

Abstract
Purpose
To describe the epidemiology, clinical features, and classification of uveitis in a large cohort of Colombian patients.
Methods
Data were collected from seven ophthalmological referral centers in the four main cities in Colombia. The study included patients with a confirmed diagnosis of uveitis from January 2010 to December 2022. Information on demographics, ophthalmic examination findings, uveitis classification, and etiology was recorded.
Results
The study reviewed 3,404 clinical records of patients with uveitis. The mean age at diagnosis was 41.1 (SD 19.0) years, and 54.2% of the patients were female. Overall, 1,341(39.4%) were infectious, 626 (18.4%) non-infectious, and four masquerade syndromes (0.1%). The most common types of uveitis were unilateral (66.7%), acute (48.3%), and non-granulomatous (83%). Anterior uveitis was the most common anatomical localization (49.5%), followed by posterior uveitis (22.9%), panuveitis (22.3%), and intermediate uveitis (5.2%). A diagnosis was established in 3,252 (95.5%) cases; idiopathic was the most common cause (27.7%), followed by toxoplasmosis (25.3%) and virus-associated uveitis (6.4%). The age group between 30 and 50 exhibited the highest frequency of uveitis.
Conclusion
This multicenter study comprehensively describes uveitis characteristics in Colombian patients, providing valuable insights into its demographic and clinical features. The study findings emphasize the need to continue updating the changing patterns of uveitis to improve diagnosis and treatment strategies for diseases associated with intraocular inflammation.
Keywords: Uveitis, Classification, Epidemiology, Colombia, Toxoplasmosis

Introduction
The term “uveitis” encompasses several diseases characterized by intraocular inflammation. It can be infectious or noninfectious, including autoimmune, autoinflammatory, traumatic, post-surgical, drug-induced, and idiopathic. Each type of uveitis has particular demographic and clinical characteristics, but in general, they predominantly affect people of working age, generating a significant economic burden [1–3].
Uveitis prevalence oscillates from 36.2 to 730 per 100,000 inhabitants, and its incidence ranges from 17 to 52.4 per 100,000 inhabitants [4]. These values vary according to the region and the study design that informs them. Similarly, global epidemiological patterns vary due to the influence of several factors, such as environmental, socioeconomic, and epigenetic elements, contributing to different etiologies' prevalence in each region [5–8].
In Colombia, Polania et al. presented the demographic and clinical characteristics of 489 uveitis patients, indicating a notable transition from infectious to immune-mediated etiologies in the last few years as the leading cause of uveitis in the country's capital city [9]. However, data was collected from a single center and may only partially represent the broader reality. Therefore, this multicenter study aims to describe the epidemiology, clinical features, and classification of uveitis in a large cohort of Colombian patients from diverse cities nationwide.
Methods
Study design
Multicenter cross-sectional study. It adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Ethics consideration
The Ethics Committee of Universidad del Rosario approved this study. In addition, this study follows the ethical principles for human research established by the Helsinki Declaration, the Belmont Report, and Colombian Resolution 008430 of 1993.
Data source and study population
We collected data from seven ophthalmological referral centers across four major cities (Bogotá, Cali, Medellín, and Bucaramanga) and spanning approximately 20 departments within Colombia. The data collection period was extended from January 2010 to December 2022. To ensure the privacy and confidentiality of the patients, all clinical information was procured using a unique identification code, thereby maintaining anonymity. Collected data include demographic details, medical history, specific etiological diagnosis (non-infectious, infectious, undetermined, and idiopathic), visual acuity, uveitis localization, onset, duration, clinical course, and ocular complications (cataract, uveitic glaucoma, macular edema, epiretinal membrane, vitreous hemorrhage, and retinal detachment, among others). Demographic data were primarily acquired during the initial patient visit by administering a questionnaire about uveitis risk factors and systemic symptoms supplemented with a comprehensive physical examination. Ocular findings were collected at the first consultation.
Co-investigators trained in data entry and management were responsible for filling the database to ensure consistency and reliability. Furthermore, two investigators independently verified the accuracy and completeness of the data. Uveitis patients with incomplete or inconsistent data or who were exclusively diagnosed with conditions such as keratitis, optic neuritis, and scleritis were excluded from the dataset (n = 92).
Ophthalmological assessment
Best-corrected visual acuity (BCVA) was measured with Snellen charts, and the values were converted to logarithms of minimal angle of resolution equivalent units (logMAR) for statistical calculations. All patients underwent a comprehensive evaluation by a uveitis specialist, including slit lamp biomicroscopy, intraocular pressure, and dilated fundus examination. Furthermore, clinical data, such as the time of initial uveitis diagnosis, the frequency of uveitis episodes, and laterality, were documented.
Uveitis definition
Uveitis and anterior chamber grading classification were determined using the Standardization of Uveitis Nomenclature (SUN) criteria [10]. Vitreous haze was graded according to the National Eye Institute system with binocular indirect ophthalmoscopy [11].
Diagnosing systemic disease associated with uveitis was established in a multidisciplinary approach with other medical specialists, including internal medicine, rheumatologists, infectious diseases specialists, and pediatricians. The condition that was the most prominent or more likely related to uveitis was regarded as the primary diagnosis whenever two or more systemic diseases occurred concurrently with uveitis. The diagnosis of ocular sarcoidosis was made according to the SUN 2021 revised criteria [12] and the International Workshop on Ocular Sarcoidosis [13]. A chest X-ray was used as the screening tool for chest imaging; computed tomography scanning was used in cases of equivocal chest radiographs or cases with high suspicion of other grounds. Additionally, in instances where sarcoidosis was highly suspected, yet imaging results were inconclusive, it was ruled out using serological tests like Angiotensin-Converting Enzyme levels [14, 15].
Diagnosis of Blau syndrome was confirmed by NOD2 mutation [16]. The criteria for a diagnosis of presumed ocular tuberculosis included the identification of a tuberculous etiology by Quantiferon Gold TB positivity or Mantoux tuberculin skin test, having or not having abnormalities on chest X-ray, exclusion of other possible causes of uveitis and response to anti-tuberculosis treatment [17]. The diagnosis of the other systemic diseases was determined using the internationally standardized criteria for each disease.
Traumatic iritis was defined as inflammatory cells or flare in the anterior chamber in a patient with recent trauma and in whom infectious and non-infectious uveitis was ruled out. Lens-induced uveitis was defined as an immune reaction to lens material. Moreover, Idiopathic Persistent Iritis after cataract surgery (IPICS) was defined as a transient, non-infectious inflammatory response in the eye that occurs after surgical procedures [18].
Regarding viral uveitis, an initial panel of serology tests was conducted, which included screening for antibodies against Herpes simplex, Herpes zoster, and Cytomegalovirus. When available, patients with atypical presentations underwent aqueous-vitreous humor sampling and a Polymerase Chain Reaction (PCR) [19, 20]. A diagnosis of confirmed virus-associated uveitis was established if a positive result was obtained in PCR. In contrast, in cases where the diagnosis relied only on clinical features and response to antiviral therapy, it was categorized as suspected viral virus-associated uveitis. Furthermore, the diagnosis of ocular toxoplasmosis was made based on clinical criteria, which included positive anti-Toxoplasma IgG and/or IgM test results with an active creamy-white focal retinal lesion with/without hyperpigmented retinochoroidal scars [21].
In cases where an etiology could not be discovered due to a lack of follow-up of the patients, without having ruled out all possible diagnoses, it was considered undetermined. Idiopathic etiology was reserved for cases where the diagnosis could not be determined after ruling out infectious and noninfectious causes of uveitis. It is important to note that while 'Pars planitis' falls under the umbrella of idiopathic conditions, this term was exclusively applied to cases characterized by non-infectious intermediate uveitis accompanied with vitritis and either inferior vitreous inflammatory condensates (“snowballs”) or pars plana “snowbanks”, unassociated with a systemic disease [22].
Uveitis diagnoses were categorized into five groups for analytical clarity and precision. These groups include infectious, non-infectious (encompassing autoimmune, autoinflammatory, and mixed etiologies as delineated by McGonagle and McDermott) [23], masquerade syndromes, idiopathic, and undetermined. Additionally, the category labeled 'others' includes specific etiologies such as traumatic iritis, IPICS, lens-induced uveitis, and drug-induced uveitis.
Statistical analysis
For the univariate analysis, the continuous variables were reported as mean and standard deviation (SD) or median and interquartile range (IQR) (25th–75th percentile) depending on its distribution, for categorical variables as relative and absolute frequencies and percentages. All the analyses were done using Jamovi (Version 2.3).
Results
From 3,496 clinical records, we included 3,404 patients diagnosed with uveitis, of which 54.2% (n = 1,847) were female. The mean age at onset was 35.7 years, ranging from 1 to 96 years. Overall, 1,341(39.4%) were infectious, 626 (18.4%) non-infectious, and four masquerade syndromes (0.1%). Bilateral involvement was observed in 33% of cases (n = 1,124), while 66.7% (n = 2,270) presented with unilateral compromise. Table 1, Figs. 1 and 2 show a summary of the demographic information of the included patients.
Table 1.
