-planners”) were randomly assigned using the same process. The “usual message group” received a general message stressing the importance of influenza vaccination. The “enhanced messages” group was asked why they were not planning to be vaccinated with five options: I think it may give me flu, Cost, Don’t think it’s safe, Don’t need it, and Other. An educational message tailored to the identified concern was sent to each participant who responded (Figures 1 and 2).
Figure 2.
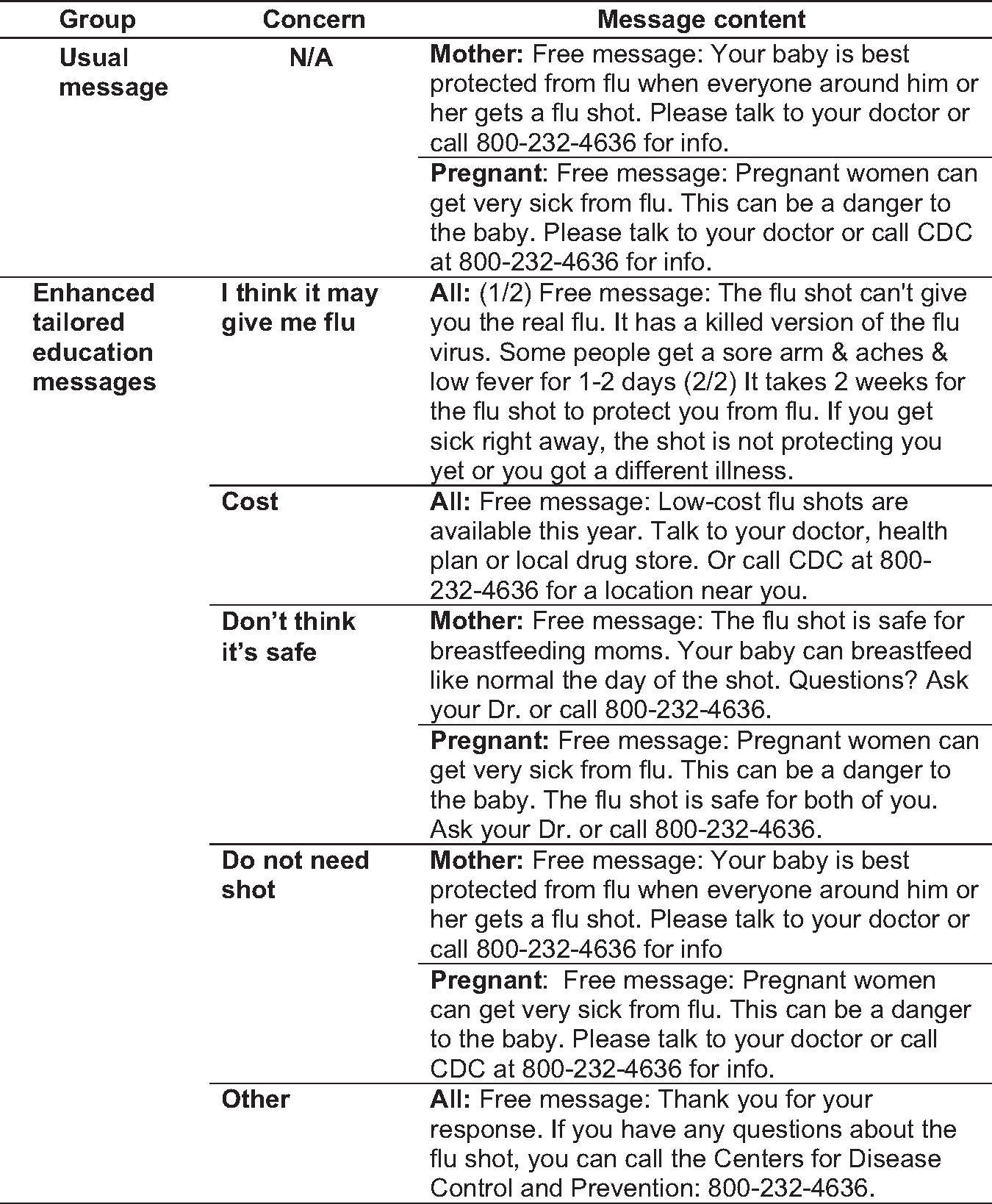
Tailored education message content for Text4baby participants not planning at baseline to get vaccinated.
