

Abstract
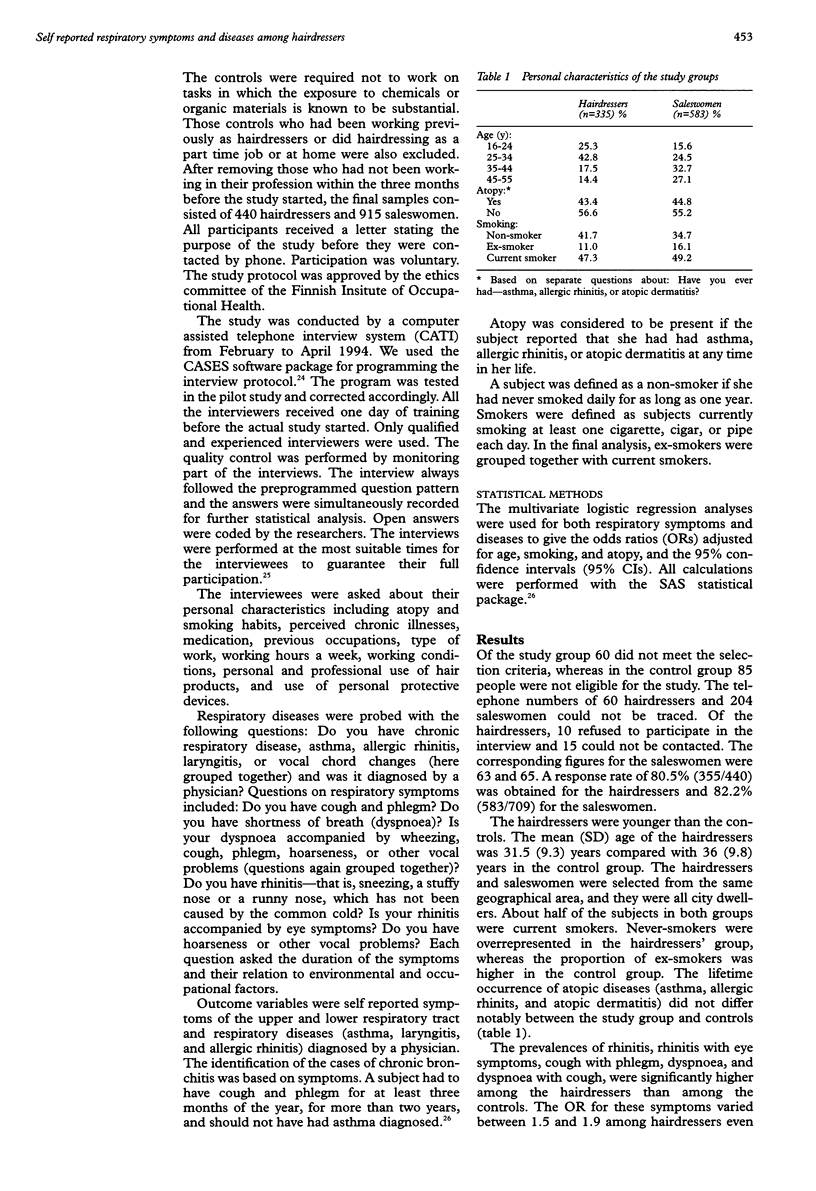
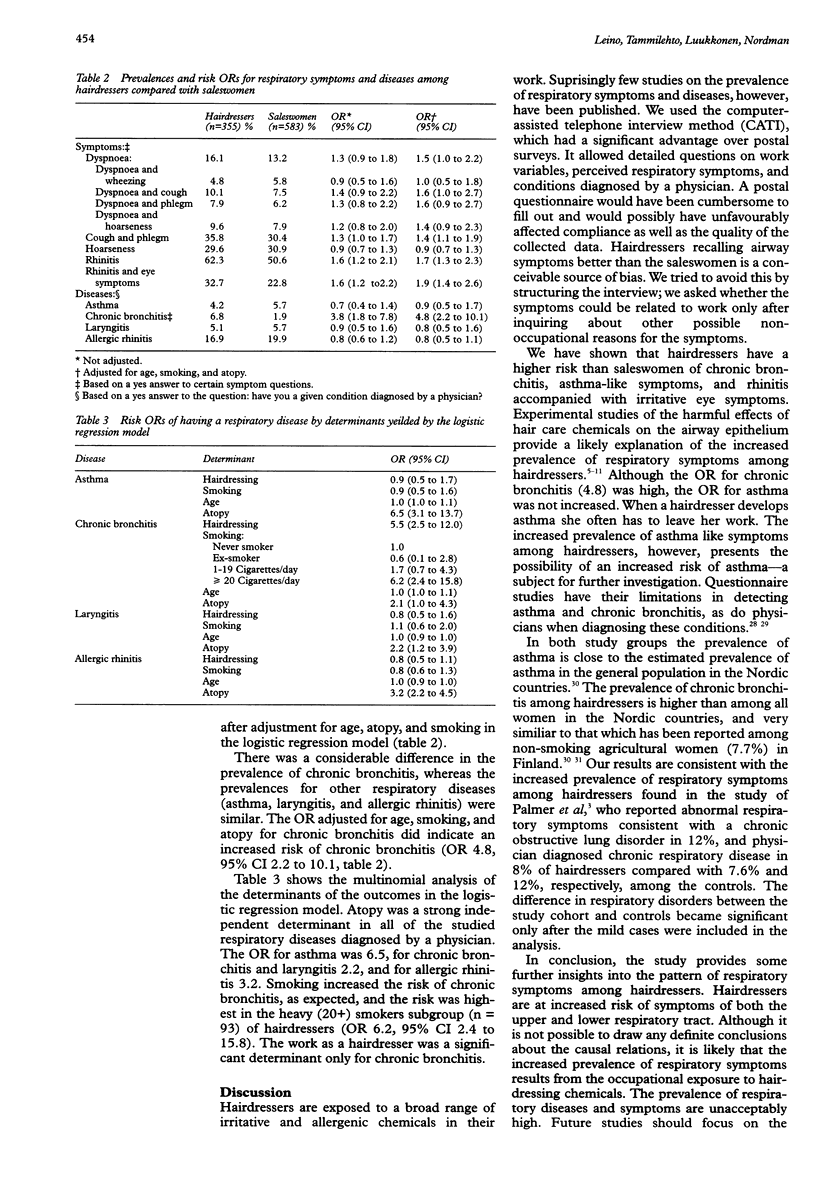
OBJECTIVES: Hairdressers are exposed to many irritative and allergenic substances capable of causing occupational respiratory symptoms and diseases. The self reported prevalence of respiratory symptoms and diseases was studied, and the risks among hairdressers compared with saleswomen was estimated. METHODS: A cross sectional prevalence study of respiratory symptoms and diseases was carried out among hairdressers and supermarket saleswomen, with a computer assisted telephone interview method (CATI). The study population comprised all the female hairdressers and supermarket saleswomen aged 15-54 years in the Helsinki metropolitan area, Finland. Disproportionate random samples of female hairdressers and sales-women were drawn from the trade union membership registers. The interviews were carried out between February and April 1994. A response rate of 80.5% (355/440) was obtained for hairdressers and 82.2% (583/709) for saleswomen. Atopy, smoking, chronic illnesses, type of work, working hours, working conditions, personal and professional use of hair products, and the use of personal protective devices were assessed. The outcome variables were self reported symptoms of the upper and lower respiratory tract. These were used to define chronic bronchitis, and asthma, laryngitis, and allergic rhinitis diagnosed by a physician. RESULTS: There was a considerable difference in the prevalence of chronic bronchitis; 6.8% in hairdressers versus 1.9% in saleswomen. The odds ratio (OR) adjusted for age, smoking, and atopy for chronic bronchitis indicated an increased risk of chronic bronchitis (OR 4.8, 95% confidence interval (95% CI) 2.2 to 10.1). No association was found between work as a hairdresser and asthma, laryngitis, and allergic rhinitis. Also the prevalence of rhinitis, rhinitis with eye symptoms, cough with phlegm, dyspnoea, and dyspnoea accompanied by cough was increased among hairdressers. The corresponding adjusted