

Abstract
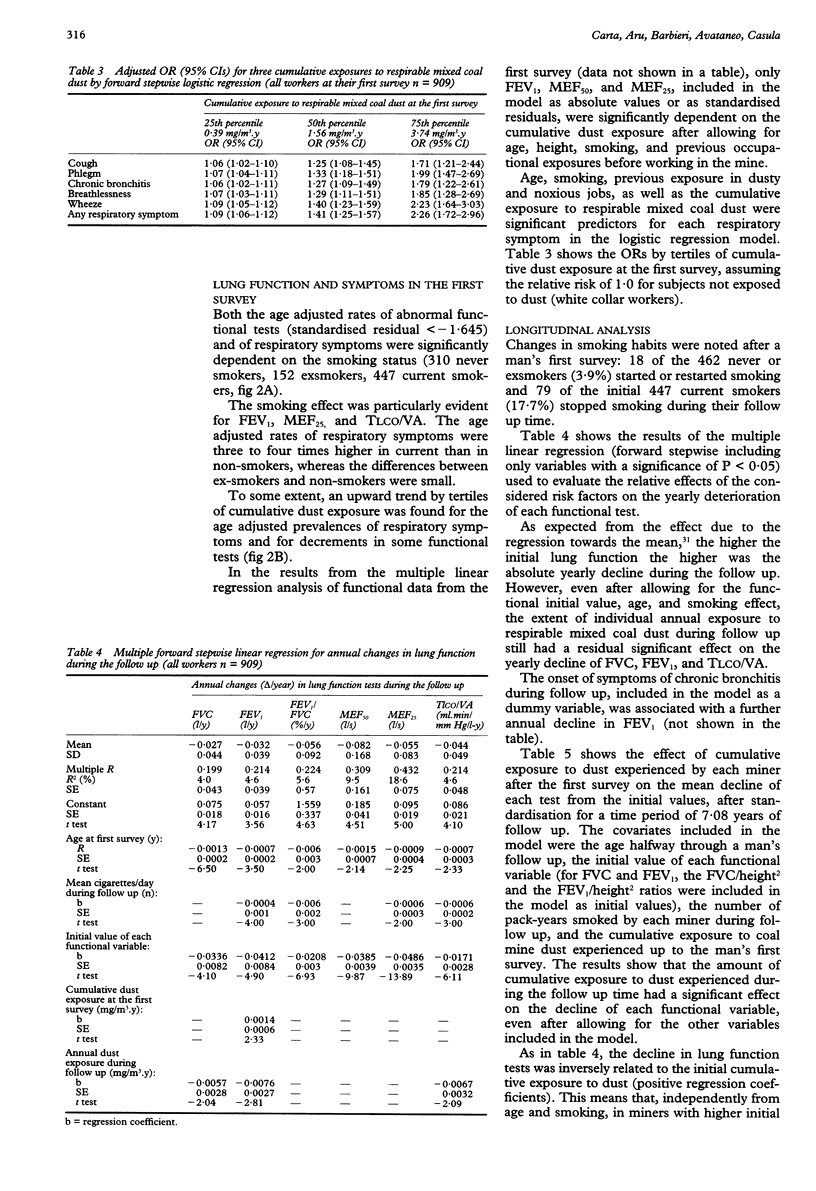
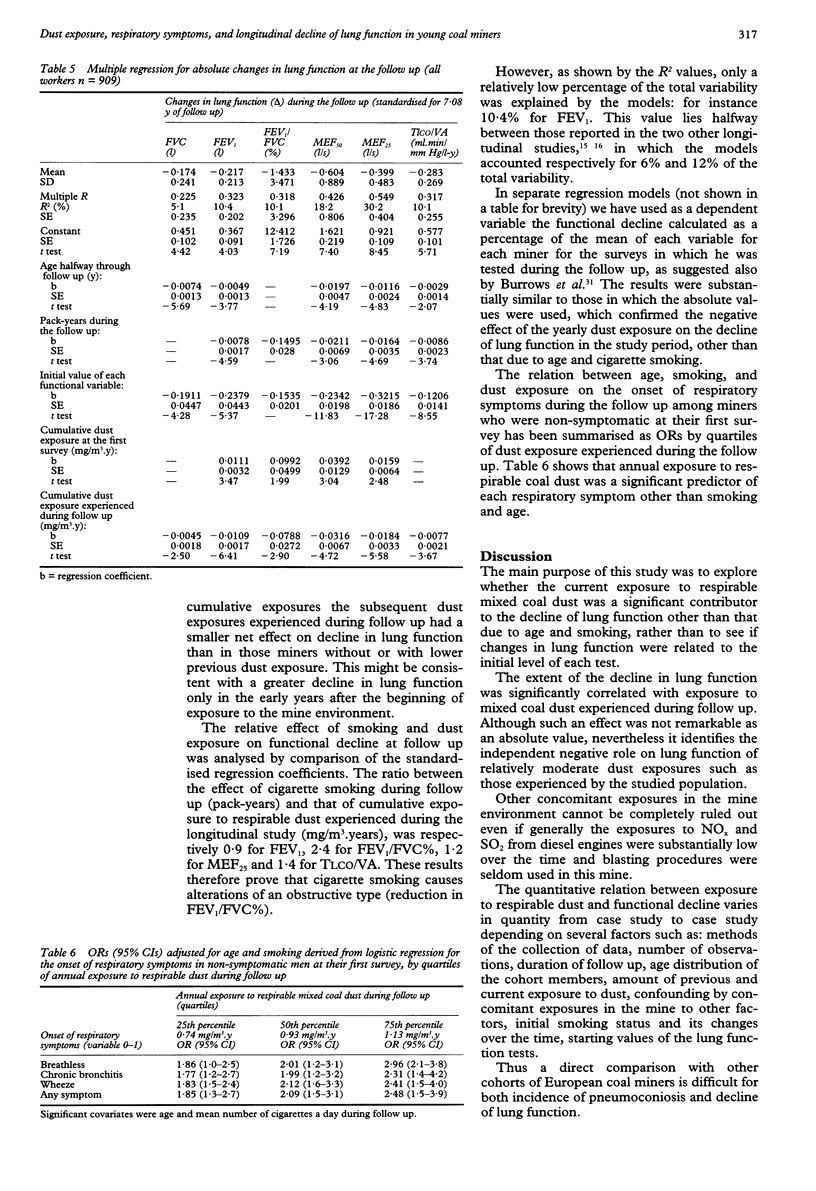
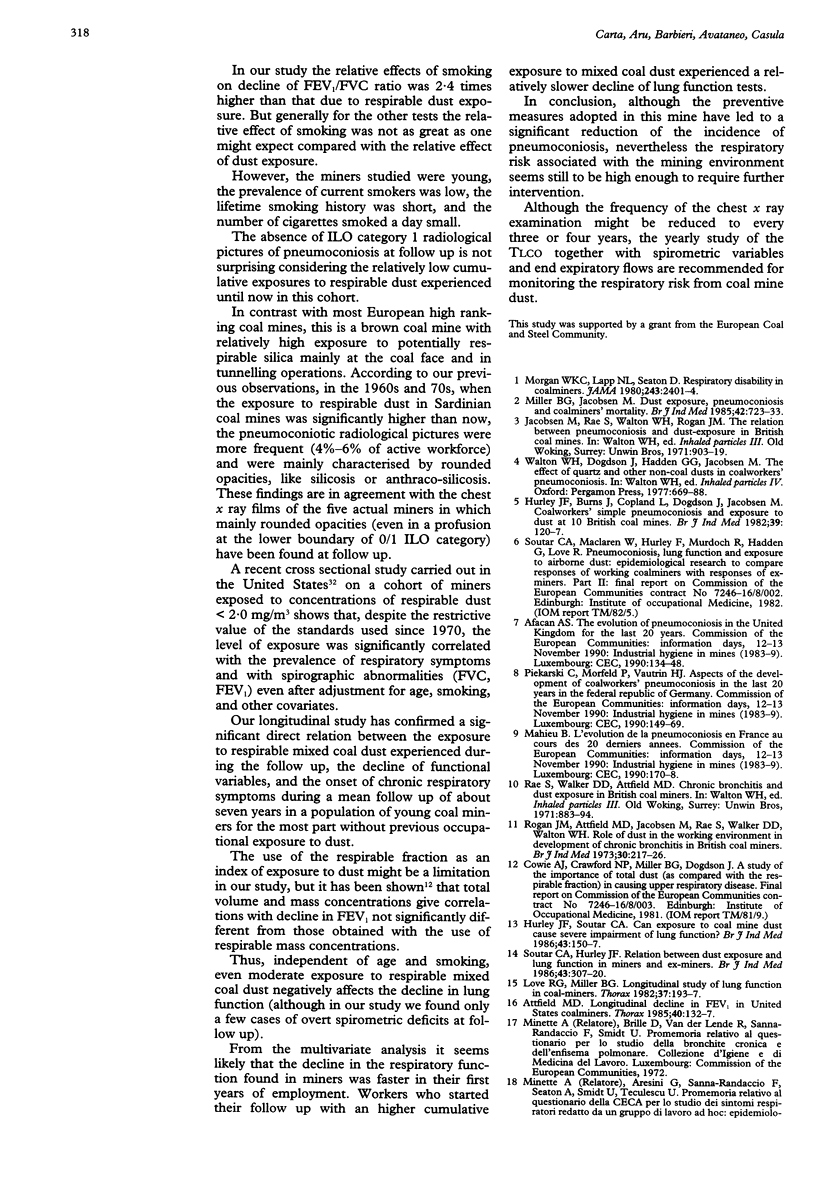
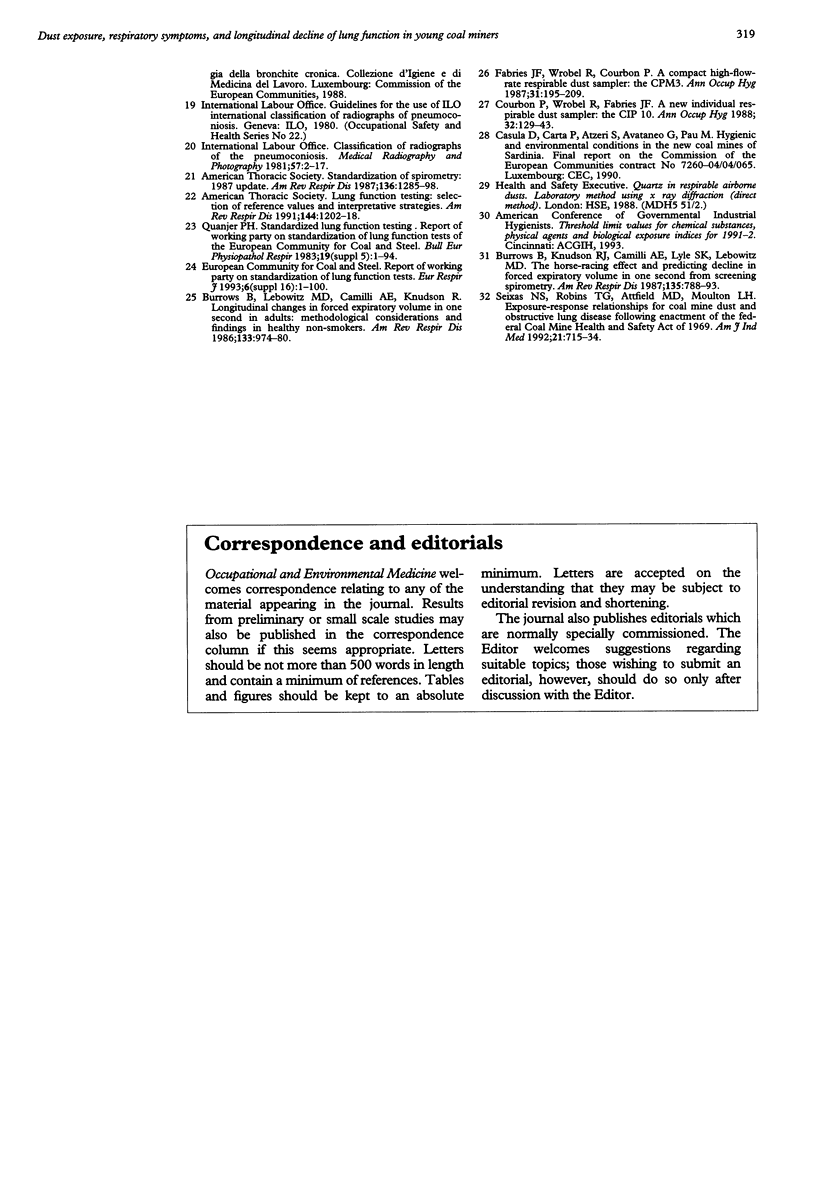
OBJECTIVES: To study the role of dust exposure on incidence of respiratory symptoms and decline of lung function in young coal miners. METHODS: The loss of lung function (forced vital capacity (FVC), forced expiratory volume in one second (FEV1), forced expiratory flow (MEF), carbon monoxide transfer factor (TLCO)) with time and the incidence of respiratory symptoms in 909 Sardinian coal miners (followed up between 1983 and 1993 with seven separate surveys) has been compared with the past and current individual exposures to respirable mixed coal dust. Multiple linear and logistic regression models were used simultaneously controlling for age, smoking, past occupational exposures, and other relevant covariates. RESULTS: According to the relatively low dust exposures experienced during the follow up few abnormal chest x ray films were detected. In the cross sectional analysis of initial data, significant associations between individual cumulative exposure to dust, decrements in FEV1 and MEFs, and increasing prevalence of respiratory symptoms were detected after