Planners who received specific reminders were sent the follow-up survey 1 week after receiving their reminder. All other participants were sent the follow-up survey in late November. The survey asked if participants received the vaccine, with three response options: Yes, No, and No, but planning to.
Data Collection
Information captured at enrollment in Text4baby includes
language preference;
enrollment date;
self-reported user type;
self-reported ZIP code; and
self-reported due date or baby’s birthdate.
Enrollees can update their due date and baby’s birthdate at any time. Enrollees not entering a birthdate by the expected end of their 41st week of pregnancy are auto-transitioned to receive postpartum messages and assigned a birthdate. Text4baby enrollees who reported their user type and did not identify as “pregnant” or “mother” were excluded from the study (4%).
In addition to baseline and follow-up survey data, the following data were available for participants. Type of participant (pregnant, mother of infant aged <1 year—hereafter referred to as “mother”) was calculated based on most recent due date or birthdate captured in the Text4baby database. Trimester (first, second, third) was calculated using date of last menstrual period based on due date at baseline. Age of infant (<6 months, 6–12 months) was calculated using birthdate at baseline. Poverty group (<20% poverty, ≥20% poverty) was assigned by matching participant’s ZIP code with ZIP code–level poverty data available through the American Community Survey (2011). Language (Spanish, English) was based on the language chosen at enrollment. Length of most recent enrollment was calculated using date of most recent registration relative to date of the baseline survey.
Statistical Analysis
Univariate and multivariable regression analyses were conducted to determine the effect of:
enhanced reminder messages on “planners”; and
enhanced tailored education messages on “non-planners.”
All analyses were stratified by type of participant at time of receipt of the enhanced or usual message because of differences in the sent messages. Predetermined subgroup analyses were performed according to stated reason for not planning to be vaccinated, and according to type of reminder (general or specific). Multinomial logistic regression models were used to assess the impact of enhanced messages on participants’ vaccination status at follow-up (in three categories: received vaccine, did not receive vaccine, planning to get vaccine). AORs and CIs were computed. Participant characteristics entered as covariates were length of most recent enrollment, trimester, age of infant, and language. Poverty group was considered only for the reminder intervention, given its relationship with the cost component of the tailored education intervention. Data analysis was performed in 2013–2014 using SAS/STAT, version 9.3. Values of p<0.05 were considered statistically significant.
Analysis of de-identified data was approved by Johns Hopkins IRB for this program evaluation. Because this evaluation is not an RCT, the CONSORT Electronic and Mobile Health Applications and online TeleHealth (CONSORT-EHEALTH) were not strictly followed.27
Results
Nearly one third (28,609/89,792) of Text4baby enrollees responded to the baseline survey. Among respondents, 36% (n=10,423) reported they received the influenza vaccination, 32% (n=9,119) reported they were planning to receive it, and 32% (n=9,067) reported they were not planning to receive it (Figure 1). Respondents were slightly more likely to be earlier in their pregnancy and most recently enrolled for a shorter period of time. Loss to follow-up could occur during the delivery of the enhanced messages or at follow-up (Figure 1) and for two reasons (failure to respond to surveys or cancellation of the service). Among women who received enhanced messages, there were no notable differences between those who were eligible to receive the follow-up survey and those who were not or between those who responded to the follow-up survey and those who did not. The same pattern emerged among women who received the usual message. The only exception was that a slightly higher proportion of Spanish language participants in the enhanced reminder group (versus usual message group) responded to the follow-up survey (13% vs 9%).
Reminder Results: Planners
Among planners, more than half (53%) of women who received the enhanced reminder messages (n=1,139) or the usual message (n=4,597) completed the follow-up survey (3,021/5,736). A total of 504 (9%) canceled their Text4baby subscription and were not eligible for the follow-up survey, and 2,211 (39%) did not respond (Figure 1). The enhanced reminder and usual message groups were similar across all characteristics for pregnant women and mothers, indicating that randomization balanced characteristics across groups and that loss to follow-up did not affect the balance (Table 1).
Table 1.