Demographic characteristics of patients with uveitis in Colombia
| Demographics | Anterior | Intermediate | Posterior | Panuveitis | Total |
|---|---|---|---|---|---|
| Age (years) mean ± SD | |||||
| At consultation | 50.2 ± 17.8 | 33.5 ± 20.1 | 38.1 ± 19.5 | 42.7 ± 18.7 | 41.1 ± 19.0 |
| At onset | 46.2 ± 18.6 | 29.9 ± 20.8 | 29.4 ± 20.4 | 37.4 ± 18.7 | 35.7 ± 19.6 |
| Gender n (%) | |||||
| Female | 935 (50.6) | 98 (5.4) | 404 (21.9) | 410 (22.2) | 1,847 (54.2) |
| Male | 752 (48.6) | 78 (5.0) | 373 (24.1) | 345 (22.3) | 1,548 (45.5) |
| Missing data | 0 | 2 (22.2) | 3 (33.3) | 4 (44.4) | 9 (0.2) |
| City of Origin n (%) | |||||
| Bogotá | 578 (38.0) | 69 (4.5) | 452 (29.7) | 422 (27.7) | 1,521 (44.7) |
| Bucaramanga | 106 (66.7) | 0 (0.0) | 23 (14.5) | 30 (18.9) | 159 (4.7) |
| Cali | 697 (58.8) | 58 (4.9) | 201 (16.9) | 230 (19.4) | 1,186 (34.8) |
| Medellín | 306 (56.9) | 51 (9.5) | 104 (19.3) | 77 (14.3) | 538 (15.8) |
| Etiology | |||||
| Infectious | 339 (25.3) | 19 (1.4) | 634 (47.3) | 349 (26.0) | 1,341 (39.4) |
| Non-infectious | 411 (65.7) | 23 (3.7) | 30 (4.8) | 162 (25.8) | 626 (18.4) |
| Masquerade | 0 (0) | 0 (0) | 1 (25.0) | 3 (75.0) | 4 (0.11) |
| Idiopathic | 684 (63.7) | 123 (11.5) | 77 (7.2) | 190 (1.8) | 1,074 (31.6) |
| Undetermined | 89 (58.6) | 8 (5.3) | 18 (11.8) | 37 (24.3) | 152 (4.5) |
| Others | 152 (80.4) | 3 (1.6) | 18 (9.5) | 16 (8.5) | 189 (5.6) |
| Missing data | 12 (66.6) | 2 (11.1) | 2 (11.1) | 2 (11.1) | 18 (0.5) |
| Total n (%) | 1,687 (49.6) | 178 (5.2) | 780 (22.9) | 759 (22.3) | 3,404 (100.0) |
Fig. 1.
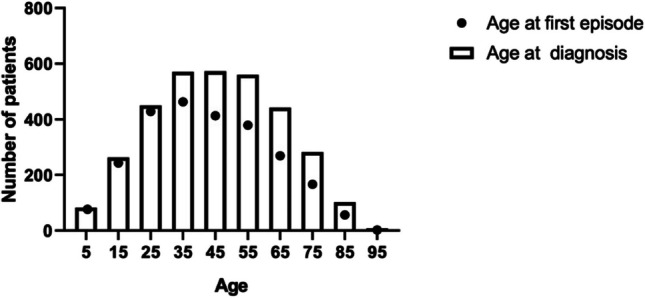
Age distribution of the patients with uveitis in Colombia
Fig. 2.

Most common etiologies and ages of onset and diagnosis among the geographical areas covered. Colombian geographical map is divided by departments; yellow represents the areas covered by Medellín centers, orange areas covered by Cali’s centers, green areas covered by Bucaramanga’s centers, and aquamarine areas covered by Bogotá centers. Departments in white are areas where these centers usually do not have coverage. Distribution of main etiologies of uveitis across the different regions
In general, anterior uveitis was the most common localization (n = 1,687, 49.5%), followed by posterior uveitis (n = 780, 22.9%), panuveitis (n = 759, 22.3%), and intermediate uveitis (n = 178, 5.2%), as evidenced in Table 2. Both anterior and posterior uveitis more frequently presented with an acute course (50.9% and 57.9%, respectively), while intermediate uveitis and panuveitis showed a chronic course in most cases. Of all the anatomical localizations, panuveitis exhibited the highest incidence of complications, including cataracts (n = 256, 33.7%), retinal detachment (n = 138, 18.2%), and macular edema (n = 125, 16.5%). For a more comprehensive overview, please refer to Table 2.
Table 2.
Characteristics of uveitis in the Colombian population divided by anatomical site of inflammation
| Characteristics | Anterior N = 1,687 | Intermediate N = 178 | Posterior N = 780 | Panuveitis N = 759 | Total N = 3,404 |
|---|---|---|---|---|---|
| Ocular involvement (%) | |||||
| Unilateral | 1,184 (70.2) | 68 (38.2) | 569 (72.9) | 449 (59.2) | 2,270 (66.7) |
| Bilateral | 502 (29.8) | 108 (60.7) | 208 (26.7) | 306 (40.3) | 1,124 (33.0) |
| Missing data | 1 (0.1) | 2 (1.1) | 3 (0.4) | 4 (0.5) | 10 (0.2) |
| Course | |||||
| Acute | 859 (50.9) | 55 (30.9) | 452 (57.9) | 275 (36.2) | 1,641 (48.3) |
| Chronic | 421 (25.0) | 83 (46.6) | 192 (24.6) | 329 (43.3) | 1,025 (30.1) |
| Recurrent | 400 (23.7) | 35 (19.7) | 124 (15.9) | 146 (19.2) | 705 (20.7) |
| Missing data | 7 (0.4) | 5 (2.8) | 12 (1.5) | 9 (1.2) | 33 (0.9) |
| Type of Inflammation | |||||
| Non-granulomatous | 1,485 (88.0) | 150 (84.3) | 638 (81.8) | 546 (71.9) | 2,819 (83.0) |
| Granulomatous | 186 (11.0) | 25 (14.0) | 130 (16.7) | 201 (26.5) | 542 (15.9) |
| Missing data | 16 (0.9) | 3 (1.7) | 12 (1.5) | 12 (1.5) | 43 (1.2) |
| Complications at consultation | |||||
| Cataract | 293 (17.3) | 41 (23.0) | 77 (9.9) | 256 (33.7) | 667 (19.7) |
| Glaucoma | 165 (9.8) | 14 (7.9) | 24 (3.1) | 101 (13.3) | 304 (9.0) |
| Macular edema | 75 (4.4) | 28 (15.7) | 35 (4.5) | 125 (16.5) | 263 (7.8) |
| Epiretinal membrane | 38 (2.3) | 17 (9.6) | 43 (5.5) | 72 (9.5) | 170 (5.0) |
| Vitreous hemorrhage | 13 (0.8) | 6 (3.4) | 21 (2.7) | 40 (5.3) | 80 (2.4) |
| Retinal detachment | 18 (1.1) | 15 (8.4) | 64 (8.2) | 138 (18.2) | 235 (6.9) |
| Band keratopathy | 23 (1.4) | 11 (6.2) | 4 (0.5) | 37 (4.9) | 75 (2.2) |
| Bullous keratopathy | 16 (0.9) | 3 (1.7) | 1 (0.1) | 18 (2.4) | 38 (1.1) |
| BCVA (LogMAR) | 0.67 ± 0.75 | 0.76 ± 0.81 | 1.09 ± 0.93 | 1.35 ± 1.04 | 0.96 ± 0.88 |
BCVA Best corrected visual acuity
A specific diagnosis was achieved in 3,252 (95.5%) cases. In 152 (4.5%) of the patients, the cause could not be determined (undetermined uveitis). Overall, idiopathic was the most common cause with 944 patients (27.7%), followed by toxoplasmosis with 858 cases (25.3%) and virus-associated anterior uveitis with 217 cases (6.4%). Regarding gender distribution, females were more commonly affected by idiopathic uveitis than men (60.6% vs 39.4%). On the contrary, men showed a higher prevalence of HLA-B27-associated acute anterior uveitis, accounting for 55.8% compared to 44.2% in women. There was a nearly equal distribution between the sexes for toxoplasmosis, with 433 cases (50.5%) in women and 425 cases (49.5%) in men. (Table 3).
Table 3.