risk ORs were 1.7 (95% CI 1.3 to 2.3) for rhinitis, 1.9 (95% CI 1.4 to 2.6) for rhinitis with eye symptoms, 1.4 (CI 1.1 to 1.9) for cough with phlegm, 1.5 (95% CI 1.0 to 2.2) for dyspnoea, and 1.6 (95% CI 1.0 to 2.7) for dyspnoea with cough. CONCLUSIONS: Our results indicate an increased prevalence of upper and lower respiratory symptoms among hairdressers. Allergenic and irritative chemicals in hairdressing are likely candidates explaining the difference found between the hairdressers and controls. Work related reasons should be considered when a hairdresser presents with airway symptoms. Preventive actions are needed to improve the working conditions and personal protection.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ameille J., Pages M. G., Capron F., Proteau J., Rochemaure J. Pathologie respiratoire induite par l'inhalation de laque capillaire. Rev Pneumol Clin. 1985;41(5):325–330. [PubMed] [Google Scholar]
- BERGMANN M., FLANCE I. J., BLUMENTHAL H. T. Thesaurosis following inhalation of hair spray; a clinical and experimental study. N Engl J Med. 1958 Mar 6;258(10):471–476. doi: 10.1056/NEJM195803062581004. [DOI] [PubMed] [Google Scholar]
- Blainey A. D., Ollier S., Cundell D., Smith R. E., Davies R. J. Occupational asthma in a hairdressing salon. Thorax. 1986 Jan;41(1):42–50. doi: 10.1136/thx.41.1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borum P., Løkkegaard N., Holten A. Nasal mucociliary clearance in hairdressers: correlation to exposure to hair spray. Clin Otolaryngol Allied Sci. 1984 Dec;9(6):329–334. doi: 10.1111/j.1365-2273.1984.tb01516.x. [DOI] [PubMed] [Google Scholar]
- Friedman M., Dougherty R., Nelson S. R., White R. P., Sackner M. A., Wanner A. Acute effects of an aerosol hair spray on tracheal mucociliary transport. Am Rev Respir Dis. 1977 Aug;116(2):281–286. doi: 10.1164/arrd.1977.116.2.281. [DOI] [PubMed] [Google Scholar]
- GELFAND H. H. RESPIRATORY ALLERGY DUE TO CHEMICAL COMPOUNDS ENCOUNTERED IN THE RUBBER, LACQUER, SHELLAC, AND BEAUTY CULTURE INDUSTRIES. J Allergy. 1963 Jul-Aug;34:374–381. doi: 10.1016/0021-8707(63)90056-x. [DOI] [PubMed] [Google Scholar]