Baseline Characteristics of Text4baby Participants Who Completed Follow-Up, by Message and User Type
| Participants planning at baseline to get vaccinated who completed follow-up |
Participants not planning at baseline to get vaccinated who completed follow-up |
|||||||
|---|---|---|---|---|---|---|---|---|
| Pregnant |
Mother with infant |
Pregnant |
Mother with infant |
|||||
| Characteristics | Usual message (n=1,360) | Enhanced reminder messages (n=292) | Usual message (n=1,061) | Enhanced reminder messages (n=308) | Usual message (n=1,228) | Enhanced tailored education messages (n=1,025) | Usual message (n=880) | Enhanced tailored education messages (n=687) |
|
| ||||||||
| Length of most recent Text4baby enrollment (days), M±SD | 64 ±53 | 58±50 | 116±72 | 113±72 | 66±54 | 68±54 | 113±71 | 113± 72 |
| Language, n (%) | ||||||||
| English | 1,259 (93) | 273 (93) | 977 (92) | 280 (91) | 1,170 (95) | 983 (96) | 828 (94) | 657 (96) |
| Spanish | 101 (7) | 19 (7) | 84 (8) | 28 (9) | 58 (5) | 42 (4) | 52 (6) | 30 (4) |
| Poverty group, n (%) | ||||||||
| ≤20% poverty | 916 (69) | 178 (62) | 698 (66) | 214 (70) | 791 (66) | 674 (66) | 584 (67) | 458 (67) |
| >20% poverty | 429 (32) | 107 (38) | 355 (34) | 91 (30) | 414 (34) | 340 (34) | 284 (33) | 225 (33) |
| Trimester at baseline survey, n (%) | ||||||||
| 1 | 188 (14) | 44 (15) | – | – | 176 (14) | 138 (13) | – | – |
| 2 | 603 (44) | 128 (44) | – | – | 516 (42) | 436 (43) | – | – |
| 3 | 569 (42) | 120 (41) | – | – | 536 (44) | 451 (44) | – | – |
| Age of infant at baseline survey, n (%) | ||||||||
| <6 | – | – | 699 (66) | 199 (69) | – | – | 618 (70) | 482 (70) |
| ≥ 6 | – | – | 362 (34) | 91 (31) | – | – | 262 (30) | 205 (30) |
| Reported vaccination at follow-up, n (%) | 821 (60) | 171 (59) | 444 (42) | 161 (52) | 267 (22) | 219 (21) | 95 (11) | 71 (10) |
Four multivariable logistic regression models assessed the impact of the enhanced reminders compared with the usual message on self-reported receipt of influenza vaccination and continued intent to be vaccinated among women who planned, at baseline, to receive vaccination (Table 2). Two models were used to assess the impact of any enhanced reminder (both general and specific) on pregnant women and mothers. Among pregnant women, receipt of any enhanced reminder increased the odds of influenza vaccination at follow-up (AOR=1.5, 95% CI=1.0, 2.1) and continued intent to be vaccinated later in the influenza season (AOR=2.1, 95% CI=1.4, 3.1). Among mothers, receipt of any enhanced reminder had significant effects on influenza vaccination (AOR=2.0, 95% CI=1.4, 2.9) and continued intent to be vaccinated (AOR=1.7, 95% CI=1.1, 2.5). For pregnant women and mothers, there was no significant difference between the effect of reminders on receipt of vaccination or continued intent.
Table 2.