Laterality and gender distribution of uveitis etiologies in Colombia
| Diagnosis | N 3404 | % | Affected eye | Gender distribution | ||
|---|---|---|---|---|---|---|
| Bilateral n (%) | Unilateral n (%) | Female n (%) | Male n (%) | |||
| Idiopathic | 944 | 27.73 | 336 (35.5) | 607 (64.3) | 572 (60.6) | 372 (39.4) |
| Toxoplasmosis | 858 | 25.34 | 179 (20.9) | 679 (79.1) | 433 (50.5) | 425 (49.5) |
| Virus-associated uveitis (confirmed) | 217 | 6.41 | 18 (8.3) | 199 (91.7) | 111 (51.2) | 106 (48.8) |
| HLA-B27 Associated Acute Anterior Uveitis | 165 | 4.87 | 67 (40.6) | 98 (59.4) | 73 (44.2) | 92 (55.8) |
| Undetermined | 152 | 4.5 | 48 (31.6) | 11 (73.0) | 87 (57.2) | 72 (47.4) |
| Pars planitis | 130 | 3.82 | 80 (61.5) | 50 (38.4) | 74 (56.9) | 56 (43.1) |
| Traumatic iritis | 114 | 3.37 | 1 (0.9) | 113 (99.1) | 21 (18.4) | 93 (81.6) |
| Spondyloarthropathies | 83 | 2.42 | 39 (47.0) | 44 (53.0) | 39 (47.0) | 44 (53.0) |
| VKH | 73 | 2.16 | 0 | 73 (100.0) | 60 (82.2) | 13 (17.8) |
| Toxocariasis | 72 | 2.13 | 6 (8.3) | 66 (91.7) | 39 (54.2) | 33 (45.8) |
| Undifferentiated autoinflammatory disease | 67 | 1.98 | 42 (62.7) | 25 (37.3) | 42 (62.7) | 25 (37.3) |
| Fuchs uveitis syndrome | 52 | 1.54 | 14 (26.9) | 38 (73.1) | 31 (59.6) | 21 (40.4) |
| Rheumatoid arthritis | 44 | 1.30 | 24 (54.5) | 20 (45.5) | 37 (84.1) | 7 (15.9) |
| Lens induced uveitis | 39 | 1.15 | 6 (15.4) | 33 (84.6) | 19 (48.7) | 20 (51.3) |
| Juvenile Idiopathic Arthritis | 37 | 1.09 | 29 (78.4) | 8 (21.6) | 26 (70.3) | 11 (29.7) |
| Syphilis | 28 | 0.83 | 9 (32.1) | 19 (67.9) | 15 (53.6) | 13 (46.4) |
| Cytomegalovirus – posterior segment infection | 21 | 0.6 | 9 (42.9) | 12 (57.1) | 3 (14.3) | 18 (85.7) |
| Presumed Ocular Tuberculosis | 21 | 0.62 | 16 (76.2) | 5 (23.8) | 10 (47.6) | 11 (52.4) |
| Granulomatous polyangiitis | 19 | 0.56 | 5 (26.3) | 14 (73.7) | 11 (57.9) | 8 (41.0) |
| SLE | 15 | 0.44 | 8 (53.3) | 7 (46.7) | 14 (93.3) | 1 (7.7) |
| Retinitis pigmentosa | 15 | 0.44 | 13 (86.7) | 2 (13.3) | 6 (40.0) | 9 (60.0) |
| Sarcoidosis (presumed) | 15 | 0.44 | 13 (86.7) | 2 (13.3) | 12 (80.0) | 3 (20.0) |
| Sarcoidosis (definite) | 13 | 0.38 | 11 (84.6) | 2 (15.4) | 11 (84.6) | 2 (15.4) |
| Drug-induced uveitis | 13 | 0.38 | 4 (30.8) | 9 (69.2) | 13 (100.0) | 0 |
| HIV associated | 13 | 0.38 | 7 (53.8) | 6 (46.2) | 2 (15.4) | 11 (84.6) |
| Sjögren syndrome | 13 | 0.38 | 5 (38.5) | 8 (61.5) | 11 (84.6) | 2 (15.4) |
| Posner-Schlossman Syndrome | 12 | 0.35 | 3 (25.0) | 9 (75.0) | 5 (41.7) | 7 (58.3) |
| Behçet's disease | 9 | 0.27 | 6 (66.7) | 3 (33.3) | 4 (44.4) | 5 (55.6) |
| Endophthalmitis (acute) | 9 | 0.27 | 1 (11.1) | 8 (88.9) | 4 (44.4) | 5 (55.6) |
| Serpiginous Choroidopathy | 9 | 0.24 | 7 (77.8) | 2 (22.2) | 4 (44.4) | 5 (55.6) |
| Sympathetic ophthalmia | 9 | 0.27 | 0 | 9 (100.0) | 5 (55.6) | 4 (44.4) |
| Ulcerative colitis | 9 | 0.27 | 5 (55.6) | 4 (44.4) | 6 (66.7) | 3 (33.3) |
| Multiple sclerosis | 8 | 0.24 | 5 (62.5) | 3 (37.5) | 6 (75.0) | 2 (25.0) |
| Virus-associated uveitis (suspected) | 7 | 0.21 | 1 (14.3) | 6 (85.7) | 3 (42.9) | 4 (57.1) |
| IPICS | 6 | 0.17 | 1 (16.6%) | 5 (83.3) | 2 (33.3) | 4 (66.6) |
| Immune recovery uveitis | 5 | 0.15 | 2 (40.0) | 3 (60.0) | 2 (40.0) | 3 (60.0) |
| Eales’ disease | 4 | 0.12 | 2 (50.0) | 2 (50.0) | 2 (50.0) | 2 (50.0) |
| TINU | 4 | 0.12 | 3 (75.0) | 1 (25.0) | 3 (75.0) | 1 (25.0) |
| Birdshot chorioretinopathy | 3 | 0.09 | 3 (100.0) | 0 | 2 (66.7) | 1 (33.3) |
| Cytomegalovirus – anterior segment infection | 3 | (0.09) | 0 | 3 (100.0) | 1 (33.3) | 2 (66.7) |
| Endophthalmitis (chronic) | 3 | 0.09 | 1 (33.3) | 2 (66.7) | 3 (100.0) | 0 |
| Histoplasmosis suspected | 3 | 0.09 | 2 (66.7) | 1 (33.3) | 1 (33.3) | 2 (66.7) |
| Idiopathic multifocal choroiditis | 3 | 0.09 | 3 (100.0) | 0 | 2 (66.7) | 1 (33.3) |
| MEWDS | 3 | 0.06 | 2 (66.7) | 1 (33.3) | 3 (100.0) | 0 |
| Primary intraocular lymphoma | 3 | 0.09 | 2 (66.7) | 1 (33.3) | 1 (33.3) | 2 (66.7) |
| Epstein Barr-Virus | 2 | 0.06 | 1 (50.0) | 1 (50.0) | 1 (50.0) | 1 (50.0) |
| Multifocal Choroiditis and Panuveitis | 2 | 0.06 | 2 (100.0) | 0 | 1 (50.0) | 1 (50.0) |
| Psoriasis | 2 | 0.06 | 1 (50.0) | 1 (50.0) | 0 | 2 (100.0) |
| Relapsing polychondritis | 2 | 0.06 | 1 (50.0) | 1 (50.0) | 2 (100.0) | 0 |
| UGH syndrome | 2 | 0.06 | 0 | 2 (100.0) | 0 | 2 (100.0) |
| AZOOR | 1 | 0.03 | 1 (100.0) | 0 | 1 (100.0) | 0 |
| Blau syndrome | 1 | 0.03 | 1 (100.0) | 0 | 0 | 1 (100.0) |
| Brucellosis suspected | 1 | 0.03 | 0 | 1 (100.0) | 0 | 1 (100.0) |
| CREST Syndrome | 1 | 0.03 | 0 | 1 (100.0) | 1 (100.0) | 0 |
| Crohn’s disease | 1 | 0.03 | 1 (100.0) | 0 | 1 (100.0) | 0 |
| Cryoglobulinemic vasculitis | 1 | 0.03 | 0 | 1 (100.0) | 1 (100.0) | 0 |
| Cysticercosis | 1 | 0.03 | 0 | 1 (100.0) | 0 | 1 (100.0) |
| IRVAN syndrome | 1 | 0.03 | 1 (100.0) | 0 | 0 | 1 |
| Leptospirosis (confirmed) | 1 | 0.03 | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Leptospirosis (suspected) | 1 | 0.03 | 1 (100.0) | 0 | 0 | 1 (100.0) |
| Reactive arthritis | 1 | 0.03 | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Takayasu arteritis | 1 | 0.03 | 1 (100.0) | 0 | 1 (100.0) | 0 |
| Undifferentiated vasculitis | 1 | 0.03 | 0 | 1 (100.0) | 1 (100.0) | 0 |
AZOOR Acute zonal occult outer retinopathy, IPICS idiopathic persistent iritis after cataract surgery, SLE Systemic lupus erythematosus, MEWDS Multiple evanescent white dot syndrome, TINU syndrome Tubulointerstitial nephritis and uveitis syndrome, UGH Uveitis-Glaucoma-Hyphema syndrome, VKH Vogt-Koyanagi-Harada disease
In patients diagnosed with anterior uveitis, idiopathic was the most prevalent cause (n = 684, 40.8%), followed by virus-associated anterior uveitis (11.9%) (Table 4). On the other hand, in patients with intermediate uveitis, pars planitis remained the leading etiology (n = 130, 73%). In posterior uveitis and panuveitis cases, toxoplasmosis was the most prevalent cause (n = 548, 70.3%, and n = 266, 35%, respectively) (Table 4).
Table 4.
