

Abstract
Abstract
Introduction
Reducing neonatal deaths in premature infants in low- and middle-income countries is key to reducing global neonatal mortality. International neonatal networks, along with patient registries of premature infants, have contributed to improving the quality of neonatal care; however, the involvement of low-to-middle-income countries was limited. This project aims to form an international collaboration among neonatal networks in Asia (AsianNeo), including low-, middle- and high-income countries (or regions). Specifically, it aims to determine outcomes in sick newborn infants, especially very low birth weight (VLBW) infants or very preterm infants, with a view to improving the quality of care for such infants.
Methods and analysis
Currently, AsianNeo comprises nine neonatal networks from Indonesia, Japan, Malaysia, Philippines, Singapore, South Korea, Sri Lanka, Taiwan and Thailand. AsianNeo will undertake the following four studies: (1) institutional questionnaire surveys investigating neonatal intensive care unit resources and the clinical management of sick newborn infants, with a focus on VLBW infants (nine countries/regions); (2) a retrospective cohort study to describe and compare the outcomes of VLBW infants among Asian countries and regions (four countries/regions); (3) a prospective cohort study to develop the AsianNeo registry of VLBW infants (six countries/regions); and (4) implementation and evaluation of educational and quality improvement projects in AsianNeo countries and regions (nine countries/regions).
Ethics and dissemination
The study protocol was approved by the Research Ethics Board of the National Center for Child Health and Development, Tokyo, Japan (reference number 2020–244, 2022–156). The study findings will be disseminated through educational programmes, quality improvement activities, conference presentations and medical journal publications.
Keywords: Mortality, Neonatal intensive & critical care, NEONATOLOGY, International health services
Strengths and limitations of this study.
One of the strengths of this study will be the participation of leading neonatologists or paediatricians from each country/region in this project as steering committee members, which will encourage the engagement of stakeholders from each country/region.
Another strength of this study will be the wide variations in neonatal intensive care unit (NICU) systems, resource availabilities, ethnicities and cultural backgrounds among participating countries/regions that will provide unique opportunities to assess how variations identified can affect clinical practices in NICUs and infant outcomes.
One of the limitations will be that not all NICUs in each country/region will participate in this project, and the proportion of participation varies among countries/regions.
All planned studies in this project will be observational studies and a potential risk of bias and confounding may limit the study findings.
Introduction
Reducing neonatal deaths is an urgent global health issue. The Sustainable Development Goals, adopted by the United Nations Sustainable Development Summit in 2015, aim to reduce neonatal mortality to as low as 12 per 1000 live births by 2030 and reduce the under-5 mortality rate to 25 per 1000 live births.1 Neonatal mortality rates have decreased in the last few decades; however, the pace of reduction has been slower for under-5 mortality. Of all deaths under the age of 5 years in 2018, 47% were neonatal deaths.2 Most neonatal deaths occur in low- and middle-income countries in Africa (neonatal mortality, 27 per 1000 live births), Eastern Mediterranean areas (26 per 1000 live births) and Southeast Asia (20 per 1000 live births).2 The leading cause of neonatal death is premature birth, followed by asphyxia.3 Therefore, the prevention of neonatal deaths in premature infants and birth asphyxia in low- and middle-income countries is key to reducing global neonatal mortality.
Over the last 30 years, various regional, national and international neonatal networks (collaborative groups of people and facilities dedicated to the care of newborn infants) accompanied with patient registries for very low birth weight (VLBW) or very preterm infants have been established, primarily in high-income countries.4,6 Quality improvement with benchmarking within and between institutions and clinical research in these neonatal networks has contributed to a reduction in neonatal mortality and severe complications in fragile premature infants.7 8 Furthermore, some neonatal networks in high-income countries have initiated international collaboration among neonatal networks, such as the International Network for Evaluation of Outcomes in Neonates (iNeo).9,11 This international collaboration is useful in benchmarking infants’ outcomes against other countries, understanding differences in clinical practice between countries and improving the quality of care for sick newborn infants through learning exchanges.9 12 However, many low- and middle-income countries have not been successful in developing their own neonatal networks and patient registries, and international collaboration among them has been limited.13 In Asia, only Japan participates in the iNeo. The potential barriers for many Asian countries (especially low- and middle-income countries) in joining such international collaborations include the lack of population-based patient registries, a lack of research funding and resources and limited incentives to collaborate with other countries.13 The effectiveness of an international neonatal network collaboration that includes both low- and middle-income countries and high-income countries remains to be evaluated; however, such collaboration may provide a unique opportunity not only for low- and middle-income countries, but also for high-income countries to learn from each other. Newborn care in high-income countries may not always be better than that in low- and middle-income countries; therefore, the former can learn from the latter in some areas (eg, the promotion of breastfeeding and kangaroo mother care).14,16
In this context, the Asian Neonatal Network Collaboration (AsianNeo), comprising nine neonatal networks spanning low-, middle- and high-income countries or regions (Indonesia, Japan, Malaysia, Philippines, Singapore, South Korea, Sri Lanka, Taiwan and Thailand), was established with the aim of providing an international platform for paediatricians or neonatologists, researchers and other healthcare providers.17 Building on the framework provided by the AsianNeo, the present study aims to evaluate and compare perinatal and neonatal medical systems, clinical practices and outcomes concerning sick newborn infants, especially VLBW or very preterm infants, to improve the quality of care in sick newborn infants in AsianNeo countries/regions. For this purpose, in this study, we will perform four projects including1 an institutional-level questionnaire survey (nine countries/regions),2 a retrospective cohort study of VLBW infants (four countries/regions),3 a prospective registry and cohort study of VLBW infants (six countries/regions) and4 a quality improvement study (nine countries/regions).
