

Abstract
Brain metastases during pregnancy poses complex conundrum in management. Stereotactic radiosurgery (SRS) offers valuable option to clinicians in this scenario. We reviewed and described the safety and effectiveness of Gamma Knife (GK) SRS in treating a solitary cerebellar metastasis in a patient with recurrent breast cancer at 28 weeks of gestation. Following multidisciplinary discussion, she consented for urgent single session GK SRS to the brain metastasis with 2 cycles of 3-weekly paclitaxel chemotherapy prior to planned delivery at term. Prior to the frame-based treatment, a trial run with dosimeters placed on the superior and inferior parts of foam knee support showed radiation exposure of 3.12 mSv and 1.06 mSv respectively. A prescription dose of 16 Gy at the 50% isodose was delivered using 24 isocentres over 39.7’ of beam on time. The treatment plan had 98% coverage, 89% selectivity and a gradient index of 2.98. Dosimeters placed near the uterine fundus and suprapubic region (consistent with location of fetal head) during the actual treatment recorded 2.83 mSv and 0.27 mSv, which is lower than the trial dosimeter readings. The patient successfully completed SRS treatment and gave birth to a healthy baby two months later. Follow-up MRI at three months interval showed total resolution of the lesion. GK SRS is known for the lowest extracranial dose compared to other SRS modalities. This report and literature review confirmed that GK is a sharp and effective, yet gentle and safe treatment for pregnant patients with brain metastases.
Keywords: stereotactic radiosurgery, Gamma Knife, pregnancy, brain metastasis, dosimetry
INTRODUCTION
Brain metastases during pregnancy poses complex conundrum in management. Treatment needs to be tailored individually according to the disease extent, expected pregnancy outcome and patients’ wish. Stereotactic radiosurgery (SRS) offers valuable option to clinicians in this context. This case report describes the safety and effectiveness of Gamma Knife (GK) SRS in treating a solitary cerebellar metastasis in a 42-year-old woman with recurrent breast cancer at the third trimester of pregnancy. Compared to surgical excision of the brain metastasis with the risk of preterm delivery and subsequent perinatal complications, GK treatment allows the pregnancy to advance with concurrent systemic treatment to ensure better overall outcome for the patient and her whole family.
Case Report
We report a 42-year-old lady who presented with dizziness and unsteady gait during her third pregnancy at 28 weeks of gestation. She had a known case of triple negative breast carcinoma with local recurrence a year ago which she had received second line chemotherapy. Upon presentation, she was fully conscious with neurological examination showing right cerebellar signs. Brain MRI showed a solitary right cerebellar enhancing mass, 2.0 × 2.7 × 2.1 cm3 with perilesional edema and a hemosiderin rim likely represent hemorrhagic metastasis. Chest X-ray showed multiple cannon ball lesions. Therefore, a diagnosis of stage 4 breast cancer with symptomatic brain and lung metastasis was made. Obstetrical assessment revealed singleton fetus with gestation appropriate growth parameters and estimated fetal weight of 1 kg.
An urgent family conference was held, and family was informed regarding her situation. The aim of treatment was for sequencing palliation of symptoms and delaying her disease progression. She expressed her wish that this pregnancy was precious to her, and she would like to maintain a safe pregnancy till term if possible. Following multidisciplinary team discussion, she was offered an urgent single session SRS to the brain metastasis with 2 cycles of 3-weekly paclitaxel chemotherapy. This would be followed by planned delivery of the fetus at term before subsequent palliative treatment. Prior to the frame-based SRS using Leksell GK Icon, we performed a trial run with two dosimeters placed on the top and bottom parts of a foam knee support at a distance from the isocentre that mimicked the patient with gravid uterus (Figure 1). The dosimeters showed a radiation exposure of 3.12 mSv and 1.06 mSv respectively, which was below the acceptable 100 mSv fetal tolerance (1). Transabdominal ultrasound was done prior to treatment in order to localize the fetal head and it was confirmed to be in cephalic position. Treatment planning was performed and 16 Gy was prescribed at the 50% isodose using 24 isocentres over 39.7’ of beam on time (Figure 2). This treatment plan provided 98% coverage and 89% selectivity with a Gradient Index 2.98. The maximum dose volume to brainstem was 8.5 Gy which was within the acceptable range. We did not use any abdominal shielding during the treatment. Dosimeters were placed near her uterine fundus and suprapubic region (consistent with localization of fetal head), and it recorded 2.83 mSv and 0.27 mSv of extracranial radiation exposure respectively (Figure 1).
Figure 1.