Causes of uveitis according to the anatomical site of inflammation
| Diagnosis | N (%) | Anterior N = 1, 687 (%) | Intermediate N = 178 (%) | Posterior N = 780 (%) | Panuveitis N = 759 (%) |
|---|---|---|---|---|---|
| Idiopathic | 944 (27.73) | 684 (40.8) | * | 77 (9.9) | 183 (24.1) |
| Toxoplasmosis | 858 (25.34) | 42 (2.5) | 3 (1.7) | 548 (70.3) | 266 (35.0) |
| Virus-associated uveitis (confirmed) | 217 (6.41) | 199 (11.9) | 3 (1.7) | 0 | 15 (2.0) |
| HLA-B27 Associated Acute Anterior Uveitis | 165 (4.87) | 153 (9.1) | 7 (3.9) | 0 | 5 |
| Undetermined | 152 (4.5) | 89 (58.6) | 8 (5.3) | 18 (11.8) | 37 (24.3) |
| Pars planitis | 130 (3.82) | 0 | 130 (73.0) | 0 | 7 (0.9) |
| Traumatic iritis | 114 (3.37) | 100 (5.9) | 2 (1.1) | 4 (0.5) | 8 (1.1) |
| Spondyloarthropathies | 83 (2.42) | 73 (4.4) | 1 (0.6) | 0 | 9 (1.2) |
| VKH | 73 (2.16) | 4 (0.2) | 1 (0.6) | 5 (0.6) | 63 (8.3) |
| Toxocariasis | 72 (2.13) | 2 (0.1) | 3 (1.7) | 55 (7.1) | 12 (1.6) |
| Undifferentiated autoinflammatory disease | 67 (1.98) | 47 (2.8) | 2 (1.1) | 1 (0.1) | 17 (2.2) |
| Fuchs uveitis syndrome | 52 (1.54) | 49 (2.9) | 2 (1.1) | 0 | 1 (0.1) |
| Rheumatoid arthritis | 44 (1.30) | 34 (2.0) | 1 (0.6) | 0 | 9 (1.2) |
| Lens induced uveitis | 39 (1.15) | 34 (2.0) | 0 | 0 | 5 |
| Juvenile Idiopathic Arthritis | 37 (1.09) | 26 (1.6) | 2 (1.1) | 1 (0.1) | 8 (1.0) |
| Syphilis | 28 (0.83) | 8 (0.5) | 3 (1.7) | 5 (0.6) | 12 (1.6) |
| Cytomegalovirus – posterior segment infection | 21 (0.6) | 0 | 0 | 13 (61.9) | 8 (38.1) |
| Presumed Ocular Tuberculosis | 21 (0.62) | 5 (0.3) | 4 (2.2) | 2 (0.3) | 10 (1.3) |
| Granulomatous polyangiitis | 19 (0.56) | 15 (0.9) | 0 | 0 | 4 (0.5) |
| SLE | 15 (0.44) | 11 | 1 (0.6) | 1 (0.1) | 2 (0.3) |
| Retinitis pigmentosa | 15 (0.44) | 0 | 0 | 13 (1.7) | 2 (0.3) |
| Sarcoidosis (presumed) | 15 (0.44) | 6 (0.4) | 3 (1.7) | 1 (0.1) | 5 (0.7) |
| Sarcoidosis (definite) | 13 (0.38) | 1 (0.1) | 2 (1.1) | 0 | 10 (1.3) |
| Drug-induced uveitis | 13 (0.38) | 10 (0.6) | 1 (0.6) | 1 (0.1) | 1 (0.1) |
| HIV associated | 13 (0.38) | 6 (0.4) | 0 | 3 (0.4) | 4 |
| Sjögren syndrome | 13 (0.38) | 10 (0.6) | 0 | 0 | 3 (0.4) |
| Posner-Schlossman Syndrome | 12 (0.35) | 12 (0.7) | 0 | 0 | 0 |
| Behçet's disease | 9 (0.27) | 5 (0.3) | 0 | 1 (0.1) | 3 (0.4) |
| Endophthalmitis (acute) | 9 (0.27) | 4 (0.2) | 0 | 1 (0.1) | 4 (0.5) |
| Serpiginous Choroidopathy | 9 (0.24) | 0 | 0 | 7 | 2 (0.3) |
| Sympathetic ophthalmia | 9 (0.27) | 0 | 0 | 2 (0.3) | 7 (0.9) |
| Ulcerative colitis | 9 (0.27) | 9 (0.5) | 0 | 0 | 0 |
| Multiple sclerosis | 8 (0.24) | 2 (0.1) | 2 (1.1) | 2 (0.3) | 2 (0.3) |
| Virus-associated uveitis (suspected) | 7 (0.21) | 5 (0.3) | 0 | 0 | 2 (0.3) |
| IPICS | 6 (0.17) | 6 (0.3) | 0 | 0 | 0 |
| Immune recovery uveitis | 5 (0.15) | 3 (0.2) | 1 (0.6) | 0 | 1 (0.1) |
| Eales’ disease | 4 (0.12) | 1 (0.1) | 0 | 3 (0.4) | 0 |
| TINU | 4 (0.12) | 2 (0.1) | 0 | 0 | 2 (0.3) |
| Birdshot chorioretinopathy | 3 (0.09) | 0 | 0 | 0 | 3 (0.4) |
| Cytomegalovirus – anterior segment infection | 3 (0.09) | 3 (0.2) | 0 | 0 | 0 |
| Endophthalmitis (chronic) | 3 (0.09) | 0 | 0 | 1 (0.1) | 2 (0.3) |
| Histoplasmosis suspected | 3 (0.09) | 1 (0.1) | 0 | 1 (0.1) | 1 (0.1) |
| Idiopathic multifocal choroiditis | 3 (0.09) | 0 | 0 | 0 | 3 (0.4) |
| MEWDS | 3 (0.06) | 0 | 0 | 3 (0.4) | 0 |
| Primary intraocular lymphoma | 3 (0.09) | 0 | 0 | 1 (0.1) | 2 (0.3) |
| Epstein Barr-Virus | 2 (0.06) | 0 | 0 | 0 | 2 (0.3) |
| Multifocal Choroiditis and Panuveitis | 2 (0.06) | 0 | 0 | 0 | 2 (0.3) |
| Psoriasis | 2 (0.06) | 0 | 0 | 1 (0.1) | 1 (0.1) |
| Relapsing polychondritis | 2 (0.06) | 2 (0.1) | 0 | 0 | 0 |
| UGH syndrome | 2 (0.06) | 2 (0.1) | 0 | 0 | 0 |
| AZOOR | 1 (0.03) | 0 | 0 | 1 (0.1) | 0 |
| Blau syndrome | 1 (0.03) | 0 | 0 | 0 | 1 (0.1) |
| Brucellosis suspected | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
| CREST Syndrome | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
| Crohn’s disease | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
| Cryoglobulinemic vasculitis | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
| Cysticercosis | 1 (0.03) | 0 | 0 | 1 (0.1) | 0 |
| IRVAN syndrome | 1 (0.03) | 0 | 0 | 1 (0.1) | 0 |
| Leptospirosis (confirmed) | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
| Leptospirosis (suspected) | 1 (0.03) | 0 | 1 (0.6) | 0 | 0 |
| Reactive arthritis | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
| Undifferentiated vasculitis | 1 (0.03) | 1 (0.1) | 0 | 0 | 0 |
AZOOR Acute zonal occult outer retinopathy, IPICS idiopathic persistent iritis after cataract surgery, SLE Systemic lupus erythematosus, MEWDS Multiple evanescent white dot syndrome, TINU syndrome Tubulointerstitial nephritis and uveitis syndrome, UGH syndrome Uveitis-Glaucoma-Hyphema-syndrome, VKH Vogt-Koyanagi-Harada disease, HIV Human immunodeficiency virus, HLA-B27 Human leukocyte antigen B27 *see pars planitis
The age group between 30 and 50 years exhibited the highest prevalence of uveitis, regardless of uveitis localization. In the younger population (< 20 years), posterior uveitis was the most common localization, ranging from 35.5% to 44.6%. Conversely, among individuals over 60 years, anterior uveitis emerged as the most prevalent anatomical localization, ranging from 60.7% to 68.8%. Regarding specific diagnoses, toxoplasmosis was the most frequent in individuals under 40 (26.5% to 44%), while idiopathic cases were more common in those over 40 (29.1% to 49.1%). For detailed data, please refer to Tables 5, 6.
Table 5.
Uveitis anatomical distribution regarding age groups
| Age group | Anterior N = 1,687 | Intermediate N = 178 | Posterior N = 780 | Panuveitis N = 759 |
|---|---|---|---|---|
| 0–9 | 12 (14.5) | 12 (14.5) | 37 (44.6) | 22 (26.5) |
| 10.-19 | 64 (24.2) | 51 (19.2) | 94 (35.5) | 56 (21.1) |
| 20–29 | 143 (31.8) | 22 (4.9) | 167 (37.1) | 118 (26.2) |
| 30–39 | 252 (43.9) | 23 (4.0) | 147 (25.6) | 152 (26.5) |
| 40–49 | 337 (56.4) | 24 (4.2) | 105 (18.2) | 123 (21.3) |
| 50–59 | 348 (59.8) | 17 (3.0) | 91 (16.1) | 119 (21.1) |
| 60–69 | 269 (60.7) | 19 (4.3) | 71 (16.0) | 84 (19.0) |
| 70–79 | 185 (65.6) | 6 (2.1) | 43 (15.2) | 48 (17.0) |
| > 80 | 77 (68.8) | 1 (0.9) | 16 (14.3) | 18 (16.1) |
*48 patients had not reported their age in the clinical record
Table 6.
