

Abstract
Objective
To explore the associations between childhood trauma, alexithymia, rumination, and non-suicidal self-injury (NSSI) among adolescents and to provide theoretical and empirical evidence for effective prevention, identification, and intervention of NSSI in the future.
Methods
Questionnaires, including the Childhood Trauma Questionnaire, the twenty-item Toronto Alexithymia scale, the Ruminative Responses Scale, and the Adolescents Self-Harm Scale, were given to 1,270 Chinese teenagers. The mediating role was simulated utilizing Amos 24.0.
Results
The Pearson’s product-difference correlation analyses indicated the two-by-two significant correlations between childhood trauma, alexithymia, rumination, and NSSI. The structural equation modeling suggests that alexithymia and rumination partially mediate between childhood trauma and NSSI in teenagers, respectively. Additionally, it reveals that alexithymia and rumination chain mediate between childhood trauma and NSSI.
Conclusion
The study confirms the impact of childhood trauma on adolescents’ NSSI and also highlights the mediating role of alexithymia and rumination between the two. This study enriches the findings of NSSI and provides a theoretical basis for preventing and intervening in dysfunctional behaviors among adolescents.
Keywords: Childhood trauma, Alexithymia, Rumination, Non-suicidal self-injury
INTRODUCTION
Non-suicidal self-injury (NSSI) is the intentional, direct damage to one’s own body that is done without the intention of killing oneself. Skin-cutting, burning, biting, and scratching are common behaviors associated with this disorder [1]. NSSI is common in mood disorders, anxiety disorders, and post-traumatic stress disorder and is a valid predictor of the development of psychiatric disorders [2,3]. Additionally, NSSI is a risk factor for suicidal ideation and behavior [4], and reaching a threshold NSSI frequency (20 episodes) increases the risk of later suicide attempts [5]. NSSI peaks in adolescence, around 15–17, and resolves in middle and young adulthood [6]. Worldwide, 22.1% of teenagers experience NSSI at some point in their lives, and 19.5% have done so within the last 12 months [7], which has become a severe and dangerous public mental health problem. Therefore, there is an urgent need to further explore the risk factors of NSSI for early identification of at-risk populations and timely preventive measures.
Childhood is a critical period of physical and mental development, and childhood trauma is a vital exposure factor for future psychiatric disorders in adolescence or adulthood [8]. Numerous studies have confirmed that childhood trauma can not only directly affect NSSI but also indirectly through certain mediating factors (e.g., social support, experiential avoidance, parent-child conflict, pathological personality disorders, emotional dysregulation, etc.) [9]. However, to date, no study has investigated the association between rumination and NSSI in the context of child maltreatment, and no study has yet synthesized and systematically examined the mediating role of emotional factors (alexithymia) and cognitive factors (rumination) in the relationship between childhood trauma and NSSI. The study relies on Nock’s [10] comprehensive theoretical model, which explains the development and maintenance of self-injury, as a crucial theoretical framework. The model emphasizes that certain risk factors occurring early in life (e.g., childhood maltreatment and a genetic predisposition to high emotional reactivity) lead to proximal vulnerabilities (e.g., internal or interpersonal vulnerabilities), which make individuals more prone to reacting to challenges or stresses in emotionally or socially dysfunctional ways, i.e., greater use of NSSI or some other extreme behaviors to regulate their emotional or social experiences. The current study focuses on the path from childhood trauma (considered as a distant risk factor) to NSSI, as well as the underlying processes of alexithymia and rumination (considered as proximal vulnerability factors) that support this pathway.
Childhood trauma refers to abusive and traumatic experiences suffered before the age of 16. It includes five distinct forms of mistreatment: emotional abuse (EA), physical abuse (PA), sexual abuse (SA), emotional neglect (EN), and physical neglect (PN) [11]. Childhood trauma, specifically abuse and neglect, is prevalent among both clinical and community populations [12]. Multiple retrospective investigations conducted within the community have consistently documented and reproduced the robust correlation between childhood trauma and self-injury [13], and childhood trauma has been recognized as a potential cause of NSSI (for a review [14]). van der Kolk [15] noted that children who have been abused frequently engage in self-destructive behaviors. These children resort to engaging in NSSI as a means to counteract the heightened arousal caused by trauma and to activate their internal opioid system. Finkelhor and Browne [16] argued that children who have experienced abuse perceive themselves as having been harmed and as being distinct from others. Consequently, they harbor anger towards their bodies and engage in NSSI to inflict punishment and harm against themselves. Yates [17] utilized the organizational model of psychopathology to examine the relationship between child abuse and self-injury. According to Yates [17], self-injury arises as a compensatory strategy for adapting to relationships and regulation when normal developmental pathways are hindered by trauma or maltreatment. NSSI is commonly understood as a dysfunctional strategy for dealing with post-traumatic stress disorder [18].