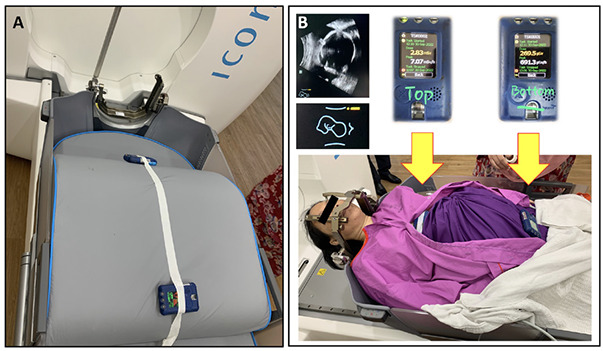
A) Trial run by placing dosimeters at the top and bottom parts of a foam knee support at a distance that mimicked the patient with gravid uterus to predict radiation exposure. B) Dosimeters placed near uterine fundus and suprapubic region (consistent with concomitant ultrasound localization of fetal head) during actual treatment recorded the actual extracranial dose exposure, which were 2.83 mSv and 0.270 mSv respectively.
Figure 2.
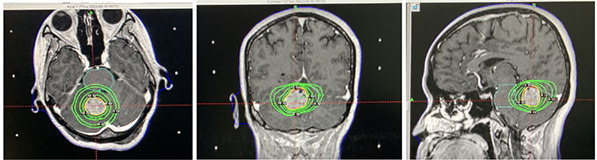
Actual treatment was performed at 16 Gy of 50% isodose in 24 shots over 39.7' beam on time. This treatment plan showed 98% coverage, 89% selectivity and gradient index 2.98. The maximum dose to brainstem was predicted at 8.5 Gy.
The patient successfully completed SRS treatment without complication. She received two cycles of chemotherapy subsequently. Repeat imaging after 4 weeks showed marked reduction of lesion size to 0.8 × 1.0 × 0.8 cm3. This represents an approximate volume reduction of approximately 94%. Two months post treatment, she gave birth to a healthy baby boy safely via caesarian section. Another MRI brain at 3 months interval showed complete resolution of the lesion with no new brain metastases (Figure 3). She had good bonding with her baby for 6 months, but she sadly succumbed at 8 months post GK treatment due to systemic disease progression despite on-going palliative chemotherapy. The baby was healthy with normal developmental progress while she remained neurologically intact with good cognitive function until she passed away.
Figure 3.
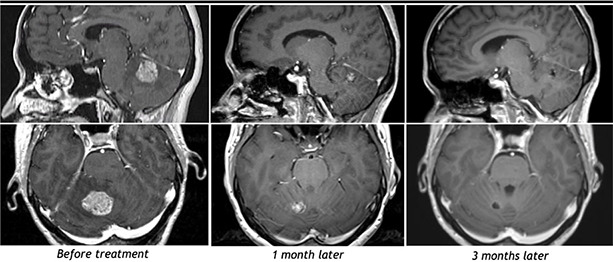
Serial MRI brain (T1WI with gadolinium) showing the result of GK SRS on the right cerebellar metastasis. There was total resolution of the lesion at 3 months post treatment.
DISCUSSION AND LITERATURE REVIEW
Brain metastasis during pregnancy is a rare and complicating occurrence with a cumulative incidence of 1 in 1000–2000 pregnancies (2,3). The most common primary cancer was found to be from breast (36%) (3). There is lack of guidelines and clinical consensus in this scenario, making it challenging to manage (2,3). Management should always ensure maternal safety during cancer treatment while maintaining fetal viability (3). Surgery followed by whole brain radiotherapy (WBRT) has been considered as standard first-line treatment for single brain metastasis in patients with favorable performance status and limited extracranial disease in a general cancer patient population of male and female non-pregnant individuals (3, 4). However, offering surgical excision to this posterior fossa lesion carries significant maternal and fetal risk in view of the difficulty in positioning and anaesthesia (4, 5). Delivering at 28 weeks of gestation will definitely increase the perinatal risk and subsequently affect the fetal outcome. At the same time, her extensive lung metastasis would preclude her from fitness for general anaesthesia. SRS treatment has been shown to result in equivalent outcome in terms of survival, neurological death rates and local recurrence when compared to surgery and WBRT in patients with single small-sized brain metastasis (6). SRS also allows treatment of multiple lesions at different locations simultaneously and it alleviates anaesthetic and surgical risks (7).
Radiation therapy and chemotherapy may be allowed during the third trimester of pregnancy without needing to deliver the fetus but risks need to be discussed with the patient (3). According to the report by American Association of Physicists in Medicine (AAPM) Radiation Committee Task Group No 36, fetal dose of ≤100 mGy from exposure to radiotherapy carries little or uncertain risk to the unborn baby (1). Thus, 100 mGy (or equivalent to 100 mSv) has been known as the usual tolerance threshold for radiotherapy during pregnancy (1, 8, 9). Another study by Ioffe et al summarized that the risk of radiation induced disorders to the foetus reduced with the advancement of pregnancy gestation (10). For example, at pre-implantation stage, a 100 mGy radiation may induce abortion, while in third trimester, only doses above 500 mGy may potentially cause growth retardation. In fact, this threshold dose for radiation effects is not generally reached with common curative radiotherapy during pregnancy, provided that tumours are located sufficiently far from the fetus and that precautions have been taken appropriately (11). As of our patient, who had reached third trimester, the risk of brain damage and other long term adverse effect is small if we carefully plan the SRS treatment following the standard guideline for fetal dose.
