

Abstract
Introduction:
In two randomized controlled trials (RCT) we tested the efficacy of a novel integrated vocational rehabilitation and mental healthcare intervention, coined INT, for sickness absentees with common mental disorders. The aim was to improve vocational outcomes compared to Service As Usual (SAU). Contrary to expectations, the delivered intervention caused worse outcomes within some diagnostic groups and some benefits in others. In this phase 4 study, we examined the effectiveness of the intervention in real-world practice.
Method:
In this prospective intervention study, we allocated adult sickness absentees with either depression, anxiety, or adjustment disorder to receive INT in a real-world setting in a Danish Municipality. We compared the vocational outcomes of this group to a matched group who received INT as a part of the RCTs, after randomization to the intervention group herein. Primary outcome was return to work at any point within 12 months.
Results:
In the real-world group, 151 participants received INT during 2019. From the randomized trials, 302 matched participants who received INT between 2016–2018 were included. On the primary outcome – return to work within 12 months – the real-word group fared worse (48.3 vs 64.6 %, OR 0.54 [95%CI: 0.37–0.79], p = 0.001). Across most other vocational outcomes, a similar pattern of statistically significant poorer outcomes in the real-world group was observed: Lower number of weeks in work and lower proportion in work at 12 months (42.3% vs. 58.3% (p = 0.002)).
Discussion:
The real-word group showed significantly worse vocational outcomes. Like in many other studies of complex interventions, implementation was difficult in the original randomized trials and perhaps even more difficult in the less structured real-world setting. Since the intervention was less effective for some groups compared to SAU in the original trial, this negative effect may be even more pronounced in a real-world setting.
Keywords: integrated care, common mental disorders, vocational rehabilitation, depression, anxiety
Introduction
Common mental disorders (CMD) like anxiety, depression, and stress-related disorders alone account for 40% of all sickness absence longer than eight weeks [1]. These disorders are associated with much suffering and large societal costs due to production loss and expenses for services and sick leave benefits. Furthermore, sick leave duration is associated with risk of permanent labour market exclusion [2]. For these reasons, much intervention research has focused on vocational outcomes, like the most frequently used being sick leave duration, but also proportion in work at follow-up is seen [3]. Many interventions have been studied with heterogenous results, but according to a comprehensive systematic review [4], the most effective interventions seem to be ones who:
have more than one component, e.g. both psychotherapy and a work-focused intervention, yielding a complex intervention defined as those “made up of various interconnecting parts”, as defined by Campbell et al. [5]; furthermore they should
focus on early, graded return to work; and finally they should
emphasize workplace involvement [4].
The interplay between components in a complex intervention can take many forms, like e.g. interconnected as mentioned above, but it has also been suggested that they should be integrated [6], and another study of such integration of interventions showed positive results [7].
But such complex or integrated interventions are quite hard to deliver with high fidelity, even in settings of a randomized controlled trial (RCT), despite often detailed intervention protocol and rigorous attempts to achieve high protocol fidelity [8]. Adding further complexity, the value of RCT results depends on their generalizability to real-world settings [9], and if external validity is low due to even lower fidelity when the rigorousness of the RCT setting is changed to a real-world setting, the gap between intervention effect in these domains may be significant [10]. For that reason, there is a growing consensus that any intervention showing significant efficacy in an RCT should followingly be tested in a so-called “phase IV study” (referring to the RCT as the typical methodology in phase III studies), to determine intervention effectiveness, being an intervention’s effect in a real-world setting [11]. The study presented in this paper, is such a phase IV study, where we compare the effect of a complex intervention we trialed in a previous study, to the effect of the same intervention in a real-world setting. The principal intervention we test in this phase IV study, is an integrated intervention we previously tested in two randomized controlled trials (RCT), the IBBIS Trials [12,13].
The original IBBIS Trials
“IBBIS” is a Danish acronym translating to “Integrated Health Care and Vocational Rehabilitation for Sick-Leave Benefit Recipients”. Both RCTs included adult participants on sick leave with common mental disorders, with an average baseline sick leave duration of 10 weeks (SD 4). One RCT included absentees with depression or anxiety as their main diagnosis (RCT1) and the other absentees with a stress-related disorder (RCT2). Both studied the effect of the IBBIS Integrated Intervention (INT) by comparing it to Service As Usual (SAU), which in Denmark consist of treatment in General Practice, combined with standard work rehabilitation intervention and case management in the local municipality, and these sector do not cooperate, but in some cases exchanges information unidirectionally from GPs to the municipality during sick-leave – see Figure 1 depicting SAU in left column. Both trials were pre-registered on ClinicalTrials.org and in two design papers [14,15].
Figure 1.