Emotion regulation is a concept that has been prominent in prior research on NSSI, and theoretical and empirical work has identified NSSI as a result of maladaptive emotion regulation. Emotion regulation is the process by which individuals exert influence over the occurrence, experience, and expression of emotions [19]. Effective emotion regulation involves 1) awareness and understanding of emotions, 2) acceptance of emotions, 3) the ability to engage in goal-directed behaviors and restrain impulses when in a negative emotion, and 4) flexibility in the use of contextually appropriate emotion regulation strategies [20]. Lack of any of these abilities implies emotional dysregulation [20]. Emotional dysregulation may be rooted in an inability to consciously experience and be aware of emotions and a lack of emotional acceptance. Based on Gross’s model of the emotion regulation process [21], Preece et al. [22] suggest that a range of difficulties in the attention and appraisal phases of the emotion regulation process can be captured through the structure of alexithymia.
Alexithymia, alternatively referred to as “affective expression disorder” or “affective dysphoria,” is a cognitive and affective condition caused by an individual’s inability to identify, process, and regulate emotions correctly. This illness presents itself through three primary domains of obstacle: difficulty in identifying feelings (DIF), difficulty in describing feelings (DDF), and externally oriented thinking (EOT) [23,24]. Alexithymia may serve as an intermediary in the relationship between childhood trauma and NSSI. Firstly, effective emotion regulation encompasses several key components: the ability to perceive a wide range of emotions to obtain relevant and directed information, the skill to manage the intensity of emotions without becoming overwhelmed or shut down, and the aptitude to express emotions and needs effectively to receive interpersonal support [25,26]. For children to learn to manage their emotions and get support from others, it is essential to monitor and respond externally to children’s feelings and needs and to instruct them on how to express their feelings and needs appropriately [27,28]. Abusive and neglectful environments can lead to strong negative emotions in children, while these emotions and related needs are often disregarded, dismissed, or violated. As a result, children who have been subjected to abuse frequently struggle to verbalize specific and varied feelings [29]. Findings suggest that various subtypes of childhood maltreatment, notably EA, EN, and PN, are strongly associated with alexithymia [30,31]. Evidence suggests that EN in childhood is particularly associated with dysregulated or impaired emotion regulation and cognitive decline. For example, Gould et al. [32] examined patterns of neuropsychological functioning associated with child maltreatment. They found that significant deficits in emotional processing and processing speed were associated with child neglect. Secondly, deficits in emotion regulation are a central process in NSSI [33]. Based on the cognitive-emotional model, individuals who have difficulties in perceiving, understanding, and accepting emotions or who fail to adopt appropriate emotion management strategies are at risk of triggering negative emotional experiences and behavioral problems such as self-injury and suicide [20,34]. A comprehensive analysis of the correlation between alexithymia and NSSI demonstrated a strong association between the two in both clinical and non-clinical groups [35]. Alexithymia was confirmed to function as a mediator in the connection between child abuse and NSSI in two separate studies. A study indicates that alexithymia serves as a mediator between child maltreatment and NSSI, although this association does not extend to SA [36]. Another study showed that alexithymia had a notable impact on diminishing the direct influences of PA and PN on NSSI [37]. These findings may be indicative of the fact that various forms of child abuse have distinct impacts on psychological and cognitive development, but further study is needed to confirm this. This study posits hypothesis 1: alexithymia serves as a mediator between childhood trauma and NSSI.
