

Key Clinical Message
Maxillary canines are often impacted, which can result in tooth disorders and adversely affect occlusal and facial development. The case report describes complete bilateral impaction of maxillary canines and significant root resorption of a central incisor. The multidisciplinary approach is the optimal strategy for addressing impacted maxillary canines.
Keywords: aesthetic veneer, flap, implant anchorage, maxillary impacted canines, multidisciplinary treatment, subcutaneous tunnel
1. INTRODUCTION
Proper tooth development of teeth is crucial in growing individuals for the prevention of malocclusion and enhancement of facial aesthetics. Dental impaction occurs when a tooth remains embedded in the alveolar bone and fails to erupt into the oral cavity at the expected time. 1 Tooth impaction is a common dental condition, affecting 0.8%–3.6% of the general population. 2 The prevalence of maxillary canine impaction ranges from 1.0% to 2.5%, with 8.0%–10.0% of these cases being bilateral. Considering factors, such as sex and geographic location, it has been reported that the incidence of impacted maxillary central incisors is more common in females, being twice that of males. In a study using cone‐beam computed tomography (CBCT), 45.2% of the maxillary canines were impacted labially, 40.5% were impacted palatally, and 14.3% were impacted in the mid‐alveolus. 3 Previous studies have recommended immediate application of orthodontic forces following surgical exposure. 4 However, several potential complications may arise following the surgical exposure and orthodontic forced eruption of impacted maxillary canines, including root resorption, periodontal defects, poor esthetic results, and immobility. The present case elucidates how multidisciplinary orthodontic treatment can significantly reduce root resorption, restore the occlusal relationship, and achieve stable and aesthetic results.
2. CASE REPORT
2.1. Case history and diagnosis
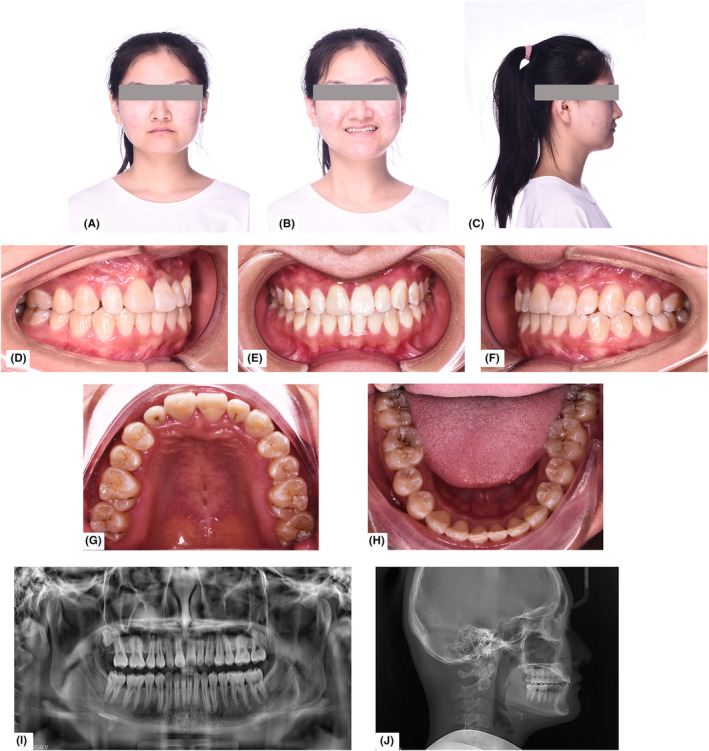
A 12‐year‐old Chinese preadolescent female presented to the orthodontic clinic with concerns about her smile. Oral examination revealed good oral hygiene. The right deciduous canine was present in the maxilla, while bilateral permanent canines were missing from the dentition. The mandibular dentition exhibited crowding, a deep curve of Spee, a Class III overbite, and lingual inclination of the anterior teeth. The bilateral molar relationship was classified as Angle Class II Division 2 (Figure 1).
FIGURE 1.