Effect of Reminders on Vaccination Status: Women Planning at Baseline to Get Vaccinated
| Vaccination status at follow-up |
||||||
|---|---|---|---|---|---|---|
| Total n | Reported did not receive the vaccine, n (%) | Reported received the vaccine, n (%) | Reported continued intent to receive the vaccine, n (%) | AOR (95% CI) for received vaccine versus did not receive the vaccinea | AOR (95% CI) for continued intent to receive the vaccine versus did not receive the vaccinea | |
|
| ||||||
| Text4baby pregnant women who reported they were planning at baseline to get vaccinated | ||||||
| Usual message | 1,360 | 278 (20) | 821 (60) | 261 (19) | 1.0 (ref) | 1.0 (ref) |
| Reminders (any) | 292 | 41 (14) | 171 (59) | 80 (27) | 1.5 (1.0, 2.1) | 2.1 (1.4, 3.1) ** |
| General | 211 | 31 (15) | 125 (59) | 55 (26) | 1.4 (0.9, 2.1) | 1.8 (1.1, 2.9) * |
| Specific | 81 | 10 (12) | 46 (57) | 25 (31) | 1.7 (0.8, 3.4) | 3.1 (1.4, 6.8) ** |
| Text4baby mothers who reported they were planning at baseline to get vaccinated | ||||||
| Usual message | 1,061 | 258 (24) | 444 (42) | 359 (34) | 1.0 (ref) | 1.0 (ref) |
| Reminders (any) | 308 | 46 (15) | 161 (52) | 101 (33) | 2.0 (1.4, 2.9) ** | 1.7 (1.1, 2.5) * |
| General | 282 | 41 (15) | 144 (51) | 97 (34) | 1.9 (1.3, 2.8) ** | 1.8 (1.2, 2.7) * |
| Specific | 26 | 5 (19) | 17 (65) | 4 (15) | 2.4 (0.9, 6.9) | 0.7 (0.2, 3.0) |
Note: Boldface indicates statistical significance.
p<0.05
p<0.01.
Adjusted for length of most recent Text4baby enrollment, trimester, age of infant, language and poverty group.
The other two models assessed the impact of enhanced reminder type (general or specific) compared with the usual message on receipt of influenza vaccination and continued intent to receive vaccination. Mothers who received a general reminder had higher odds of vaccination at follow-up (AOR=1.9, 95% CI=1.3, 2.8), and both pregnant women and mothers who received a general reminder had higher odds of continued intent (pregnant, AOR=1.8, 95% CI=1.1, 2.9; mother, AOR=1.8, 95% CI=1.2, 2.7). Pregnant women who received a specific reminder had increased odds of continued intent (AOR=3.1, 95% CI=1.4, 6.8); they also had higher odds of continued intent than actual vaccination (AOR=2.0, 95% CI=1.1, 3.3; data not shown).
Tailored Education Results: the Non-Planners
Among non-planners, slightly less than half (46%) of women who received enhanced tailored education messages (n=3,725) or the usual message (n=4,591) completed the follow-up survey (3,820/8,316). A total of 968 (12%) canceled their Text4baby subscription and were not eligible to receive the follow-up survey, and 3,528 (43%) did not respond (Figure 1). The enhanced tailored education and usual message groups were similar across all characteristics for pregnant women and mothers (Table 1).
For women who did not plan to be vaccinated at baseline, receipt of the enhanced tailored education messages compared to the usual message was not associated overall with self-reported receipt of influenza vaccination or intent to receive vaccination (Table 3). There was also no significant difference between the effect of tailored education on receipt of vaccination or intent to be vaccinated. However, among mothers who reported they were not planning to be vaccinated because of cost, those who received a single tailored message about where to obtain low-cost or free vaccination had nearly two times higher odds of reporting vaccination at follow-up (AOR=1.9, 95% CI=1.1, 3.5). No other significant effects were observed at the individual message level for tailored messages that addressed other concerns.
Table 3.