Across different modalities of SRS, GK has been the safest in terms of lowest peripheral dose (12). Study by Di Betta et al has shown that, the Model C GK was associated with the lowest peripheral dose yet achieved comparable treatment dose at the target site compared to Linac, CyberKnife and TomoTherapy (12). Recently, Paddick et al has examined the extracranial dose received during GK intracranial SRS treatment and its related risks (13). Compared to Linac and CyberKnife, the newer GK Perfexion again showed the lowest mean extracranial dose with less than 0.002% prescription dose detected near the gonads (13). This potential extracranial dose is influenced by multiple factors, including treatment platform, prescription dose, collimator size, beam number and other planning variables (13). With the treatment plan for this patient, we verified dosimetrically that the extracranial radiation exposure to the fetal head was as low as 0.27 mGy, which is unlikely to be harmful to the unborn baby. We also showed that the readily available foam knee support may act adequately as a “phantom” in the urgent situation where proper anthropomorphic phantom is not available, and predicted the actual radiation exposure to within 10%. In view of this negligible peripheral dose from trial run, we did not apply any abdominal shielding for this patient during the actual treatment.
In the literature review by Sharma et al, there was a total of four cases of brain metastases from breast cancer during pregnancy reported, in which three were surgically treated combined with or without conventional radiotherapy and systemic chemotherapy (2). Of these cases, two were complicated with perinatal morbidity (2). Pantelis et al reported a case of rapidly growing deep-seated high grade glioma during the third trimester of pregnancy which was successfully treated using CyberKnife SRS and a recorded fetal dose of 40 mGy (14). On another hand, Yu et al reported their treatment using a Model C GK for a patient with solitary metastatic melanoma of the brain at 25th week of pregnancy (15). Similarly, the authors pre-ran with a phantom estimation and subsequently recorded a safe fetal radiation dose of 1.5–3.1 mGy, which is in concordance to our data (15).
In our patient, GK treatment to the symptomatic cerebellar metastasis avoided her from an invasive neurosurgical procedure which carried significant anaesthetic and fetal risk. It also eliminated the need for preterm delivery and allowed her to carry on with pregnancy till term. Adequate gestational age and fetal weight would markedly improve the pregnancy outcome by lowering perinatal risk and maternal morbidity. This approach also allowed concurrent chemotherapy for better disease control in patients with extensive systemic disease, which conventionally would be delayed if surgery was performed.
Of utmost importance, the patient and family’s wish needs to be taken into consideration in the treatment plan. A multidisciplinary team meeting and consensus is crucial in order to consider all potential problems and offer best treatment of care tailored individually according to the patient’s need.
CONCLUSION
In conclusion, with a low fetal dose exposure and serial imaging, we confirmed that GK SRS is effective in treating brain metastases, yet gentle and safe even in pregnant patients. Most importantly, it improves patient’s quality of life and fetal outcome with lower perinatal risk and maternal morbidity.
ACKNOWLEDGEMENTS
We acknowledged the contributions of all medical and healthcare professionals from all subspecialties in the management of this complex case. Part of the data in this case report has been presented in a regional conference in the form of online oral presentation in February 2023, but not published in any proceedings.
Authors’ disclosure of potential conflicts of interest
The authors have nothing to disclose.