Causes of uveitis by age in Colombia
| Diagnosis | 0–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | > 80 |
|---|---|---|---|---|---|---|---|---|---|
| N = 83 | N = 265 | N = 450 | N = 574 | N = 589 | N = 575 | N = 443 | N = 282 | N = 112 | |
| Idiopathic | 15 (1.6) | 47 (5.0) | 99 (10.5) | 139 (14.7) | 160 (17.0) | 160 (17.0) | 143 (15.1) | 118 (12.5) | 54 (5.7) |
| Toxoplasmosis | 22 (26.5) | 88 (33.2) | 198 (44.0) | 197 (34.3) | 119 (20.6) | 102 (18.1) | 74 (16.7) | 40 (14.2) | 12 (10.7) |
| Virus-associated uveitis (confirmed) | 1 (1.2) | 8 (3.0) | 20 (4.4) | 34 (5.9) | 36 (6.2) | 39 (6.9) | 42 (9.5) | 24 (8.5) | 11 (9.8) |
| HLA-B27 Associated Acute Anterior Uveitis | 2 (2.4) | 4 (1.5) | 15 (3.3) | 30 (5.2) | 42 (7.3) | 40 (7.1) | 19 (4.3) | 9 (3.2) | 2 (1.8) |
| Undetermined | 2 (2.4) | 7 (2.6) | 7 (1.6) | 24 (4.2) | 25 (4.2) | 29 (5.0) | 24 (5.4) | 22 (7.8) | 4 (3.5) |
| Pars planitis | 10 (13.0) | 42 (32.3) | 19 (14.6) | 18 (13.8) | 17 (13.1) | 8 (6.2) | 11 (8.5) | 3 (2.3) | 1 (0.8) |
| Traumatic iritis | 1 (1.2) | 6 (2.3) | 19 (4.2) | 26 (4.5) | 33 (5.6) | 14 (2.5) | 8 (1.8) | 4 (1.4) | 3 (2.7) |
| Spondyloarthropathies | 0 | 0 | 7 (1.6) | 11 (1.9) | 26 (4.5) | 17 (3.0) | 16 (3.6) | 6 (2.1) | 0 |
| VKH | 0 | 3 (1.1) | 10 (2.2) | 10 (1.7) | 19 (3.3) | 19 (3.4) | 7 (1.6) | 3 (1.1) | 0 |
| Toxocariasis | 12 (14.5) | 26 (9.8) | 17 (3.8) | 8 (1.4) | 5 (0.9) | 3 (0.5) | 0 | 1 (0.4) | 0 |
| Undifferentiated autoinflammatory disease | 1 (1.2) | 6 (2.3) | 1 (0.2) | 13 (2.3) | 12 (2.1) | 18 (3.2) | 13 (2.9) | 3 (1.1) | 0 |
| Fuchs uveitis syndrome | 0 | 0 | 1 (0.2) | 11 | 11 (1.9) | 16 (2.8) | 6 (1.4) | 4 (1.4) | 3 (2.7) |
| Rheumatoid arthritis | 0 | 0 | 1 (0.2) | 1 (0.2) | 2 (0.3) | 3 (0.5) | 3 (0.7) | 3 (1.1) | 2 (1.8) |
| Lens induced uveitis | 0 | 0 | 0 | 3 (0.5) | 4 (0.7) | 7 (1.2) | 9 (2.0) | 13 (4.6) | 3 (2.7) |
| Juvenile Idiopathic Arthritis | 10 (12.0) | 17 (6.4) | 7 (1.6) | 0 | 2 (0.3) | 1 (0.2) | 0 | 0 | 0 |
| Syphilis | 0 | 0 | 3 (0.7) | 3 (0.5) | 5 (0.9) | 8 (1.4) | 4 (0.9) | 3 (1.1) | 2 (1.8) |
| Cytomegalovirus – posterior segment infection | 1 (1.2) | 0 | 1 (0.2) | 7 (1.2) | 8 (1.4) | 4 (0.7) | 0 | 0 | 0 |
| Presumed Ocular Tuberculosis | 2 (2.4) | 0 | 3 (0.7) | 2 (0.3) | 4 (0.7) | 3 (0.5) | 6 (1.4) | 1 (0.4) | 0 |
| Granulomatous polyangiitis | 0 | 0 | 0 | 2 (0.3) | 3 (0.5) | 5 (0.9) | 4 (0.9) | 2 (0.7) | 3 (2.7) |
| SLE | 0 | 0 | 0 | 0 | 2 (0.3) | 2 (0.4) | 5 (1.1) | 3 (1.1) | 0 |
| Retinitis pigmentosa | 0 | 0 | 0 | 0 | 0 | 1 (0.2) | 1 (0.2) | 0 | 0 |
| Sarcoidosis (presumed) | 1 (1.2) | 2 (0.8) | 0 | 2 (0.3) | 1 (0.2) | 3 (0.5) | 3 (0.7) | 0 | 1 (0.9) |
| Sarcoidosis (definite) | 0 | 0 | 0 | 4 (0.7) | 9 (1.6) | 12 (2.1) | 14 (3.2) | 4 (1.4) | 1 (0.9) |
| Drug-induced uveitis | 0 | 0 | 0 | 2 (0.3) | 0 | 7 (1.2) | 4 (0.9) | 0 | 0 |
| HIV associated | 0 | 0 | 2 (0.4) | 3 (0.5) | 2 (0.3) | 4 (0.7) | 2 (0.5) | 0 | 0 |
| Sjögren syndrome | 0 | 0 | 1 (0.2) | 1 (0.2) | 0 | 3 (0.5) | 3 (0.7) | 0 | 1 (0.9) |
| Posner-Schlossman Syndrome | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 2 (0.7) | 1 (0.9) |
| Behçet's disease | 0 | 0 | 2 (0.4) | 3 (0.5) | 0 | 4 (0.7) | 0 | 0 | 0 |
| Endophthalmitis (acute) | 0 | 0 | 1 (0.2) | 0 | 0 | 2 (0.4) | 2 (0.5) | 2 (0.7) | 2 (1.8) |
| Serpiginous Choroidopathy | 1 (1.2) | 3 (1.1) | 1 (0.2) | 1 (0.2) | 3 (0.5) | 1 (0.2) | 2 (0.5) | 2 (0.7) | 1 (0.9) |
| Sympathetic ophthalmia | 0 | 0 | 0 | 1 (0.2) | 2 (0.3) | 4 (0.7) | 1 (0.2) | 1 (0.4) | 0 |
| Ulcerative colitis | 0 | 0 | 0 | 2 (0.3) | 2 (0.3) | 1 (0.2) | 2 (0.5) | 1 (0.4) | 1 (0.9) |
| Multiple sclerosis | 0 | 0 | 1 (0.2) | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
| Virus-associated uveitis (suspected) | 0 | 1 (0.4) | 1 (0.2) | 0 | 1 (0.2) | 2 (0.4) | 1 (0.2) | 0 | 0 |
| IPICS | 0 | 2 (0.5) | 0 | 0 | 0 | 0 | 2 (0.5) | 0 | 2 (0.5) |
| Immune recovery uveitis | 0 | 0 | 0 | 1 (0.2) | 3 (0.5) | 1 (0.2) | 0 | 0 | 0 |
| Eales’ disease | 0 | 0 | 1 (0.2) | 0 | 1 (0.2) | 1 (0.2) | 1 (0.2) | 0 | 0 |
| TINU | 1 (1.2) | 1 (0.4) | 0 | 0 | 1 (0.2) | 0 | 1 (0.2) | 0 | 0 |
| Birdshot chorioretinopathy | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 2 (0.7) | 0 |
| Cytomegalovirus – anterior segment infection | 0 | 0 | 0 | 2 (0.3) | 0 | 0 | 0 | 1 (0.4) | 0 |
| Endophthalmitis (chronic) | 0 | 0 | 0 | 0 | 0 | 1 (0.2) | 1 (0.2) | 1 (0.4) | 0 |
| Histoplasmosis suspected | 0 | 0 | 1 (0.2) | 0 | 1 (0.2) | 0 | 0 | 0 | 1 (0.9) |
| Idiopathic multifocal choroiditis | 0 | 0 | 0 | 1 (0.2) | 0 | 2 (0.4) | 0 | 0 | 0 |
| MEWDS | 0 | 1 (0.4) | 0 | 2 (0.3) | 3 (0.5) | 5 (0.9) | 2 (0.5) | 1 (0.4) | 1 (0.9) |
| Primary intraocular lymphoma | 0 | 0 | 1 (0.2) | 1 (0.2) | 3 (0.5) | 6 (1.1) | 1 (0.2) | 0 | 0 |
| Epstein Barr-Virus | 0 | 0 | 0 | 1 | 0 | 0 | 1 (0.2) | 0 | 0 |
| Multifocal Choroiditis and Panuveitis | 0 | 0 | 1 (0.2) | 1 (0.2) | 0 | 0 | 1 (0.2) | 0 | 0 |
| Psoriasis | 0 | 0 | 0 | 0 | 1 (0.2) | 1 (0.2) | 0 | 1 (0.4) | 0 |
| Relapsing polychondritis | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 |
| UGH syndrome | 0 | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 1 (0.4) | 0 |
| AZOOR | 0 | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 0 |
| Blau syndrome | 1 (1.2) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Brucellosis suspected | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 | 0 | 0 |
| CREST Syndrome | 0 | 0 | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 |
| Crohn’s disease | 0 | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 0 |
| Cryoglobulinemic vasculitis | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Cysticercosis | 0 | 1 (0.4) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| IRVAN syndrome | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 | 0 | 0 |
| Leptospirosis (confirmed) | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 | 0 | 0 |
| Leptospirosis (suspected) | 0 | 1 (0.4) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Reactive arthritis | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 | 1 (0.4) | 0 |
| Takayasu arteritis | 0 | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 |
| Undifferentiated vasculitis | 0 | 0 | 0 | 1 (0.2) | 0 | 0 | 0 | 0 | 0 |
AZOOR Acute zonal occult outer retinopathy, IPICS idiopathic persistent iritis after cataract surgery, SLE Systemic lupus erythematosus, MEWDS Multiple evanescent white dot syndrome, TINU syndrome Tubulointerstitial nephritis and uveitis syndrome, UGH syndrome Uveitis-Glaucoma-Hyphema-syndrome, VKH Vogt-Koyanagi-Harada disease, HIV Human immunodeficiency virus, HLA-B27 Human leukocyte antigen B27
Discussion
In Colombia, two prior studies have focused on the epidemiology of uveitis. The first was conducted in 2009, encompassing 693 patients from two centers in Bogotá [24]. The second was conducted in 2023 by Polania et al., evaluating 489 patients from a single private center in Bogotá [9]. In the current study, patients from the Polania et al. study were incorporated and combined with six other referral centers from various Colombian cities.
In accordance with prior literature, the demographic group most significantly affected is working-age individuals [25, 26]. The mean age at uveitis diagnosis in our study population was 41.1 years, closely mirroring the findings of a previous single-center report [9]. However, a notable divergence exists in the mean duration between symptom onset and diagnosis, with the current study reporting 5.4 years compared to the previous report's 3.7 years. This discrepancy is concerning, given the substantial burden that delayed treatment initiation can impose in cases of uveitis.
The significant delay between the onset of uveitis symptoms and its diagnosis in Colombia may be attributed to the scarcity of uveitis specialists in the country. This leads to initial referrals of uveitis patients to general ophthalmologists or retina specialists, ultimately resulting in delayed diagnosis and treatment. The frequency of complications related to anatomical localization of uveitis is presented in Table 2.
Regional differences were observed in the time from the initial uveitis presentation to diagnosis. Cali reported an average diagnosis time of 3.53 ± 6.88 years, while Bucaramanga had a lower average of 1.29 ± 3.44 years. Conversely, Bogotá exhibited a considerably a higher diagnosis time of 6.23 ± 6.28 years. This divergence can be attributed to the fact that Bogotá is the most populated city, where the waiting time to be attended could be longer due to high demand and low number of specialists [27].