Effect of Tailored Education on Vaccination Status: Women Not Planning at Baseline to Get Vaccinated
| Vaccination status at follow-up |
||||||
|---|---|---|---|---|---|---|
| Education | Total n | Reported did not receive vaccine, n (%) | Reported received the vaccine, n (%) | Reported intent to receive the vaccine, n (%) | AOR (95% CI) for received the vaccine versus did not receive vaccinea | AOR (95% CI) for intent to receive the vaccine versus did not receive vaccinea |
|
| ||||||
| Text4baby pregnant women who reported they were not planning at baseline to get vaccinated | ||||||
| Usual message | 1,228 | 758 (62) | 267 (22) | 203 (17) | 1.0 (ref) | 1.0 (ref) |
| Tailored education (Any) | 1,025 | 658 (64) | 219 (21) | 148 (14) | 1.0 (0.8, 1.2) | 0.8 (0.7, 1.1) |
| Don’t need it | 165 | 110 (67) | 34 (21) | 21 (13) | 0.9 (0.6, 1.3) | 0.7 (0.4, 1.2) |
| Safety | 316 | 206 (65) | 60 (19) | 50 (16) | 0.8 (0.6, 1.1) | 0.9 (0.6, 1.3) |
| Cost | 49 | 30 (61) | 9 (18) | 10 (20) | 0.8 (0.4, 1.7) | 1.2 (0.6, 2.4) |
| Shot gives you flu | 207 | 132 (64) | 46 (22) | 29 (14) | 1.1 (0.8, 1.5) | 0.8 (0.6, 1.2) |
| Other | 288 | 180 (63) | 70 (24) | 38 (13) | 1.0 (0.7, 1.5) | 0.8 (0.5, 1.3) |
| Text4baby mothers who reported they were not planning at baseline to get vaccinated | ||||||
| Usual message | 880 | 620 (70) | 95 (11) | 165 (19) | 1.0 (ref) | 1.0 (ref) |
| Tailored education (Any) | 687 | 493 (72) | 71 (10) | 123 (18) | 0.9 (0.7, 1.3) | 0.9 (0.7, 1.2) |
| Don’t need it | 109 | 76 (70) | 12 (11) | 21 (19) | 1.1 (0.6, 2.0) | 1.1 (0.6, 1.8) |
| Safety | 168 | 130 (77) | 12 (7) | 26 (15) | 0.6 (0.3, 1.1) | 0.8 (0.5, 1.2) |
| Cost | 83 | 53 (64) | 16 (19) | 14 (17) | 1.9 (1.1, 3.5) | 1.0 (0.5, 1.8) |
| Shot gives you flu | 147 | 113 (77) | 10 (7) | 24 (16) | 1.1 (0.7, 1.9) | 1.2 (0.8, 1.8) |
| Other | 180 | 121 (67) | 21 (12) | 38 (21) | 0.6 (0.3, 1.2) | 0.8 (0.5, 1.3) |
Note: Boldface indicates statistical significance (p<0.05).
Adjusted for length of most recent Text4baby enrollment, trimester, age of infant and language.
Discussion
A novel, randomized, text-based approach was used to assess the effect of enhanced Text4baby messages. This type of evaluation methodology allows for assessment and rapid improvement of mHealth programs without the high costs and length of time usually associated with traditional RCTs, which can be especially challenging to conduct given the quick evolution of technology.27,28
In this evaluation, an additional reminder appeared effective at improving rates of influenza vaccination or continued intent to receive vaccination among participants planning to be vaccinated. However, with only 22 mothers who received a specific reminder, there was inadequate statistical power to determine whether a specific reminder might be more effective at improving vaccination than a general reminder. The single tailored message providing information on free and low-cost influenza vaccination was effective at overcoming the concern about cost for mothers, but not pregnant women. This finding could be the result of Type I error, but the association is large (AOR=1.9) and is plausible. Cost is a barrier that a single practical message could help overcome for mothers who may have lost insurance coverage after delivery. However, a single tailored message was not effective at improving vaccination receipt or intent among women who reported more-complex concerns, such as vaccine safety.
Many mHealth initiatives, including Text4baby, are grounded in traditional health behavior theories, using both unidirectional and bidirectional messaging as cues to action and behavior change.19,20 Five reviews14,29–31 of text-based interventions show evidence of significant effects for behavior change and healthcare processes, such as appointment attendance. Findings from this evaluation are consistent with two recent RCTs15,16 that found a positive association between text reminders and improved influenza vaccination among children, adolescents, and pregnant women. However, in this evaluation, the addition of a single reminder was assessed as compared to five weekly messages and two appointment reminders sent to pregnant women, suggesting the number of reminders needed to encourage influenza vaccination should be studied further.