allowing for the covariates included in the model. The yearly decline of FVC, FEV1, and single breath carbon monoxide transfer factor (TLCO/VA) was still significantly related to the individual exposure to dust experienced during the follow up, even after allowing for age, smoking, initial cumulative exposure to dust, and initial level of each functional variable. In logistic models, dust exposure was a significant predictor of the onset of respiratory symptoms besides age and smoking. CONCLUSIONS: The results show that even moderate exposures to mixed coal dust, as in our study, significantly affect lung function and incidence of symptoms of underground miners. Although the frequency of chest x ray examination might be fixed at every three or four years, yearly measurements of lung function (spirometry, MEFs, and TLCO) are recommended for evaluation of the respiratory risk from the coal mine environment to assess the need for further preventive interventions.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Attfield M. D. Longitudinal decline in FEV1 in United States coalminers. Thorax. 1985 Feb;40(2):132–137. doi: 10.1136/thx.40.2.132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burrows B., Knudson R. J., Camilli A. E., Lyle S. K., Lebowitz M. D. The "horse-racing effect" and predicting decline in forced expiratory volume in one second from screening spirometry. Am Rev Respir Dis. 1987 Apr;135(4):788–793. doi: 10.1164/arrd.1987.135.4.788. [DOI] [PubMed] [Google Scholar]
- Burrows B., Lebowitz M. D., Camilli A. E., Knudson R. J. Longitudinal changes in forced expiratory volume in one second in adults. Methodologic considerations and findings in healthy nonsmokers. Am Rev Respir Dis. 1986 Jun;133(6):974–980. doi: 10.1164/arrd.1986.133.6.974. [DOI] [PubMed] [Google Scholar]
- Hurley J. F., Burns J., Copland L., Dodgson J., Jacobsen M. Coalworkers' simple pneumoconiosis and exposure to dust at 10 British coalmines. Br J Ind Med. 1982 May;39(2):120–127. doi: 10.1136/oem.39.2.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurley J. F., Soutar C. A. Can exposure to coalmine dust cause a severe impairment of lung function? Br J Ind Med. 1986 Mar;43(3):150–157. doi: 10.1136/oem.43.3.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Love R. G., Miller B. G. Longitudinal study of lung function in coal-miners. Thorax. 1982 Mar;37(3):193–197. doi: 10.1136/thx.37.3.