Methods and analyses
AsianNeo structure
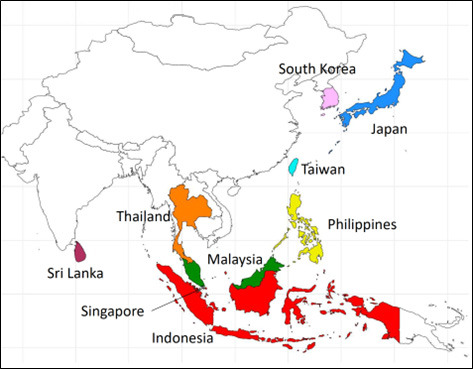
AsianNeo is an international collaboration that includes national and regional neonatal networks in Asian countries. Nine neonatal networks already participate in AsianNeo from the following countries: Indonesia, Japan, Malaysia, the Philippines, Singapore, South Korea, Sri Lanka, Taiwan and Thailand (figure 1). Moving forward, AsianNeo will be open to additional member countries/regions, welcoming the participation of other countries and regions. New countries that are not currently members of the AsianNeo may apply for membership through the AsianNeo website (https://asian-neo.org/index.html), and on approval by all the steering committee members, may join the AsianNeo.17 As shown in online supplemental table 1, there are wide variations in income levels, economic equality and baseline perinatal indexes (birth rates, preterm birth rates, neonatal mortalities, etc) among the participating countries/regions. The governance structure of AsianNeo is shown in online supplemental s-Figure 1. The AsianNeo steering committee consists of one or two representatives from each neonatal network (ie, voting members). Steering committee members comprise experienced neonatologists or paediatricians, who are leaders in the field of neonatology in each country/region. The steering committee holds monthly meetings (mostly online) to discuss collaboration activities. AsianNeo invites stakeholders both in and out of member countries/regions to provide advice on its activities. These stakeholders may include academic paediatric organisations, government organisations and funding agencies of member countries, regions and global organisations. The AsianNeo Bureau is housed at the National Center for Child Health and Development (NCCHD), Tokyo, Japan.
Figure 1. Asian Neonatal Network Collaboration countries or regions.
Characteristics of AsianNeo member countries or regions
In preparation for the AsianNeo project, we conducted a brief network-level survey to assess the healthcare systems, resources and clinical practices of each country/region. We asked one representative from each network (country/region) in AsianNeo, familiar with the overall picture of the systems and clinical practices of neonatal intensive care units (NICUs) in their country/region, to respond to a country-level or region-level questionnaire. In most networks, births of newborn infants occur at hospitals or clinics, except in Indonesia and the Philippines, where there are still a substantial number of home births (online supplemental table 2). All networks, including those in low- and middle-income countries, report resuscitating extremely preterm infants at <26 weeks of gestational age, although there are slight differences in the lowest gestational age (range, 22–26 weeks) and birth weight (range, <300–600 g) of very preterm infants who receive active resuscitation (limit of viability). Among the nine networks, five (Japan, Korea, Malaysia, Taiwan and Thailand) have nationwide patient registry databases of VLBW infants, where data and outcomes are prospectively collected. Population coverage of the databases ranges from 50% to close to 90%. The availability of medications and medical devices for monitoring or treatment varies among the networks (figure 2, online supplemental table 3). Despite some medical devices (eg, incubators, continuous positive airway pressure, pulse oximeters) being generally available in all nine networks, the availability of many other medications and devices is limited in some low- and middle-income countries.
Figure 2. Availability of treatment and diagnostic tests. The information in the table is based on the personal understanding of the steering committee members regarding NICU care in their respective countries. The words of ‘Mostly’, ‘Often’, ‘Sometimes’, ‘Rarely’ and ‘Never’ indicate the proportions of 80–100%, 50–79%, 20–49%, 1–19%, and <1 %, respectively. *Available only in level-III NICUs. aEEG, amplitude-integrated electroencephalogram; CO2, carbon dioxide; CPAP, continuous positive airway pressure; HFO, high-frequency oscillation; SpO2, oxygen saturation.

Project 1: an institutional-level questionnaire survey
To understand differences in perinatal and neonatal healthcare systems, resources and clinical management of sick newborns in Asian countries/regions, we plan to conduct an international questionnaire survey at the institutional level concerning the human and physical resources of NICUs (eg, types of NICUs, care levels, patient volume, workforce, availability of devices and facilities) and clinical management of very preterm infants (eg, resuscitation, respiration, circulation, nutrition/feeding, neurology and follow-up systems). This questionnaire is written in English and is coded using an online SurveyMonkey tool.18 Responses to the questionnaire will be written in English whenever possible. In non-English-speaking countries, where responding to the survey in English is challenging, respondents will complete the questionnaire in their native language and their responses will be translated into English. An invitation to complete the survey will be sent by the representative of each neonatal network to all NICUs participating in nine AsianNeo countries/regions. When the survey results are published, individual facility names will be anonymised and unidentifiable, excluding acknowledgements concerning participation in the survey. NICU resources and clinical management of preterm infants will be compared between countries/regions. Information obtained from responses to this survey will be essential to understanding the current situation of neonatal healthcare systems and resources and the clinical management of sick newborn infants in AsianNeo countries/regions.