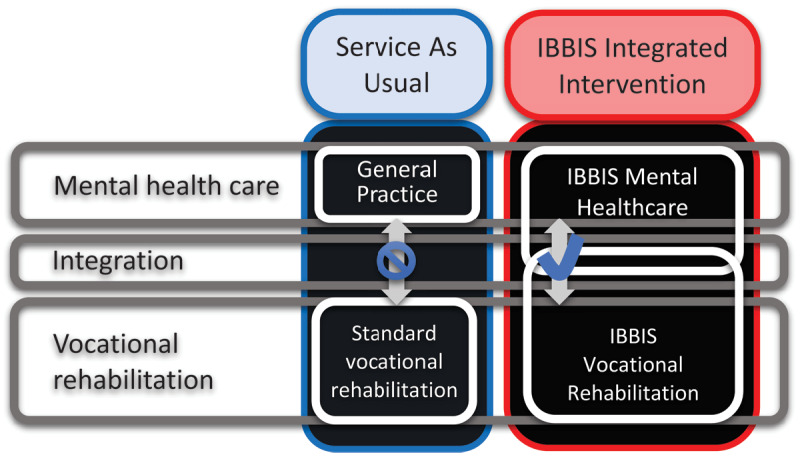
Composition of intervention components. “IBBIS” is a Danish acronym translating to “Integrated Health Care and Vocational Rehabilitation for Sick-Leave Benefit Recipients”.
Results of the IBBIS Trials
In RCT1 (target group: anxiety and depression), we found that INT showed benefits regarding probability of being in full-time work at 12-month follow-up (a secondary outcome) but no effect on the primary outcome, return to work measured at 12-month follow-up [16]. In RCT2 (target group: stress-related disorders), INT consistently showed significantly worse vocational outcomes across different measures [17].
In both IBBIS Trials, implementation was suboptimal. A process evaluation study showed that diverging norms and goals between staff groups of the different sectors supposed to be integrated regarding norms and goals. It was concluded that that hindered the integration of the intervention components [18]. The intervention protocol stipulated that intervention components should imply goal alignment between the goals of the healthcare staff and the employment consultants delivering the vocational rehabilitation intervention, but instead a goal hierarchy gradually developed and settled during the two-year trial period, with the goals of the latter staff group dominated over the other [19]. These implementation issues constituted the largest challenges to the studies’ external validity. Either the implementation issues meant that the results of the trial could not be ascribed the true effects of the IBBIS Integrated Intervention, if it had been delivered, or either this intervention is so hard to deliver, even in a rigorous RCT setting that in the real-world it is unfeasible.
Aim of this study
In accordance with the above discussion, a process evaluation of the IBBIS Trials led to the conclusion that a complex intervention like INT needs substantial managerial attention to be successfully implemented in a real-world setting [18]. After the inclusion to the IBBIS Trials was concluded, the Copenhagen Municipality decided to continue to deliver the IBBIS Integrated Intervention to the population of sickness absentees for which in was intended. This gave rise to the opportunity to study the effectiveness of the intervention in a real-world setting, and hence quantify any differential from the (negative) efficacy measured in the RCT setting. The aim was to compare the vocational outcomes of sickness absentees who received INT in the IBBIS RCTs with a comparable group of sickness absentees who received INT in a real-world setting INT (henceforth “real-world-INT”) after the RCTs ended.
Methods
This study was registered before final analyses were performed. The preregistered statistical analysis plan can be found at https://osf.io/3ca5m/.
Data sources
As in the original RCTs, we retrieved vocational information about the absentees from Danish national registers on social benefits and income (the Danish DREAM register). Information about diagnosis and start date of sick leave was collected by research staff. Covariate data on education, social benefit history and employment status was retrieved from Statistics Denmark.
Recruitment procedure, eligibility assessment and inclusion
The study population in real-world-INT was recruited from the agency in Copenhagen Municipality, managing the cases of sick-leave benefiters. Recruitment procedure, and inclusion criteria was similar to the procedure in the IBBIS RCTs, except participants were not randomized, but offered inclusion in the intervention group if eligibility was established.
In RCT-INT, participants underwent a randomization procedure, before eligibility assessment, which again was conducted before receiving INT, whereas in the real-world-INT group, participants did not undergo randomization, but allocation to intervention if they were found eligible and gave written consent. Yet, in both groups, after recruitment to, and as a part of the eligibility assessment, participants a thorough mental health assessment, called the IBBIS Mental Health Assessment (IBBIS-MHA). IBBIS-MHA was performed by a psychiatrist or by a mental health professional (a nurse, psychologist, or psychiatric medical resident) supervised by a psychiatrist. The IBBIS-MHA consisted of a clinical interview with a focus on current mental health issues. The clinical interview started with a pragmatic clinical interview where the participants was asked about main health issues, and about what they experienced as main cause of sick leave. That part of the interview was followed by a) the semi-structured MINI International Neuropsychiatric Interview [20], to ensure a systematic approach to assessment of main mental health symptom domains; furthermore, to screen for personality disorders it was followed by the clinician-rated b) Standardized Assessment of Personality – Abbreviated Scale (SAPAS) [21] and c) Attention deficit hyperactivity disorder symptom checklist for adults, Adult Self-Report Scale (ASRS) [22]. The Mini-Mental State Examination (MMSE) was used if dementia was clinically suspected by the assessor [23]. Before the interview, participants filled in the validated Danish version of the Four-Dimensional Symptom Questionnaire (4DSQ) that measures levels of depression, anxiety, distress, and somatization [24]. Assessors had access to the results to guide their clinical assessment. We studied the isolated effects of the IBBIS-MHA in a separate study, since we could not rule out that this procedure could itself influence vocational outcomes. Hence, the outcomes in the SAU group in the IBBIS Trials may not totally reflect a true real-world-SAU, and the effect of IBBIS-MHA was needed to inform discussion of the external validity of the results of the IBBIS Trials. Due to methodological limitations, no strong conclusions could be drawn from that study, but we saw tendencies towards a negative effect on vocational outcomes from this assessment per se [25]. Before study inclusion, participants in RCT-INT filled in self-report questionnaires that participants in real-world-INT did not, but this data was not available to the assessors, solely used for study purposes in the RCTs why they where not utilized in this study.