- Gebbers J. O., Tetzner C., Burkhardt A. Alveolitis due to hair-spray. Ultrastructural observations in two patients and the results of experimental investigations. Virchows Arch A Pathol Anat Histol. 1979 Jun 29;382(3):323–338. doi: 10.1007/BF00430408. [DOI] [PubMed] [Google Scholar]
- Li J. T., O'Connell E. J. Clinical evaluation of asthma. Ann Allergy Asthma Immunol. 1996 Jan;76(1):1–15. doi: 10.1016/S1081-1206(10)63400-X. [DOI] [PubMed] [Google Scholar]
- Meredith S., Nordman H. Occupational asthma: measures of frequency from four countries. Thorax. 1996 Apr;51(4):435–440. doi: 10.1136/thx.51.4.435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmer A., Renzetti A. D., Jr, Gillam D. Respiratory disease prevalence in cosmetologists and its relationship to aerosol sprays. Environ Res. 1979 Jun;19(1):136–153. doi: 10.1016/0013-9351(79)90042-2. [DOI] [PubMed] [Google Scholar]
- Pankow W., Hein H., Bittner K., Wichert P. Persulfat-Asthma im Friseurberuf. Pneumologie. 1989 Mar;43(3):173–175. [PubMed] [Google Scholar]
- Parra F. M., Igea J. M., Quirce S., Ferrando M. C., Martín J. A., Losada E. Occupational asthma in a hairdresser caused by persulphate salts. Allergy. 1992 Dec;47(6):656–660. doi: 10.1111/j.1398-9995.1992.tb02391.x. [DOI] [PubMed] [Google Scholar]
- Pepys J., Hutchcroft B. J., Breslin A. B. Asthma due to inhaled chemical agents--persulphate salts and henna in hairdressers. Clin Allergy. 1976 Jul;6(4):399–404. doi: 10.1111/j.1365-2222.1976.tb01922.x. [DOI] [PubMed] [Google Scholar]
- Renzetti A. D., Jr, Conrad J., Watanabe S., Palmer A., Armstrong J. Thesaurosis--from hairspray exposure--a nondisease. Validation studies of an epidemiologic survey of cosmetologists. Environ Res. 1980 Jun;22(1):130–138. doi: 10.1016/0013-9351(80)90124-3. [DOI] [PubMed] [Google Scholar]
- Schlueter D. P., Soto R. J., Baretta E. D., Herrmann A. A., Ostrander L. E., Stewart R. D. Airway response to hair spray in normal subjects and subjects with hyperreactive airways. Chest. 1979 May;75(5):544–548. doi: 10.1378/chest.75.5.544. [DOI] [PubMed] [Google Scholar]