Several researchers32–34 have demonstrated high acceptability of tailored health information and that health programs that stimulate interaction and engagement are more likely to promote behavior change. Lewis and colleagues35 tested delivery of text-based tailored health information among participants with HIV infection and found strong acceptability and improved self-reported adherence to HIV medication. Although the single tailored message providing information on free and low-cost influenza vaccination was effective for mothers, the type and number of messages were not sufficient for women with other concerns, such as vaccine safety. Similar results were reported in another study that sent 12 weekly texts to pregnant women in their first or second trimester who previously declined vaccination.17
This evaluation has several strengths. It was based on established conceptual models of health behavior, benefited from a large, geographically diverse sample, and had a sample of individuals who are likely similar in their health consciousness, thus partially controlling for the effect of health-seeking behavior on vaccination receipt. The innovative text-based survey approach allowed for rapid data collection and analysis for program evaluation. Based on the results of this evaluation, Text4baby enrollees during the 2013–2014 influenza season were sent an educational message with information on low-cost influenza vaccinations, an offer to receive a free influenza vaccination through a partnership with Rite Aid, and a separate influenza vaccination reminder. External validity of the findings is supported by the similarity of the vaccination rate among Text4baby pregnant enrollees responding to baseline or follow-up surveys (51%) to the national rate reported for pregnant women by CDC for the same time frame (47%).36 Additionally, reported vaccination concerns are similar to findings reported from the November 2012 CDC Internet panel survey; vaccine safety and efficacy were the most frequently reported concerns in both surveys.10 Finally, the design gave unvaccinated usual message participants an opportunity to receive enhanced messages during influenza season (after follow-up).
Limitations
This evaluation also has limitations. Given the non-response that occurred throughout the evaluation, these findings cannot be generalized to the overall Text4baby population or to other mHealth programs. Additionally, because the amount and type of information that can be collected by text are limited, and collecting too much data may deter enrollment, only very basic information is collected by Text4baby. Some standard demographic data such as education level and race/ethnicity are not collected. Further, all data are either self-report (e.g., vaccination status) or proxy data (poverty group, language, and birthdate for participants who were auto-transitioned) and were not independently verified. Other characteristics not assessed as part of this evaluation may have differed between the enhanced and usual message groups and between participants and those lost to follow-up, potentially impacting the findings. However, there were no notable differences in participant characteristics at baseline and for those who were lost to follow-up. Thus, the findings are internally consistent. Participants had to respond to one or more additional questions to receive enhanced messaging; thus, it is possible that these participants were those who were more favorably inclined toward vaccination. Additionally, a slightly higher proportion of Spanish language participants responded to the follow-up survey in the enhanced reminder group compared to the usual message group. However, the number of Spanish language participants is very small; future research should explore if there are differential effects for those who receive Spanish (versus English) messages. Finally, the design made it impossible to evaluate the end-of-season effects of enhanced messaging by collecting additional data after November 2012.
Conclusions
Given that mHealth is still in its infancy, rigorous research and evaluations are needed to understand factors contributing to successful, effective programs. As mHealth programs grow in popularity given their potential to improve healthcare access, behaviors, and outcomes, future considerations include
choosing research designs and comparison groups to answer specific questions (i.e., an external comparison group is needed to assess the net effect of Text4baby separately from the effectiveness of the messaging assessed here);
exploring the relationship between length of program exposure and number of messages on a topic and the outcome; and
using a mixed methods approach to better understand motivations that underlie specific behaviors and options for addressing motivations using mHealth.
These evaluation results contribute to growing evidence that text-based reminders and tailored education can encourage positive health behavior, such as influenza vaccination, among vulnerable populations.
Acknowledgments
The authors thank Lalida Thaweethai, Senior Product Manager for Voxiva, and Amy Pirretti, Clinical Quality Director for Text4baby, for their leadership in developing and implementing the 2012–2013 Text4baby Influenza Module. The authors would also like to acknowledge and thank Text4baby partners and supporters for their efforts to share Text4baby with pregnant women and mothers across the country, and founding sponsor Johnson & Johnson. No specific funding was obtained to support this study.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of CDC.
Dr. Pamela Johnson is a co-founder, board member, and stockholder in Voxiva. No other financial disclosures were reported by the authors of this paper.
Footnotes
The Text4baby Content Development Council is made up of the following leading national medical health organizations and federal partners who review messages to keep content current and accurate: American College of Nurse-Midwives; CDC, USDHHS; March of Dimes; American Academy of Pediatrics; Association of Women’s Health, Obstetric and Neonatal Nurses; Society for Maternal-Fetal Medicine; ACOG; National Association of Pediatric Nurse Practitioners; and Health Resources and Services Administration, USDHHS.