Although Polania et al. found a higher incidence of uveitis among females [9], the present study shows similar proportions between males and females, similar to what other studies have reported [28]. Including more centers in this study contributes to the heightened representability of uveitis characteristics, which could account for the observed sex differences [29, 30]. Specifically, our study found a higher occurrence of idiopathic uveitis in females (60%). This observation suggests a potential link to the hypothesis that idiopathic uveitis may be influenced by underlying non-infectious conditions and the role of female hormones in stimulating autoimmune responses where inflammation plays a vital role [31]. However, further comprehensive research is essential to fully understand and substantiate these associations.
In the 2009 study, the prevailing characteristics of uveitis included a predominance of unilateral cases (73.4%), an acute clinical course (68.3%), and a non-granulomatous nature (90.6%) [24]. In contrast, Polania et al. in 2023 reported a shift with a higher prevalence of bilateral involvement (52.8%), recurrent presentations (47.6%), and a persistent non-granulomatous pattern (90.8%) [9]. In the current study, the most frequently encountered type of uveitis remains unilateral (66.7%), presenting acutely (48.3%) and maintaining a non-granulomatous nature (83.0%). These consistent features are typically associated with idiopathic uveitis, which emerged as the most prevalent etiology in our study.
Regarding the specific diagnoses, idiopathic uveitis emerged as the most prevalent cause, with toxoplasmosis occupying the second position and virus-associated uveitis ranking third. This pattern of idiopathic uveitis as the predominant etiology is consistent with findings from studies conducted in developed and developing countries [32–38]. This study reinforces the transition in the predominant causes of uveitis in Colombia from infectious to immune-mediated etiologies [9].
Ocular toxoplasmosis remains one of the major causes of uveitis in South America. This is expected due to the higher seroprevalence of Toxoplasma gondii in South American countries (45.2%) compared to other regions like Europe (30%) or Western Pacific (11.2%) [39]. Also, clinical presentation tends to be more severe than in other regions [40, 41]. In Colombia, 47.1% of the population have positive IgG titers against Toxoplasma gondii and 10.5% of the population have reticochoroidal scars [42]. A nationwide population-based study, found an increasing trend in toxoplasmosis incidence between 2015 and 2019 [43]. This highlights the importance of ongoing patient education about Toxoplasma gondii infection. In this context, adhering to practical clinical guidelines is crucial [44].
For anterior uveitis, idiopathic etiology remained the primary cause, followed by virus-related etiologies such as Herpes simplex or zoster and HLA-B27-associated uveitis. Other studies in Colombia similarly report idiopathic uveitis as the leading cause [9]. The higher prevalence of virus-related uveitis in the present study compared to the study conducted by Polania et al. in 2023 could be attributed to the multicenter nature of the current study. This study included several geographic regions, each with differing prevalence of viral diseases, potentially influencing the observed increase [45].
For posterior uveitis and panuveitis, toxoplasmosis remained the primary cause; numerous factors contribute to this, including the Colombian geographical localization in a tropical area with high rainfall (pluviosity) [46] and the presence of certain strains with virulence factors like rhoptry virulent-alleles of proteins (ROP) 16 and ROP 18 [40, 41].
Intermediate uveitis was the least common localization of uveitis, accounting for only 5.2% of the cases, and it was most frequently associated with an idiopathic etiology (pars planitis); this aligns with the typical pattern observed in intermediate uveitis epidemiological data [32, 33, 35–38, 47]. Some studies report diseases like sarcoidosis, multiple sclerosis, and intraocular lymphoma as possible causes of intermediate uveitis [25, 48]. Although these diseases were present in our cohort, they did not represent a significant number of intermediate uveitis [4]. Etiological diagnosis of intermediate uveitis varies between age groups. In children, Pars planitis accounts for most of the cases; this was also observed in this study [49, 50]. Conversely, in older populations (> 70 years old), suspicion of other etiologies like Primary intraocular lymphoma (PIOL) must be considered; [51] the setting of molecular and pathological diagnosis greatly influences the rate of lymphoma detection, in this cohort, PIOL presents as posterior inflammation (1 case) or panuveitis (2 cases). However, we acknowledge the setting of molecular and pathological diagnosis greatly influences the rate of lymphoma detection [52].
Regarding regional variances, anterior uveitis prevailed as the primary localization in Bucaramanga, Cali, and Medellín, in line with global literature [53–55]. However, in Bogotá, posterior uveitis was the most frequently observed, accounting for 29.7% of cases. This divergence can be attributed to the specialization of one of the Bogotá centers in treating toxoplasmosis.
In patients under 16 years, posterior uveitis was the most frequent localization, a pattern attributed to toxoplasmosis being the primary etiology in this age group. As age increased, the frequency of anterior uveitis rose, reaching a peak in the age group between 40 and 60 years, after which it decreased. In the 2009 Colombian study, panuveitis was the most common localization in young and middle-aged adults (16–50 years) [24]. However, the study of Polanía et al. also evidences a change to anterior uveitis [9]. This may be attributed to an increase in idiopathic cases where anterior uveitis was the most common localization and a greater capacity to perform the test for HLA-B27 + identification.
In patients over 50 years old, anterior uveitis remained the predominant localization [9]. This could be associated with increased idiopathic cases and virus-associated uveitis, where anterior uveitis was more commonly observed. Specifically, the incidence of Herpes zoster ophthalmicus in Colombia increased from 0.85 to 1.35 per 100,000 persons between 2015 and 2019, with people over 50 most affected [45].
Compared with other multicenter, population-based studies worldwide, our findings align with the observation that working-age females are predominantly affected, especially for non-infectious conditions. In a study encompassing 3,000 patients in the UK, Jones identified a clear preference for the female gender in cases of Juvenile idiopathic arthritis-associated uveitis (78%), Punctate Inner Choroidopathy (76%), and Chronic Anterior Uveitis (62%) [56]. In our analysis, females significantly outnumbered males in conditions such as Multiple evanescent white dot syndrome (100%), Vogt-Koyanagi-Harada syndrome (82.2%), Multiple Sclerosis (75%), and idiopathic etiology (60%). Conversely, males showed a higher prevalence of trauma iritis (81.6%), IPICS (66%), and infectious causes like Human Immunodeficiency Virus (89.6%) and Acute Retinal Necrosis (78.8%). Different factors could contribute to these differences, including genetics, sex hormones, and social factors [57–59].
Anterior uveitis is the more prevalent localization in both the Western [53, 56] and Eastern world, [54, 55], with idiopathic etiology leading the list, trailed by infectious and non-infectious [54]. However, distinct patterns emerge in certain developing countries. For instance, Brazil reported a deviation from this trend, with posterior uveitis accounting for most cases (43.1%); [26], although this was observed in 1,053 patients, they were all from a single center. Similarly, in Colombia, posterior uveitis was the most common localization decades ago [24]. Nevertheless, this study noted a recent increase in cases of anterior uveitis. This shift is explained by the increase in idiopathic cases, which were commonly anterior.
To rule out an infectious etiology is a pivotal step of uveitis diagnosis and treatment, then it is essential to know the main etiologies according to the geographical prevalence. In South America, toxoplasmosis remains the predominant infectious cause, with viral anterior uveitis following closely. This aligns with other South American countries where toxoplasmosis accounts for 24.03% of all uveitis cases [26]. However, it differs from Asian countries where ocular tuberculosis is more prevalent compared to our population (19.6% vs. 0.3%) [54]. Other infections, such as syphilis, although not the most common, must always be ruled out [55].
The main strength of this study is the multicenter methodology across different cities in Colombia, providing a comprehensive description of uveitis. Prior research has often relied on small samples from tertiary centers or focused solely on specific causes, limiting their generalizability. Our study includes seven referral centers from four main cities in Colombia, providing a comprehensive representation of patients from the central regions of the country (where most of the population is located) (Fig. 2). Uveitis is generally an alarming entity that forces patients to consult and in most cases general ophthalmologists refer patients to the uveitis specialist, so we estimate that many of the patients who live in cities other than the evaluated surely consulted in one of these centers, which reduces the potential loss of cases.
Our study has some limitations. Due to economic and accessibility disparities among the country's regions, the potential for selection bias cannot be entirely ruled out. Nonetheless, by encompassing private and public centers in our study, we aimed to reduce this risk, considering the extensive coverage reported by the Colombian health system (97.78%). Furthermore, as our data was gathered from tertiary referral centers, there is a potential for overestimating rarer etiologies and underestimating cases of uveitis that are easily treatable. Moreover, previous Colombian studies reported the prevalence of an undetermined etiology at around 16.5% and 21.6%, but in our study, it was only 4.5% [9, 24]. Therefore, we acknowledge the possibility that some undetermined cases could have been mistakenly categorized as idiopathic. However, given that experienced uveitis specialists conducted most diagnoses, and the data was meticulously recorded by knowledgeable personnel following the SUN criteria, the likelihood of this risk is minimized. Moreover, we report diagnoses like rheumatoid arthritis, systemic lupus erythematosus, and antiphospholipid syndrome. However, these diseases should be understood as possible systemic associated conditions to uveitis and not as a direct cause [9, 60–63].
In conclusion, this is the most extensive multicenter study conducted in South America, focusing on the epidemiology of uveitis. Infectious uveitis remains the most common etiology, with ocular toxoplasmosis as the most frequent cause. However, compared to previous studies, an increase in non-infectious conditions was also observed. This study emphasizes the importance of conducting multicenter research to identify changes in the patterns of uveitis and keep updated the epidemiological knowledge of these group of diseases.