Eligibility criteria
To be eligible for inclusion in the study groups participants had to be at least 18 years of age, be on sick leave for at least 4 consecutive weeks, have undergone a mental health assessment with a primary diagnosis of either anxiety, depression, or an adjustment disorder, including exhaustion disorder [26] or stress according to the Four-Dimensional Symptom Questionnaire [24].
Study intervention: The IBBIS Integrated Intervention (INT)
Both study groups received INT, the IBBIS Integrated Intervention, yet in RCT- versus real-world- settings, respectively. The IBBIS Integrated Intervention (INT), consists of IBBIS Mental Healthcare and IBBIS Vocational Rehabilitation, and these two intervention components were integrated – see Figure 1, right column.
INT consisted of the integration of IBBIS Vocational Rehabilitation and IBBIS Mental Healthcare. These intervention components and the methods for integration are described in detail in the RCT study design papers [14,15]. IBBIS Mental Healthcare was a stepped-care intervention with treatment options depending on diagnosis. For participants with stress-related disorders, treatment included predominantly clinical monitoring, stress-coaching or, for those with exhaustion disorders, mindfulness-based stress-reduction (MBSR). Treatment of participants with anxiety or depression adhered to the guidelines from National Institute of Clinical Excellence [27], consisting primarily of psychoeducation, clinical monitoring, psychotherapy, medication or, in more severe cases, a combination hereof. Treatment was delivered by care managers, who were mental healthcare professionals with at least one year of experience and training in general mental healthcare and psychotherapy. IBBIS Vocational Rehabilitation was based on the principles of the Sharp-at work intervention [28] and Individual Placement and Support [29]. The vocational rehabilitation intervention components were provided by employment consultants, who also functioned as the case-managers of the participants sick-leave benefit cases.
These two principal intervention components, IBBIS Mental Healthcare and IBBIS Vocational Rehabilitation, were sought integrated through the following activities: I) co-location of staff; II) at least one roundtable-meeting between the care manager, the employment consultant, and each participant; and III) interdisciplinary training and supervision for care managers and employment consultants.
Protocol adherence in RCT-INT
In RCT-INT, staff adherence to the study intervention manuals was examined through fidelity interviews. While IBBIS Mental Healthcare was implemented with high fidelity, IBBIS Vocational Rehabilitation and the activities to ensure integration were only implemented with fair fidelity. For example, a central intervention component activity like work contact was only delivered to rather few participants. We saw a slight tendency of increasing fidelity over time during the study period, but we did not perform any statistical test.
Control group selection
The group of study participants in the control group, RCT-INT, was a selected subset of participants from the group of participants randomized to INT in the original IBBIS Trials (RCT-INT).
We could not rule out that there were differences between group who were referred for eligibility assessment for an RCT, and a group referred to the same intervention in a less rigorous real-world setting. Therefore, through propensity score matching [30], we selected two controls per participant in the intervention group. Propensity score matching is a statistical method for finding the most similar participants(s) per one case, when several variables are available, and no exact match can be found, but one wish to find the most similar other case(s). Matching variables were age, sex, primary diagnosis (as established during the IBBIS Mental Health Assessment), employment status (with or without a current employment), work branch category (as defined by Statistics Denmark, e.g. farming, production, teaching, administration etc.), and social benefit history (how many weeks during the two years before baseline had the participant received social benefit payments). These co-variates were selected as matching variables since they are likely to influence vocational outcomes [31]. The general employment rate is also known to impact vocational outcomes among sickness absentees but could not be included as a matching variable; employment rates in society at the time of observation differed between the groups, as the groups received the interventions at different points in time between which the level of employment in society changed (before and after mid-2018, respectively). Crude employment rates are reported without any adjustment since such adjustment would entail assumptions about the exact causal effect of specific changes in employment rates on the vocational outcomes of the study population. Post-hoc, we conducted sensitivity analyses using municipality as a matching variable, since municipality was also associated with vocational outcomes in the RCTs. However, this halved the sample size of the RCT-INT group, as real-world-INT was only delivered in one of the municipalities involved in the RCTs. For that reason, municipality was not a matching variable in the main analyses.
Outcomes
The primary outcome of this study was any return to work any time before 12-month follow-up. We chose this outcome because of its higher sensitivity compared to the more commonly used time-to-event analyses [3] and because, in one of the RCTs, INT seemed to have effect around 12-month rather than 6-month follow-up [32]. Return to work was defined as consecutive period of at least four weeks in which the participant did not receive any social benefit, like sick-leave benefit, and in which period the participant earned a salary through working in a competitive ordinary job. Two secondary outcomes were in a similar fashion any return to work but measured at 6- and 24-month follow-up, respectively. Further secondary outcomes, were, at 6-, 12-, and 24-month follow-up, respectively, proportion in work at follow-up, and number of weeks in work between baseline and follow-up.