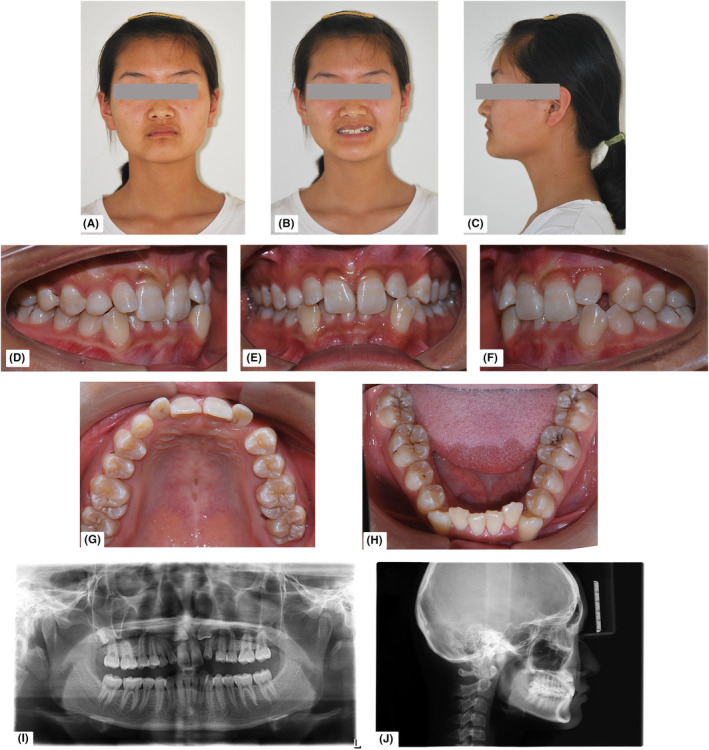
Pre‐treatment facial photographs (A–C), intraoral photographs (D–H), panoramic radiograph (I), and cephalometric radiograph (J).
A cephalometric radiograph indicated a tendency toward a horizontal growth pattern (Figure 1, Table 1). Both maxillary canines were impacted, located mesially at a high level. CBCT was performed following informed consent to assess the condition of the bilateral impacted canines. The crown of the upper left canine was positioned mesial to the apex of the root of the upper left lateral incisor, while that of the upper right canine was present above the upper right incisor root, with more than two‐thirds of the root resorbed (Figure 2).
TABLE 1.
Cephalometric analysis in pre‐treatment and after‐treatment.
| Measurement | Initial | Final | Normal | Standard deviation |
|---|---|---|---|---|
| SNA | 80.8 | 86.3 | 83 | 4 |
| SNB | 83.1 | 83.9 | 80 | 4 |
| ANB | −2.3 | −0.7 | 3 | 2 |
| Facial angle | 88.7 | 89.2 | 85 | 3 |
| NA‐APo (convexity) | −5.5 | −4.2 | 6 | 4 |
| U1‐NA (mm) | 6 | 4.7 | 5 | 2 |
| U1‐NA | 25.7 | 27.8 | 23 | 5 |
| L1‐NB (mm) | 0.3 | 3 | 7 | 2 |
| L1‐NB | 14.8 | 24.2 | 30 | 6 |
| U1‐L1 | 141.8 | 130.3 | 124 | 8 |
| U1‐SN | 99.5 | 106.4 | 106 | 6 |
| SN‐MP | 25 | 19.6 | 30 | 6 |
| IMPA | 86.7 | 93.7 | 97 | 6 |
| Y‐axis (SGn‐FH) | 61 | 61.8 | 64 | 2 |
| Po‐NB (mm) | 2.8 | 3.9 | 4 | 2 |
FIGURE 2.
