

Abstract
Background and purpose
Electric scooters (e-scooters) have become increasingly popular as a mode of transportation in recent years. The impact of e-scooter accidents on the healthcare system and resulting orthopaedic injuries remains largely unknown. This study describes the distribution of fractures caused by e-scooter accidents.
Methods
All patients who had one or more fractures from e-scooter accidents registered in the Swedish Fracture Register (SFR) between 7 April 2019 and 30 December 2022 were included. Fractures were classified using the AO Foundation/Orthopaedic Trauma Association (AO/OTA) fracture classification system. We analysed the distribution of fractures, the proportion that required surgical management and seasonal variation of injuries.
Results
During the study period, 1,874 fractures in 1,716 patients were registered in the SFR. The mean age of patients was 29 (SD 14) years and 70% of fractures occurred in males. High-energy accidents accounted for 299 fractures (16%). The most common fractures were of the hand (n = 363, 19%), wrist (n = 352, 19%) and proximal forearm (n = 356, 19%). Wrist fractures were the most common injury in children (n = 183), accounting for 44% of paediatric fractures. Surgical treatment was performed on 556 (30%) fractures, with wrist fractures being the most commonly treated in both adults (n = 78, 17%) and children (n = 36, 36%).
Interpretation
Fractures caused by e-scooter accidents predominantly occur in the upper extremity. E-scooter accidents comprise a new source of injury requiring attention and surgical resources from an already strained healthcare system.
Keywords: E-scooter, Fractures, Trauma, Fracture distribution, Swedish fracture register, Transportation
Introduction
Background
In recent years the popularity of electric scooters (e-scooters) has dramatically increased, providing a convenient alternative for short-distance travel. However, along with their growing popularity, there has been a noticeable increase in orthopaedic injuries. These injuries encompass a wide range of musculoskeletal trauma, most commonly affecting young males and resulting in upper extremity fractures [1–3]. This new type of transport injury have been shown to significantly affect health care costs [4].
E-scooter-related injuries can be caused by several factors. There is an inherent risk of riding a two-wheeled vehicle with disproportionately small wheels and a short wheelbase. Rider inexperience, lack of protective gear and intoxication could further increase the risk of sustaining a fracture, along with environmental factors and traffic conditions.
In order to reduce the number of accidents and develop effective prevention strategies, it is important for health-care professionals, policymakers and the general public to gain further knowledge regarding the nature of e-scooter related injuries.
Objective
This study aimed to explore types of fracture, age and sex distribution in individuals who sustained fractures from e-scooter accidents. A further aim was to study the proportion of surgically treated patients and the seasonal variation in e-scooter accidents.
Patients and methods
Study design and setting
This observational study was based on data from the Swedish Fracture Register (SFR), which contains data on injury mechanism, fracture classification and treatment (surgical and non-surgical) of Swedish citizens with a fracture sustained in Sweden [5]. The injury mechanism is registered by the treating orthopaedic surgeon. Since the introduction of e-scooters, this mode of transportation has been added as a subtype to the registration of bicycle accidents. Fractures are classified according to the AO/OTA classification (2007 version) [6]. Several studies have investigated the accuracy of the SFR classification and found it reliable [7–9]. The coverage of the SFR has gradually increased from one active department in 2011 to 75% coverage in 2016 and full national coverage in 2021 (54 of 54 orthopaedic departments).
A comparison with the National Patient Register (NPR) in 2022 demonstrated a completeness of the SFR of approximately 60% for all fractures and 81% for femoral fractures. These figures are conservative as the NPR overestimates the number of fractures, mostly due to miscoding old fractures as new at follow-up visits [10].
Patients and outcome variables
All patients with fractures acquired in an e-scooter accident registered in the SFR between 7 April 2019 and 30 December 2022 were included in the study. Data collected included demographics (age and sex), injury date, fracture classification and location, presence of open fracture and primary treatment (non-surgical or surgical). Patients ≥ 18 years old at injury were classified as adults and patients < 18 years as children. Fracture classification was used to group fractures into the following body part locations: clavicle, scapula, humerus, forearm (including distal radius), hand, spine, pelvis, femur, patella, tibia, ankle and foot. Sub-analyses included segment location of long bones: proximal, diaphyseal and distal parts. The primary outcome investigated was the distribution of fractures, expressed as percentage for the respective body part in relation to all fractures. Furthermore, the proportion of surgically-treated fractures and seasonal variation were investigated.