Project 2: a retrospective cohort study of VLBW infants
To describe and compare outcomes in sick newborns in Asian countries/regions, a retrospective cohort study of VLBW infants will be conducted in four networks, namely, Japan, Malaysia, Taiwan and Thailand, using existing nationwide databases of VLBW infants. After these networks have approved the study protocol, the data of VLBW infants born in these five networks will be sent to the AsianNeo Bureau in NCCHD in a secure manner with password protection. Four other countries (Indonesia, the Philippines, Singapore and Sri Lanka) do not currently have a nationwide patient database; however, some of the NICUs in these networks may consider participating either through submitting their existing individual NICU database to a similar password-protected platform or retrospectively collecting data concerning VLBW infants in their NICUs.
Eligibility criteria of the database
All VLBW or very preterm infants (birth weight <1500 g or birth at <32 weeks of gestation) born in or admitted to hospitals participating in each neonatal network within 48 hours of birth from 2015 to 2023 (or for a part of this period) will be eligible for this study. Some networks have even more limited inclusion criteria; therefore, those networks are not required to provide data on infants not included in their registry. For example, the registry of the Taiwan Neonatal Network (TNN) includes infants born at ≤29 weeks gestational age or those with birth weights ranging from 401 g to 1500 g. Therefore, the TNN will not provide data on infants born at 30–31 weeks gestational age with a birth weight of ≥1500 g who are eligible for this study.
Database variables
The variables included in this cohort study are summarised in online supplemental s-Table 1. A common variable list was developed through evaluating the types and definitions of the variables used in the participating networks and harmonising the variable definitions among the networks.
Perinatal and neonatal baseline characteristics
Baseline characteristic data concerning the study infants will include perinatal variables (maternal age, hypertension during pregnancy, maternal antenatal steroid and delivery mode (caesarean section or vaginal delivery)) and neonatal variables (gestational age at birth, birth weight, sex, Apgar score at 1 min and 5 min and outborn infants transferred from lower-level perinatal centres within 2 days after birth).
Primary and secondary outcomes
The primary outcome for the comparison between countries and regions will be all-cause mortality prior to NICU discharge. The main secondary outcomes will include the following five major neonatal morbidities: (1) severe intraventricular haemorrhage (IVH), defined as grade III or IV IVH according to Papile’s classification19; (2) necrotising enterocolitis, defined as stage ≥2 according to Bell’s criteria or requiring surgical intervention; (3) retinopathy of prematurity requiring treatment, including laser treatment and intraocular injections of anti-vascular endothelial growth factor agents; (4) chronic lung disease, defined as supplemental oxygen use or any respiratory support at 36 weeks post-menstrual age; and (5) late-onset sepsis, defined as culture-positive sepsis after 72 hours of birth.20 Respiratory distress syndrome, air leak or pneumothorax, early onset sepsis with positive culture within 72 hours of birth, patent ductus arteriosus requiring pharmacological or surgical treatment, cystic periventricular leukomalacia, the number of days on mechanical ventilation and the number of days on continuous positive airway pressure will also be assessed.
Analyses
Descriptive analyses of baseline factors
The perinatal and neonatal baseline characteristics of the study infants will be summarised as counts and percentages for categorical variables, and as means and SDs or medians and IQRs for continuous variables. A χ2 test for categorical variables and analysis of variance or Mood’s median test for continuous variables will be used to compare the baseline characteristics among all networks.
Comparisons of outcomes between networks
Pairwise comparisons of the primary and secondary outcomes between specific networks will be performed using multivariable regression models adjusted for potential confounders (eg, gestational age at birth, small for gestational age or birth weight z-score, outborn status, sex and Apgar score at 1 min of birth). Generalised linear mixed models will be used to account for the clustering of infants within networks and units. Calculated adjusted ORs and 95% CIs for each network compared with a reference network (Japan) will be graphically displayed as forest plots. In addition, standardised outcome ratios for the primary and secondary outcomes will be calculated for each network using indirect standardisation. The standardised outcome ratios will be calculated from the observed outcome rates in each network divided by the expected rates estimated using multivariate regression models derived from the samples from all other networks. The standardised outcome ratios will be displayed graphically using funnel plots with 95% prediction intervals to compare between the networks. Complete case analysis will be used.
Analyses of the associations between institutional-level NICU resources or clinical practice and clinical outcomes for VLBW infants
Institutional-level information regarding NICU resources and clinical management of VLBW infants surveyed in Project 1 will be combined with patient-level data in this retrospective cohort study. The association between institutional-level NICU characteristics and the clinical outcomes of VLBW infants will then be assessed using generalised mixed-effect models with individual-level analyses, including institutions as a random effect.
Data security (data transfer/data centre)
De-identified patient data with unique AsianNeo facility codes assigned by each network will be stored in an Excel file in each network and locked with a password. The data file will be securely sent from each network to the AsianNeo Bureau at the NCCHD, Tokyo, Japan, via an online file transfer using Dropbox (Dropbox, California, USA). The password for the Excel data file will be sent from each network to the AsianNeo Bureau. The transferred data will be stored with password protection. Access to the data will be restricted, and persons who handle the data must obtain permission from the AsianNeo steering committee. A table linking the unique AsianNeo facility codes with facility names will be stored and managed by representatives from each country/region.