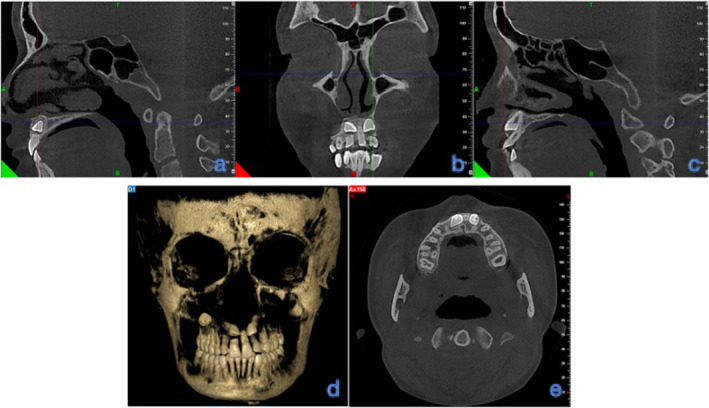
Cross‐sectional cone‐beam computed tomography (CBCT) views (A–E).
2.2. Treatment alternatives
Two treatment options were considered. The first option involved the orthodontic forced eruption of tooth 13 to replace tooth 11, and enhancing the crown appearance of tooth 13 with aesthetic veneers. The second option involved removing tooth 11, maintaining the gap, and correcting tooth 13 to align with the dentition. The gap resulting from the removal of tooth 11 is typically addressed through implant placement once the patient reaches adulthood. However, the drawback of this approach is the poor aesthetic appearance of the patient's smile before adulthood, potentially hindering physiological and psychological development. Consequently, this option was rejected by the patient and her parents.
2.3. Treatment objectives
The treatment objectives included: correcting dentition crowding; orthodontic forced eruption of the impacted bilateral upper canines to their correct positions due to severe root resorption of tooth 11 and its poor long‐term prognosis, leading to the recommendation of extracting tooth 11 and replacing it with tooth 13; establishing normal overbite and overjet relationships; restoring the aesthetics of the anterior teeth; and caries restoration using aesthetic resin for long‐term health.
2.4. Treatment progress
2.4.1. Orthodontic phase
Fixed brackets were bonded to all teeth except for teeth 12, 22, 32, 42, 31, and 41.
2.4.2. Surgical phase
One week later, under local infiltration anesthesia, a flap surgical procedure was performed to expose the coronal and labial aspects of maxillary teeth 13 and 23 (Figure 3). Using CBCT guidance, bone resistance was removed to expose tooth 13. A subcutaneous tunnel was created by removing bone tissue resistance, extending from the mesial side of tooth 25 to the distal side of tooth 24. An elastic chain was attached to tooth 13, passed through the subcutaneous tunnel, and positioned at the implant anchorage, with 4.5 oz force applied every 3 weeks. Additionally, an upright axial spring was attached to the crown of tooth 13 to manage the path and root torque during the distal orthodontic forced eruption of the canine. The central incisor provided the tensile force until resistance was encountered. The central incisor was then extracted, and implant anchorage, reinforced with a stainless‐steel wire, was obtained from the mesial alveolar bone of tooth 14 (Figures 3D and 4B,C).
FIGURE 3.
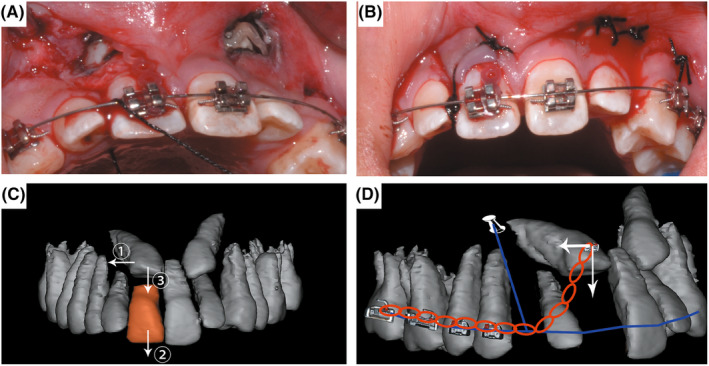
Photographs and schematic diagrams of orthodontic forced eruption design for tooth 13. (A) surgical exposure of bilaterally impacted canines, (B) subcutaneous channels for bilaterally impacted canines, (C) cone‐beam computed tomography (CBCT) reconstruction of maxillary dentition using MIMICS, ① guiding the dental crown of tooth 13 distally, ② hopeless tooth 11 was extracted when resistance was encountered during vertical traction of tooth 13, and ③ guiding the crown of tooth 13 towards the vertical direction; (D) mechanical analysis of the traction applied to tooth 13; blue line: stainless steel archwire; red chain: elastic chain for orthodontic forced eruption of tooth 13.