Ethics, funding, data presentation and potential conflicts of interest
The study was conducted according to the Helsinki Declaration and approval was obtained from the Swedish Ethical Review Authority (Dnr 2022-04355-01). No individual patient consent was needed according to the Swedish Patient Law. The dataset analysed in this study is not freely available because of legislation on register data and restrictions stipulated in the ethical permission only to report aggregated data. Data can be obtained from the Center of Registers, Västra Götaland if ethical approval is granted. The STROBE recommendations for reporting observational studies were applied [11].
The authors declare no competing interests related to this body of work.
Statistics
Baseline demographic data are presented as the number of patients and fractures, means with standard deviation (SD) and proportions (%). All statistical analyses were performed using R version 4.2.2 [12].
Results
Some 1,874 fractures in 1,716 patients involved in e-scooter accidents were registered in the SFR and included in the study. The mean age was 29 years and 70% of patients were male. Some 415 fractures (22%) occurred in children. Most were closed fractures (n = 1,842, 98%) (Table 1).
Table 1.
Characteristics of the study population
| Patients | 1716 |
| Fractures | 1874 |
| Mean age (SD) | 29 (14) |
| Sex | |
| Males | 1194 (70%) |
| Females | 522 (30%) |
| Adult fractures | 1459 (78%) |
| Paediatric fractures (< 18 years) | 415 (22%) |
| Paediatric population’s mean age (SD) | 13 years (3) |
| Open fractures | 32 (2%) |
Fracture distribution
The upper extremity was the most prevalent injury site, accounting for 1,459 (78%) fractures. The most frequently injured part of the upper extremity was the forearm (n = 757, 40%), followed by the hand (n = 363, 20%) (Fig. 1; Table 2).
Fig. 1.
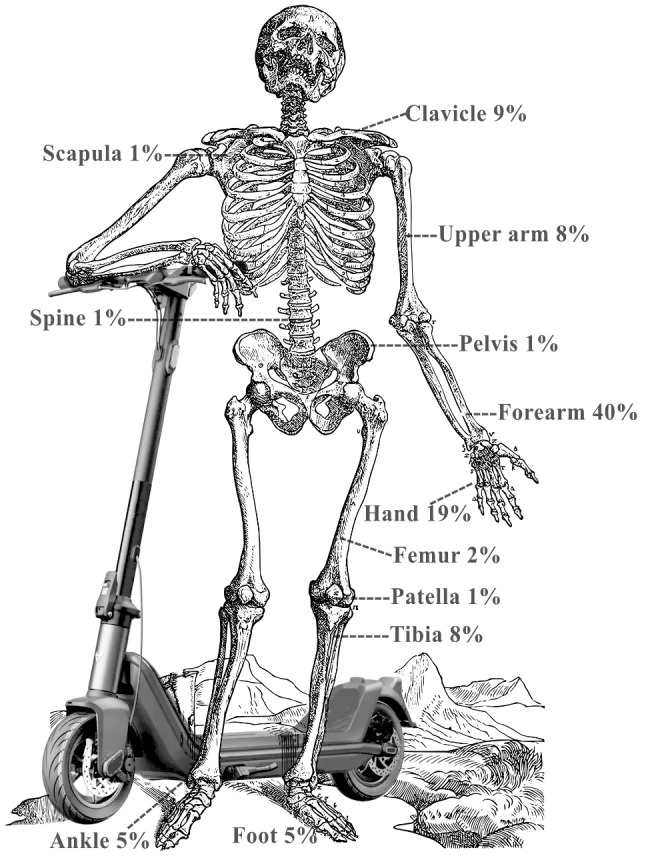
Distribution
Table 2.