Sample size and others
The sample size of this study will be determined based on convenience sampling (data availability in each country/region). All statistical analyses were performed using R Statistical Software (V.4.3.1; R Core Team 2021) with a two-sided significance level of 0.05.21
Project 3: a prospective registry and cohort study of VLBW infants
To establish a prospective patient registry of sick newborn infants (eg, VLBW infants) among AsianNeo countries/regions through harmonising database variable definitions, we will develop an AsianNeo registry of VLBW infants using the same variable set and common variable definitions to perform a cohort study in six countries/regions (Indonesia, Japan, Malaysia, Philippines, Taiwan and Thailand). For this purpose, the definitions of the data variables among the participating networks have been harmonised in as far as possible. For networks that do not have their own VLBW infant registry (Indonesia, Philippines), we will develop the AsianNeo registry database using Research Electronic Data Capture (REDCap) tools hosted at the NCCHD that enable caregivers or research assistants to enter the information on VLBW infants online on their mobile phones or personal computers.22 23 Automated data checkers will be in place in the REDCap tool. The training of data collectors in each country/regions will be provided online by the AsianNeo bureau.
Eligibility criteria and database variables
All VLBW or very preterm infants (birth weight <1500 g or birth at <32 weeks of gestation) born in or admitted to hospitals participating in each neonatal network within 48 hours of birth from 2024 to 2026 will be eligible for this study. The sample size of this study will be determined based on convenience sampling (data availability in each country/region). The same database variables as the Project 2 (the same perinatal and neonatal baseline characteristics and the same primary and secondary outcomes) will be assessed (online supplemental s-Table 1).
Cause of death algorithm
Cause of death data comprise important information, with definitions or categorisations often varying among countries; therefore, we have developed a common algorithm to describe the cause of death of VLBW infants in the registry, with reference to previous studies (figure 3).24,26 This algorithm has been approved by the AsianNeo steering committee. Each participating network will attempt to collect cause of death data using this common algorithm.
Figure 3. Cause of death algorithm. abn, abnormality; ARD, acute respiratory distress; CLD, chronic lung disease; FIP, focal intestinal perforation; IVH, intraventricular haemorrhage; NEC, necrotising enterocolitis.

Analyses
The same analysis used in Project 2 will be used in Project 3. In addition, cause-specific mortality will be compared between the networks using generalised mixed-effect models. Furthermore, changes in clinical outcomes among VLBW infants between 2015 and 2020 and after 2020 will be evaluated for the four neonatal networks participating in Project 2.
Project 4: education programmes and quality improvement of care
Based on the information obtained in Projects 1–3, we will develop and implement educational programmes and quality improvement activities among all nine AsianNeo country/regions and evaluate the effectiveness of their implementations. We will hold online conferences to share the results of Projects 1–3 with participating NICUs. Based on information obtained from Projects 1–3, we will identify areas (NICU systems, clinical practices and outcomes) that need to be improved in each country, region or NICU and develop quality improvement projects to address challenges identified in these areas. Quality improvement projects will comprise the identification of such challenges, plan for practice changes, evaluation and monitoring of outcomes and practices and follow Plan-Do-Study-Act cycles.27 Furthermore, this international quality improvement project will include regular meetings for mutual learning from other countries/regions and the dispatch of experts from high-performing NICUs to those requiring improvement. The effectiveness of the quality improvement projects will be assessed through comparing outcomes before and after the implementation of the quality improvement projects using data from the prospective VLBW infant registry developed in Project 3 (six participating countries/regions).
Patient and public involvement statement
There is no plan to involve patient/participants and public in designing or any phase of the study.
Ethics and dissemination
All methods were carried out in accordance with relevant guidelines and regulations. This study protocol was approved by the Research Ethics Board of the NCCHD, Tokyo, Japan (reference number 2020–244, 2022–156). In addition, the research ethics approvals were obtained in Japan, Taiwan, Thailand and Philippines for this study. In Indonesia and Malaysia, the research ethics approval for this study will be applied before using individual patent data. Because South Korea, Singapore and Sri Lanka participate only in the unit-level questionnaire survey, these countries do not require the research ethics approval other than the one that has been obtained in the NCCHD, Tokyo, Japan. Each network will obtain regulatory or research ethics approval or the equivalent from its local committee to send de-identified data from the network to the AsianNeo Bureau at the NCCHD. All networks signed data transfer agreements with the NCCHD before data transfer. No data identifiable at the patient level will be collected or transmitted to the AsianNeo bureau, and only aggregate data will be reported to the public. Written informed consent was obtained from each participant in Project 1 (questionnaire survey). For Projects 2–3 (retrospective and prospective cohort studies), an opt-out approach for informed consent was approved by the research ethics board of the NCCHD. This is because these studies will collect only de-identified data without any study interventions on patients. However, according to local or regional regulatory requirements or research ethics board requirements, some units or countries may still require written informed consent from each patient registered in the database.
To disseminate the study findings, we will develop educational programmes and quality improvement activities using Plan-Do-Study-Act cycles among AsianNeo countries/regions as in Project 4. In addition, the study findings will be presented in national or international medical conferences and published in peer-reviewed medical journals.
Data ownership and intellectual properties
The survey and patient data collected in AsianNeo will be used for various projects (eg, clinical research, quality improvement of care and policymaking) proposed by any individual or group (paediatricians, epidemiologists, researchers or policymakers) after approval from all AsianNeo steering committee members of the countries/regions that provide the data to the project. All neonatal networks have the right to decline participation in certain projects or decline the use of data collected in their countries/regions for such projects. A network could cease to participate in the study at any time.
