

Abstract
Introduction
Ventriculoperitoneal shunt insertion (VPSI) and endoscopic third ventriculostomy (ETV) are the major procedures for treating pediatric hydrocephalus. However, studies comparing motor development following the two treatments are limited.
Objective
We aimed to determine motor development outcomes in children with hydrocephalus up to 2 years of age after undergoing VPSI or ETV, to identify which surgical approach yields better motor outcomes and may be more effective for Malawian children.
Methods
This was a cross-sectional study where we recruited two groups of participants: one group consisted of children with hydrocephalus treated with VP shunt whilst the other group were treated with ETV, at least 6 months prior to this study. Participants were identified from the hospital records and were called to come for neurodevelopmental assessment using the Malawi Development Assessment Tool (MDAT).
Results
A total 152 children treated for hydrocephalus within an 18-month period met the inclusion criteria. Upon follow up and tracing, we recruited 25 children who had been treated: 12 had VPSI and 13 had ETV. MDAT revealed delays in both assessed motor domains: 19 out of the 25 children had delayed gross motor whilst 16 of 25 had delayed fine motor development. There was no significant difference between the shunted and the ETV groups.
Conclusion
Children with hydrocephalus demonstrate delays in motor development six to 18 months after treatment with either VPSI or ETV. This may necessitate early and prolonged intensive rehabilitation to restore motor function after surgery. Long-term follow-up studies with bigger sample sizes are required to detect the effect of the two treatment approaches.
Keywords: Hydrocephalus, Malawi, ventriculostomy, ventriculoperitoneal shunt, motor development, Malawi Development Assessment Tool
Introduction
Motor development is an important aspect of quality of life in children. During the first 6 months of life, infants tend to engage in exploratory and social play, all of which involve motor skills. Therefore, a child must master both gross motor skills (large muscle movements in the arms and legs, such as crawling, standing, and walking) and fine motor skills (small muscle movements in the hands and fingers, such as grasping, writing), which then leads to a cascade of cognitive, social, emotional and language development1. Delayed motor development therefore impairs a child's ability to explore the environment, leading to poor social skills and reduced independence in activities of daily living2. Any disease condition affecting the functioning of the neurons in the brain, whether congenital or acquired, infection or structural (brain tumors, hydrocephalus), impairs the development of the brain which in turn affects the motor abilities discussed above. One such condition is hydrocephalus, a relatively common neurological condition affecting children worldwide3,4. In hydrocephalus, there is progressive distension of the ventricles associated with an increase in intracranial pressure5. Through complex and multifactorial mechanisms, enlargement of the cerebral ventricles in hydrocephalus causes the gradual destruction of periventricular white matter axons, impairs neuronal maturation, and impairs cerebral vasculature2,6,7. This results in compromised early development of these structures which are central to motor function, thereby placing affected individuals at risk of abnormal motor development2,7. However, despite the evident motor deficits observed in children with hydrocephalus, there is a paucity of information regarding their motor development profile. This knowledge gap extends to understanding how their motor development profile differs from that of children with typical development, how it varies among different etiologies with varying time of onset, and the potential influence of treatment on their motor outcome2. Thus, a comprehensive understanding of these aspects is critical for improving clinical management and therapeutic interventions for children with hydrocephalus.
Unlike other conditions (prolonged acute global brain ischemia, severe infections like cerebral malaria and meningitis), acquired structural conditions like hydrocephalus (and brain tumor), develop gradually, and depending on how soon the condition is treated, the changes at the neuronal level may be reversed albeit not completely8. Primary treatment techniques for paediatric hydrocephalus include ventriculoperitoneal, (VPSI), ventriculo-atrial shunt insertion or, endoscopic third ventriculostomy (ETV), with or without choroid plexus cauterization (CPC)5,6. Many attempts have been made to compare the two treatment techniques but it is inconclusive as to which technique is superior in most outcomes9-14. With shunt insertion, accumulated CSF in the ventricles is drained to the peritoneal cavity or the right atrium of the heart, thereby reducing the volume of CSF within the ventricles of the brain. On the contrary, in ETV, there is no significant reduction in the volume of CSF within the ventricles, although there is appreciable changes in intracranial pressure and improvement in brain functionality9. Through the mechanisms of neuronal changes during hydrocephalus, and the excretory functions of CSF, the effects of continued presence of high volumes of CSF in the brain in patients treated with ETV are not fully known.