Distribution of fractures in e-scooter accidents overall and separately for adults and children, number of fractures (% of group)
| Region | Adults (n = 1459) | Children (n = 415) | Overall (n = 1874) | |
|---|---|---|---|---|
| Clavicle | 150 (10.3%) | 27 (6.5%) | 177 (9.4%) | |
| Scapula | 21 (1.4%) | 0 | 21 (1.1%) | |
| Upper arm | 113 (7.7%) | 28 (6.7%) | 141 (7.5%) | |
| Forearm | 513 (35.2%) | 244 (58.8%) | 757 (40.4%) | |
| Hand | 319 (21.9%) | 44 (10.6%) | 363 (19.4%) | |
| Spine | 7 (0.5%) | 2 (0.5%) | 9 (0.5%) | |
| Pelvis | 13 (0.9%) | 2 (0.5%) | 15 (0.8%) | |
| Femur | 31 (2.1%) | 6 (1.4%) | 37 (2.0%) | |
| Patella | 17 (1.2%) | 0 | 17 (0.9%) | |
| Tibia | 102 (7.0%) | 44 (10.6%) | 146 (7.8%) | |
| Ankle | 90 (6.2%) | 7 (1.7%) | 97 (5.2%) | |
| Foot | 83 (5.7%) | 11 (2.7%) | 94 (5.0%) |
When adults and children were considered separately, the forearm remained the most frequently injured site, with 513 (35% of all adult fractures) adult fractures and 244 (59% of all paediatric fractures) paediatric fractures.
Surgically treated fractures
Some 556 fractures (30%) were treated surgically. Fractures of the forearm were the leading cause of surgical treatment (n = 216 or 39%), with distal radius fractures accounting for most cases (n = 114, 21%). This pattern remained when adult (n = 455) and paediatric fractures (n = 101) were analysed separately, with distal radius fractures being the most frequent injury necessitating surgical treatment in adults (n = 78, 17%) and children (n = 36, 36%) (Table 3).
Table 3.
Distribution of fractures treated surgically following e-scooter accidents, long bone fractures presented as proximal, diaphyseal and distal segment fractures. Data are presented overall and separately for adults and children (number (% of surgically treated fractures in respective group)),
| Region | Adults (n = 455) | Children (n = 101) | Overall (n = 556) | |
|---|---|---|---|---|
| Clavicle | 27 (5.9%) | 5 (5.0%) | 32 (5.8%) | |
| Scapula | 2 (0.4%) | 0 | 2 (0.4%) | |
|
Humerus Proximal Diaphyseal Distal |
37 (8.1%) 28 (6.2%) 1 (0.2%) 8 (1.8%) |
5 (5.0%) 2 (2.0%) 0 3 (3.0%) |
42 (7.5%) 30 (5.4%) 1 (0.2%) 11 (2.0%) |
|
|
Forearm Proximal Diaphyseal Distal radius |
162 (35.6%) 62 (13.6%) 22 (4.8%) 78 (17.1%) |
54 (53.4%) 2 (2.0%) 16 (15.8%) 36 (35.6%) |
216 (38.8%) 64 (11.5%) 38 (6.8%) 114 (20.5%) |
|
| Hand | 50 (11.0%) | 6 (5.9%) | 56 (10.1%) | |
| Spine | 0 | 0 | 0 | |
| Pelvis | 1 (0.2%) | 0 | 1 (0.2%) | |
|
Femur Proximal Diaphyseal Distal |
30 (6.6%) 24 (5.3%) 3 (0.7%) 3 (0.7%) |
4 (4.0%) 2 (2.0%) 1 (1.0%) 1 (1.0%) |
34 (6.1%) 26 (4.7%) 4 (0.7%) 4 (0.7%) |
|
| Patella | 5 (1.1%) | 0 | 5 (0.9%) | |
|
Tibia Proximal Diaphyseal Distal |
70 (15.4%) 50 15 5 |
21 (20.7%) 3 (2.9%) 6 (5.9%) 12 (11.9%) |
91 (16.4%) 53 (9.5%) 21 (3.8%) 17 (3.1%) |
|
| Ankle | 57 (12.5%) | 6 (5.9%) | 63 (11.3%) | |
| Foot | 14 (3.1%) | 0 | 14 (2.5%) |
Seasonal and weekly variation of injuries
Our analysis of monthly variation indicates a prominent spike in e-scooter-related fractures during the summer months, with July having the highest number of accidents (Fig. 2).