The research programme will be administered by the AsianNeo Bureau, housed at the NCCHD, Tokyo, Japan. The policies and procedures for data transfer, application for data use, data analysis and publication of the results will be finalised in discussion with steering committee members, and agreements will be signed between each network and the AsianNeo Bureau at the NCCHD.
Strength and limitations
The strengths of this study will be as follows. First, leading neonatologists or paediatricians in the area of neonatology in each country/region will participate in this project as steering committee members. Involving such a nationwide network of healthcare providers in NICUs will encourage the engagement of stakeholders from each country/region. Second, compared with other international collaborations, such as the iNEO, which involves countries across the globe, this project fosters geographically close collaboration in Asia. This will facilitate having regular online meetings with minimal time differences and may help promote mutual visits to learn from each other’s countries/regions. Third, wide variations in NICU systems, resource availabilities, ethnicities and cultural backgrounds among participating countries/regions will provide unique opportunities to assess how variations identified can affect clinical practices in NICUs and infant outcomes. Finally, the openness of this collaboration, which welcomes additional future participation from other countries/regions, will be helpful in expanding collaboration across Asia.
This study has some limitations. One major limitation is that not all NICUs in each country/region will participate in this project, and the proportion of participation varies among countries/regions. Across most networks, large tertiary or quaternary NICUs are more likely to participate in this project rather than small or secondary NICUs, which may limit the generalisability of our results. However, the potential success of the AsianNeo project may prompt non-participating NICUs to join in the future. Five networks already have nationwide patient registries for VLBW or very preterm infants; however, the population coverage in some registries is suboptimal (<80%), which may limit the generalisability of results derived from registry data. In addition, the lack of patient registries in the other four networks is likely to limit our retrospective evaluation at a patient level. We hope that Project 3 to address Aim 3 (a prospective registry of VLBW infants) will resolve this issue through developing prospective patient registries in these four networks. Finally, all planned studies in this project will be observational studies; therefore, a potential risk of bias and confounding may limit the findings. However, we hope that this international collaboration will evolve into a platform for promoting international multicentre clinical research in Asia.
supplementary material
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Funding: This study is supported by grants from the National Center for Child Health and Development (No. 30-16 in 2018–2020; No. 2021B-8 in 2021–2023; No. 2024B-1 in 2024–2026) and JSPS KAKENHI (Grant no: JP22K07929) in 2022–2024.
Prepub: Prepublication history and additional supplemental material for this paper are available online. To view these files, please visit the journal online (https://doi.org/10.1136/bmjopen-2023-082712).
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Not applicable.
Map disclaimer: The inclusion of any map (including the depiction of any boundaries therein), or of any geographical or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Collaborators: From Indonesia Neonatal Network: Isra Firmansyah, Pertin Sianturi, Eny Yantri, Afifa Ramadanti, Henri Azis, Ied Imelda, Rizalya Dewi, Mustarim, Benny Sana Putra, Jumnalis, Leni Ervina, Andhika Tiurmaida Hutapea, Rinawati Rohsiswatmo, Nadia Dwi Insani, Agnes Yunie Purwita Sari, Ellen Sianipar, Naomi Esthernita Dewanto, Thomas Harry Adoe, Arif Budiman, Arief Budiman, Tetty Yuniarti, Adhie Nur Radityo S, Dwi Hidayah, Tunjung Wibowo, Kartika Darma Handayani, Risa Etika, Dina Djojo Husodo, Brigitta Ida Resita Vebrianti Corebima, Retno Wulandari, Made Sukmawati, I Ketut Adi Wirawan, Pudji Andayani, Made Yuliari, Rocky Wilar, Ema Alasiry, James Thimoty, Sandra Bulan