In recent years, it has been realized that the functional outcome is a more useful indicator of the effectiveness of hydrocephalus treatment10,15. This means that not only the symptoms of active hydrocephalus need to be resolved, but also ensuring optimal conditions for the regeneration of affected neural structures to ensure further development and optimal quality of life11,12. In our setting, the performance of the two treatment procedures has been evaluated only in terms of complications and mortality at one year of follow-up10. A research group at our institution also succeeded in demonstrating the usefulness of a local neurodevelopment assessment tool in evaluating the functional outcomes of children with hydrocephalus after treatment16. However, no comparisons of the functional outcomes, including motor development, in children treated with either of the two treatment procedures have been done. Therefore, we conducted this study to compare the motor development outcomes of a group of children with hydrocephalus treated with VPSI or ETV at Queen Elizabeth Central Hospital in Blantyre, Malawi, to determine which surgical procedure provides better outcomes in terms of motor development, and may therefore be the more effective for our children with hydrocephalus. Our results will also increase knowledge about the motor development profile of these children after treatment, which will aid therapists design appropriate rehabilitation programs.
Methods
Setting
The study was conducted at the department of neurosurgery, at Queen Elizabeth Central Hospital (QECH) in the southern city of Blantyre, Malawi, which serves as a tertiary referral hospital for patients with hydrocephalus in the region.
Participants
In this cross-sectional study, we recruited two groups of participants (1) the VPSI group (those who underwent shunting), and (2) the ETV group (those who underwent Endoscopic Third Ventriculostomy).
In order to recruit our participants, we used the patient flow in hydrocephalus care in our hospital. After undergoing surgical treatment, children are reviewed in the weekly outpatient clinic, 2 to 4 weeks later, depending on the patient's proximity to the clinic and their ability to travel to the clinic. Thereafter, patients are reviewed 6-8 weeks later, then after 3 months and then after every 6 months. In our study, we aimed to review children who were below 2 years of age and had had their hydrocephalus operation, at least 6 months prior to the date of assessment. According to the follow up plan in the clinic, and the low turn up for follow up in the patients, we reverted to contacting patients through mobile phone calls, and inviting them to come to the clinic for assessment. We used the Neurosurgery department's electronic medical records to get contact details of caregivers.
Children were included in the study if they met the following inclusion criteria: (1) a primary diagnosis of hydrocephalus, regardless of type (e.g., congenital, post-infectious), (2) the age range of 7-24 months and (3) treated with ETV or VPSI at least 6 to 18 months prior to the study (i.e. those treated for hydrocephalus between June 1, 2019, and December 31, 2020, were eligible). We excluded children who had the following: (1) presence of spina bifida/myelomeningocele, (2) undergoing repeat operations for hydrocephalus, such as subsequent surgeries following a failed ETV or shunt procedure (3) serious illness (such as malaria) that would make the child unfit to undergo a motor assessment as per the MDAT protocol.
Assessment, Scoring and Analysis
We collected background information from all consenting caregivers. This captured demographic, perinatal and clinical details of the child such as age, sex, mode of delivery, whether infant was born full term or premature, age of hydrocephalus diagnosis, type and date of surgery. We then proceeded with direct developmental assessments on the children using the Malawi Developmental Assessment Tool (MDAT). This is a norm-referenced standardized tool that was initially developed and validated in Malawi, and has been found to be specific and sensitive in assessing neurodevelopment in such settings17. It has also been piloted on children with hydrocephalus by one of the study groups at our hospital and it showed ability to detect developmental delay in high proportion of children with hydrocephalus hence recommended for use in larger trials and studies to understand effect of interventions16. It has now been used in over 25 countries and has been well validated to assess child development in Sub-Saharan Africa17. The MDAT is easy to administer and can be completed within 30 minutes.
The tool examines development in four domains: [1] gross motor, [2] fine motor, [3] language and [4] social. The gross motor, fine motor and language domains are assessed by directly observing the child while the social domain is assessed by directing questions to the caregiver. It is a 136-item tool with 34 items in each developmental domain. The assessor scores items as “pass” or “fail” and if the child is uncooperative or unwell the score is recorded as “don't know”17,18. During evaluation of each domain, the assessor employs floor and ceiling assessment methods. In this approach, the assessor ensures that the child can successfully complete up to seven consecutive items from their entry point before discontinuing assessment below the child's developmental age. Conversely, if the child fails seven consecutive items, no further assessment is done in that domain. This practice is a common technique in developmental screening tests as it prevents the examiner from needlessly prolonging the examination by administering tasks that are obviously below or above the child's developmental stage. Delay in any domain was defined as failure on three or more items from the entry point according to age.
