

Abstract
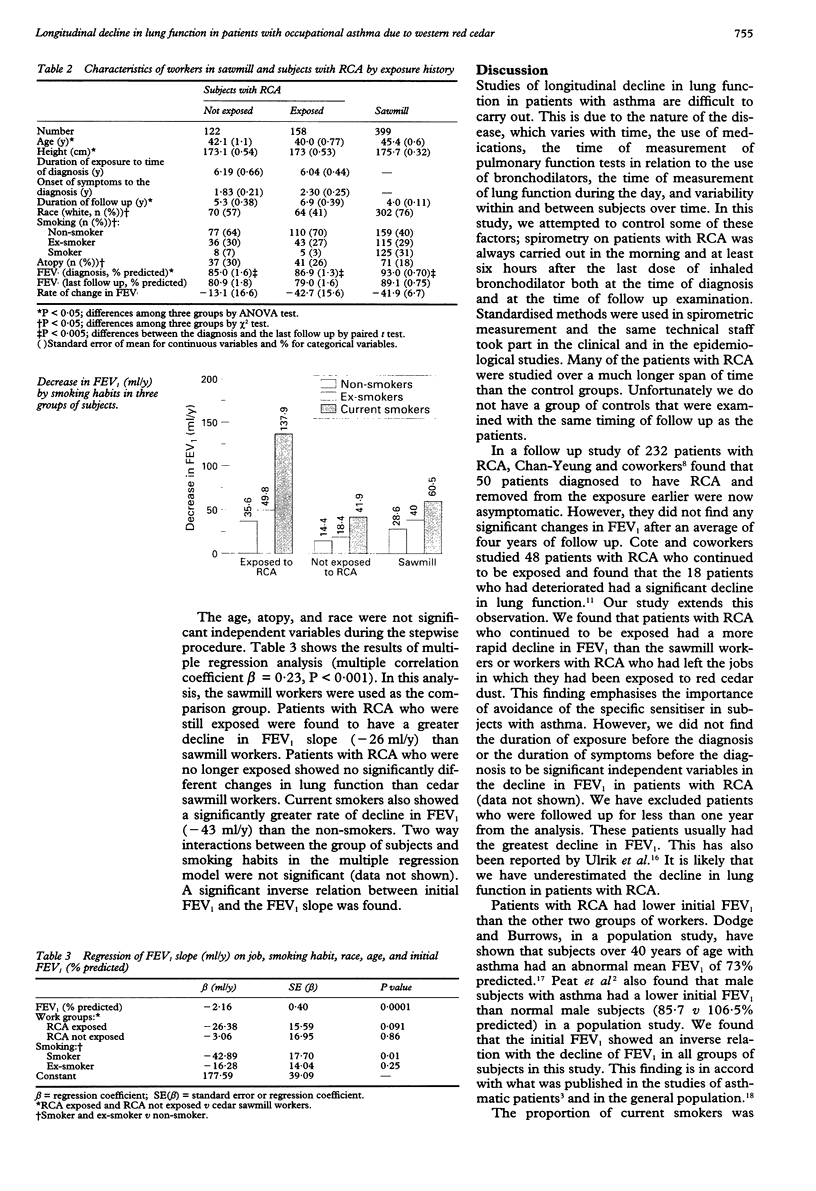
BACKGROUND: There are few reports about longitudinal changes in lung function in asthmatic patients. Patients with asthma had a greater loss of lung function than normal healthy adults. To date, there have been no studies about the longitudinal changes in lung function in patients with occupational asthma. METHODS: 280 male patients with red cedar asthma (RCA) who were followed up for at least one year were the study group. The exposed controls consisted of 399 male sawmill workers. Forced expiratory volume in one second (FEV1) was measured with a Collins water spirometer. Changes in FEV1 over time (FEV1 slope) were calculated by a two point method for each subject. Atopy was considered to be present if the subjects showed at least one positive response to three allergens by skin prick test. RESULTS: Multiple regression analysis was carried out to examine factors that might affect longitudinal decline in FEV1. Patients with RCA who were still exposed had a greater decline in FEV1 slope (-26 ml/y) than sawmill workers. Smokers also showed a greater rate of decline in FEV1 (-43 ml/y) than non-smokers. CONCLUSIONS: Patients with RCA who continued to be exposed had a greater rate of decline in FEV1 than sawmill workers. Early diagnosis of occupational asthma and removal of these patients from a specific sensitiser is important in the prevention of further deterioration of lung function and respiratory symptoms.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Blanc P. Occupational asthma in a national disability survey. Chest. 1987 Oct;92(4):613–617. doi: 10.1378/chest.92.4.613. [DOI] [PubMed] [Google Scholar]
- Brown P. J., Greville H. W., Finucane K. E. Asthma and irreversible airflow obstruction. Thorax. 1984 Feb;39(2):131–136. doi: 10.1136/thx.39.2.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burrows B., Knudson R. J., Camilli A. E., Lyle S. K., Lebowitz M. D. The "horse-racing effect" and predicting decline in forced expiratory volume in one second from screening spirometry. Am Rev Respir Dis. 1987 Apr;135(4):788–793. doi: 10.1164/arrd.1987.135.4.788. [DOI] [PubMed] [Google Scholar]
- Chan-Yeung M., Lam S., Koener S. Clinical features and natural history of occupational asthma due to western red cedar (Thuja plicata). Am J Med. 1982 Mar;72(3):411–415. doi: 10.1016/0002-9343(82)90497-1. [DOI] [PubMed] [Google Scholar]
- Chan-Yeung M., MacLean L., Paggiaro P. L. Follow-up study of 232 patients with occupational asthma caused by western red cedar (Thuja plicata). J Allergy Clin Immunol. 1987 May;79(5):792–796. doi: 10.1016/0091-6749(87)90212-0. [DOI] [PubMed] [Google Scholar]
