

Abstract
Background
Despite restoration of epicardial blood flow in acute ST-elevation myocardial infarction (STEMI), inadequate microcirculatory perfusion is common and portends a poor prognosis. Intracoronary (IC) thrombolytic therapy can reduce microvascular thrombotic burden; however, contemporary studies have produced conflicting outcomes.
Objectives
This meta-analysis aims to evaluate the efficacy and safety of adjunctive IC thrombolytic therapy at the time of primary percutaneous coronary intervention (PCI) among patients with STEMI.
Methods
Comprehensive literature search of six electronic databases identified relevant randomised controlled trials. The primary outcome was major adverse cardiac events (MACE). The pooled risk ratio (RR) and weighted mean difference (WMD) with a 95% CI were calculated.
Results
12 studies with 1915 patients were included. IC thrombolysis was associated with a significantly lower incidence of MACE (RR=0.65, 95% CI 0.51 to 0.82, I2=0%, p<0.0004) and improved left ventricular ejection fraction (WMD=1.87; 95% CI 1.07 to 2.67; I2=25%; p<0.0001). Subgroup analysis demonstrated a significant reduction in MACE for trials using non-fibrin (RR=0.39, 95% CI 0.20 to 0.78, I2=0%, p=0.007) and moderately fibrin-specific thrombolytic agents (RR=0.62, 95% CI 0.47 to 0.83, I2=0%, p=0.001). No significant reduction was observed in studies using highly fibrin-specific thrombolytic agents (RR=1.10, 95% CI 0.62 to 1.96, I2=0%, p=0.75). Furthermore, there were no significant differences in mortality (RR=0.91; 95% CI 0.48 to 1.71; I2=0%; p=0.77) or bleeding events (major bleeding, RR=1.24; 95% CI 0.47 to 3.28; I2=0%; p=0.67; minor bleeding, RR=1.47; 95% CI 0.90 to 2.40; I2=0%; p=0.12).
Conclusion
Adjunctive IC thrombolysis at the time of primary PCI in patients with STEMI improves clinical and myocardial perfusion parameters without an increased rate of bleeding. Further research is needed to optimise the selection of thrombolytic agents and treatment protocols.
Keywords: Acute Coronary Syndrome, Myocardial Infarction, Meta-Analysis, Atherosclerosis
WHAT IS ALREADY KNOWN ON THIS TOPIC
ST-elevation myocardial infarction (STEMI) is a significant cause of morbidity and mortality worldwide. Microvascular obstruction affects about half of patients with STEMI, leading to adverse outcomes. Previous studies on adjunctive intracoronary thrombolysis have shown inconsistent results.
WHAT THIS STUDY ADDS
This meta-analysis demonstrates that adjunctive intracoronary thrombolysis during primary percutaneous coronary intervention (PCI) significantly reduces major adverse cardiac events and improves left ventricular ejection fraction. Furthermore, it significantly improves myocardial perfusion parameters without increasing bleeding risk.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Adjunctive intracoronary thrombolysis in patients with STEMI undergoing primary PCI shows promise for clinical benefit. Future studies should identify high-risk patients for microcirculatory dysfunction to optimise treatment strategies and clinical outcomes.
Introduction
Ischaemic heart disease remains a leading cause of morbidity and mortality worldwide.1 2 ST-elevation myocardial infarction (STEMI) occurs due to coronary vessel occlusion causing transmural myocardial ischaemia and subsequent necrosis.3 The cornerstone of contemporary management involves prompt reopening of the occluded coronary artery with percutaneous coronary intervention (PCI).4 5 Despite restoring epicardial blood flow, roughly 50% of patients fail to achieve adequate microvascular perfusion.6 This phenomenon, known as microvascular obstruction (MVO), is predictive of a poor cardiac prognosis driven by left ventricular remodelling and larger infarct size.7–9
In patients with STEMI, MVO is characterised by distal embolisation of atherothrombotic debris and fibrin-rich microvascular thrombi.10 A growing body of evidence supports the efficacy of adjunctive low-dose intracoronary (IC) thrombolysis in this population. Sezer et al performed the first randomised controlled trial (RCT), demonstrating an improvement in myocardial perfusion with low-dose IC streptokinase post-PCI.11 Subsequent studies focused on newer fibrin-specific agents with a lower propensity for systemic bleeding.12 Despite encouraging results, many studies were inadequately powered and yielded conflicting outcomes. This meta-analysis aims to evaluate the efficacy and safety of adjunctive IC thrombolytic therapy at the time of primary PCI in patients with STEMI.
Methods
The present study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.13
Search strategy and study selection
Electronic searches were performed using PubMed, Ovid Medline, Cochrane Library, ProQuest, ACP Journal Club and Google Scholar from their dates of inception to January 2022. The search terms “STEMI” AND “intracoronary” AND (“thrombolysis” OR “tenecteplase” OR “alteplase” OR “prourokinase” OR “urokinase” OR “streptokinase”) were combined as both keywords and Medical Subject Headings terms, with filters for RCTs. This was supplemented by hand searching the bibliographies of review articles and all potentially relevant studies.
Two reviewers (RR and SV) independently screened the title and abstracts of articles identified in the search. Full-text publications were subsequently reviewed separately if either reviewer considered the manuscript as being potentially eligible. Any disagreements regarding final study inclusion were resolved by discussion and consensus with a third reviewer (CCYW).
Eligibility criteria
Studies were included if they met following inclusion criteria: (1) RCT, (2) STEMI population, (3) IC thrombolysis given to treatment group with comparison with a control group (CG) receiving no thrombolytic therapy, (4) major adverse cardiovascular event (MACE) was an outcome reported.