Statistical analysis was performed using standard statistical software, Stata Version 16. Level of statistical significance was set at p< 0.05 (Fischer exact test). We set the confidence interval (CI) at 95%.
Ethics
The study was approved as undergraduate research by the College of Medicine Research Ethics Committee (COMREC) in Malawi with the certificate number - U.02/21/3255. Informed consent was obtained in written form from accompanying caregivers before the assessments were done. Additionally, the consent forms were translated into the local language, Chichewa, and verbally read to all caregivers. The MDAT is already available in the local language.
Results
Data collection was done in a period of 4 weeks (31st May to 25th June 2021). We found a total of 184 records of children with hydrocephalus aged 7 to 24 months in the electronic records system, who were treated for hydrocephalus from 1st June 2019 to 31st December 2020. Of these 184 children, 169 came from the southern region of Malawi which is the catchment area for our hospital, and these were considered for recruitment for the ease of mobility to our clinic. However, our records showed that 17 children from this group had undergone repeat operations for failed shunt or ETV, and were excluded from the study. Thus, 152 children were eligible for the study: 79 for VPSI and 73 having undergone ETV. Out of these 152 patients, 88 (58%) did not have any contacts recorded in the electronic records system. Of the remaining 64 with contacts, 19 phone numbers were unreachable. We therefore managed to contact 45 patients. Of these, 5 children were reported to have died, and 15 were not able to come for assessment even though we had promised to refund their transport money. As such, only 25 children were available for assessment: 12 with VPSI and 13 with ETVs and were successfully recruited into the study. These findings have been summarized in a flow chart in Figure 1.
Figure 1.
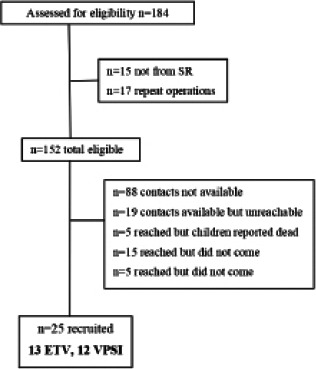
Flow chart of identification of study participants for neurodevelopmental assessment
Study findings
All the findings in the study have been summarized in Table 1. The mean age at the time of assessment was 15.5 months for the shunted group and 19.4 months for the ETV group.
About half the children (13/25) were male and most (80%) had normal birth weights. Most children (19 out of 25) were being followed up in the outpatient clinic. However, very few were attending physiotherapy sessions (9 out of 25). There were no statistically significant differences in the background characteristics, which included gender, birth history, post-operative infections and follow-up visits, and physiotherapy intervention after surgery, between the ETV and VPSI Upon assessment using MDAT, our results showed that the participants in both groups had delays in all 4 domains and there was no any statistical significance between the two groups with all p-values > 0.05: gross motor, fine motor, social and language. We also analysed for the effect of physiotherapy on motor outcomes by comparing those development in those who reported that they were attending physiotherapy sessions with those who were not attending. Only nine of the 25 participants said that their children were going for physiotherapy.
Discussion
In a group of children with hydrocephalus managed at a tertiary hospital in Malawi, we compared motor development outcomes between those that underwent ETV and those that underwent VPSI. The results did not show any significant difference between those that underwent ETV and those that underwent VPSI (p-value 0.645 for gross motor and 0.097 for fine motor). This is in accordance with findings of a Nigerian study which found no difference in milestone improvement between infants treated with ETV or VPSI over a 3-year period19. Also in support are findings of Kulkarni et al where there was no significant difference in health status and quality of life between infants treated with ETV and VPSI after 1 year follow up20. In contrast to these findings, however, various studies have reported significant difference between the two groups in various outcomes where those treated with ETV fared better than shunted group5,13,21. Several authors have argued that the high delay percentage in neuropsychological development associated with VPSI could be contributed by the selection bias in the surgical decision of shunt versus ETV22. Patient selection is based on the severity of brain damage whereby those with more severe brain damage are more likely to be shunted while those with less brain damage (intact cerebral cortex) have a higher chance of ETV being technically successful22. As such, adequate development can be achieved in infants treated with ETV although catch-up is slow20. Overall, the results could be this way because the advantages of ETV take several years to be realized5,9.