- Cote J., Kennedy S., Chan-Yeung M. Outcome of patients with cedar asthma with continuous exposure. Am Rev Respir Dis. 1990 Feb;141(2):373–376. doi: 10.1164/ajrccm/141.2.373. [DOI] [PubMed] [Google Scholar]
- Crapo R. O., Morris A. H., Gardner R. M. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am Rev Respir Dis. 1981 Jun;123(6):659–664. doi: 10.1164/arrd.1981.123.6.659. [DOI] [PubMed] [Google Scholar]
- Dodge R. R., Burrows B. The prevalence and incidence of asthma and asthma-like symptoms in a general population sample. Am Rev Respir Dis. 1980 Oct;122(4):567–575. doi: 10.1164/arrd.1980.122.4.567. [DOI] [PubMed] [Google Scholar]
- Frew A. J., Kennedy S. M., Chan-Yeung M. Methacholine responsiveness, smoking, and atopy as risk factors for accelerated FEV1 decline in male working populations. Am Rev Respir Dis. 1992 Oct;146(4):878–883. doi: 10.1164/ajrccm/146.4.878. [DOI] [PubMed] [Google Scholar]
- Malo J. L. Compensation for occupational asthma in Quebec. Chest. 1990 Nov;98(5 Suppl):236S–239S. doi: 10.1378/chest.98.5_supplement.236s. [DOI] [PubMed] [Google Scholar]
- Mapp C. E., Corona P. C., De Marzo N., Fabbri L. Persistent asthma due to isocyanates. A follow-up study of subjects with occupational asthma due to toluene diisocyanate (TDI). Am Rev Respir Dis. 1988 Jun;137(6):1326–1329. doi: 10.1164/ajrccm/137.6.1326. [DOI] [PubMed] [Google Scholar]
- Meredith S. K., Taylor V. M., McDonald J. C. Occupational respiratory disease in the United Kingdom 1989: a report to the British Thoracic Society and the Society of Occupational Medicine by the SWORD project group. Br J Ind Med. 1991 May;48(5):292–298. doi: 10.1136/oem.48.5.292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peat J. K., Woolcock A. J., Cullen K. Rate of decline of lung function in subjects with asthma. Eur J Respir Dis. 1987 Mar;70(3):171–179. [PubMed] [Google Scholar]
- Proceedings of the Task Force on Guidelines for Standardizing Old and New Technologies Used for the Diagnosis and Treatment of Allergic Diseases. Washington, DC. June 18-19, 1987. J Allergy Clin Immunol. 1988 Sep;82(3 Pt 2):487–526. doi: 10.1016/0091-6749(88)90958-x. [DOI] [PubMed] [Google Scholar]
- Schachter E. N., Doyle C. A., Beck G. J. A prospective study of asthma in a rural community. Chest. 1984 May;85(5):623–630. doi: 10.1378/chest.85.5.623. [DOI] [PubMed] [Google Scholar]
- Ulrik C. S., Backer V., Dirksen A. A 10 year follow up of 180 adults with bronchial asthma: factors important for the decline in lung function. Thorax. 1992 Jan;47(1):14–18. doi: 10.1136/thx.47.1.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ulrik C. S., Lange P. Decline of lung function in adults with bronchial asthma. Am J Respir Crit Care Med. 1994 Sep;150(3):629–634. doi: 10.1164/ajrccm.150.3.8087330. [DOI] [PubMed] [Google Scholar]