All publications were limited to those involving human subjects and no restrictions were based on language. Reviews, meta-analyses, abstracts, case reports, conference presentations, editorials and expert opinions were excluded. When institutions published duplicate studies with accumulating numbers of patients or increased lengths of follow-up, only the most complete reports were included for assessment.
Data extraction and quality assessment
Two investigators (RR and SV) independently extracted data from text, tables and figures. Any discrepancies were resolved by discussion and consensus with a third reviewer (CCYW). For each of the included trials, the following data were extracted: publication year, number of patients, baseline characteristics of participants, treatment details (including specific agents administered), follow-up duration and endpoints.
Study quality and risk of bias were critically appraised using the updated Cochrane Collaboration Risk-of-Bias Tool V.2.14 Five domains of bias were evaluated: (1) randomisation process, (2) deviations from study protocol, (3) missing outcome data, (4) outcome measurement and (5) selective reporting of results.
Outcomes
The predetermined primary endpoint was MACE, which represented a composite outcome as defined by each individual study. While the individual components of MACE were generally consistent across studies, minor discrepancies existed (online supplemental table 1). Secondary outcomes included clinical endpoints (mortality, heart failure (HF), major and minor bleeding), myocardial perfusion endpoints (thrombolysis in myocardial infarction (TIMI) flow grade 3, TIMI myocardial perfusion grade (TMPG), corrected TIMI frame count (CTFC), ST-resolution (STR)) and echocardiographic parameters (left ventricular ejection fraction (LVEF)). Subgroup analysis for MACE was conducted based on fibrin specificity of the thrombolytic agent. This classification comprised non-fibrin-specific agents (streptokinase and urokinase), moderately fibrin-specific agents (prourokinase) and highly fibrin-specific agents (alteplase and tenectaplase). Clinical outcomes were assessed at the end of the follow-up period, which ranged from 1 to 12 months, while echocardiographic parameters were evaluated within a time frame of 1–6 months.
heartjnl-2024-324078supp001.pdf (1MB, pdf)
Statistical analysis
The mean difference (MD) or relative risk (RR) was used as summary statistics and reported with 95% CIs. Meta-analyses were performed using random-effects models to take into account the anticipated clinical and methodological diversity between studies. The I2 statistic was used to estimate the percentage of total variation across studies due to heterogeneity rather than chance, with values exceeding 50% indicative of considerable heterogeneity. For meta-analysis of continuous data, values presented as median and IQR were converted to mean and SD using the quantile method previously described by Wan et al.15 For subgroup analyses, a standard test of heterogeneity was used to assess for significant difference between subgroups with p<0.05 considered statistically significant.
Meta-regression analyses were performed to explore potential heterogeneity with the following moderator variables individually assessed for significance: publication year, mean age, proportion of male participants, percentage of left anterior descending artery infarcts, proportion of smokers, as well as baseline prevalence of diabetes, hypertension and dyslipidaemia.
Publication bias was assessed for the primary endpoint of MACE using funnel plots comparing log of point estimates with their SE. Egger’s linear regression method and Begg’s rank correlation test were used to detect funnel plot asymmetry.16 17 Statistical analysis was conducted with Review Manager V.5.3.5 (Cochrane Collaboration, Oxford, UK) and Comprehensive Meta-Analysis V.3.0 (Biostat, Englewood, New Jersey, USA). All p values were two sided, and values <0.05 were considered statistically significant.
Results
A total of 245 unique records were identified through electronic searches using six online databases, from which 85 duplicates were removed. Of these, 120 were excluded based on title and abstract alone. After screening the full text of the remaining 40 articles, 12 studies18–29 were found to meet the inclusion criteria, as summarised on the PRISMA flow chart in figure 1.
Figure 1.
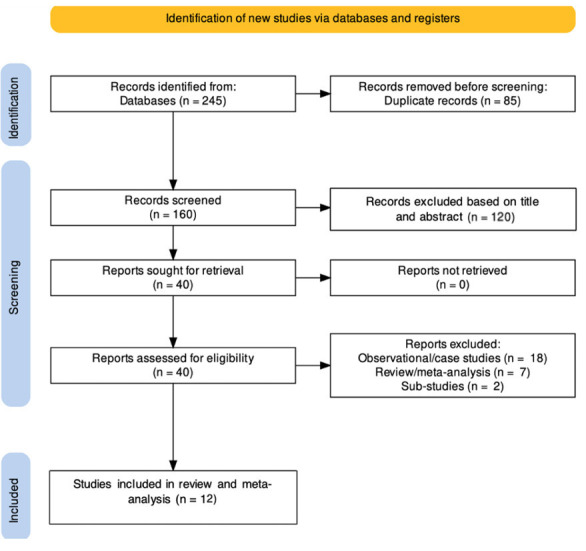
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart of literature search and study selection.
IC thrombolysis was examined in 12 studies (n=1030 received IC thrombolysis and 885 no IC thrombolysis). Included studies used non-fibrin-specific (streptokinase, urokinase), moderately fibrin-specific (prourokinase) and highly fibrin-specific thrombolytic (alteplase, tenecteplase) agents. The timing and delivery of IC thrombolytic therapy varied between studies. A complete summary of study characteristics and baseline participant characteristics is presented in tables 1 and 2, respectively. Primary and secondary outcomes are summarised in online supplemental table 2. According to the revised Cochrane tool, the overall risk of bias assessment for procedural measures was judged to be ‘low risk’ in two studies, ‘some concerns’ in eight studies and ‘high risk’ in two studies (online supplemental figure 1).
Table 1.