In our study, a small proportion (9/25) of the participants attended physiotherapy in the follow up period after surgery. However, the physiotherapy intervention did not seem to have any effect on neurological outcomes of this group as they still had severe delays in both gross and fine motor domains similar to those that did not attend (Table 1). This could be due to lack of adherence and consistency to therapy as most guardians reported of inaccessibility of rehabilitation services within their area. They only access rehabilitation services during their surgical reviews which happen once in 3-6 months at QECH. However, in order to enhance neural plasticity and motor and functional restoration, it is recommended that the rehabilitation program should incorporate intensive and repetitive exercises in a good environment without which the rehabilitation would not be effective23. The need for early and intensive therapy has also been confirmed by a case report done by Marcelo et al which looked at normal motor development in infants with congenital hydrocephalus where great improvement was seen after intensive therapy7. Therefore, it would be crucial to provide community-based rehabilitation specifically tailored to this group since currently, very few children with hydrocephalus receive physiotherapy on a scale that would make a difference, which makes it all the more important to prioritize such efforts and ensure that every child receives the rehabilitation they need. It is also worth noting that rehabilitation is a vital component of the process of gaining independence, and therefore, it should start as early as possible. During the first months of a child's life, their nervous system is most adaptable, making it the ideal time to begin the rehabilitation process. By improving the rehabilitation process, we can help improve outcomes and increase their chances of achieving independence.
Overall, the results of this study support previous findings that children with hydrocephalus have significant developmental delays which do not improve after 6 months of treatment with either VPSI or ETV. In the same vein, findings of a recent exploratory study conducted at the same tertiary hospital demonstrated severe developmental delay in a cohort of children with hydrocephalus16. This has been attributed to the severity of the initial brain injury caused by infection in hydrocephalus children13. However, severity of developmental delay varies depending on severity of the hydrocephalus and age of diagnosis and intervention; especially in Malawi where a good number of children will present late for treatment which influences the outcome. This therefore highlights the need for further research using groups of children with similar characteristics such as brain damage severity, age of diagnosis and treatment.
In a nutshell, one goal of evaluating motor development by type of surgical procedure was to provide information that may eventually be integrated into clinical decision-making for management of hydrocephalus in children. If, for example, children who were treated with ETV fared better than those treated with shunts, a decision would be to adopt use of ETV for most children with hydrocephalus. Or conversely, if those treated with shunts performed better, the opposite would be true. The lack of significance difference between the two groups in this study therefore necessitates the need for a larger study with a longer follow up period.
The study had several limitations. First, the small sample size which may have hindered the possibility of demonstrating significant difference in our findings. Second, the follow up period was too short to detect improvements, if any, in neurodevelopment. We also had a selection bias where only those close to Blantyre and accessible by phone were available for assessment.
Conclusion
The results of this study show that children treated for hydrocephalus have significant delays in neurodevelopment in first year of treatment. There is need for a prospective large-scale follow-up study on motor developmental outcomes in infants with hydrocephalus before and after ETV or VPSI. Future studies should compare ETV with VPSI in infants with similar degrees of brain injury, with minimal selection bias.
| Characteristics | ETV | VPSI | Total | p-value |
| No. of children (n) | 13 | 12 | 25 | |
| Mean age (months) ± SD | 19.38 ± 1.59 | 15.50± 1.79 | 0.0001 | |
| Gender | ||||
| Male (n) | 8 | 5 | 13 | 0.434 |
| Female (n) | 5 | 7 | 12 | |
| Birth weight | ||||
| Normal (n) | 11 | 9 | 19 | 0.645 |
| Underweight(n) | 2 | 3 | 6 | |
| Positive history of post-operative infection (n) | 3 | 1 | 4/25 | 0.593 |
| Positive compliance with postoperative follow-up visits (n) | 10 | 9 | 19/25 | 1.000 |
| Positive compliance with post-surgery physiotherapy (n) | 4 | 5 | 9/25 | 0.688 |
| Delays on MDAT assessment | ||||
| Gross motor (n) | ||||
| Proportion (CI) | 9/13 | 10/12 | 19/25 | 0.645 |
| 0.69 (0.39-0.91) | 0.83 (0.51-0.98) | 0.76 (0.59-0.91) | ||
| Fine Motor (n) | ||||
| Proportion (CI) | 6/13 | 10/12 | 16/25 | 0.097 |
| 0.46 (0.19-0.75) | 0.83 (0.51-0.98) | 0.64 (0.43-0.82) | ||
| Social (n) | ||||
| Proportion (CI) | 4/13 | 5/12 | 9/25 | 0.688 |
| 0.31 (0.9-0.61) | 0.41 (0.15-0.72) | 0.36 (0.18-0.57) | ||
| Language (n) | ||||
| Proportion (CI) | 2/13 | 3/12 | 5/25 | 0.645 |
| 0.15 (0.02-0.45) | 0.25 (0.05-0.57) | 0.20 (0.07-0.41) | ||
| The effect of physiotherapy sessions on motor development | ||||
| Physiotherapy compliant | Physiotherapy not compliant | Total | p-value | |
| Delayed motor development | ||||
| Gross motor (n) | ||||
| Proportion (CI) | 8/9 | 11/16 | 19/25 | 0.364 |
| 0.89 (0.52-1.0) | 0.69 (0.41-0.89) | 0.76 (0.59-0.91) | ||
| Fine motor (n) | 6/9 | 10/16 | 16/25 | 1.000 |
| Proportion (CI) | 0.67 (0.30-0.93) | 0.63 (0.35-0.85) | 0.64 (0.43-0.82) | |
Acknowledgements
We extend our gratitude to Annie Mika-Bonongwe for her invaluable support in facilitating the orientation and training sessions for the data collectors in the use of the Malawi Development Assessment Tool (MDAT).