References
- 1.Dodds L, McNeil SA, Fell DB. Impact of influenza exposure on rates of hospital admission and physician visits because of respiratory illness among pregnant women. CMAJ. 2007;176(4):463–468. 10.1503/cmaj.061435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kennedy ED, Ahluwalia IB, Ding H, Lu PJ, Singleton JA, Bridges CB. Monitoring seasonal influenza vaccination coverage among pregnant women in the United States. Am J Obstet Gynecol. 2012;207(3)(suppl):S9–S16. 10.1016/j.ajog.2012.06.069. [DOI] [PubMed] [Google Scholar]
- 3.Neuzil KM, Reed GW, Mitchel EF, Simonsen L, Griffin MR. Impact of influenza on acute cardiopulmonary hospitalizations in pregnant women. Am J Epidemiol. 1998;148(11):1094–1102. 10.1093/oxfordjournals.aje.a009587. [DOI] [PubMed] [Google Scholar]
- 4.CDC. Updated recommendations for obstetric health care providers related to use of antiviral medications in the treatment and prevention of influenza (current for the 2013–2014 season). 2014. www.cdc.gov/flu/professionals/antivirals/avrec_ob.htm.
- 5.Prevention Beigi R. and management of influenza in pregnancy. Obstet Gynecol Clin N Am. 2014;41:535–546. 10.1016/j.ogc.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 6.USDHHS. Pregnant women. www.flu.gov/at-risk/pregnant.
- 7.CDC. Flu information for parents with young children. 2011. www.cdc.gov/flu/parents/index.htm.
- 8.Eick AA, Uyeki TM, Klimov A, et al. Maternal influenza vaccination and effect on influenza virus infection in young infants. Arch Pediatr Adolesc Med. 2011;165(2):104–111. 10.1001/archpediatrics.2010.192. [DOI] [PubMed] [Google Scholar]
- 9.American College of Obstetricians and Gynecologists. Influenza Vaccination During Pregnancy. Washington, DC: Committee Opinion; 2010. Report No.: 468. www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Influenza-Vaccination-During-Pregnancy. [Google Scholar]
- 10.CDC. Influenza vaccination coverage among pregnant women—United States, 2012–13 Influenza Season. MMWR Morb Mortal Wkly Rep. 2013;62(38):787–792. [PMC free article] [PubMed] [Google Scholar]
- 11.Pew Research Center. Mobile Technology Fact Sheet. Pew Internet: mobile. 2014. www.pewinternet.org/Commentary/2012/February/Pew-Internet-Mobile.aspx. [Google Scholar]
- 12.Pew Research Center. Americans and text messaging. Washington, DC: Pew Internet & American Life Project; 2011. www.pewinternet.org/~/media/Files/Reports/2011/Americans%20and%20Text%20Messaging.pdf. [Google Scholar]
- 13.Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med. 2009;36(2):165–173. 10.1016/j.amepre.2008.09.040. [DOI] [PubMed] [Google Scholar]
- 14.Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev. 2010;32(1):56–59. 10.1093/epirev/mxq004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Stockwell MS, Kharbanda EO, Martinez RA, Vargas CY, Vawdrey DK, Camargo S. Effect of a text messaging intervention on influenza vaccination in an urban, low-income pediatric and adolescent population: a randomized controlled trial. JAMA. 2012;307(16):1702–1708. 10.1001/jama.2012.502. [DOI] [PubMed] [Google Scholar]
- 16.Stockwell MS, Westhoff C, Kharbanda EO, et al. Influenza vaccine text message reminders for urban, low-income pregnant women: a randomized controlled trial. Am J Public Health. 2014;104(suppl 1):e7–e12. 10.2105/AJPH.2013.301620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Moniz MH, Hasley S, Meyn LA, Beigi RH. Improving influenza vaccination rates in pregnancy through text messaging: a randomized controlled trial. Obstet Gynecol. 2013;121(4):734–740. 10.1097/AOG.0b013e31828642b1. [DOI] [PubMed] [Google Scholar]
- 18.Whittaker R, Matoff-Stepp S, Meehan J, et al. Text4baby: development and implementation of a national text messaging health information service. Am J Public Health. 2012;102(12):2207–2213. 10.2105/AJPH.2012.300736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Evans WD, Abroms LC, Poropatrich R, Nielsen PE, Wallace JL. Mobile health evaluation methods: the Text4baby case study. J Health Commun. 2012;17(1):22–29. 10.1080/10810730.2011.649157. [DOI] [PubMed] [Google Scholar]
- 20.Jordan ET, Ray EM, Johnson P, Evans WD. Using text messaging to improve maternal and newborn health. Nurs Womens Health. 2011;15 (3):206–212. 10.1111/j.1751-486X.2011.01635.x. [DOI] [PubMed] [Google Scholar]
- 21.Gazmararian JA, Elon L, Yang B, Graham M, Parker R. Text4baby program: an opportunity to reach underserved pregnant and postpartum women? Matern Child Health J. 2014;18(1):223–232. 10.1007/s10995-013-1258-1. [DOI] [PubMed] [Google Scholar]
- 22.Martinez KM, Uekusa S. National Survey of Text4baby Participants. 2013. www.csusm.edu/anthropology/docsandfiles/Text4baby.pdf.