Statistical Analyses
Sample size was not determined through calculations, since the cohort size was determined externally, but before analyses were conducted, we calculated that with the number of participants in the study groups, power would be at least 0.8, for a difference of at least 13%-point between groups, since we assumed proportion of positive cases on the primary outcome would be between 0.2 and 0.65 (as observed in the original IBBIS Trials). We applied the intention-to-treat principles in all analyses. Due to the comprehensive nature of the Danish registers, we did not expect missing data and thus did not plan for this eventuality. Treatment effects were estimated using logistic regression for binary outcomes, including the primary outcome. Poisson regression with bootstrapped non-parametric standard errors was used for numeric outcomes, and 1000 resamples were applied. A significance level of 5% in two-sided tests was used throughout. This applied to p-values and all confidence intervals reported. All tests formally reflected a superiority expectation. Type I error rates were controlled for by selecting and prioritizing tests, and therefore no statistical correction of multiple tests was carried out. No distributional assumptions were made. Covariate linearity was controlled using a likelihood ratio test of simple models with and without an added quadratic term. Baseline was defined as the third week of sickness absence, since all participants received sickness benefits, which are only available after at least four weeks of sick leave. Accordingly, no participants had returned to work before that period. The propensity score was estimated using a random forest, that is, an assumption-free tree-based ensemble model that captures non-linear associations well (i.e. interactions).
Results
Baseline
In this study, 151 participants gave written consent to receive real-world-INT. They were included from August 2018 to January 2019. From the group of 416 participants who in 2016–2018 were randomized RCT-INT, we identified and included 302 participants.
Baseline characteristics of the included participants are shown in Table 1. After matching, variables were balanced. Most participants were female (>70 %) and approx. 43 years of age (SD ~10–11). In the two years preceding index sick leave, participants had ~16 weeks (SD ~10) of sick leave and ~7–9 weeks (SD ~16–19) of unemployment. The average unemployment rate was 3.8% during the inclusion of the real-world-INT group and 4.2% regarding RCT-INT.
Table 1.
Baseline characteristics.
|
| |||
|---|---|---|---|
| RCT-INT | REAL WORLD-INT | p-VALUE | |
|
| |||
| n = | 302 | 151 | |
|
| |||
| Sex (male) | 90 (29,8%) | 48 (31,8%) | 0.745 |
|
| |||
| Age | 43.17 (SD: 10,12) | 42.72 (SD: 11,11) | 0.676 |
|
| |||
| Diagnosis: Anxiety, other | 53 (17,5%) | 19 (12,6%) | 0.234 |
|
| |||
| Diagnosis: Anxiety, social | 14 (4,6%) | 12 (7,9%) | |
|
| |||
| Diagnosis: Exhaustion disorder | 86 (28,5%) | 40 (26,5%) | |
|
| |||
| Diagnosis: Depression, mild/moderate | 80 (26,5%) | 48 (31,8%) | |
|
| |||
| Diagnosis: Depression, severe | 26 (8,6%) | 17 (11,3%) | |
|
| |||
| Diagnosis: Stress | 43 (14,2%) | 15 (9,9%) | |
|
| |||
| Benefit history (no transfer in last 2 years) | 74.84 (24,4%) | 71.69 (28,07%) | 0.604 |
|
| |||
| Weeks on unemployment insurance (within 2 years) | 7.36 (SD: 16,63) | 8.99 (SD: 19,41) | 0.875 |
|
| |||
| Education (weeks within 2 years) | 0.52 (SD: 3,6) | 0.83 (SD: 4,68) | 0.570 |
|
| |||
| Sickness benefit (weeks within 2 years) | 15.52 (SD: 9,91) | 16.54 (SD: 10,55) | 0.162 |
|
| |||
| Parent leave (weeks within 2 years) | 3.30 (SD: 11,9) | 3.26 (SD: 12,2) | 0.854 |
|
| |||
| Subsidized employment (weeks within 2 years) | 0.24 (SD: 4,14) | 0.53 (SD: 6,51) | 0.617 |
|
| |||
| Unemployment benefit (weeks within 2 years) | 0.37 (SD: 3,25) | 0.50 (SD: 3,67) | 0.826 |
|
| |||
Outcomes
On the primary outcome (at least 4 consecutive weeks in return to work within 12 months after baseline), 64.6% of the RCT-INT group had experienced RTW but only 48.3% in the real-world INT group (OR 0.51 [95%CI: 0.35–0.76], p = 0.001). The real world-INT group had a lower number of weeks in work (p < 0.001) at all follow-ups. Work status at 6-month follow-up was not statistically different between the two groups but at both 12- and 24-month follow-up, a smaller proportion of the real-world INT group were working, 42.3% vs. 58.3% in the RCT-INT group (p = 0.002). Similarly they have had less weeks in work since baseline at these two follow-ups, but not statistically sign. at 6-month follow-up. All outcome estimates are presented in Table 2, and Figure 2 shows the proportion in stable work per week after baseline.
Table 2.