From Neonatal Reserach Network of Japan: Takashi Nasu, Yukiteru Tachibana, Ayumu Noro, Toshihiko Mori, Ken Nagaya, Masaru Shirai, Toru Ishioka, Toshiya Saito, Yosuke Kaneshi, Masaki Kobayashi, Nobuko Shiono, Nobuhiro Takahashi, Yusuke Ohkado, Tatsuro Satomi, Mika Nakajima, Eiki Nakamura, Tomofumi Ikeda, Genichiro Sotodate, Mari Ishii, Toru Huchimukai, Takahide Hosokawa, Rikio Suzuki, Masatoshi Sanjo, Michiya Kudo, Takushi Hanita, Hirokazu Arai, Masato Ito, Satoshi Niwa, Masanari Kawamura, Satoshi Watanabe, Yousuke Sudo, Hiroshi Yoshida, Tsutomu Ishii, Takashi Imamura, Maki Sato, Yoshiya Yukitake, Yayoi Miyazono, Goro Asada, Yumi Kono, Yasuaki Kobayashi, Hiroshi Suzuki, Yasushi Oki, Kenji Ichinomiya, Toru Fujiu, Hideaki Fukushima, Tetsuya Kunikata, Fumihiko Namba, Masaki Shimizu, Shigeharu Hosono, Chika Morioka, Motoichiro Sakurai, Hiroshi Matsumoto, Naoto Nishizaki, Satoshi Toishi, Harumi Otsuka, Masahiko Sato, Kenichiro Hirakawa, Kenichiro Hosoi, Keiji Goishi, Yuji Ito, Kyone Ko, Hiromichi Shoji, Atsuo Miyazawa, Yuko Nagaoki, Naoki Ito, Ken Masunaga, Reiko Kushima, Sakae Kumasaka, Manabu Sugie, Daisuke Haruhara, Masahiro Kobayashi, Satsuki Kakiuchi, Riki Nishimura, Kaoru Okazaki, Hitoshi Yoda, Atsushi Nakao, Ichiro Morioka, Daisuke Ogata, Fumihiko Ishida, Daisuke Nishi, Miho Sato, Ayako Fukuyama, Kuriko Nakamura, Kanji Ogo, Masahiko Murase, Katsuaki Toyoshima, Isamu Hokuto, Maha Suzuki, Atsushi Uchiyama, Yoshio Shima, Hidehiko Nakanishi, Atsushi Nemoto, Akira Shimazaki, Tatsuya Yoda, Yukihide Miyosawa, Takehiko Hiroma, Yosuke Shima, Gen Kuratsuji, Yoshihisa Nagayama, Tohei Usuda, Rei Kobayashi, Hiroaki Imamura, Takeshi Hutani, Taketoshi Yoshida, Azusa Kobayashi, Kazuhide Ohta, Shuya Nagaoki, Yasuhisa Ueno, Toru Ando, Ritsuyo Taguchi, Takashi Okuno, Hiroshi Yamamoto, Takeshi Arakawa, Shinji Usui, Yasushi Uchida, Takashi Tachibana, Tokuso Murabayashi, Tadayuki Kumagai, Shigeru Oki, Reiji Nakano, Taizo Ueno, Mitsuhiro Ito, Masami Shirai, Akira Oishi, Hikaru Yamamoto, Hiroshi Takeshita, Yuichi Kato, Masashi Hayashi, Kuniko Ieda, Koji Takemoto, Toshiyuki Ono, Masashi Miyata, Makoto Ohshiro, Masanori Kowaki, Osamu Shinohara, Yasunori Koyama, Osuke Iwata, Takahiro Muramatsu, Akinobu Taniguchi, Naoki Kamata, Hiroshi Uchizono, Kanemasa Maki, Takahide Yanagi, Kenji Nakamura, Masahito Yamamoto, Jitsuko Ohira, Machiko Sawada, Kozue Shiomi, Ryosuke Araki, Daisuke Kinoshita, Ryuji Hasegawa, Akira Nishimura, Hiroshi Komatsu, Koji Nozaki, Shinsuke Adachi, Toru Yamakawa, Masahiko Kai, Hiroshi Sumida, Hirotaka Minami, Kenji Mine, Reiko Negi, Satoru Ogawa, Ryoko Yoshinare, Yasuyuki Tokunaga, Kiyoaki Sumi, Akihiro Takatera, Atsushi Ogihara, Satoshi Onishi, Taho Kim, Hiroyuki Ichiba, Misao Yoshii, Hitomi Okabe, Yoshio Kusumoto, Shinya Hirano, Hiroshi Mizumoto, Yae Michinomae, Makoto Nabetani, Takeshi Morisawa, Masaaki Ueda, Takahiro Okutani, Masaru Yamakawa, Kazumichi Fujioka, Tomoaki Ioroi, Takeshi Utsunomiya, Seiji Yoshimoto, Tamaki Ohashi, Toshiya Nishikubo, Ken Kumagaya, Akiko Tamura, Masumi Miura, Yuki Hasegawa, Rie Kanai, Kei Takemoto, Koichi Tsukamoto, Misao Kageyama, Takashi Nakano, Hironobu Tokumasu, Moriharu Sugimoto, Rie Fukuhara, Yutaka Nishimura, Seiichi Hayakawa, Yasuhiko Sera, Masahiro Tahara, Shinosuke Fukunaga, Keiko Hasegawa, Kazumasa Takahashi, Hiroshi Tateishi, Tomomasa Terada, Takashi Yamagami, Takahiko Saijo, Kosuke Koyano, Toru Kuboi, Osamu Matsuda, Shinosuke Akiyoshi, Takahiro Motoki, Yoichi Kondo, Yusei Nakata, Hideaki Harada, Masayuki Ochiai, Toshinori Nakashima, Toshiharu Hikino, Shutaro Suga, Mitsuaki Unno, Hiroshi Kanda, Yasushi Takahata, Hiroyasu Kawano, Takayuki Kokubo, Toshimitsu Takayanagi, Mikio Aoki, Muneichiro Sumi, Fumiko Kinoshita, Tsutomu Ogata, Kei Inomata, Masanori Iwai, Naoki Fukushima, Koichi Iida, Mitsushi Goshi, Yuki Kodama, Shuichi Yanagibe, Yuko Maruyama, Takuya Tokuhisa, Yoriko Kisato, Tatsuo Oshiro, Kazuhiko Nakasone, Asao Yara
From Korean Neonatal Network: Yun Sil Chang, Ee-Kyung Kim, ChangWon Choi, Young-Ah Youn, Jae Won Shim, Juyoung Lee, Jang Hoon Lee, Soon Min Lee, Ga Won Jeon, Byong Sop Lee, Jin A Lee, Jae Woo Lim, Su Jin Cho.