Fig. 2.

Months
Regarding weekly variation, Saturdays had the highest occurrence of e-scooter-related fractures, contributing to the overall higher injury rate on weekends (Fig. 3).
Fig. 3.

Days
Discussion
During the study period, e-scooter accidents resulted in 1,874 registered fractures. The majority of these fractures occurred in the upper extremity, particularly the forearm.
This pattern did not change when adults and children were analysed separately. Most patients in our study were younger males (mean age 29 years). These findings are in line with those reported by a recent systematic review of 34 studies examining injuries after e-scooter accidents [13]. The mean age of the participants in that review was 33 years and 58% (vs. 70% in our study) were males. The most common type of injury was bony injuries in which upper extremity fractures dominated. Unlike our study, that review encompassed studies investigating non-orthopaedic injuries such as head injuries, lacerations and contusions.
James et al. estimated a mortality rate of 9% in road traffic accidents with e-scooters, highlighting that injuries caused by e-scooters transcend orthopaedic diagnoses [14].
Other studies focusing on orthopaedic injuries corroborate our findings, where sex and age distributions align with previous studies investigating e-scooter-associated injuries [14–17].
The main focus of the current study was to assess the distribution of orthopaedic injuries caused by e-scooter accidents, rather than the associated burden. Nevertheless, given that 1,874 fractures were registered during the study period of roughly 3,5 years, out of which one third required surgical treatment, these injuries alone constitute a significant burden on healthcare systems especially given that the true number of injuries is likely significantly higher.
Ahluwalia et al. [18] found that injuries caused by e-scooter accidents impose a substantial burden on the healthcare system. The authors describe an average cost of almost 1,500 £ per patient in their study of 202 e-scooter injuries. Another study assessed the absence of work secondary to e-scooter accidents and found - quite surprisingly - that non-surgically treated patients were absent for about 1 month and surgically treated patients for up to 3 months [19].
A rise in e-scooter related injuries during the summer months was observed, consistent with previous research [15, 20]. This variation is not surprising because summer is the peak time for e-scooter usage, leading to increased demand. E-scooter use is not ideal in Sweden during winter due to snowy and icy road conditions. A Swedish study on e-scooter injuries [15] also found a peak in injuries during the weekend. Intoxication could be the reason behind the increase in weekend injuries seen in our studies, as studies have shown a strong link between intoxication and e-scooter injuries [21–23]. Because we lack data on alcohol and drug consumption, this contention is purely speculative.
By identifying common fractures caused by e-scooter accidents, we hope to raise awareness about the importance of safe e-scooter usage, including wearing protective gear, encouraging injury prevention measures and ultimately reducing the incidence and severity of orthopaedic injuries in this growing population.
Strengths and limitations
The major strength of the study is the large number of fractures that ensured an adequately large sample size to calculate the distribution of fractures caused by e-scooter accidents reliably. The SFR is a reliable source of information regarding demographic data, fracture classification and choice of treatment. However, because the analysis is based on the SFR, only injuries resulting in a fracture contingent on orthopaedic treatment are included. Hence, other injuries that may arise in e-scooter accidents, such as head injuries, thoracic and abdominal injuries and lacerations, are not reported. Fatally injured patients will never be included in the SFR. Moreover, the SFR, in its present form, does not report injuries with e-scooter involved suffered by pedestrians or cyclists as e-scooter injuries. Combined, these factors add to an underestimation regarding true impact of e-scooter-related fractures. Our study did not aim to describe the overall incidence of e-scooter accidents, but rather focused on the distribution of e-scooter orthopaedic injuries and their treatment.