Vocational outcomes. +: primary outcome. Ratio estimates are odds ratios for the binary outcomes and rate ratios for rate of weeks in employment.
|
| ||||
|---|---|---|---|---|
| OUTCOMES MEASURE | ESTIMATE | p-VALUE | RCT-INT (n = 302) | REAL WORLD-INT (n = 151) |
|
|
|
|||
| RATIOS (95% CI) | MEAN/N (SD/%) | MEAN/N (SD/%) | ||
|
| ||||
| At any point within 24 months, n (%) | 0.60 (0.38, 0.94) | 0.027 | 235 (77.8%) | 88 (67.7%) |
|
| ||||
| At any point within 12 months, n (%)+ | 0.51 (0.35, 0.76) | 0.001 | 195 (64.6%) | 73 (48.3%) |
|
| ||||
| At any point within 6 months, n (%) | 0.73 (0.47, 1.12) | 0.149 | 98 (32.5%) | 39 (25.8%) |
|
| ||||
| Weeks within 24 months, mean (SD) | 0.70 (0.56, 0.84) | 0.000 | 43.3 (SD: 33.2) | 30.3 (SD: 29.6) |
|
| ||||
| Weeks within 12 months, mean (SD) | 0.68 (0.54, 0.85) | 0.000 | 14.5 (SD: 14.3) | 9.9 (SD: 12.6) |
|
| ||||
| Weeks within 6 months, mean (SD) | 0.56 (0.37, 0.82) | 0.000 | 2.7 (SD: 4.9) | 1.5 (SD: 3.4) |
|
| ||||
| Status at 24 months, n (%) | 0.53 (0.35, 0.80) | 0.002 | 176 (58.3%) | 55 (42.3%) |
|
| ||||
| Status at 12 months, n (%) | 0.43 (0.28, 0.64) | 0.000 | 162 (53.6%) | 50 (33.1%) |
|
| ||||
| Status at 6 months, n (%) | 0.73 (0.47, 1.14) | 0.164 | 93 (30.8%) | 37 (24.5%) |
|
| ||||
Figure 2.
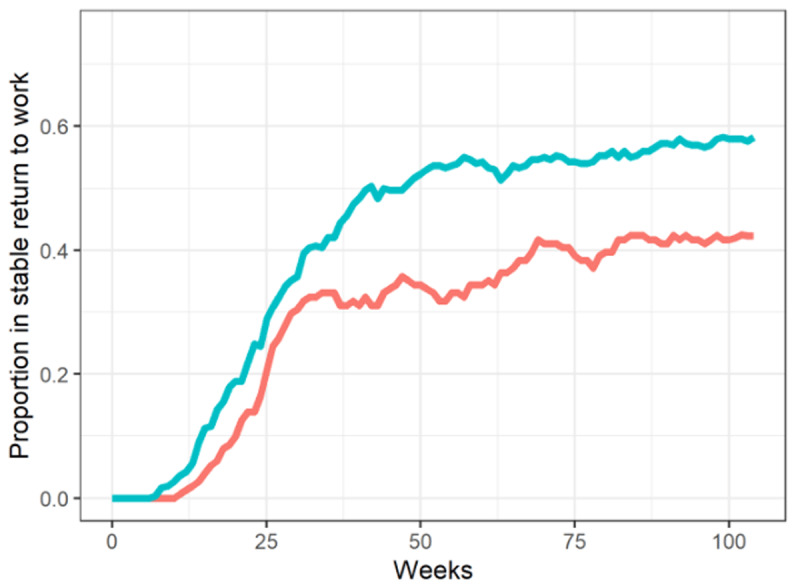
Proportion in stable work, per week. Red line: Real world-INT; Greenish line: RCT-INT.
Sensitivity Analyses
No differences in results were observed between the main analysis and the sensitivity analyses, in which the 151 participants in the real world-INT group were matched to 151 participants in the RCT-INT group in the same municipality. Yet, on some measures the p-value was lower, thereby increasing the overall level of statistical significance in favour of the RCT-INT group’s outcomes. These results are found in the Results Supplement.
Discussion
In this phase IV study, we tested the efficacy of The IBBIS Integrated Intervention (INT) when delivered in a real-world setting by comparing it to its effect when delivered in an RCT setting. To the authors’ belief this is the first phase 4 study in the area of return-to-work interventions for target populations of people on sick-leave with common mental disorders. On the primary outcome, we found a statistically significantly lower proportion of 48.3% had experienced return to work in the real-world-INT group, compared to 64.6% in the RCT-INT group (p = 0.001). Consistently this was the pattern among almost all other measures, with real-world-INT showing worse outcomes compared to RCT-INT.
We believe that most likely the greatest part of the difference is a true difference in causal effect between the two intervention delivery settings. In the randomized trials, we had observed moderate implementation issues, being a low fidelity particularly regarding the vocational rehabilitation intervention components, but a tendency of in rising fidelity over time. We therefore hypothesized that the effect could be similar in the real-world setting, due to fidelity perhaps reaching a level to at least be sufficient to equal the effect in the RCT setting. Contrary to this hypothesis, we saw that vocational outcomes of real-world INT were significantly worse across almost all measures and different periods of follow-up. We believe that a substantial part of the negative outcomes reflects the difference between interventions in real-world vs. RCT settings that is often referred to as the difference between effectiveness and efficacy [33]. One possible explanation could be that the real-word setting implementation was relatively poorer – a tendency also observed in other comparisons of RCTs and real-world settings [33]. During the RCT, managerial focus on protocol adherence was greater to ensure protocol fidelity and, subsequently, internal validity, but the results in this study support the suspicion that the intervention might be rather unfeasible.