References
- 1.Adolph KE, Hoch JE. The importance of motor skills for development. Building Future Health and Well-Being for Thriving Toddlers and Young Children [Internet] 2020. pp. 136–144. Available from: [DOI] [PubMed]
- 2.Hetherington R, Dennis M. Motor function profile in children with early onset hydrocephalus. Dev Neuropsychol. 2009;15(1):25–51. [Google Scholar]
- 3.Isaacs AM, Riva-cambrin J, Yavin D, Hockley A, Pringsheim TM, Jette N, et al. Age-specific global epidemiology of hydrocephalus : Systematic review, metanalysis and global birth surveillance. PLoS One [Internet] 2018;13(10):1–24. doi: 10.1371/journal.pone.0204926. Available from: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dewan MC, Rattani A, Mekary R, Glancz LJ, Yunusa I, Baticulon RE, et al. Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. 2019 April;130:1065–1079. doi: 10.3171/2017.10.JNS17439. [DOI] [PubMed] [Google Scholar]
- 5.Kamalo P. Point of view: Exit ventriculoperitoneal shunt; enter endoscopic third ventriculostomy (ETV): Contemporary views on hydrocephalus and their implications on management. Malawi Med J. 2013;25(3):78–82. [PMC free article] [PubMed] [Google Scholar]
- 6.Kahle KT, Kulkarni A V, Jr DDL, Warf BC. Hydrocephalus in children. Lancet [Internet] 2015;6736(15):1–12. doi: 10.1016/S0140-6736(15)60694-8. Available from: [DOI] [Google Scholar]
- 7.Ramires De Oliveira G, Fabris Vidal M. A normal motor development in congenital hydrocephalus after Cuevas Medek Exercises as early intervention : A case report. Clin Case Reports. 2020;00:1–4. doi: 10.1002/ccr3.2860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Del Bigio MR. Pathophysiologic Consequences of Hydrocephalus. J Neurosurg Clin North Am. 2001;12(4):639–649. [PubMed] [Google Scholar]
- 9.Takahashi Y. Long-term outcome and neurologic development after endoscopic third ventriculostomy versus shunting during infancy. Child's Nerv Syst. 2006;22:1591–1602. doi: 10.1007/s00381-006-0190-8. [DOI] [PubMed] [Google Scholar]
- 10.Chimaliro S, Hara C, Kamalo P. Mortality and complications 1 year after treatment of hydrocephalus with endoscopic third ventriculostomy and ventriculoperitoneal shunt in children at Queen Elizabeth Central Hospital, Malawi. Acta Neurochir. 2023;165(1):61–69. doi: 10.1007/s00701-022-05392-7. [DOI] [PubMed] [Google Scholar]
- 11.Kulkarni A V, Shams I, Cochrane DD, McNeedy DP. Quality of life after endscopic third ventriculostomy and cerebrospinal fluid shunting: an adjusted multivariable analysis in a large cohort. J Neurosurg Pediatr. 2010;6(1):11–16. doi: 10.3171/2010.3.PEDS09358. [DOI] [PubMed] [Google Scholar]
- 12.Larysz P, Larysz D, Mandera M. Radiological findings in relation to the neurodevelopmental outcome in hydrocephalic children treated with shunt insertion or endoscopic third ventriculostomy. Child's Nerv Syst. 2014;30:99–104. doi: 10.1007/s00381-013-2200-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kulkarni AV, Schiff SJ, Mbabazi-Kabachelor E, Mugamba J, Ssenyonga P, Donnelly R, et al. Endoscopic Treatment versus Shunting for Infant Hydrocephalus in Uganda. N Engl J Med. 2017;377(25):2456–2464. doi: 10.1056/NEJMoa1707568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kulkarni A V, Drake JM, Malluci CL, Sgouros S, Constantini S. Endoscopic third ventriculostomy vs cerebrospinal fluid shuntin the treatment of hydrocephalus in children: a propensity score-adjusted analysis. Neurosurgery. 2010;67(3):588–593. doi: 10.1227/01.NEU.0000373199.79462.21. [DOI] [PubMed] [Google Scholar]