As in all register-based studies, our study runs the risk of miscoding, misclassification, and transferring errors.
Future perspectives
With the help of data from the SFR, future investigations can examine trends in e-scooter-related orthopaedic trauma. A more comprehensive depiction of the orthopaedic trauma caused by e-scooter injuries could be achieved by adjusting the SFR to account for other injuries (e.g., individuals hit by an e-scooter or who trip over one). In addition, enabling registration of skull and rib fractures would strengthen the register’s ability to make an accurate description of the full panorama of skeletal injuries resulting from e-scooter accidents.
Conclusion
E-scooter-associated orthopaedic injuries tend to primarily affect the upper extremity. They constitute an increasing burden on emergency and orthopaedic departments in Sweden and other countries. The majority of patients were younger males, and there was a peak in injuries during summer and weekends. The study highlights the need for implementation of protective measures, in order to minimize these injuries.
Author contributions
BH: Writing of initial draft and revision of manuscript, interpretation of data. Preparation of figures. AB: Writing of manuscript, interpretation of data. Preparation of figures. Statistical analysis OW: Study design. Statistical analysis. Writing of manuscript All authors reviewed the manuscript.
Funding
Open access funding provided by Uppsala University.
Data availability
This study is based on data from the Swedish Fracture Register, who can be contacted via frakturregistret@vgregion.se.
Declarations
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Vallmuur K, Mitchell G, McCreanor V, Droder B, Catchpoole J, Eley R, et al. Electric personal MObility DEvices Surveillance (E-MODES) study: Injury presentations to emergency departments in Brisbane, Queensland. Injury. 2023. S0020-1383(23)00378-9. [DOI] [PubMed]
- 2.Coelho A, Feito P, Corominas L, Sánchez-Soler JF, Pérez-Prieto D, Martínez-Diaz S, et al. Electric Scooter-related injuries: a New Epidemic in Orthopedics. J Clin Med. 2021;10(15):3283. 10.3390/jcm10153283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Trivedi TK, Liu C, Antonio ALM, Wheaton N, Kreger V, Yap A, et al. Injuries Associated with Standing Electric Scooter Use. JAMA Netw Open. 2019;2(1):e187381. 10.1001/jamanetworkopen.2018.7381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bekhit MNZ, Le Fevre J, Bergin CJ. Regional healthcare costs and burden of injury associated with electric scooters. Injury. 2020;51(2):271–7. 10.1016/j.injury.2019.10.026 [DOI] [PubMed] [Google Scholar]
- 5.Möller M, Wolf O, Bergdahl C, Mukka S, Rydberg EM, Hailer NP, et al. The Swedish Fracture Register - ten years of experience and 600,000 fractures collected in a National Quality Register. BMC Musculoskelet Disord. 2022;23(1):141. 10.1186/s12891-022-05062-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, et al. Fracture and dislocation classification compendium – 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007;21(10 Suppl):S1–133. 10.1097/00005131-200711101-00001 [DOI] [PubMed] [Google Scholar]
- 7.Knutsson SB, Wennergren D, Bojan A, Ekelund J, Möller M. Femoral fracture classification in the Swedish Fracture Register – a validity study. BMC Musculoskelet Disord. 2019;20(1):197. 10.1186/s12891-019-2579-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bergvall M, Bergdahl C, Ekholm C, Wennergren D. Validity of classification of distal radial fractures in the Swedish fracture register. BMC Musculoskelet Disord. 2021;22(1):587. 10.1186/s12891-021-04473-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Juto H, Möller M, Wennergren D, Edin K, Apelqvist I, Morberg P. Substantial accuracy of fracture classification in the Swedish fracture Register: evaluation of AO/OTA-classification in 152 ankle fractures. Injury. 2016;47(11):2579–83. 10.1016/j.injury.2016.05.028 [DOI] [PubMed] [Google Scholar]
- 10.Bergdahl C, Nilsson F, Wennergren D, Ekholm C, Möller M. Completeness in the Swedish Fracture Register and the Swedish National Patient Register: an Assessment of Humeral Fracture registrations. Clin Epidemiol. 2021;13:325–33. 10.2147/CLEP.S307762 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of Observational studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg Lond Engl. 2014;12(12):1495–9. 10.1016/j.ijsu.2014.07.013 [DOI] [Google Scholar]
- 12.R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. [Internet]. 2023. https://www.R-project.org/.