From Malaysia National Neonatal Network: Zuraidah Abdul Latif, Zainah Shaikh Hedra, Baizura Jamaluddin, Hasri Hafidz, Zainab Ishak, Geok Hoon Ngian, Chiong Hung Kiew, Mehala Devi Baskaran, Maslina Mohamad, Chee Sing Wong, Rozitah Razman, Maneet Kaur, Ann Cheng Wong, Choo Hau Lim, Maizatul Akmar, Sheila Gopal Krishnan, Chae Hee Chieng, Chong Meng Choo, Eric Boon- Kuang Ang, Shiau Chuen Diong, Angeline Seng- Lian Wan, Sharifah Huda Engku Alwi, Kwee Ching See, Rohani Abdul Jalil, Agnes Suganthi, Mei Ling Lee, Ee Lee Ang, Pauline Poh-Ling Choo, Lee Ser Chia, Azanna Ahmad Kamar, Anand Mohan A/L Mohana Lal, Zainab Ishak, Agnes Huei- Hwen Foo, Abdul Nasir Mohamed Abdul Kadher
From Philippines: Ma. Lourdes Imperial, Belen Velasco, Ma. Esterlita V. Uy, Daisy Evangeline Garcia, Eleanor DR Cuarte, Jacinto Blas Mantaring III
From Singapore: Bin Huey Quek, Woei Bing Poon, Zubair Amin
From Sri Lanka: Saman Kumara, Kapila Jayaratne, Nethmini Thenuwara
From Taiwan Neonatal Network: Ming-Chou Chiang, Lan-Wan Wang, Chih-Cheng Chen, Xiao-Ping Wang, Hsiu-Ling Chen, Yi-Li Hung, Yung Chieh Lin, Pen-Hua Su, Yung-Ning Yang, Po-Nein Tsao, Shu-Chi Mu, Hung-Chih Lin, Ming-Chih Lin, Mei-Jy Jeng, Hung-Yang Chang, Liang-Ti Huang, Yi-Yu Su, Shau-Ru Ho, Yan-Yan Ng, Kai-Ti Tseng, Yi-Yin Chen, Tsung-Yu Wu, Wei-Tse Chiu, Li-Jung Fang, Kao-Hsian Hsieh
From Thai Newborn Registry Network: Anavat Bupphachareonsuk, Anchalee Limrungsikul, Anita Luvira, Anucha Thatrimontrichai, Buranee Swatesutipun, Buranee Yangthara, Chayatat Ruangkit, Cholticha Laohajeeraphan, Hathitip Chaiprapa, Junya Jirapradittha, Kanmalee Jenjarat, Kannikar Booranavanich, Namtip Intub, Narongsak Nakwan, Patcharin Thanomsingh, Pirarat Kotcharit, Piyawan Phummaphuti, Pornpimon Janyoungsak, Prapaiporn Chongkongkiat, Rapeephun Hansuebsai, Roongrawee Torbunsupachai, Santi Punnahitanan, Shanika Kosarat, Sommon Jindakul, Sopida Tanthawat, Sudarat Sirichaipornsak, Sudatip Kositamongkol, Supamas Supabanpot, Suparat Tipprasert, Tanin Pirunnet, Thanatda Siriporn, Usakorn Taesiri, Vasita Jirasakuldech
Correction notice: This article has been corrected since it was published Online First. The collborator name (Eleanor DR Cuarte) was misspelled.
Contributor Information
Tetsuya Isayama, Email: isayama-t@ncchd.go.jp.
Fuyu Miyake, Email: fmiyake1228@gmail.com.
Rinawati Rohsiswatmo, Email: rinarohsis@gmail.com.
Rizalya Dewi, Email: rizalya@yahoo.com.
Yuri Ozawa, Email: ozawa-y@ncchd.go.jp.
Seiichi Tomotaki, Email: stomotaki@kuhp.kyoto-u.ac.jp.
Naho Morisaki, Email: morisaki-n@ncchd.go.jp.
Seok Chiong Chee, Email: seokchiong@gmail.com.
Siew Hong Neoh, Email: neohsh2002@yahoo.com.
Ma Lourdes S Imperial, Email: pinkysi2@gmail.com.
Belen Amparo E Velasco, Email: drbelen.velasco@gmail.com.
Yun Sil Chang, Email: yunsil.chang@gmail.com.
Su Jin Cho, Email: sujin-cho@ewha.ac.kr.
YoungAh Youn, Email: lea732@hanmail.net.
Bin Huey Quek, Email: quek.bin.huey@singhealth.com.sg.
Woei Bing Poon, Email: poon.woei.bing@singhealth.com.sg.
Zubair Amin, Email: paeza@nus.edu.sg.
Kapila Jayaratne, Email: kapjay613@gmail.com.
Saman Kumara, Email: drsamankumara@yahoo.com.
Yuh-Jyh Lin, Email: yj.lin.nckuh@gmail.com.
Jui-Hsing Chang, Email: jhchang4519@gmail.com.
Hsiang Yu Lin, Email: hylin.neo@gmail.com.
Ming-Chih Lin, Email: mingclin@gmail.com.
Pracha Nuntnarumit, Email: pracha.nun@mahidol.ac.th.
Sopapan Ngerncham, Email: ngsopa@gmail.com.
Chatchay Prempunpong, Email: chatchaypr@gmail.com.
Pathaporn Prempraphan, Email: pathaporn@nmu.ac.th.
Sarayut Supapannachart, Email: sarayut.sup@mahidol.ac.th.
Satoshi Kusuda, Email: kusuda-satoshi@nrnj.org.
References
- 1.UN General Assembly Transforming our world: the 2030 agenda for sustainable development, A/RES/70/1. 2015. https://www.refworld.org/docid/57b6e3e44.html Available.