Abbreviations
- JIA
Juvenile idiopathic arthritis
- AZOOR
Acute zonal occult outer retinopathy
- BCVA
Best-corrected visual acuity
- HIV
Human Immunodeficiency Virus
- HLA-B27
Human leukocyte antigen B27
- IOL
Intra-ocular lens
- IPICS
Idiopathic persistent iritis after cataract surgery
- MEWDS
Multiple evanescent white dot syndrome
- PIOL
Primary intraocular lymphoma
- SUN
Standardization of uveitis nomenclature
- STROBE
Strengthening the reporting of observational studies in epidemiology
- SLE
Systemic lupus erythematosus
- TINU syndrome
Tubulointerstitial nephritis and uveitis syndrome
- UGH
Uveitis-Glaucoma-Hyphema syndrome
- VKH
Vogt-Koyanagi-Harada disease
Author contribution
All authors attest that they meet the current ICMJE criteria for Authorship.
Funding
Open Access funding provided by Colombia Consortium. This research has not received specific aid from public sector agencies, the commercial sector, or non-profit entities.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Declarations
Ethics approval
This study was approved by the Ethics Committee of Universidad del Rosario under the reference DVO005 2101—CV1615. Additionally, this study adheres to the ethical principles for human research established by the Helsinki Declaration, the Belmont Report, and Colombian Resolution 008430 of 1993.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Luca C, Raffaella A, Sylvia M et al (2017) Changes in patterns of uveitis at a tertiary referral center in Northern Italy: analysis of 990 consecutive cases. Int Ophthalmol. 10.1007/s10792-016-0434-x 10.1007/s10792-016-0434-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rathinam S, Babu M (2013) Algorithmic approach in the diagnosis of uveitis. Indian J Ophthalmol 61:255. 10.4103/0301-4738.114092 10.4103/0301-4738.114092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Albini TA, Rice JB, White AG et al (2020) Economic burden of Non-Infectious Inflammatory Eye Disease (NIIED) in a commercially-insured population in the United States. Ocul Immunol Inflamm 28:164–174. 10.1080/09273948.2018.1560476 10.1080/09273948.2018.1560476 [DOI] [PubMed] [Google Scholar]
- 4.Tsirouki T, Dastiridou A, Symeonidis C et al (2018) A focus on the epidemiology of uveitis. Ocul Immunol Inflamm 26:2–16. 10.1080/09273948.2016.1196713 10.1080/09273948.2016.1196713 [DOI] [PubMed] [Google Scholar]
- 5.Gritz D (2004) Incidence and prevalence of uveitis in Northern California The Northern California Epidemiology of Uveitis Study. Ophthalmology 111:491–500. 10.1016/j.ophtha.2003.06.014 10.1016/j.ophtha.2003.06.014 [DOI] [PubMed] [Google Scholar]
- 6.Mezei G, Chang ET, Mowat FS, Moolgavkar SH (2021) Comments on a recent case-control study of malignant mesothelioma of the pericardium and the tunica vaginalis testis. Scand J Work Environ Health 47:85–86. 10.5271/sjweh.3909 10.5271/sjweh.3909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Acharya NR, Tham VM, Esterberg E et al (2013) Incidence and prevalence of uveitis: results from the pacific ocular inflammation study. JAMA Ophthalmol 131:1405. 10.1001/jamaophthalmol.2013.4237 10.1001/jamaophthalmol.2013.4237 [DOI] [PubMed] [Google Scholar]
- 8.Hart CT, Zhu EY, Crock C et al (2019) Epidemiology of uveitis in urban Australia. Clin Exp Ophthalmol ceo.13517. 10.1111/ceo.13517 [DOI] [PubMed]
- 9.Polanía D, Reyes-Guanes J, Rojas-Carabali W et al (2023) A new look into uveitis in Colombia: changes in distribution patterns and clinical characteristics over the last 25 years. Graefes Arch Clin Exp Ophthalmol 261:561–573. 10.1007/s00417-022-05796-2 10.1007/s00417-022-05796-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.(2005) Standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. Am J Ophthalmol 140:509–516. 10.1016/j.ajo.2005.03.057 [DOI] [PMC free article] [PubMed]
- 11.Davis JL, Madow B, Cornett J et al (2010) Scale for photographic grading of vitreous haze in uveitis. Am J Ophthalmol 150:637-641.e1. 10.1016/j.ajo.2010.05.036 10.1016/j.ajo.2010.05.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.The Standardization of Uveitis Nomenclature (Sun) Working Group (2021) Classification criteria for sarcoidosis-associated uveitis. Am J Ophthalmol 228:220–230.10.1016/j.ajo.2021.03.047 [DOI] [PMC free article] [PubMed]
- 13.Mochizuki M, Smith JR, Takase H et al (2019) Revised criteria of International Workshop on Ocular Sarcoidosis (IWOS) for the diagnosis of ocular sarcoidosis. Br J Ophthalmol 103:1418–1422. 10.1136/bjophthalmol-2018-313356 10.1136/bjophthalmol-2018-313356 [DOI] [PubMed] [Google Scholar]
- 14.Baarsma GS, La Hey E, Glasius E et al (1987) The predictive value of serum angiotensin converting enzyme and lysozyme levels in the diagnosis of ocular sarcoidosis. Am J Ophthalmol 104:211–217. 10.1016/0002-9394(87)90406-5 10.1016/0002-9394(87)90406-5 [DOI] [PubMed] [Google Scholar]
- 15.Borciuch C, El-Jammal T, Kodjikian L et al (2024) Value of chest x-ray and chest computed tomography for systemic sarcoidosis diagnosis in undifferentiated uveitis. Ocul Immunol Inflamm 32:161–167. 10.1080/09273948.2023.2226203 10.1080/09273948.2023.2226203 [DOI] [PubMed] [Google Scholar]
- 16.Mao L, Dhar A, Meng G et al (2022) Blau syndrome NOD2 mutations result in loss of NOD2 cross-regulatory function. Front Immunol 13:988862. 10.3389/fimmu.2022.988862 10.3389/fimmu.2022.988862 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Agrawal R, Agarwal A, Jabs DA et al (2020) Standardization of nomenclature for ocular tuberculosis – Results of Collaborative Ocular Tuberculosis Study (COTS) Workshop. Ocul Immunol Inflamm 28:74–84. 10.1080/09273948.2019.1653933 10.1080/09273948.2019.1653933 [DOI] [PubMed] [Google Scholar]
- 18.Soifer M, Mousa HM, Jammal AA et al (2022) Diagnosis and management of Idiopathic Persistent Iritis after Cataract Surgery (IPICS). Am J Ophthalmol 234:250–258. 10.1016/j.ajo.2021.10.004 10.1016/j.ajo.2021.10.004 [DOI] [PubMed] [Google Scholar]
- 19.Fekri S, Barzanouni E, Samiee S, Soheilian M (2023) Polymerase chain reaction test for diagnosis of infectious uveitis. Int J Retin Vitr 9:26. 10.1186/s40942-023-00465-w 10.1186/s40942-023-00465-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rangel CM, Restrepo-Arango M, Mejía-Salgado G et al (2023) Acute retinal necrosis: experience in a reference center in Santander – Colombia. Ocul Immunol Inflamm 1–9. 10.1080/09273948.2023.2244076 [DOI] [PubMed]
- 21.Goh EJH, Putera I, La Distia NR et al (2023) Ocular toxoplasmosis. Ocul Immunol Inflamm 31:1342–1361. 10.1080/09273948.2022.2117705 10.1080/09273948.2022.2117705 [DOI] [PubMed] [Google Scholar]
- 22.(2021) Classification criteria for pars planitis. Am J Ophthalmol 228:268–274. 10.1016/j.ajo.2021.03.045 [DOI] [PMC free article] [PubMed]
- 23.McGonagle D, McDermott MF (2006) A Proposed Classification of the Immunological Diseases. PLoS Med 3:e297. 10.1371/journal.pmed.0030297 10.1371/journal.pmed.0030297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.de-la-Torre A, López-Castillo CA, Rueda JC et al (2009) Clinical patterns of uveitis in two ophthalmology centres in Bogota, Colombia. Clin Exp Ophthalmol 37:458–466.10.1111/j.1442-9071.2009.02082.x [DOI] [PubMed]
- 25.Liberman P, Gauro F, Berger O, Urzua CA (2015) Causes of uveitis in a tertiary center in Chile: a cross-sectional retrospective review. Ocul Immunol Inflamm 23:339–345. 10.3109/09273948.2014.981548 10.3109/09273948.2014.981548 [DOI] [PubMed] [Google Scholar]
- 26.Gonzalez Fernandez D, Nascimento H, Nascimento C et al (2017) Uveitis in São Paulo, Brazil: 1053 new patients in 15 months. Ocul Immunol Inflamm 25:382–387. 10.3109/09273948.2015.1132741 10.3109/09273948.2015.1132741 [DOI] [PubMed] [Google Scholar]
- 27.Amaya J, Beltrán A, Chavarro D et al (2013) Estudio de disponibilidad y distribución de la oferta de médicos especialistas, en servicios de alta y mediana complejidad en Colombia. https://www.minsalud.gov.co/salud/Documents/Observatorio%20Talento%20Humano%20en%20Salud/DisponibilidadDistribuciónMdEspecialistasCendex.pdf. Accessed 20 Oct 2023
- 28.Miserocchi E, Fogliato G, Modorati G, Bandello F (2013) Review on the worldwide epidemiology of uveitis. Eur J Ophthalmol 23:705–717. 10.5301/ejo.5000278 10.5301/ejo.5000278 [DOI] [PubMed] [Google Scholar]