Summary of studies investigating intracoronary thrombolysis for patients with STEMI
| Study | Year | No of patients (N) | Treatment arms | Route of delivery | Timing of delivery | P2Y12 inhibitor | GPIIb/IIIa inhibitor (%) | Unfractionated heparin | Thrombus aspiration (%) | Follow-up |
| Sezer et al 25 | 2009 | 95 |
|
Guide catheter | Post-stent | Clopidogrel |
|
100 U/kg | NR | 6 months |
| Zhao et al 18 | 2015 | 183 |
|
Micro-catheter | Post-thrombus aspiration, pre-stent | Clopidogrel | NR | 8000–9000 U (additional 1000 U every 1 hour as required) | NR | 30 days |
| Greco et al 29 | 2013 | 102 |
|
Micro-catheter | Pre-stent | Clopidogrel | NR | 100 U/kg | NR | 6 months |
| Geng et al 20 | 2018 | 230 |
|
Punctured balloon catheter | Post-balloon, pre-stent | Ticagrelor | NR | 3000 U+70 U/kg for PCI | NR | 6 months |
| Xiao et al 28 | 2019 | 71 |
|
Micro-catheter | Post-balloon, pre-stent | Ticagrelor |
|
50–70 U/kg |
|
12 months |
| Fu et al 19 | 2019 | 39 |
|
Micro-catheter, child-in-mother catheter or pierced balloon | Pre-stent | Clopidogrel/ticagrelor | NR | NR |
|
90 days |
| McCartney et al 24 | 2019 | 440 |
|
Aspiration catheter or guide catheter if selectively engaged | Post-balloon, pre-stent | Clopidogrel/ticagrelor/prasugrel |
|
10 000 U |
|
3 months |
| Gibson et al 21 | 2020 | 36 |
|
Balloon catheter | 1st dose: pre-balloon; 2nd dose: post-stent | Clopidogrel |
|
70 U/kg | NR | 30 days |
| Wang et al 26 | 2020 | 182 |
|
Aspiration catheter | Post-thrombus aspiration, pre-stent | Ticagrelor |
|
3000 U (additional dosage by ACT) |
|
6 months |
| Wu et al 27 | 2020 | 50 |
|
Aspiration catheter | Post-thrombus aspiration, pre-stent | Ticagrelor |
|
5000 U (additional dosage guided by ACT) |
|
3 months |
| Huang et al 22 | 2021 | 345 |
|
Intracoronary catheter | Post-balloon or thrombus aspiration; pre-stent | Clopidogrel/ticagrelor |
|
70–100 U/kg |
|
30 days |
| Jiang et al 23 | 2021 | 260 |
|
Balloon catheter | Post-balloon, pre-stent | Ticagrelor | NR | 100 U/kg |
|
6 months |
ACT, activated clotting time; GPIIb/IIIa, glycoprotein IIb/IIIa; NR, not reported; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
Table 2.
Summary of baseline patient characteristics in studies investigating intracoronary thrombolysis for patients with STEMI
| Study | Group | Age (years) | Male N (%) |
Diabetes N (%) |
Hypertension N (%) |
Smokers N (%) |
Dyslipidaemia N (%) |
LAD-related infarct N (%) |
| Sezer et al 25 | TG | 52.5±8.9 | 45 (88) | 4 (8) | 17 (33) | 38 (74) | 18 (35) | 28 (55) |
| CG | 57.8±11.3 | 38 (84) | 10 (23) | 16 (36) | 27 (61) | 20 (45) | 28 (63) | |
| Zhao et al 18 | TG | 58.4±13.4 | 67 (74) | 28 (31) | 41 (45) | 35 (39) | 69 (76) | 57 (63) |
| CG | 58.7±14.5 | 70 (76) | 33 (36) | 45 (49) | 33 (36) | 63 (69) | 56 (61) | |
| Greco et al 29 | TG | 61±15 | 38 (75) | 8 (16) | 24 (47) | 30 (59) | 22 (43) | 29 (57) |
| CG | 59±12 | 34 (67) | 9 (18) | 28 (55) | 32 (63) | 25 (49) | 26 (51) | |
| Geng et al 20 | TG | 53.5±11.4 | 77 (65) | 26 (22) | 84 (71) | 50 (42) | 44 (37) | 60 (51) |
| CG | 55.2±10.4 | 70 (63) | 22 (20) | 69 (62) | 58 (52) | 47 (42) | 55 (49) | |
| Xiao et al 28 | TG | 64.9±13 | 28 (76) | 15 (39) | 20 (53) | 21 (55) | 17 (44) | 15 (39) |
| CG | 62.2±15.8 | 27 (83) | 11 (33) | 24 (73) | 17 (52) | 16 (48) | 19 (58) | |
| Fu et al 19 | TG | 62.6±11.1 | 16 (80) | 4 (20) | 11 (55) | 13 (65) | 9 (45) | NR |
| CG | 63.2±11.2 | 15 (79) | 5 (26) | 10 (53) | 9 (47) | 9 (47) | NR | |
| McCartney et al 24 | CG: | 60.7±11 | 127 (84) | 19 (13) | 47 (31) | 75 (50) | 42 (28) | 61 (45) |
| TG (alt 10 mg) | 59.6±10.3 | 124 (86) | 19 (13.2) | 45 (31) | 72 (50) | 28 (19) | 61 (47) | |
| TG (alt 20 mg) | 61.2±9.7 | 123 (85) | 18 (12) | 49 (34) | 62 (43) | 32 (22) | 60 (46) | |
| Gibson et al 21 | TG | 57 | 15 (75) | 2 (10) | 13(65) | 11 (55) | 10 (50) | 5 (25) |
| CG | 59 | 13 (81) | 3 (19) | 6 (38) | 12 (75) | 6 (38) | 4 (25) | |
| Wang et al 26 | TG | 61.1±11 | 76(83) | 20(22) | 54(59) | 51(55) | 19(21) | 51(55) |
| CG | 58.8±11 | 73(81) | 22(24) | 46(51) | 55(61) | 14(16) | 42(47) | |
| Wu et al 27 | TG | 59.5±14 | 21 (81) | 8 (32) | 17 (47) | 12 (48) | 8 (30) | 8 (32) |
| CG | 61±13 | 22 (88) | 6 (24) | 19 (53) | 13 (52) | 5 (20) | 10 (40) | |
| Huang et al 22 | TG | 59.4±10.1 | 100 (90) | 21 (19) | 52 (47) | 67 (60) | 71 (64) | 60 (54) |
| CG | 58.5±9.9 | 105 (90) | 21 (18) | 58 (50) | 75 (64) | 89 (76) | 54 (46) | |
| Jiang et al 23 | TG | 53.9±6.6 | 96 (77) | 40 (32) | 77 (62) | 86 (69) | 49 (39) | 82 (66) |
| CG | 55.1±6.8 | 119 (88) | 47 (35) | 93 (69) | 104 (77) | 59 (44) | 93 (69) |
Alt, alteplase; CG, control group; LAD, left anterior descending; STEMI, ST-elevation myocardial infarction; TG, thrombolysis group.