- 13.Singh P, Jami M, Geller J, Granger C, Geaney L, Aiyer A. The impact of e-scooter injuries: a systematic review of 34 studies. Bone Jt Open. 2022;3(9):674–83. 10.1302/2633-1462.39.BJO-2022-0096.R1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.James A, Harrois A, Abback PS, Moyer JD, Jeantrelle C, Hanouz JL, et al. Comparison of Injuries Associated with Electric Scooters, motorbikes, and bicycles in France, 2019–2022. JAMA Netw Open. 2023;6(6):e2320960. 10.1001/jamanetworkopen.2023.20960 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Stigson H, Malakuti I, Klingegård M. Electric scooters accidents: analyses of two Swedish accident data sets. Accid Anal Prev. 2021;163:106466. 10.1016/j.aap.2021.106466 [DOI] [PubMed] [Google Scholar]
- 16.Raubenheimer K, Szeliga K, Manara JR, Fatovich DM, Plant JGA, Blakeney WG. Incidence, management, and Hospital costs of Orthopaedic injuries of E-Scooter riders in Western Australia. J Clin Med. 2023;12(20):6591. 10.3390/jcm12206591 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Leyendecker J, Hackl M, Leschinger T, Bredow J, Krane F, Eysel P, et al. Lessons learned? Increasing injury severity of electric-scooter accidents over a period of one year: a monocentric follow-up study at a level 1 trauma center. Eur J Orthop Surg Traumatol Orthop Traumatol. 2023;33(8):3643–8. 10.1007/s00590-023-03583-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ahluwalia R, Grainger C, Coffey D, Malhotra PS, Sommerville C, Tan PS, et al. The e-scooter pandemic at a UK Major Trauma Centre: a cost-based cohort analysis of injury presentation and treatment. Surg J R Coll Surg Edinb Irel. 2023;21(4):256–62. [DOI] [PubMed] [Google Scholar]
- 19.Kayaalp ME, Kilic NC, Kandemir I, Bayhan M, Eceviz E. Electric scooter-associated orthopedic injuries cause long absence from work, regret and are emerging as a major cause of hip fractures in young individuals: a comprehensive study from a regional trauma center in a densely populated urban setting. Eur J Trauma Emerg Surg off Publ Eur Trauma Soc. 2023;49(6):2505–13. 10.1007/s00068-023-02322-9 [DOI] [PubMed] [Google Scholar]
- 20.Uluk D, Lindner T, Dahne M, Bickelmayer JW, Beyer K, Slagman A, et al. E-scooter incidents in Berlin: an evaluation of risk factors and injury patterns. Emerg Med J EMJ. 2022;39(4):295–300. 10.1136/emermed-2020-210268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Osti N, Aboud A, Gumbs S, Engdahl R, Carryl S, Donaldson B, et al. E-scooter and E-bike injury pattern profile in an inner-city trauma center in upper Manhattan. Injury. 2023;54(5):1392–5. 10.1016/j.injury.2023.02.054 [DOI] [PubMed] [Google Scholar]
- 22.Blomberg SNF, Rosenkrantz OCM, Lippert F, Collatz Christensen H. Injury from electric scooters in Copenhagen: a retrospective cohort study. BMJ Open. 2019;9(12):e033988. 10.1136/bmjopen-2019-033988 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Puzio TJ, Murphy PB, Gazzetta J, Dineen HA, Savage SA, Streib EW, et al. The electric scooter: a surging new mode of transportation that comes with risk to riders. Traffic Inj Prev. 2020;21(2):175–8. 10.1080/15389588.2019.1709176 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
This study is based on data from the Swedish Fracture Register, who can be contacted via frakturregistret@vgregion.se.