FIGURE 4.
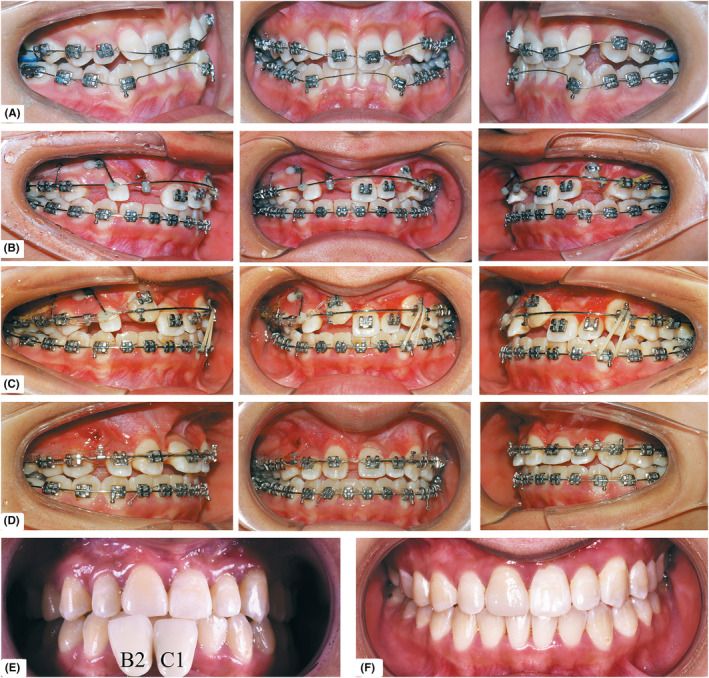
Treatment progress. (A) Aligning of dentition, (B) traction of impacted teeth 13 and 23, (C) replacing tooth 11 with tooth 13, (D) correct midline achieved using implant anchorage, (E) crown restoration of tooth 13 using aesthetic veneer imitating tooth 21, and (F) dental whitening.
Two weeks postoperatively, 0.016‐in. nickel‐titanium (NiTi) arch wires were replaced. A NiTi spring was used to expand the space between teeth 22 and 24. Tooth 11, showing progressive root resorption due to the eruption of tooth 13, was promptly extracted. An elastic chain was applied to the erupting tooth 13 until the traction hook was vertically pulled downward, and the elastic chain was replaced with 0.018 × 0.025 in. stainless steel wire.
Upon successful orthodontic forced eruption of teeth 13 and 23, implant anchorage was applied between teeth 12 and 14 to mesially adjust the upper right dentition. This approach, combined with a hook, enhanced the anchorage of the anterior teeth during the orthodontic forced eruption, resulting in the complete alignment of teeth 13 and 23 within the dental arch. The upper right posterior dentition was mesially repositioned using implant anchorage (Figure 4).
2.4.3. Prosthetic phase
Aesthetic veneer restoration of teeth 12 and 13 was performed by the Department of Prosthodontics. The crown shape of tooth 13 was modified to resemble tooth 11. To enhance the aesthetic appeal of the anterior teeth, a tooth whitening procedure was performed. Additionally, resin restorations of the decayed teeth, including 12, 16, 22, 26, 36, 37, 46, and 47, were performed (Figures 5 and 6).
FIGURE 5.
Post‐treatment facial photographs (A–C), intraoral photographs (D–H), panoramic radiograph (I), and cephalometric radiograph (J).
FIGURE 6.
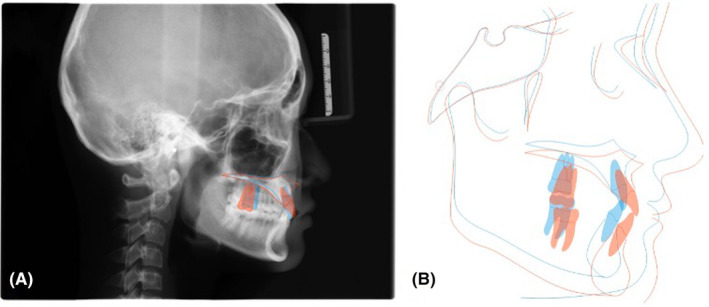
Cephalometric overlap pre‐treatment and after‐treatment.