Author contributions
Data collection: BeeHong Soon, Marfu’ah Nik Ezzamudden, Shahizon Azura Mohamed Mukari, Aida-Widure Mustapha Mohd Mustapha, Aida Hani Mohd Kalok
Literature review: Fuad Ismail, Norlia Abdullah
Manuscript writing: BeeHong Soon, Ramesh Kumar
Final approval of manuscript: Ian Paddick, Ramesh Kumar
REFERENCES
- 1.Stovall M, Blackwell C, Cundiff J, Novack D, Palta J, Wagner L, Webster E, Shalek R. Fetal dose from radiotherapy with photon beams: Report of AAPM Radiation Therapy Committee Task Group No 36. Med. Phys. 1995;22:63–82. doi: 10.1118/1.597525 [DOI] [PubMed] [Google Scholar]
- 2.Sharma A, Nguyen HS, Lozen A, Sharma A, Mueller W. Brain metastases from breast cancer during pregnancy. Surg Neurol Int. 2016. Sep 1;7(Suppl 23):S603–S606. doi: 10.4103/2152-7806.189730. PMID: 27656319; PMCID: PMC5025954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Proskynitopoulos PJ, Lam FC, Sharma S, Young BC, Laviv Y, Kasper EM. A review of the neurosurgical management of brain metastases during pregnancy. Can J Neurol Sci. 2021. Sep;48(5):698–707. doi: 10.1017/cjn.2020.254. Epub 2020 Nov 20. PMID: 33213549; PMCID: PMC8527832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nahed BV, Alvarez-Breckenridge C, Brastianos PK, Shih H, Sloan A, Ammirati M, Kuo JS, Ryken TC, Kalkanis SN, Olson JJ. Congress of Neurological Surgeons systematic review and evidence-based guidelines on the role of surgery in the management of adults with metastatic brain tumors. Neurosurgery. 2019. Mar 1;84(3):E152–E155. doi: 10.1093/neuros/nyy542. PMID: 30629227. [DOI] [PubMed] [Google Scholar]
- 5.Shiro R., Murakami K., Miyauchi M., Sanada Y., Matsumura N. Management strategies for brain tumors diagnosed during pregnancy: A case report and literature review. Medicina 2021;57:613. https://doi.org/10.3390/medicina57060613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Muacevic A, Wowra B, Siefert A, Tonn JC, Steiger HJ, Kreth FW. Microsurgery plus whole brain irradiation versus Gamma Knife surgery alone for treatment of single metastases to the brain: a randomized controlled multicentre phase III trial. J Neurooncol. 2008. May;87(3):299–307. doi: 10.1007/s11060-007-9510-4. Epub 2007 Dec 22. PMID: 18157648. [DOI] [PubMed] [Google Scholar]
- 7.Meier R. Stereotactic radiosurgery for brain metastases. Transl Cancer Res 2014;3(4):358–366. doi: 10.3978/j.issn.2218-676X.2014.08.03 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Michalet M, Dejean C, Schick U, Durdux C, Fourquet A, Kirova Y. Radiotherapy and pregnancy. Cancer Radiother. 2022. Feb-Apr;26(1–2):417–423. doi: 10.1016/j.canrad.2021.09.001. Epub 2021 Dec 23. PMID: 34953688. [DOI] [PubMed] [Google Scholar]
- 9.ICRP 2000 Pregnancy and medical radiation. ICRP Publication 84. Ann. ICRP 30 (1). [DOI] [PubMed]
- 10.Ioffe V, Hudes RS, Shepard D, Simard JM, Chin LS, Yu C. Fetal and ovarian radiation dose in patients undergoing Gamma Knife radiosurgery. Surg Neurol. 2002. Jul;58(1):32–41; discussion 41. doi: 10.1016/s0090-3019(02)00742-5. PMID: 12361645. [DOI] [PubMed] [Google Scholar]
- 11.Kal HB, Struikmans H. Radiotherapy during pregnancy: Fact and fiction. Lancet Oncol. 2005. May;6(5):328–333. doi: 10.1016/S1470-2045(05)70169-8. PMID: 15863381. [DOI] [PubMed] [Google Scholar]
- 12.Di Betta E, Fariselli L, Bergantin A, Locatelli F, Del Vecchio A, Broggi S, Fumagalli ML. Evaluation of the peripheral dose in stereotactic radiotherapy and radiosurgery treatments. Med Phys. 2010. Jul;37(7):3587–3594. doi: 10.1118/1.3447724. PMID: 20831066; PMCID: PMC2902541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Paddick I, Cameron A, Dimitriadis A. Extracranial dose and the risk of radiation-induced malignancy after intracranial stereotactic radiosurgery: Is it time to establish a therapeutic reference level? Acta Neurochir (Wien). 2021. Apr;163(4):971–979. doi: 10.1007/s00701-020-04664-4. Epub 2020 Dec 15. PMID: 33325003; PMCID: PMC7966618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pantelis E, Antypas C, Frassanito MC, Sideri L, Salvara K, Lekas L, Athanasiou O, Piperis M, Salvaras N, Romanelli P. Radiation dose to the fetus during CyberKnife radiosurgery for a brain tumor in pregnancy. Phys Med. 2016. Jan;32(1):237–241. doi: 10.1016/j.ejmp.2015.09.014. Epub 2015 Oct 23. PMID: 26508017. [DOI] [PubMed] [Google Scholar]
- 15.Yu C, Jozsef G, Apuzzo ML, MacPherson DM, Petrovich Z. Fetal radiation doses for model C Gamma Knife radiosurgery. Neurosurgery. 2003. Mar;52(3):687–693; discussion 693. doi: 10.1227/01.neu.0000048479.23069.24. PMID: 12590695. [DOI] [PubMed] [Google Scholar]