Clinical outcomes
All 12 RCTs reported the incidence of MACE. Compared with the CG, IC thrombolysis treatment significantly improved the occurrence of MACE at the end of follow-up (RR=0.65, 95% CI 0.51 to 0.82, I2=0%, p<0.0004; figure 2). Subgroup analysis demonstrated a significant reduction in MACE for trials using non-fibrin (RR=0.39, 95% CI 0.20 to 0.78, I2=0%, p=0.007) and moderately fibrin-specific thrombolysis (RR=0.62, 95% CI 0.47 to 0.83, I2=0%, p=0.001). MACE was observed at a similar rate in studies using highly fibrin-specific thrombolysis (RR=1.10, 95% CI 0.62 to 1.96, I2=0%, p=0.75). Test for subgroup difference was not significant (p=0.07). Furthermore, IC thrombolysis was associated with an improvement of LVEF (weighted MD (WMD)=1.87; 95% CI, 1.07 to 2.67; I2=25%; p<0.0001; online supplemental figure 2). There was a trend towards lower incidence of HF hospitalisation (RR=0.66; 95% CI 0.42 to 1.05; I2=0%; p=0.08; online supplemental figure 3), though not statistically significant. No significant differences were observed in mortality (RR=0.95; 95% CI 0.50 to 1.81; I2=0%; p=0.88; online supplemental figure 4), major bleeding (RR=1.24; 95% CI 0.47 to 3.28; I2=0%; p=0.67; online supplemental figure 5) and minor bleeding events (RR=1.47; 95% CI 0.90 to 2.40; I2=0%; p=0.12; online supplemental figure 6) between the two groups.
Figure 2.

Forest plot displaying relative risk for major adverse cardiovascular events with intracoronary (IC) thrombolysis (stratified by fibrin-specific and non-fibrin-specific agents) or placebo in ST-elevation myocardial infarction. Squares and diamonds=risk ratios. Lines=95% CIs.
Myocardial perfusion outcomes
In patients with STEMI, IC thrombolysis significantly improved TIMI flow grade 3 (RR=1.09; 95% CI 1.02 to 1.15; I2=63%; p=0.006), TMPG (RR=1.38; 95% CI 1.13 to 1.68; I2=54%; p=0.001), complete STR (RR=1.20; 95% CI 1.10 to 1.31; I2=51%; p<0.0001) and CTFC (WMD=−4.58; 95% CI −6.23 to –2.72; I2=41%; p<0.0001) when compared with the CG (figure 3).
Figure 3.

Forest plots of myocardial perfusion outcomes with intracoronary (IC) thrombolysis or placebo in ST-elevation myocardial infarction. (A) Thrombolysis in myocardial infarction (TIMI) flow grade 3. (B) TIMI myocardial perfusion grade 3. (C) ST-segment resolution. (D) Corrected TIMI frame count. Squares and diamonds=risk ratios/weighted mean difference. Lines=95% CIs.
Meta-regression results
For primary endpoint of MACE, meta-regression analyses did not identify the following moderator variables as significant effect modifiers: publication year (p=0.97), proportion of male (p=0.23), prevalence of diabetes (p=0.44), proportion of smokers (p=0.68), prevalence of dyslipidaemia (p=0.44) and prevalence of hypertension (p=0.21).
Publication bias
Both Egger’s linear regression method (p=0.73) and Begg’s rank correlation test (p=0.63) suggested that publication bias was not an influencing factor when MACE was selected as the primary endpoint.
Discussion
The present meta-analysis examined 12 RCTs that included 1915 patients with STEMI undergoing primary PCI. All trials evaluated the efficacy and safety of IC thrombolytic agents compared with a CG. The main findings were that patients administered IC thrombolysis had: (1) significantly lower incidence of MACE, (2) improvement in LVEF and (3) superior myocardial perfusion parameters (TIMI flow grade 3, TMPG, CTFC and complete STR). Notably, there were no significant differences observed in mortality and bleeding events in both groups.