We cannot completely rule out that unobserved between-group differences confounded the results. It is, for example, possible that the level of disorder was higher in the real-world group, causing worse outcomes. While we tried to handle this potential confounder by matching diagnoses, levels of illness could still vary within diagnostic groups because the municipal body had different incentives for referring potential participants during recruitment to the real-world study (after the RCTs). Other studies have previously suggested that RCT participants and real-world individuals may differ [34]. Societal factors that change over time, like e.g. employment rates could explain some of the findings through confounding, but it is not very likely. During observation of the real-world group, the average baseline unemployment rate was lower, and one would therefore have expected increased return-to-work rates among sickness absentees rather than the decreased rates we observed [35]. Similarly, sickness benefit legislation was reformed some years prior to the study, and that could influence the general return to work rates differently in the two time periods the two study groups were compared. Yet, the RCTs took place during the gradual implementation of this reform, from 2016 to 2019, and we observed that return-to-work rates after sick leave tended to increase over time, so this cannot explain the decrease in return-to-work rates seen in this study. Finally, sensitivity analyses were performed to adjust for municipality, but though the sample size of the control group was halved, statistical significance increased, making it more likely that results represented a true difference.
Strengths and limitations
The major strength of this study is the ability to track all participants in a highly consistent manner with few-to-no missing data. Given the comprehensive and precise Danish registers, individual observations are probably quite accurate. However, the use of register-based data also has certain limitations, most notably the fact that the available information only describes utilization of sickness benefits and not level of disease. Several other studies have shown that the utilization of sickness benefits is influenced by a range of contextual factors other than level of disease, for example the degree of employment protection in a country [36] and the level of sick leave benefit control [37]. This study is limited by the fact that the two study groups were separated in time, and we cannot exclude the possibility that time is a confounder, not least since contextual factors might have changed between the study periods. However, as discussed above, this effect alone would most likely produce the opposite of what we have found. Another strength is that the study was publicly pre-registered before any analysis was performed, thus reducing the risk of Type 1 errors. While not adjusting for multiple tests could be a limitation, it is negligible in this study since all findings of highly statistically significant differences favour only one of the interventions. Also, all tests support the same overall hypothesis of treatment effects on vocational recovery.
Conclusion
This study has a number of implications. First and foremost, it highlights that INT is either non-feasible or ineffective for common mental disorders on a group level. While the original IBBIS Trial targeting people with anxiety and depression tended to show some positive effect in the group of people with anxiety, this effect was not seen consistently across outcome measures, and this study casts further doubt on the effectiveness of the intervention, specifically when these are translated into real-world setting. Assuming that interventions are usually implemented with higher protocol fidelity in RCTs than in real-world settings, this study confirms that the efficacy of a complex intervention like INT requires a high level of managerial control, as previously documented in the process evaluation of the original RCTs [18]. While INT may have positive effects that are not observed in this study, for example on well-being, implementing INT in a real-world setting like it was here will most likely not improve vocational outcomes for the common mental disorder population as a whole.
Additional File
The additional file for this article can be found as follows:
This supplement contains results of the sensitivity analysis.
Funding Statement
The Danish Agency for Labour Market and Recruitment sponsored most of the IBBIS project, which was conducted in collaboration with the Mental Health Services in the Capital Region of Denmark. The four collaborating municipalities partly financed the salary of the employment consultants.
Ethics and Consent
The original trials were registered at https://www.clinicaltrials.gov/ (#NCT02885519 and #NCT02872051). Like these two trials, the present study was evaluated and approved by the Regional Ethics Committees of the Capital Region (#H-16015724) and the Danish Data Protection Agency (#RHP-2016-006). A research team member informed participants about the objective of the study and the implications of participation, and all participants gave oral and written consent before enrolment.
Reviewers
Professor Nick Goodwin, PhD Director, Central Coast Research Institute for Integrated Care, NSW, Australia.
One anonymous reviewer.
Funding Information
The Danish Agency for Labour Market and Recruitment had a say in the design of the study (decisions regarding target population and selected interventions modalities) but did not parttake in any decisions regarding analysis, interpretation of the data or publication of results.
Competing Interests
The authors have no competing interests to declare.