Rumination refers to an individual’s repetitive, negative thinking style, which focuses on negative emotions, their causes, and possible consequences after experiencing an adverse life event rather than actively taking action to improve their situation or solve their problems [38]. Rumination could potentially function as a mediator in the connection between childhood trauma and NSSI. In the first place, childhood abuse can potentially serve as a developmental antecedent to rumination [39,40]. Adverse childhood experiences inhibit people from embracing their emotions, ideas, and experiences without judgment as well as accepting new experiences [41,42]; traumatic experiences are repeated over and over in mind, resulting in rumination [43]. The findings of a comprehensive study, encompassing both qualitative and quantitative methods, indicate a clear and positive association between childhood trauma and rumination. Abused individuals often struggle to disentangle themselves from the lasting effects of their traumatic experiences, leading to a repetitive cycle of reliving these [44]. In other, retrospective investigations have demonstrated that rumination exacerbates psychopathology by exacerbating the intensity and prolonging the duration of negative emotions, impeding problem-solving and purposeful behavior, and decreasing the sensitivity to cope with unexpected situations [45]. A systematic review revealed a direct association between rumination and a prior history of NSSI. Furthermore, people exhibiting elevated levels of rumination had a greater propensity to partake in NSSI, engage in such behavior more often, and use a more comprehensive array of self-injury techniques [46,47]. NSSI may have succeeded in distracting from rumination [48]. Research has demonstrated that rumination functions as a significant mediator in the relationship between childhood trauma and depression/anxiety [43]. The associations between suicidal thoughts and traumatic experiences in childhood are also mediated by rumination [49]. This study posits hypothesis 2: rumination serves as a mediator between childhood trauma and NSSI.
Emotional competence is one of the critical mechanisms explaining the relationship between trauma and children’s impairment [50]. An effective strategy for managing emotions involves identifying feelings (emotional clarity) and handling and bouncing back from negative emotions [20]. It is difficult for individuals with poor emotional clarity to regulate negative emotions effectively [51]. As a result, individuals with alexithymia may feel powerless to change their situation and experience overwhelming and confusing emotional messages [52]. Based on the Emotional Cascade Theory [48], powerful negative feelings trigger a process of rumination. This rumination further amplifies the initial negative emotion, resulting in a vicious loop leading to progressively severe emotional cascades. This process may set off behaviors like NSSI because such actions provide strong physical sensations that divert attention from ruminating and obstruct the emotional chain reaction. After engaging in NSSI, people experience a decrease in negative emotions [53]. It is a negative reinforcing effect, and people are likelier to continue NSSI for emotional regulation [48]. This study posits hypothesis 3: alexithymia and rumination serially mediate the relationship between childhood trauma and NSSI.
In summary, the purpose of this study was to examine the impact of childhood trauma on adolescents’ NSSI and to test the mediating properties of alexithymia and rumination in this relationship (see Figure 1 for the theoretical model). The study sought to reveal how childhood trauma affects adolescents’ NSSI through cognitive and emotional factors to provide a theoretical and empirical basis for the early identification and assessment of adolescents’ NSSI.
Figure 1.
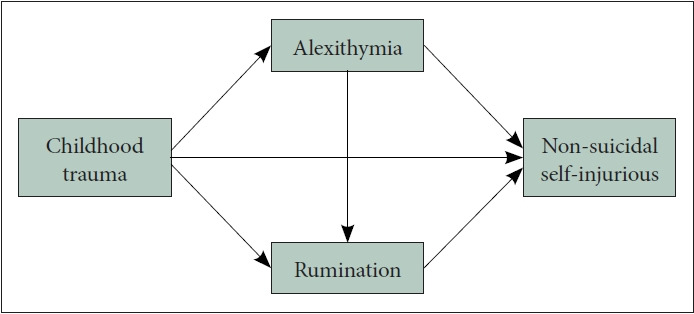
Theoretical model.
METHODS
Participants
Five regular and vocational high schools in Yantai City, Shandong Province, were chosen for the study. 1,500 questionnaires were distributed using a whole cluster sampling method and classroom-based. Before administering the test, the researcher informed the students and their custodians about the study’s primary goal, content, and related confidentiality principles and obtained informed consent from them. The questionnaires were collected uniformly at the end of the administration. Inclusion criteria for valid questionnaires: 1) 15–17 years old, 2) students enrolled in school; and exclusion criteria: survey items not fully completed. A total of 1,270 (84.67%) valid questionnaires were obtained in this study. The sample comprised 527 (41.50%) males and 743 (58.50%) females. In terms of grade level, 485 (38.19%) were first-year high school students, 512 (40.31%) were second-year high school students, and 273 (21.50%) were third-year high school students. Additionally, 669 (52.68%) were enrolled in general high school programs, while 601 (47.32%) were in vocational high school programs. The participants comprised an average age of 15.92±0.78 years. We use the Monte Carlo simulation [54] for the power analysis, in which the total number of power analysis replications is set to 5,000, the number of coefficient draws per replication is set to 20,000, the random seed is set to 1,234, and the confidence level is set to 95%. In this study, the power for mediation models ranges from 0.92 to 0.99, i.e., the sample size meets the requirement.