Mortality rates following STEMI remain high, with 30-day mortality rates ranging from 5.4% to 14% and 1-year mortality rates ranging from 6.6% to 17.5%.30 Despite the increased availability of primary PCI facilities and advancements in reperfusion strategies, there has been limited improvement in STEMI mortality rates.31 Moreover, complications such as HF, arrhythmia, repeat revascularisation and reinfarction continue to be prevalent.32–34 Despite restoring epicardial blood flow through PCI, MVO is evident in almost half of patients with STEMI.6 It is characterised by distal embolisation of atherothrombotic debris, de novo microvascular thrombosis formation and plugging of circulating blood cells.35 Furthermore, the upregulation of inflammatory mediators leads to intramyocardial haemorrhage and further microvascular necrosis.36 37 These mechanistic pathways contribute to a larger infarct size, adverse myocardial remodelling and worse prognosis.7 8 38
Thrombolytic therapy is an effective treatment for acute coronary thrombosis.39 It inhibits red blood cell aggregation and dissolves thrombi to facilitate adequate microvascular perfusion.40 41 Thrombolytic agents are commonly classified based on their affinity for fibrin. Streptokinase and urokinase lack fibrin specificity, indiscriminately activating both circulating and clot-bound plasminogen. Prourokinase has moderate fibrin specificity with a propensity for activation on fibrin surfaces, although systemic fibrinogen degradation has been observed. Alteplase and tenectaplase are highly fibrin specific, activating fibrin-bound plasminogen with minimal impact on circulating free plasminogen.
Utilisation of a facilitated PCI strategy with adjunctive intravenous thrombolysis improves coronary flow acutely,42 however, causes paradoxical activation of thrombin, leading to increased bleeding.43 44 As a result, clinicians considered the administration of IC thrombolytic therapy. Encouraging results from an open-chest animal model45 led to the first randomised trial using adjunctive IC streptokinase in 41 patients with STEMI undergoing primary PCI.11 In the IC streptokinase group, patients demonstrated improved coronary flow reserve, index of microcirculatory resistance (IMR) and CTFC 2 days after primary PCI.11 Further RCTs with moderately fibrin-specific thrombolytic agents (prourokinase) demonstrated similar results with improved myocardial perfusion parameters.19 20 22 23 26–28 Notably, the T-TIME Study, a large RCT of 440 patients comparing a highly fibrin-specific thrombolytic agent (alteplase) against placebo, reported different outcomes. At 3-month follow-up, there were no significant differences in rates of death or HF hospitalisation between groups. In addition, microvascular obstruction (% left ventricular mass) on cardiac magnetic resonance (CMR) between groups at 2–7 days did not differ. The ICE T-TIMI trial, which also used a highly fibrin-specific thrombolytic agent (tenecteplase), investigated its efficacy in 40 patients. This small study administered two fixed doses of 4 mg of IC tenecteplase and evaluated the primary endpoint of culprit lesion per cent diameter stenosis after the first bolus of tenecteplase or placebo. The results indicated no significant difference in the primary endpoint between the two groups.
In an initial meta-analysis of six RCTs investigating the use of IC thrombolysis in patients with STEMI compared with placebo, findings revealed a reduction in MVO but no impact on MACE.46 Subsequent analyses, including studies with larger sample sizes or focusing on specific thrombolytic agents, have since been conducted with varied results.47 48 Our meta-analysis, which is the largest to date, demonstrates that adjunctive IC thrombolysis in patients with STEMI improves both clinical and microcirculation outcomes. Although bleeding events did not significantly increase, it is plausible that a tradeoff may exist for reducing MACE. Notably, subgroup analysis for MACE demonstrated no significant benefit for highly fibrin-specific agents (figure 2).
Intuitively, fibrin-specific thrombolytics are presumed to offer inherent advantages over their less fibrin-specific counterparts. In vivo studies have revealed that administration of alteplase in patients with STEMI induced shorter periods of thrombin and kallikrein activation, less reduction in fibrinogen, and a decrease in D-dimer and plasmin–antiplasmin complexes compared with streptokinase.49 In this regard, tenecteplase demonstrates superior performance relative to alteplase with almost no paradoxical procoagulant effect due to reduced activation of thrombin and the kallikrein–factor XII system.50
Nonetheless, other variables may diminish the significance of fibrin specificity. It has been argued that administration of IC alteplase, a short-acting thrombolytic with a half-life of 4–6 min, before flow optimisation with stenting may have contributed to the negative results seen in T-TIME. Although prourokinase has a similarly short half-life and was also given before stenting in multiple studies, it was associated with better results.19 20 22 23 26–28 The therapeutic efficacy of prourokinase predominantly relies on its conversion to urokinase, a non-fibrin-specific direct plasminogen activator, potentially resulting in a prolonged duration of action. Furthermore, inducing a systemic fibrinolytic state with a non-selective agent may be paradoxically desirable in patients receiving adjunctive IC thrombolytics during primary PCI. This approach can potentially prevent further thrombus reaccumulation and embolisation to the microcirculation, especially in a highly thrombogenic environment. In contrast, fibrin-specific agents may heighten the risk of rethrombosis and reocclusion due to their limited impact on systemic fibrinogen depletion. Nevertheless, such varied outcomes across these studies could be attributed to the heterogeneous methodologies used.
Despite encouraging results, future studies targeting patients at the highest risk of MVO with appropriately powered sample sizes are required. The ongoing RESTORE-MI (Restoring Microcirculatory Perfusion in STEMI) trial (NCT03998319) has a unique approach in which all study participants will undergo assessment of microvascular integrity after primary PCI prior to inclusion. Only patients with objective evidence of microvascular dysfunction (IMR value >32) following reperfusion will be randomised to treatment with IC tenecteplase or placebo. The primary endpoint measured will be cardiovascular mortality and rehospitalisation for HF at 24 months, in addition to infarct size on CMR at 6 months post-PCI. This study may potentially support a novel therapeutic approach towards treating MVO in patients with STEMI in the future.