References
- 1.Søgaard HJ, Bech P. Psychiatric disorders in long-term sickness absence – a population-based cross-sectional study. Scand J Public Health. 2009; 37: 682–9. DOI: 10.1177/1403494809344357 [DOI] [PubMed] [Google Scholar]
- 2.Fagot J-P, Cuerq A, Samson S, Fagot-Campagna A. Cohort of one million patients initiating antidepressant treatment in France: 12-month follow-up. Int J Clin Pract Suppl. 2016; 70: 744–751. DOI: 10.1111/ijcp.12850 [DOI] [PubMed] [Google Scholar]
- 3.Hoving J, Ravinskaya M, Verbeek J, Langendam M, Kunz R, Verstappen S, et al. The reporting of work participation outcomes and measurement methods in randomized controlled trials: a systematic review. Saf Health Work. 2022; 13: S103–S103. DOI: 10.1016/j.shaw.2021.12.1076 [DOI] [PubMed] [Google Scholar]
- 4.Mikkelsen MB, Rosholm M. Systematic review and meta-analysis of interventions aimed at enhancing return to work for sick-listed workers with common mental disorders, stress-related disorders, somatoform disorders and personality disorders. Occupational and Environmental Medicine. 2018. DOI: 10.1136/oemed-2018-105073 [DOI] [PubMed] [Google Scholar]
- 5.Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, et al. Framework for design and evaluation of complex interventions to improve health. BMJ. 2000; 321: 694–696. DOI: 10.1136/BMJ.321.7262.694 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.OECD. The Organization for Economic coordination and Development. Sick on the Job? Myths and Realities about Mental Health and Work. 2012. [Google Scholar]
- 7.Reme SE, Grasdal AL, Løvvik C, Lie SA, Øverland S. Work-focused cognitive-behavioural therapy and individual job support to increase work participation in common mental disorders: A randomised controlled multicentre trial. Occup Environ Med. 2015; 72: 745–752. DOI: 10.1136/oemed-2014-102700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bonfils IS, Hansen H, Dalum HS, Eplov LF. Implementation of the individual placement and support approach–facilitators and barriers. Scandinavian Journal of Disability Research. 2017; 19: 318–333. DOI: 10.1080/15017419.2016.1222306 [DOI] [Google Scholar]
- 9.Cochrane A. Effectiveness and efficiency: random reflections on health services. 1972. Available: https://repository.library.georgetown.edu/handle/10822/764041 [DOI] [PubMed]
- 10.Rothwell PM. External validity of randomised controlled trials: “To whom do the results of this trial apply?” The Lancet (British edition). 2005; 365: 82–93. DOI: 10.1016/S0140-6736(04)17670-8 [DOI] [PubMed] [Google Scholar]
- 11.Pinnock H, Epiphaniou E, Taylor SJC. Phase IV implementation studies. The forgotten finale to the complex intervention methodology framework. Ann Am Thorac Soc. 2014; 11 Suppl 2: S118–S122. DOI: 10.1513/AnnalsATS.201308-259RM [DOI] [PubMed] [Google Scholar]
- 12.Hoff A, Poulsen RM, Fisker JP, Hjorthøj C, Nordentoft M, Christensen U, et al. Integrated Mental Healthcare and Vocational Rehabilitation for People on Sick Leave with Anxiety or Depression: 24-Month Follow-up of the Randomized IBBIS Trial. J Occup Rehabil. 2023; 33: 570–580. DOI: 10.1007/S10926-023-10094-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hoff A, Poulsen RM, Fisker JP, Hjorthøj C, Nordentoft M, Bojesen AB, et al. Integrated mental healthcare and vocational rehabilitation for people on sick leave with stress-related disorders: 24-month follow-up of the randomized IBBIS trial. Scand J Work Environ Health. 2023; 49: 303–308. DOI: 10.5271/SJWEH.4084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Poulsen R, Fisker J, Hoff A, Hjorthøj C, Eplov LF. Integrated mental health care and vocational rehabilitation to improve return to work rates for people on sick leave because of exhaustion disorder, adjustment disorder, and distress (the Danish IBBIS trial): Study protocol for a randomized controlled trial. Trials. 2017; 18: 1–15. DOI: 10.1186/S13063-017-2273-0/TABLES/6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Poulsen R, Hoff A, Fisker J, Hjorthøj C, Eplov LF. Integrated mental health care and vocational rehabilitation to improve return to work rates for people on sick leave because of depression and anxiety (the Danish IBBIS trial): Study protocol for a randomized controlled trial. Trials. 2017; 18: 1–14. DOI: 10.1186/S13063-017-2272-1/TABLES/7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hoff A, Poulsen RM, Fisker J, Hjorthøj C, Rosenberg N, Nordentoft M, et al. Integrating vocational rehabilitation and mental healthcare to improve the return-to-work process for people on sick leave with depression or anxiety: results from a three-arm, parallel randomised trial. Occup Environ Med. 2022; 79: 134–142. DOI: 10.1136/OEMED-2021-107894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hoff A, Fisker J, Poulsen RM, Hjorthøj C, Rosenberg NK, Nordentoft M, et al. Integrating vocational rehabilitation and mental healthcare to improve the return-to-work process for people on sick leave with stress-related disorders: results from a randomized trial. Scand J Work Environ Health. 2022; 48: 361–371. DOI: 10.5271/SJWEH.4021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Poulsen RM, Pii KH, Bültmann U, Meijer M, Eplov LF, Albertsen K, et al. Developing Normative Integration among Professionals in an Intersectoral Collaboration: A Multi-Method Investigation of an Integrated Intervention for People on Sick Leave Due to Common Mental Disorders. Int J Integr Care. 2019; 19. DOI: 10.5334/IJIC.4694 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Poulsen RM, Pii KH, Eplov LF, Meijer M, Bültmann U, Christensen U. Developing interpersonal trust between service users and professionals in integrated services: Compensating for latent distrust, vulnerabilities and uncertainty shaped by organisational context. Int J Integr Care. 2021; 21. DOI: 10.5334/ijic.5599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sheehan D, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry. 1998; 22–33. DOI: 10.1016/S0924-9338(99)80239-9 [DOI] [PubMed] [Google Scholar]