- Schwaiblmair M., Baur X., Fruhmann G. Asthma bronchiale durch Blondiermittel im Friseurberuf. Dtsch Med Wochenschr. 1990 May 4;115(18):695–697. doi: 10.1055/s-2008-1065068. [DOI] [PubMed] [Google Scholar]
- Schwartz H. J., Arnold J. L., Strohl K. P. Occupational allergic rhinitis in the hair care industry: reactions to permanent wave solutions. J Occup Med. 1990 May;32(5):473–475. doi: 10.1097/00043764-199005000-00015. [DOI] [PubMed] [Google Scholar]
- Starr J. C., Yunginger J., Brahser G. W. Immediate type I asthmatic response to henna following occupational exposure in hairdressers. Ann Allergy. 1982 Feb;48(2):98–99. [PubMed] [Google Scholar]
- Stringer G. C., Hunter S. W., Bonnabeau R. C., Jr Hypersensitivity pneumonitis following prolonged inhalation of hair spray. Thesaurosis. JAMA. 1977 Aug 22;238(8):888–889. [PubMed] [Google Scholar]
- Terho E. O., Husman K., Vohlonen I. Prevalence and incidence of chronic bronchitis and farmer's lung with respect to age, sex, atopy, and smoking. Eur J Respir Dis Suppl. 1987;152:19–28. [PubMed] [Google Scholar]
- Torén K., Brisman J., Järvholm B. Asthma and asthma-like symptoms in adults assessed by questionnaires. A literature review. Chest. 1993 Aug;104(2):600–608. doi: 10.1378/chest.104.2.600. [DOI] [PubMed] [Google Scholar]
- Warr G. A., Martin R. R., Holleman C. L., Criswell B. S. Classification of bronchial lymphocytes from nonsmokers and smokers. Am Rev Respir Dis. 1976 Jan;113(1):96–100. doi: 10.1164/arrd.1976.113.1.96. [DOI] [PubMed] [Google Scholar]
- Zuskin E., Bouhuys A., Beck G. Hair sprays and lung function. Lancet. 1978 Dec 2;2(8101):1203–1203. doi: 10.1016/s0140-6736(78)92186-4. [DOI] [PubMed] [Google Scholar]
- Zuskin E., Loke J., Bouhuys A. Helium-oxygen flow-volume curves in detecting acute response to hair spray. Int Arch Occup Environ Health. 1981;49(1):41–44. doi: 10.1007/BF00380807. [DOI] [PubMed] [Google Scholar]