Limitations
Several key limitations should be considered when interpreting the findings of the present meta-analysis. First, several studies were subject to bias due to issues in randomisation and blinding, leading to an increased chance of type 1 (false-positive) error. In addition, the sample size of individual studies, except for the T-TIME trial, was relatively small. Second, inconsistencies in the duration of follow-up and the definition of clinical outcomes, such as MACE, were observed among the studies. Third, interventional protocols varied between RCTs. For example, IC thrombolytic therapy differed in agent, dosage, timing and route of administration. Initial studies used non-fibrin-specific agents, while contemporary studies moved towards newer fibrin-specific therapy. Besides Sezer et al,25 all other studies administered IC thrombolysis therapy prior to stent implantation.18–24 26–29 Within the latter group, some delivered before flow restoration,19 21 29 though most did so after balloon dilation or thrombus aspiration.18 20 22–24 26–28 Similarly, the methods of IC administration of the agents varied between non-selective delivery through guiding catheters24 25 to selective delivery via IC catheters.18–24 26–29 Furthermore, antiplatelet, anticoagulant and glycoprotein IIb/IIIa inhibitors (GPI) regimens also differed (table 1). Finally, patient selection was diverse between studies. Though regression analysis did not detect any significant effect modifiers, total ischaemic time was omitted due to significant heterogeneity in reporting.
Conclusion
Impaired myocardial perfusion remains a clinical challenge in patients with STEMI. Despite its limitations, this meta-analysis favours the use of IC thrombolytic therapy during primary PCI. Overall, IC thrombolysis reduced the incidence of MACE and improved myocardial perfusion markers without increasing the risk of bleeding. Future clinical trials should be appropriately powered for clinical outcomes and focus on patients at high risk of microcirculatory dysfunction.
Footnotes
@RajanRehan23
Contributors: RR—conceptualisation, methodology, data analysis, writing (original draft preparation), reviewing and editing the final manuscript. SV—methodology, data analysis. CCYW—conceptualisation, methodology, data analysis. FP—supervision, writing (reviewing and editing). JL—supervision, writing (reviewing and editing). AK—supervision, writing (reviewing and editing). AY—conceptualisation, methodology, writing (reviewing and editing). HDW—conceptualisation, methodology, writing (reviewing and editing). WF—conceptualisation, methodology, writing (reviewing and editing). MN—conceptualisation, methodology, supervision, writing (reviewing and editing), guarantor.
Funding: This study is funded by the National Health and Medical Research Council (2022150).
Competing interests: JL has received minor honoraria from Abbott Vascular, Boehringer Ingelheim and Bayer. AY has received minor honoraria and research support from Abbot Vascular and Philips Healthcare. WF has received research support from Abbott Vascular and Medtronic; and has minor stock options with HeartFlow. MN has received research support from Abbot Vascular. HDW has received grant support paid to the institution and fees for serving on Steering Committees of the ODYSSEY trial from Sanofi and Regeneron Pharmaceuticals, the ISCHEMIA and MINT Study from the National Institutes of Health, the STRENGTH trial from Omthera Pharmaceuticals, the HEART-FID Study from American Regent, the DAL-GENE Study from DalCor Pharma UK, the AEGIS-II Study from CSL Behring, the CLEAR OUTCOMES Study from Esperion Therapeutics, and the SOLIST-WHF and SCOREDS trials from Sanofi Aventis Australia. The remaining authors have nothing to disclose.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
Not applicable.
References
- 1. Roth GA, Abate D, Abate KH. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet 2018;392:1736–88. 10.1016/S0140-6736(18)32203-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Kyu HH, Abate D, Abate KH. Global, regional, and national disability-adjusted life-years (Dalys) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet 2018;392:1859–922. 10.1016/S0140-6736(18)32335-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Maseri A, Chierchia S, Davies G. Pathophysiology of coronary occlusion in acute infarction. Circulation 1986;73:233–9. 10.1161/01.cir.73.2.233 [DOI] [PubMed] [Google Scholar]
- 4. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: executive summary: a report of the American college of cardiology/American heart association joint committee on clinical Practice guidelines. Circulation 2022;145:e4–17. 10.1161/CIR.0000000000001039 [DOI] [PubMed] [Google Scholar]
- 5. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2017;39:119–77. 10.1093/eurheartj/ehx393 [DOI] [PubMed] [Google Scholar]
- 6. Sorajja P, Gersh BJ, Costantini C, et al. Combined Prognostic utility of ST-segment recovery and myocardial blush after primary percutaneous coronary intervention in acute myocardial infarction. Eur Heart J 2005;26:667–74. 10.1093/eurheartj/ehi167 [DOI] [PubMed] [Google Scholar]
- 7. van de Hoef TP, Bax M, Meuwissen M, et al. Impact of coronary Microvascular function on long-term cardiac mortality in patients with acute ST-segment-elevation myocardial infarction. Circ Cardiovasc Interv 2013;6:207–15. 10.1161/CIRCINTERVENTIONS.112.000168 [DOI] [PubMed] [Google Scholar]