2.5. Treatment results
Following the intervention, significant outcomes were observed (Figures 5 and 7).
Multidisciplinary treatment successfully guided teeth 13 and 23 into the dentition; the roots showed no obvious resorption, and the gingival shapes were well‐maintained. The crown shape of tooth 13 was modified to resemble tooth 11, and tooth 12 was restored using aesthetic veneers.
The aesthetics of anterior teeth were favorably restored.
Anterior crowding and occlusion were successfully corrected.
The facial profile showed significant improvement.
FIGURE 7.
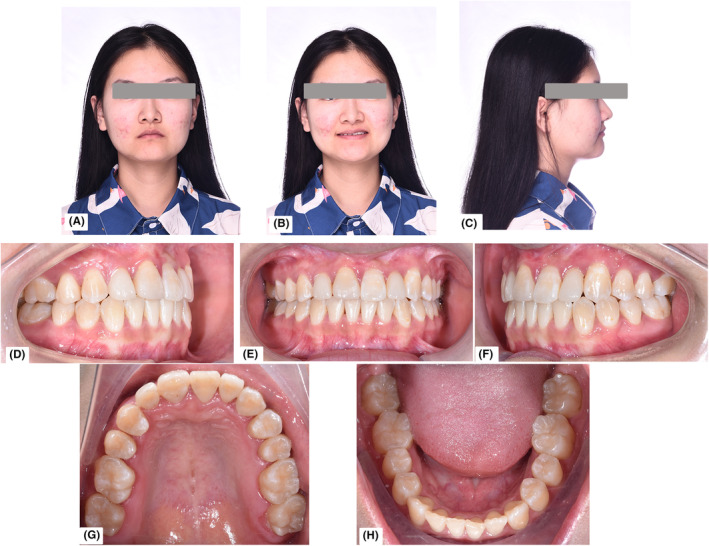
Facial (A–C) and intraoral (D–H) photographs after 3 years of follow‐up.
3. DISCUSSION
Bilateral canine impaction can lead to various complications, including aesthetic and phonetic compromises, arch length reduction, and referred pain. 5 , 6 , 7 Management strategies for impacted canines include surgical exposure followed by orthodontic forced eruption, replacement through fixed prosthodontics with or without dental implants, and removable prosthodontics. 8 In this case, both upper canines were classified as high‐level impacted teeth, with over two‐thirds root resorption of tooth 11 due to the compressive force from the crown of tooth 13. Based on the principle of maximum preservation and aesthetic considerations, the maxillary impacted canine was used to replace a central incisor with poor prognosis through multidisciplinary treatment.
Cassina et al. 9 stated that canine localization and its orthodontic forced eruption path are significantly associated with treatment duration. For buccal canine impactions, the position relative to the mucogingival junction determines the choice of surgical procedure, Class II impacted maxillary canines are often located in the center of or labial to the alveolar crest. 10 In these cases, management involves a closed eruption technique with flap repositioning. Depending on the direction of force, this surgical technique can facilitate forced eruption through an adequate zone of keratinized gingiva. The primary advantages of this technique include less postoperative discomfort compared to gingivectomy and forced eruption through a zone of keratinized gingiva. 10 , 11 , 12
In the early stage of this case, implant anchorage was obtained from a high position of the zygomatic alveolar ridge region of the left maxilla. Additionally, a subcutaneous tunnel was designed within the vestibular sulcus. Orthodontic force was primarily used to achieve distal movement of tooth 13 until bone resistance was encountered. Subsequently, vertical force was applied only after tooth 13 had been distally repositioned to align with tooth 12.