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller B. G., Jacobsen M. Dust exposure, pneumoconiosis, and mortality of coalminers. Br J Ind Med. 1985 Nov;42(11):723–733. doi: 10.1136/oem.42.11.723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan W. K., Lapp N. L., Seaton D. Respiratory disability in coal miners. JAMA. 1980 Jun 20;243(23):2401–2404. [PubMed] [Google Scholar]
- Rogan J. M., Attfield M. D., Jacobsen M., Rae S., Walker D. D., Walton W. H. Role of dust in the working environment in development of chronic bronchitis in British coal miners. Br J Ind Med. 1973 Jul;30(3):217–226. doi: 10.1136/oem.30.3.217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seixas N. S., Robins T. G., Attfield M. D., Moulton L. H. Exposure-response relationships for coal mine dust and obstructive lung disease following enactment of the Federal Coal Mine Health and Safety Act of 1969. Am J Ind Med. 1992;21(5):715–734. doi: 10.1002/ajim.4700210511. [DOI] [PubMed] [Google Scholar]
- Soutar C. A., Hurley J. F. Relation between dust exposure and lung function in miners and ex-miners. Br J Ind Med. 1986 May;43(5):307–320. doi: 10.1136/oem.43.5.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Standardized lung function testing. Report working party. Bull Eur Physiopathol Respir. 1983 Jul;19 (Suppl 5):1–95. [PubMed] [Google Scholar]