- 8. Regenfus M, Schlundt C, Krähner R, et al. Six-year Prognostic value of Microvascular obstruction after Reperfused ST-elevation myocardial infarction as assessed by contrast-enhanced cardiovascular magnetic resonance. Am J Cardiol 2015;116:1022–7. 10.1016/j.amjcard.2015.06.034 [DOI] [PubMed] [Google Scholar]
- 9. Fearon WF, Shah M, Ng M, et al. Predictive value of the index of Microcirculatory resistance in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol 2008;51:560–5. 10.1016/j.jacc.2007.08.062 [DOI] [PubMed] [Google Scholar]
- 10. Lerman A, Holmes DR, Herrmann J, et al. Microcirculatory dysfunction in ST-elevation myocardial infarction: cause, consequence, or both European Heart Journal 2007;28:788–97. 10.1093/eurheartj/ehl501 [DOI] [PubMed] [Google Scholar]
- 11. Sezer M, Oflaz H, Gören T, et al. Intracoronary Streptokinase after primary percutaneous coronary intervention. N Engl J Med 2007;356:1823–34. 10.1056/NEJMoa054374 [DOI] [PubMed] [Google Scholar]
- 12. Collen D. Fibrin-selective thrombolytic therapy for acute myocardial infarction. Circulation 1996;93:857–65. 10.1161/01.CIR.93.5.857 [DOI] [PubMed] [Google Scholar]
- 13. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009;151:264. 10.7326/0003-4819-151-4-200908180-00135 [DOI] [PubMed] [Google Scholar]
- 14. Sterne JAC, Savović J, Page MJ, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898. 10.1136/bmj.l4898 [DOI] [PubMed] [Google Scholar]
- 15. Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or Interquartile range. BMC Med Res Methodol 2014;14:135. 10.1186/1471-2288-14-135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088–101. 10.2307/2533446 [DOI] [PubMed] [Google Scholar]
- 17. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34. 10.1136/bmj.315.7109.629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Zhao B, Liu L, Liu Y. Effects of intracoronary low-dose urokinase injection combined with stent implantation in acute STEMI patients on myocardial perfusion and its influence on short-term prognosis. Med J Chin PLA 2015;40:661–5. 10.11855/j.issn.0577-7402.2015.08.12 [DOI] [Google Scholar]
- 19. Fu Y, Gu XS, Hao GZ, et al. Comparison of myocardial Microcirculatory perfusion after catheter-administered intracoronary Thrombolysis with Anisodamine versus standard thrombus aspiration in patients with ST-elevation myocardial infarction. Catheter Cardiovasc Interv 2019;93:839–45. 10.1002/ccd.28112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Geng W, Zhang Q, Liu J, et al. A randomized study of prourokinase during primary percutaneous coronary intervention in acute ST-segment elevation myocardial infarction. J Interv Cardiol 2018;31:136–43. 10.1111/joic.12461 [DOI] [PubMed] [Google Scholar]
- 21. Gibson CM, Kumar V, Gopalakrishnan L, et al. Feasibility and safety of low-dose intra-coronary tenecteplase during primary percutaneous coronary intervention for ST-elevation myocardial infarction (ICE T-TIMI 49). Am J Cardiol 2020;125:485–90. 10.1016/j.amjcard.2019.11.018 [DOI] [PubMed] [Google Scholar]
- 22. Huang D, Qian J, Liu Z, et al. Effects of intracoronary pro-Urokinase or Tirofiban on coronary flow during primary percutaneous coronary intervention for acute myocardial infarction: A multi-center, placebo-controlled, single-blind, randomized clinical trial. Front Cardiovasc Med 2021;8:710994. 10.3389/fcvm.2021.710994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Jiang W, Xiong X, Du X, et al. Safety and efficacy study of Prourokinase injection during primary percutaneous coronary intervention in acute ST-segment elevation myocardial infarction. Coron Artery Dis 2021;32:25–30. 10.1097/MCA.0000000000000898 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. McCartney PJ, Eteiba H, Maznyczka AM, et al. Effect of low-dose intracoronary Alteplase during primary percutaneous coronary intervention on Microvascular obstruction in patients with acute myocardial infarction: A randomized clinical trial. JAMA 2019;321:56. 10.1001/jama.2018.19802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Sezer M, Cimen A, Aslanger E, et al. Effect of intracoronary Streptokinase administered immediately after primary percutaneous coronary intervention on long-term left ventricular infarct size, volumes, and function. J Am Coll Cardiol 2009;54:1065–71. 10.1016/j.jacc.2009.04.083 [DOI] [PubMed] [Google Scholar]
- 26. Wang X, Liu H, Wu H, et al. Safety and efficacy of intracoronary prourokinase administration in patients with high thrombus burden. Coron Artery Dis 2020;31:493–9. 10.1097/MCA.0000000000000853 [DOI] [PubMed] [Google Scholar]
- 27. Wu Y, Fu X, Feng Q, et al. Efficacy and safety of intracoronary prourokinase during percutaneous coronary intervention in treating ST-segment elevation myocardial infarction patients: a randomized, controlled study. BMC Cardiovasc Disord 2020;20:308. 10.1186/s12872-020-01584-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Xiao Y, Fu X, Wang Y, et al. Effects of different strategies on high thrombus burden in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary catheterization. Coron Artery Dis 2019;30:555–63. 10.1097/MCA.0000000000000743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Greco C, Pelliccia F, Tanzilli G, et al. Usefulness of local delivery of thrombolytics before thrombectomy in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention (the delivery of thrombolytics before thrombectomy in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention [DISSOLUTION] randomized trial. Am J Cardiol 2013;112:630–5. 10.1016/j.amjcard.2013.04.036 [DOI] [PubMed] [Google Scholar]