- 2.United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) New York: United Nations Children’s Fund; 2019. Levels & trends in child mortality: report 2019, estimates developed by the United Nations inter-agency group for child mortality estimation. [Google Scholar]
- 3.Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform Post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–40. doi: 10.1016/S0140-6736(14)61698-6. [DOI] [PubMed] [Google Scholar]
- 4.Horbar JD. The Vermont Oxford network: evidence-based quality improvement for neonatology. Pediatrics. 1999;103:350–9. [PubMed] [Google Scholar]
- 5.Kusuda S, Fujimura M, Uchiyama A, et al. Trends in morbidity and mortality among very-low-birth-weight infants from 2003 to 2008 in Japan. Pediatr Res. 2012;72:531–8. doi: 10.1038/pr.2012.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lee SK, McMillan DD, Ohlsson A, et al. Variations in practice and outcomes in the Canadian NICU network: 1996-1997. Pediatrics. 2000;106:1070–9. doi: 10.1542/peds.106.5.1070. [DOI] [PubMed] [Google Scholar]
- 7.Lee SK, Shah PS, Singhal N, et al. Association of a quality improvement program with neonatal outcomes in extremely preterm infants: a prospective cohort study. CMAJ. 2014;186:E485–94. doi: 10.1503/cmaj.140399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Edwards EM, Ehret DEY, Soll RF, et al. Vermont Oxford network: a worldwide learning community. Transl Pediatr. 2019;8:182–92. doi: 10.21037/tp.2019.07.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Isayama T, Lee SK, Mori R, et al. Comparison of mortality and morbidity of very low birth weight infants between Canada and Japan. Pediatrics. 2012;130:e957–65. doi: 10.1542/peds.2012-0336. [DOI] [PubMed] [Google Scholar]
- 10.Isayama T, Mirea L, Mori R, et al. Patent Ductus Arteriosus management and outcomes in Japan and Canada: comparison of Proactive and selective approaches. Am J Perinatol. 2015;32:1087–94. doi: 10.1055/s-0035-1548727. [DOI] [PubMed] [Google Scholar]
- 11.Shah PS, Lui K, Sjörs G, et al. Neonatal outcomes of very low birth weight and very preterm neonates: an international comparison. J Pediatr. 2016;177:144–52. doi: 10.1016/j.jpeds.2016.04.083. [DOI] [PubMed] [Google Scholar]
- 12.Helenius K, Sjörs G, Shah PS, et al. Survival in very preterm infants: an international comparison of 10 national neonatal networks. Pediatrics. 2017;140:e20171264. doi: 10.1542/peds.2017-1264. [DOI] [PubMed] [Google Scholar]
- 13.Stevenson AG, Tooke L, Edwards EM, et al. The use of data in resource limited settings to improve quality of care. Semin Fetal Neonatal Med. 2021;26:101204. doi: 10.1016/j.siny.2021.101204. [DOI] [PubMed] [Google Scholar]
- 14.Simkiss DE. Kangaroo mother care. J Trop Pediatr. 1999;45:192–4. doi: 10.1093/tropej/45.4.192. [DOI] [PubMed] [Google Scholar]
- 15.Hoddinott P, Tappin D, Wright C. Breast feeding. BMJ. 2008;336:881–7. doi: 10.1136/bmj.39521.566296.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Neves PAR, Vaz JS, Maia FS, et al. Rates and time trends in the consumption of breastmilk, formula, and animal milk by children younger than 2 years from 2000 to 2019: analysis of 113 countries. Lancet Child Adolesc Health. 2021;5:619–30. doi: 10.1016/S2352-4642(21)00163-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Asian neonatal network collaboration (AsianNeo) https://asian-neo.org/index.html n.d. Available.
- 18.Surveymonkey. Momentive Inc., CA, USA. https://www.surveymonkey.com n.d. Available.
- 19.Papile LA, Burstein J, Burstein R, et al. Incidence and evolution of Subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 GM. J Pediatr. 1978;92:529–34. doi: 10.1016/s0022-3476(78)80282-0. [DOI] [PubMed] [Google Scholar]
- 20.Shennan AT, Dunn MS, Ohlsson A, et al. Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics. 1988;82:527–32. [PubMed] [Google Scholar]
- 21.R Core Team . Vienna, Austria: R Foundation for Statistical Computing; 2023. R: A language and environment for statistical computing.https://www.R-project.org Available. [Google Scholar]
- 22.Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)--A metadata-driven methodology and workflow process for providing translational research Informatics support. J Biomed Inform. 2009;42:377–81. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi: 10.1016/j.jbi.2019.103208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patel RM, Kandefer S, Walsh MC, et al. Causes and timing of death in extremely premature infants from 2000 through 2011. N Engl J Med. 2015;372:331–40. doi: 10.1056/NEJMoa1403489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schindler T, Koller-Smith L, Lui K, et al. Causes of death in very preterm infants cared for in neonatal intensive care units: a population-based retrospective cohort study. BMC Pediatr. 2017;17:59. doi: 10.1186/s12887-017-0810-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Goldenberg RL, Muhe L, Saleem S, et al. Criteria for assigning cause of death for stillbirths and neonatal deaths in research studies in low-middle income countries. J Matern Fetal Neonatal Med. 2019;32:1915–23. doi: 10.1080/14767058.2017.1419177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lee SK, Beltempo M, McMillan DD, et al. Outcomes and care practices for preterm infants born at less than 33 weeks' gestation: a quality-improvement study. CMAJ. 2020;192:E81–91. doi: 10.1503/cmaj.190940. [DOI] [PMC free article] [PubMed] [Google Scholar]