For canines in less favorable positions, the demand for anchorage is crucial. 13 In this case, tooth 11 exhibited negligible retention value due to significant root resorption. Aligning tooth 13 with tooth 11 in the initial phase, following the surgical flap procedure, minimized anchorage loss by directing the eruption of tooth 13 toward the crown and root of tooth 11. This allowed retention of tooth 11 during the initial phase, and reduced the potential for accelerated alveolar bone resorption, following its extraction. Previous studies have suggested that root resorption of the maxillary incisor after traction of bilateral impacted canines through reinforced anchorage does not pose a risk to the integrity of the maxillary incisor root. 14 In this case, after traction of tooth 23, the root of tooth 21 did not undergo root resorption. Following the successful correction of teeth 13 and 23, implant anchorage was used to move the right upper posterior teeth and shift the molar from a neutral to a distal relationship. The midline alignment of the upper and lower dentitions remained unaltered with implant anchorage. These factors indicated that an optimized anchorage design could reduce the complication rate during the traction of impacted teeth and achieve better aesthetics after treatment.
Orthodontic forced canine replacement of incisors can result in side‐effects, such as poor occlusal function, early cusp contact, and poor aesthetics. 15 , 16 Numerous studies have indicated that oral restorations can be used to alter the crown or veneer of the teeth in the replacement position, enhancing both function and aesthetics during the later phases of multidisciplinary treatment. 17 , 18 In this case, the aesthetic veneer restoration design for tooth 13 was modified to resemble the crown shape of tooth 21, significantly improving the aesthetic appearance of the dental arch.
4. CONCLUSIONS
Multidisciplinary orthodontic treatment required a comprehensive diagnosis and adequate evaluation to formulate a reasonable treatment plan. This led to good treatment control and improved patient compliance. The multidisciplinary treatment concept facilitated stable and successful treatment, and achieved ideal aesthetics for the patient.
AUTHOR CONTRIBUTIONS
Li‐Ming Wen: Data curation; formal analysis; methodology; writing – original draft; writing – review and editing. Yang‐Yang Song: Project administration; writing – review and editing. Ji‐Nan Liu: Data curation; formal analysis; methodology. Ye Zhu: Data curation; formal analysis; methodology. Xiao‐Feng Huang: Conceptualization; methodology; project administration; supervision; validation; writing – review and editing.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
It is our routine standard surgical procedure, so ethical clearance was not required.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
ACKNOWLEDGMENTS
The authors do not have any financial interest in the companies whose materials are included in this article.
Wen L‐M, Song Y‐Y, Liu J‐N, Zhu Y, Huang X‐F. Maxillary impacted canine replacing a central incisor with root resorption: Multidisciplinary treatment in a preadolescent patient. Clin Case Rep. 2024;12:e9230. doi: 10.1002/ccr3.9230
DATA AVAILABILITY STATEMENT
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
REFERENCES
- 1. Bedoya MM, Park JH. A review of the diagnosis and management of impacted maxillary canines. J Am Dent Assoc. 2009;140(12):1485‐1493. doi: 10.14219/jada.archive.2009.0099 [DOI] [PubMed] [Google Scholar]
- 2. Dalessandri D, Parrini S, Rubiano R, Gallone D, Migliorati M. Impacted and transmigrant mandibular canines incidence, aetiology, and treatment: a systematic review. Eur J Orthod. 2017;39(2):161‐169. doi: 10.1093/ejo/cjw027 [DOI] [PubMed] [Google Scholar]
- 3. Liu DG, Zhang WL, Zhang ZY, Wu YT, Ma XC. Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone‐beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(1):91‐98. doi: 10.1016/j.tripleo.2007.01.030 [DOI] [PubMed] [Google Scholar]