- 30. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke Statistics-2016 update: a report from the American heart Association. Circulation 2016;133:e38–360. 10.1161/CIR.0000000000000350 [DOI] [PubMed] [Google Scholar]
- 31. Yeh RW, Sidney S, Chandra M, et al. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med 2010;362:2155–65. 10.1056/NEJMoa0908610 [DOI] [PubMed] [Google Scholar]
- 32. Jenča D, Melenovský V, Stehlik J, et al. Heart failure after myocardial infarction: incidence and predictors. ESC Heart Fail 2021;8:222–37. 10.1002/ehf2.13144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Windecker S, Bax JJ, Myat A, et al. Future treatment strategies in ST-segment elevation myocardial infarction. Lancet 2013;382:644–57. 10.1016/S0140-6736(13)61452-X [DOI] [PubMed] [Google Scholar]
- 34. Bajaj A, Sethi A, Rathor P, et al. Acute complications of myocardial infarction in the current era: diagnosis and management. J Investig Med 2015;63:844–55. 10.1097/JIM.0000000000000232 [DOI] [PubMed] [Google Scholar]
- 35. Konijnenberg LSF, Damman P, Duncker DJ, et al. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc Res 2020;116:787–805. 10.1093/cvr/cvz301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Betgem RP, de Waard GA, Nijveldt R, et al. Intramyocardial haemorrhage after acute myocardial infarction. Nat Rev Cardiol 2015;12:156–67. 10.1038/nrcardio.2014.188 [DOI] [PubMed] [Google Scholar]
- 37. Yellon DM, Hausenloy DJ. Myocardial reperfusion injury. N Engl J Med 2007;357:1121–35. 10.1056/NEJMra071667 [DOI] [PubMed] [Google Scholar]
- 38. Ganame J, Messalli G, Dymarkowski S, et al. Impact of myocardial haemorrhage on left ventricular function and remodelling in patients with Reperfused acute myocardial infarction. Eur Heart J 2009;30:1440–9. 10.1093/eurheartj/ehp093 [DOI] [PubMed] [Google Scholar]
- 39. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second international study of infarct survival) collaborative group. Lancet 1988;2:349–60. 10.1016/S0140-6736(88)92833-4 [DOI] [PubMed] [Google Scholar]
- 40. Schwartz RS, Burke A, Farb A, et al. Microemboli and Microvascular obstruction in acute coronary thrombosis and sudden coronary death: relation to epicardial plaque Histopathology. J Am Coll Cardiol 2009;54:2167–73. 10.1016/j.jacc.2009.07.042 [DOI] [PubMed] [Google Scholar]
- 41. Zalewski J, Undas A, Godlewski J, et al. No-reflow phenomenon after acute myocardial infarction is associated with reduced clot permeability and susceptibility to lysis. Arterioscler Thromb Vasc Biol 2007;27:2258–65. 10.1161/ATVBAHA.107.149633 [DOI] [PubMed] [Google Scholar]
- 42. Hillis WS, Jones CR, Been M, et al. Intracoronary thrombolytic therapy performed within a coronary care unit: one year’s experience. Scott Med J 1986;31:25–9. 10.1177/003693308603100106 [DOI] [PubMed] [Google Scholar]
- 43. Primary versus Tenecteplase-facilitated percutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction (ASSENT-4 PCI): randomised trial. The Lancet 2006;367:569–78. 10.1016/S0140-6736(06)68147-6 [DOI] [PubMed] [Google Scholar]
- 44. Ellis SG, Tendera M, de Belder MA, et al. Facilitated PCI in patients with ST-elevation myocardial infarction. N Engl J Med 2008;358:2205–17. 10.1056/NEJMoa0706816 [DOI] [PubMed] [Google Scholar]
- 45. Woo KS, Armiger LC, White HD, et al. Can Streptokinase produce beneficial effects additional to coronary Recanalization? quantitative Microvascular analysis of critically injured Reperfused myocardium. Microvasc Res 2000;60:8–20. 10.1006/mvre.2000.2236 [DOI] [PubMed] [Google Scholar]
- 46. Alyamani M, Campbell S, Navarese E, et al. Safety and efficacy of intracoronary Thrombolysis as Adjunctive therapy to primary PCI in STEMI: A systematic review and meta-analysis. Can J Cardiol 2021;37:339–46. 10.1016/j.cjca.2020.03.034 [DOI] [PubMed] [Google Scholar]
- 47. Chen L, Shi L, Tian W, et al. Intracoronary Thrombolysis in patients with ST-segment elevation myocardial infarction: A meta-analysis of randomized controlled trials. Angiology 2021;72:679–86. 10.1177/0003319721995039 [DOI] [PubMed] [Google Scholar]
- 48. Yin XS, Huang YW, Li ZP, et al. Efficacy and safety of intracoronary pro-Urokinase injection during percutaneous coronary intervention in treating ST elevation myocardial infarction patients: a systematic review and meta-analysis of randomized controlled trials. Eur Rev Med Pharmacol Sci 2022;26:5802–13. 10.26355/eurrev_202208_29518 [DOI] [PubMed] [Google Scholar]
- 49. Hoffmeister HM, Szabo S, Kastner C, et al. Thrombolytic therapy in acute myocardial infarction: comparison of Procoagulant effects of Streptokinase and Alteplase regimens with focus on the Kallikrein system and Plasmin. Circulation 1998;98:2527–33. 10.1161/01.cir.98.23.2527 [DOI] [PubMed] [Google Scholar]
- 50. Szabo S, Letsch R, Ehlers R, et al. Absence of paradoxical thrombin activation by fibrin-specific Thrombolytics in acute myocardial infarction: comparison of single-bolus Tenecteplase and front-loaded Alteplase. Thromb Res 2002;106:113–9. 10.1016/s0049-3848(02)00084-1 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
heartjnl-2024-324078supp001.pdf (1MB, pdf)
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplemental information.