- 29.Heiligenhaus A, Minden K, Föll D, Pleyer U (2015) Uveitis in juvenile idiopathic arthritis. Dtsch Arztebl Int. 10.3238/arztebl.2015.0092 10.3238/arztebl.2015.0092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rothova A, Buitenhuis HJ, Meenken C et al (1992) Uveitis and systemic disease. Br J Ophthalmol 76:137–141. 10.1136/bjo.76.3.137 10.1136/bjo.76.3.137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yeung IYL, Popp NA, Chan C-C (2015) The role of sex in uveitis and ocular inflammation. Int Ophthalmol Clin 55:111–131. 10.1097/IIO.0000000000000072 10.1097/IIO.0000000000000072 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.ÇakarÖzdal MP, Yazici A, Tüfek M, Öztürk F (2014) Epidemiology of uveitis in a referral hospital in Turkey. Turk J Med Sci 44:337–342. 10.3906/sag-1302-132 10.3906/sag-1302-132 [DOI] [PubMed] [Google Scholar]
- 33.Silpa-archa S, Noonpradej S, Amphornphruet A (2015) Pattern of uveitis in a referral ophthalmology center in the central district of Thailand. Ocul Immunol Inflamm 23:320–328. 10.3109/09273948.2014.943773 10.3109/09273948.2014.943773 [DOI] [PubMed] [Google Scholar]
- 34.Zheng Y, Zhang L-X, Meng Q-L et al (2015) Clinical patterns and characteristics of uveitis in a secondary hospital in southern China. Int J Ophthalmol 8:337–341. 10.3980/j.issn.2222-3959.2015.02.22 10.3980/j.issn.2222-3959.2015.02.22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Dogra M, Singh R, Agarwal A et al (2017) Epidemiology of uveitis in a tertiary-care Referral Institute in North India. Ocul Immunol Inflamm 25:S46–S53. 10.1080/09273948.2016.1255761 10.1080/09273948.2016.1255761 [DOI] [PubMed] [Google Scholar]
- 36.Siak J, Kumaradas M, Chee S-P (2017) The pattern of uveitis in Sri Lanka. Ocul Immunol Inflamm 25:S63–S68. 10.1080/09273948.2017.1313991 10.1080/09273948.2017.1313991 [DOI] [PubMed] [Google Scholar]
- 37.Abaño JM, Galvante PR, Siopongco P et al (2017) Review of epidemiology of uveitis in Asia: pattern of uveitis in a tertiary hospital in the Philippines. Ocul Immunol Inflamm 25:S75–S80. 10.1080/09273948.2017.1335755 10.1080/09273948.2017.1335755 [DOI] [PubMed] [Google Scholar]
- 38.Nguyen M, Siak J, Chee S-P, Diem VQH (2017) The spectrum of uveitis in southern Vietnam. Ocul Immunol Inflamm 25:S100–S106. 10.1080/09273948.2016.1231826 10.1080/09273948.2016.1231826 [DOI] [PubMed] [Google Scholar]
- 39.Bigna JJ, Tochie JN, Tounouga DN et al (2020) Global, regional, and country seroprevalence of Toxoplasma gondii in pregnant women: a systematic review, modelling and meta-analysis. Sci Rep 10:12102. 10.1038/s41598-020-69078-9 10.1038/s41598-020-69078-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Alvarez C, de-la-Torre A, Vargas M et al (2015) Striking divergence in Toxoplasma ROP16 nucleotide sequences from human and meat samples. J Infect Dis 211:2006–2013.10.1093/infdis/jiu833 [DOI] [PubMed]
- 41.Sánchez V, de-la-Torre A, Gómez-Marín JE (2014) Characterization of ROP18 alleles in human toxoplasmosis. Parasitol Int 63:463–469.10.1016/j.parint.2013.10.012 [DOI] [PubMed]
- 42.Gómez-Marín JE, Muñoz-Ortiz J, Mejía-Oquendo M et al (2021) High frequency of ocular toxoplasmosis in Quindío, Colombia and risk factors related to the infection. Heliyon 7:e06659. 10.1016/j.heliyon.2021.e06659 10.1016/j.heliyon.2021.e06659 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cifuentes-González C, Zapata-Bravo E, Sierra-Cote MC et al (2022) Colombian Ocular Infectious Epidemiology Study (COIES): ocular toxoplasmosis incidence and sociodemographic characterization, 2015–2019. Int J Infect Dis 117:349–355. 10.1016/j.ijid.2022.02.028 10.1016/j.ijid.2022.02.028 [DOI] [PubMed] [Google Scholar]
- 44.Ministerio de Salud y Protección Social (2013) Guías de Práctica Clínica para la prevención, detección temprana y tratamiento de las complicaciones del em- barazo, parto o puerperio. Bogotá
- 45.Cifuentes-González C, Rojas-Carabali W, Fonseca-Mora MA et al (2022) Colombian Ocular Infectious Epidemiology Study (COIES): herpes zoster ophthalmicus prevalence and sociodemographic characterization, 2015–2019. Int J Infect Dis 116:27–33. 10.1016/j.ijid.2021.12.332 10.1016/j.ijid.2021.12.332 [DOI] [PubMed] [Google Scholar]
- 46.Boada-Robayo L, Cruz-Reyes DL, Cifuentes-González C et al (2022) Exploring the association between precipitation and population cases of ocular toxoplasmosis in Colombia. PLoS Negl Trop Dis 16:e0010742. 10.1371/journal.pntd.0010742 10.1371/journal.pntd.0010742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chen S-C, Chuang C-T, Chu M-Y, Sheu S-J (2017) Patterns and etiologies of uveitis at a tertiary referral center in Taiwan. Ocul Immunol Inflamm 25:S31–S38. 10.1080/09273948.2016.1189577 10.1080/09273948.2016.1189577 [DOI] [PubMed] [Google Scholar]
- 48.Birnbaum AD, French DD, Mirsaeidi M, Wehrli S (2015) Sarcoidosis in the national veteran population. Ophthalmology 122:934–938. 10.1016/j.ophtha.2015.01.003 10.1016/j.ophtha.2015.01.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Smith JA, Mackensen F, Sen HN et al (2009) Epidemiology and course of disease in childhood uveitis. Ophthalmology 116:1544-1551.e1. 10.1016/j.ophtha.2009.05.002 10.1016/j.ophtha.2009.05.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ozdal PÇ, Sen E, Yazici A, Ozturk F (2012) Patterns of childhood-onset uveitis in a referral center in Turkey. J Ophthal Inflamm Infect 2:13–19. 10.1007/s12348-011-0044-8 10.1007/s12348-011-0044-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sagoo MS, Mehta H, Swampillai AJ et al (2014) Primary intraocular lymphoma. Surv Ophthalmol 59:503–516. 10.1016/j.survophthal.2013.12.001 10.1016/j.survophthal.2013.12.001 [DOI] [PubMed] [Google Scholar]
- 52.Heiferman MJ, Yu MD, Mruthyunjaya P (2022) Update in molecular testing for intraocular lymphoma. Cancers 14:4546. 10.3390/cancers14194546 10.3390/cancers14194546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.García-Aparicio A, Alonso Martín L, LópezLancho R et al (2021) Epidemiology of uveitis in a Spanish Region: prevalence and etiology. Ophthalmic Epidemiol 28:227–236. 10.1080/09286586.2020.1815802 10.1080/09286586.2020.1815802 [DOI] [PubMed] [Google Scholar]
- 54.Sabhapandit S, Murthy SI, Singh VM et al (2017) Epidemiology and clinical features of uveitis from urban populations in South India. Ocul Immunol Inflamm 25:S39–S45. 10.1080/09273948.2016.1236971 10.1080/09273948.2016.1236971 [DOI] [PubMed] [Google Scholar]
- 55.Yang P, Zhong Z, Du L et al (2021) Prevalence and clinical features of systemic diseases in Chinese patients with uveitis. Br J Ophthalmol 105:75–82. 10.1136/bjophthalmol-2020-315960 10.1136/bjophthalmol-2020-315960 [DOI] [PubMed] [Google Scholar]
- 56.Jones NP (2015) The manchester uveitis clinic: the first 3000 patients—epidemiology and casemix. Ocul Immunol Inflamm 23:118–126. 10.3109/09273948.2013.855799 10.3109/09273948.2013.855799 [DOI] [PubMed] [Google Scholar]
- 57.Anaya J-M, Rojas-Villarraga A, García-Carrasco M (2012) The autoimmune tautology: from polyautoimmunity and familial autoimmunity to the autoimmune genes. Autoimmune Dis 2012:1–2. 10.1155/2012/297193 10.1155/2012/297193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Mathew RG, Goh BT, Westcott MC (2014) British Ocular Syphilis Study (BOSS): 2-year national surveillance study of intraocular inflammation secondary to ocular syphilis. Invest Ophthalmol Vis Sci 55:5394. 10.1167/iovs.14-14559 10.1167/iovs.14-14559 [DOI] [PubMed] [Google Scholar]
- 59.Yurkovetskiy L, Burrows M, Khan AA et al (2013) Gender bias in autoimmunity is influenced by microbiota. Immunity 39:400–412. 10.1016/j.immuni.2013.08.013 10.1016/j.immuni.2013.08.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Hogan MJ, Thygeson P, Kimura SJ (1956) Uveitis in association with rheumatism. Trans Am Ophthalmol Soc 54:93–114; discussion, 114–120 [PMC free article] [PubMed]
- 61.Gallagher K, Viswanathan A, Okhravi N (2015) Association of systemic lupus erythematosus with uveitis. JAMA Ophthalmol 133:1190. 10.1001/jamaophthalmol.2015.2249 10.1001/jamaophthalmol.2015.2249 [DOI] [PubMed] [Google Scholar]
- 62.Uribe-Reina P, Muñoz-Ortiz J, Cifuentes-Gonzalez C et al (2021) Ocular manifestations in colombian patients with systemic rheumatologic diseases. OPTH 15:2787–2802. 10.2147/OPTH.S306621 10.2147/OPTH.S306621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Shapira Y, Ben-Arie-Weintrob Y, Gilburd B et al (2021) Antiphospholipid antibodies may be associated with uveitis. Eur J Ophthalmol 31:2446–2450. 10.1177/1120672120968729 10.1177/1120672120968729 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.