- 4. Motamedi MH, Tabatabaie FA, Navi F, Shafeie HA, Fard BK, Hayati Z. Assessment of radiographic factors affecting surgical exposure and orthodontic alignment of impacted canines of the palate: a 15‐year retrospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(6):772‐775. doi: 10.1016/j.tripleo.2008.12.022 [DOI] [PubMed] [Google Scholar]
- 5. Arriola‐Guillén LE, Aliaga‐Del Castillo A, Ruíz‐Mora GA, Rodríguez‐Cárdenas YA, Dias‐Da Silveira HL. Influence of maxillary canine impaction characteristics and factors associated with orthodontic treatment on the duration of active orthodontic traction. Am J Orthod Dentofacial Orthop. 2019;156(3):391‐400. doi: 10.1016/j.ajodo.2018.10.018 [DOI] [PubMed] [Google Scholar]
- 6. Alqerban A, Jacobs R, Fieuws S, Willems G. Predictors of root resorption associated with maxillary canine impaction in panoramic images. Eur J Orthod. 2016;38(3):292‐299. doi: 10.1093/ejo/cjv047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lempesi E, Karamolegkou M, Pandis N, Mavragani M. Maxillary canine impaction in orthodontic patients with and without agenesis: a cross‐sectional radiographic study. Angle Orthod. 2014;84(1):11‐17. doi: 10.2319/022413-155.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Chapokas AR, Almas K, Schincaglia GP. The impacted maxillary canine: a proposed classification for surgical exposure. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(2):222‐228. doi: 10.1016/j.tripleo.2011.02.025 [DOI] [PubMed] [Google Scholar]
- 9. Cassina C, Papageorgiou SN, Eliades T. Open versus closed surgical exposure for permanent impacted canines: a systematic review and meta‐analyses. Eur J Orthod. 2018;40(1):1‐10. doi: 10.1093/ejo/cjx047 [DOI] [PubMed] [Google Scholar]
- 10. Hirschhaut M, Leon N, Gross H, Flores‐Mir C. Guidance for the clinical management of impacted maxillary canines. Compend Contin Educ Dent. 2021;42(5):220‐228. [PubMed] [Google Scholar]
- 11. Fournier A, Turcotte JY, Bernard C. Orthodontic considerations in the treatment of maxillary impacted canines. Am J Orthod. 1982;81(3):236‐239. doi: 10.1016/0002-9416(82)90056-2 [DOI] [PubMed] [Google Scholar]
- 12. Mathews DP. Surgical and orthodontic management of the ectopic, labially impacted, maxillary canines: a case series. Int J Periodontics Restorative Dent. 2022;42(6):713‐720. doi: 10.11607/prd.6255 [DOI] [PubMed] [Google Scholar]
- 13. Grisar K, Luyten J, Preda F, et al. Interventions for impacted maxillary canines: a systematic review of the relationship between initial canine position and treatment outcome. Orthod Craniofac Res. 2021;24(2):180‐193. doi: 10.1111/ocr.12423 [DOI] [PubMed] [Google Scholar]
- 14. Arriola‐Guillén LE, Ruíz‐Mora GA, Rodríguez‐Cárdenas YA, Aliaga‐Del Castillo A, Dias‐Da Silveira HL. Root resorption of maxillary incisors after traction of unilateral vs bilateral impacted canines with reinforced anchorage. Am J Orthod Dentofacial Orthop. 2018;154(5):645‐656. doi: 10.1016/j.ajodo.2018.01.015 [DOI] [PubMed] [Google Scholar]
- 15. Nabbout F, Skaf Z, Hlayhel J. Maxillary tooth transposition: a report of two cases. Int Orthod. 2017;15(3):467‐482. doi: 10.1016/j.ortho.2017.06.023 [DOI] [PubMed] [Google Scholar]
- 16. Sabri R, Zaher A, Kassem H. Tooth transposition: a review and clinical considerations for treatment. World J Orthod. 2008;9(4):303‐318. [PubMed] [Google Scholar]
- 17. Sampaio CS, Tonolli G, Marin G, Atria PJ. Multidisciplinary clinical approach of an orthodontic treatment and complete digital rehabilitation of laminate veneers for esthetically compromised worn teeth. Int J Comput Dent. 2021;24(2):181‐194. [PubMed] [Google Scholar]
- 18. Korkmaz YN, Yagci F. Multidisciplinary treatment of severe upper incisor root resorption secondary to transposed canine. J Esthet Restor Dent. 2017;29(1):5‐12. doi: 10.1111/jerd.12237 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.