- 23.Evans WD, Wallace JL, Snider J. Pilot evaluation of the Text4baby mobile health program. BMC Public Health. 2012;12:1031. 10.1186/1471-2458-12-1031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Text4baby. Text4baby Research and Evaluation. 2014. www.text4baby.org/index.php/about/data-and-evaluation.
- 25.CDC. Influenza vaccination coverage among pregnant women—United States, 2011–12 Influenza Season. MMWR Morb Mortal Wkly Rep. 2012;61(38):758–763. [PubMed] [Google Scholar]
- 26.Lynch MM, Mitchell EW, Williams JL, et al. Pregnant and recently pregnant women’s perceptions about influenza A pandemic (H1N1) 2009: implications for public health and provider communication. Matern Child Health J. 2012;16(8):1657–1664. 10.1007/s10995-011-0865-y. [DOI] [PubMed] [Google Scholar]
- 27.Eysenbach G CONSORT-EHEALTH: improving and standardizing evaluation reports of web-based and mobile health interventions. J Med Internet Res. 2011;13(4):e126. 10.2196/jmir.1923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Payne P Do mHealth apps require randomized controlled trials—panel discusses at mHealth Summit. 2012. www.imedicalapps.com/2012/12/mhealth-apps-require-randomized-controlled-trials-mhealth-summit/.
- 29.Krishna S, Boren S, Balas E. Healthcare via cell phones: a systematic review. Telemed J E Health. 2009;15(3):231–240. 10.1089/tmj.2008.0099. [DOI] [PubMed] [Google Scholar]
- 30.Whittaker R, McRobbie H, Bullen C, Borland R, Rodgers A, Gu Y. Mobile phone-based interventions for smoking cessation. Cochrane Database Syst Rev. 2012;11:CD006611. 10.1002/14651858.CD006611.pub3. [DOI] [PubMed] [Google Scholar]
- 31.Whittaker R, Merry S, Dorey E, Maddison R. A development and evaluation process for mHealth interventions: examples from New Zealand. J Health Commun. 2012;17:11–21. 10.1080/10810730.2011.649103. [DOI] [PubMed] [Google Scholar]
- 32.Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol Bull. 2007;133(4):673–693. 10.1037/0033-2909.133.4.673. [DOI] [PubMed] [Google Scholar]
- 33.Kreuter MW, Farrell D, Olevitch L, Brennan L. Tailoring Health Messages: Customizing Communication With Computer Technology. Mahwah, NJ: Erlbaum, 2000. [Google Scholar]
- 34.Doak CC, Doak LG, Root JH. Teaching Patients With Low Literacy Skills, 2nd ed., Philadelphia, PA: J.B. Lippincott Company, 1996. [Google Scholar]
- 35.Lewis MA, Uhring JD, Bann CM, et al. Tailored text messaging intervention for HIV adherence: a proof-of-concept study. Health Psychol. 2013;32(3):248–253. 10.1037/a0028109. [DOI] [PubMed] [Google Scholar]
- 36.CDC. Influenza vaccination coverage among pregnant women—United States, 2011–12 Influenza Season, United States. MMWR Morb Mortal Wkly Rep. 2012;61(31):758–763. [PubMed] [Google Scholar]