- 21.Moran P, Leese M, Lee T, Walters P, Thornicroft G, Mann A. Standardised Assessment of Personality – Abbreviated Scale (SAPAS): Preliminary validation of a brief screen for personality disorder. British Journal of Psychiatry. 2003; 183: 228–232. DOI: 10.1192/bjp.183.3.228 [DOI] [PubMed] [Google Scholar]
- 22.Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005; 35: 245–256. DOI: 10.1017/S0033291704002892 [DOI] [PubMed] [Google Scholar]
- 23.Cole MG, McCusker J, Elie M, Dendukuri N, Latimer E, Belzile E. Systematic detection and multidisciplinary care of depression in older medical inpatients: a randomized trial. Can Med Assoc J. 2006; 174: 38–44. DOI: 10.1503/cmaj.050519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Terluin B, Hoff A, Falgaard Eplov L. Assessing measurement equivalence of the Danish and Dutch Four-Dimensional Symptom Questionnaire using differential item and test functioning analysis. Scand J Public Health. 2021; 49: 479–486. DOI: 10.1177/1403494820942074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hoff A, Bojesen AB, Fisker J, Poulsen RM, Hjorthøj C, Nordentoft M, et al. Does a specialized assessment improve vocational outcomes for people on sick leave with a suspected common mental disorder? Results from the Mental Health Assessment Study (MeHAS). PLOS Mental Health. 2024; 1: e0000020. DOI: 10.1371/JOURNAL.PMEN.0000020 [DOI] [Google Scholar]
- 26.Besèr A, Sorjonen K, Wahlberg K, Peterson U, Nygren A, Asberg M. Construction and evaluation of a self rating scale for stress-induced Exhaustion Disorder, the Karolinska Exhaustion Disorder Scale. Scand J Psychol. 2014; 55: 72–82. DOI: 10.1111/sjop.12088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.The National Institute for Health and Care Excellence. The NICE Guideline on the Treatment and Depression the Treatment and Management of Depression. NICE guidelines [CG90]. 2009. [Google Scholar]
- 28.Arends I, van der Klink JJL, van Rhenen W, de Boer MR, Bültmann U. Prevention of recurrent sickness absence in workers with common mental disorders: results of a cluster-randomised controlled trial. Occup Environ Med. 2014; 71: 21–9. DOI: 10.1136/oemed-2013-101412 [DOI] [PubMed] [Google Scholar]
- 29.Modini M, Joyce S, Mykletun A, Christensen H, Bryant RA, Mitchell PB, et al. The mental health benefits of employment: Results of a systematic meta-review. Australasian Psychiatry. 2016; 24: 331–336. DOI: 10.1177/1039856215618523 [DOI] [PubMed] [Google Scholar]
- 30.Chen JW, Maldonado DR, Kowalski BL, Miecznikowski KB, Kyin C, Gornbein JA, et al. Best Practice Guidelines for Propensity Score Methods in Medical Research: Consideration on Theory, Implementation, and Reporting. A Review. Arthroscopy - Journal of Arthroscopic and Related Surgery. 2022; 38. DOI: 10.1016/j.arthro.2021.06.037 [DOI] [PubMed] [Google Scholar]
- 31.Fisker J, Hjorthøj C, Hellström L, Mundy SS, Rosenberg NG, Eplov LF. Predictors of return to work for people on sick leave with common mental disorders: a systematic review and meta-analysis. Int Arch Occup Environ Health. 2022; 95: 1–13. DOI: 10.1007/s00420-021-01827-3 [DOI] [PubMed] [Google Scholar]
- 32.Hoff A, Poulsen RM, Fisker J, Hjorthøj C, Rosenberg N, Nordentoft M, et al. Integrating vocational rehabilitation and mental healthcare to improve the return-to-work process for people on sick leave with depression or anxiety: results from a three-arm, parallel randomised trial. Occup Environ Med. 2022; 79: 134–142. DOI: 10.1136/OEMED-2021-107894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. Framework for the development and evaluation of complex interventions: gap analysis, workshop and consultation-informed update. Health Technol Assess. 2021; 25: 1–132. DOI: 10.3310/hta25570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pinnock H, Epiphaniou E, Taylor SJC. Phase IV implementation studies. The forgotten finale to the complex intervention methodology framework. Ann Am Thorac Soc. 2014; 11 Suppl 2: S118–S122. DOI: 10.1513/AnnalsATS.201308-259RM [DOI] [PubMed] [Google Scholar]
- 35.Aagestad C, Tyssen R, Johannessen HA, Gravseth HM, Tynes T, Sterud T. Psychosocial and organizational risk factors for doctor-certified sick leave: a prospective study of female health and social workers in Norway. BMC Public Health. 2014; 14: 1016–1016. DOI: 10.1186/1471-2458-14-1016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Metcalfe JD, Drake RE, Bond GR. Economic, Labor, and Regulatory Moderators of the Effect of Individual Placement and Support Among People With Severe Mental Illness: A Systematic Review and Meta-analysis. Schizophr Bull. 2018; 44: 22–31. DOI: 10.1093/schbul/sbx132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Johansson P, Lindahl E. Can sickness absence be affected by information meetings? Evidence from a social experiment. Empir Econ. 2013; 44: 1673–1695. DOI: 10.1007/s00181-012-0593-1 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
This supplement contains results of the sensitivity analysis.