- 15.Sobana M, Halim D, Aviani JK, Gamayani U, Achmad TH. Neurodevelopmental outcomes after ventriculoperitoneal shunt placement in children with non-infectious hydrocephalus: a meta-analysis. Child's Nerv Syst. 2021;37(4):1055–1065. doi: 10.1007/s00381-021-05051-9. [DOI] [PubMed] [Google Scholar]
- 16.Rush J, Pala A, Kapapa T, Wirtz CR, Mayer B, Micah-Bonongwe A, et al. Assessing neurodevelopmental outcome in children with hydrocephalus in Malawi. A pilot study. Clin Neurol Neurosurg. 2022 December;212:6–10. doi: 10.1016/j.clineuro.2021.107091. 2021. [DOI] [PubMed] [Google Scholar]
- 17.Gladstone M, Lancaster GA, Umar E, Nyirenda M, Kayira E, Van NR. The Malawi Developmental Assessment Tool (MDAT): The Creation, Validation, and Reliability of a Tool to Assess Child Development in Rural The Malawi Developmental Assessment Tool(MDAT): The Creation, Validation, and Reliability of a Tool to Asses. PLos Med. 7(5) doi: 10.1371/journal.pmed.1000273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Den Heuvel V, Reijneveld S, Chidzalo K, Voskuijl W, Bandsma R, Gladstone M. Developmental and behavioual problems in children with severe acute malnutrition in Malawi: A cross-sectional study. J Glob Health. 2017;7(2) doi: 10.7189/jogh.07.020416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Uche OE, Okorie C, Illoabachie I, Amuta DS, Uche NJ. Endoscopic third ventriculostomy (ETV) and ventriculoperitoneal shunt (VPS) in non-communicating hydrocephalus (NCH): comparison outcome profiles in Nigerian children. Child's Nerv Syst. 2018;34(9):1683–1689. doi: 10.1007/s00381-018-3848-0. [DOI] [PubMed] [Google Scholar]
- 20.Kulkarni A V, Sgouros S, Leitner Y, Constantini S. International Infant Hydrocephalus Study (IIHS): 5-year health outcome results f a prospective, multicenter comparison of endoscopic third ventriculostomy (ETV) and for infant hydrocephalus. Child's Nerv Syst. 2018;34:2391–2397. doi: 10.1007/s00381-018-3896-5. [DOI] [PubMed] [Google Scholar]
- 21.Reid T, Grudziak J, Rodriguez-ormaza N, Maine RG, Msiska N, Quinsey C, et al. Complications and 3-month outcomes of children with hydrocephalus treated with ventriculoperitoneal shunts in Malawi. J Neurosurg Pediatr. 2019 August;24:120–127. doi: 10.3171/2019.2.PEDS18325. [DOI] [PubMed] [Google Scholar]
- 22.Kulkarni A V, Drake JM, Kestle JRW, Malluci CL, Sgouros S, Constantini S. Endoscopic Third Ventriclustomy Vs Cerebrospinal Fluid Shunt in the Treatment of Hydrocephalus in Children : A Propensity Score - Adjusted Analysis. Neurosurgery. 2010;67(3):588–593. doi: 10.1227/01.NEU.0000373199.79462.21. [DOI] [PubMed] [Google Scholar]
- 23.Takeuchi N, Izumi S. Rehabilitation with Poststroke Motor Recovery : A Review with a Focus on Neural Plasticity. Stroke ResTreat. 2013;2013:128641. doi: 10.1155/2013/128641. [DOI] [PMC free article] [PubMed] [Google Scholar]