Measures
Childhood Trauma Questionnaire
The Childhood Trauma Questionnaire (CTQ), initially created by Bernstein et al. [55] and later refined by Zhao et al. [56], was utilized. Questions on the scale included “I feel loved by my family” and so on. The scale contains 28 entries covering five clinical subscales of EA, PA, SA, EN, and PN, each containing 5 entries and an additional 3 entries for validity assessment. Each entry is evaluated using a 5-point scale (1, never; 2, occasionally; 3, sometimes; 4, often; and 5, always). The subscale score is calculated by summing all the items inside the subscale. The overall scale score is calculated by adding up the values of the five subscales. Higher scores on the scale indicate more severe childhood trauma. Within this research investigation, the Cronbach’s alpha coefficient for the overall scale was 0.90, and the Cronbach’s alpha coefficients for the five subscales were 0.87, 0.83, 0.63, 0.88, and 0.75, respectively. Confirmatory factor analysis revealed that the factor loadings for all items ranged from 0.43 to 0.87, with fit indices of χ2/df=2.94, root mean square error of approximation (RMSEA)=0.04, goodness of fit index (GFI)=0.95, normed fit index (NFI)=0.94, relative fit index (RFI)=0.93, incremental fit index (IFI)=0.95, and comparative fit index (CFI)=0.96.
The twenty-item Toronto Alexithymia scale
The twenty-item Toronto Alexithymia scale (TAS-20), initially established by Bagby et al. [24] and subsequently refined by Yi et al. [57], was employed. Questions on the scale included “I find it difficult to describe my feelings in appropriate terms” and so on. The scale contains 20 entries covering three factors: DIF, DDF, and EOT, each containing 7, 5, and 8 entries, respectively. Each entry was evaluated using a 5-point scale (1, strongly disagree; 2, disagree; 3, neither agree nor disagree; 4, agree; and 5, strongly agree). The factor score was calculated by summing all the entries within each factor, and the scale’s total score was obtained by summing the three-factor scores. Stronger scores correlated with increased levels of alexithymia. Within this research investigation, the Cronbach’s alpha coefficient for the total scale was 0.94, and the Cronbach’s alpha coefficients for the three factors were 0.94, 0.89, and 0.93, respectively. Confirmatory factor analysis revealed that the factor loadings for all items ranging from 0.76 to 0.86 with fit indices of χ2/df=2.79, RMSEA=0.04, GFI=0.96, NFI=0.97, RFI=0.97, IFI=0.98, and CFI=0.98.
Ruminative Responses Scale
The Ruminative Responses Scale (RRS), initially formulated by Nolen-Hoeksema [38] and subsequently modified by Han and Yang [58], was utilized. Questions on the scale include “I often wonder why I am always like this,” and so on. The scale contains 22 entries covering three factors: symptom rumination, reflective pondering, and brooding, each containing 12, 5, and 5 entries, respectively. The evaluation for each entry was established utilizing a 4-point scale (1, never; 2, sometimes; 3, often; and 4, always). The factor score was calculated by adding all the entries within each factor, and the overall score of the scale was calculated by adding the scores of the three factors. A greater score indicates a stronger tendency towards rumination. Within this research investigation, the Cronbach’s alpha coefficient for the total scale was 0.93, while the Cronbach’s alpha coefficients for the three factors were 0.93, 0.84, and 0.83, respectively. Confirmatory factor analysis showed that the factor loadings for all items ranged from 0.61 to 0.76, with the fit indices of χ2/df= 4.75, RMSEA=0.05, GFI=0.95, NFI=0.93, RFI=0.92, IFI=0.95, and CFI=0.95.
Adolescents Self-Harm Scale
The Adolescents Self-Harm Scale (ASHS), initially developed by Zheng [59] and then improved by Feng [60], was utilized. Questions on the scale included “I purposely scratched my skin to bleed,” among others. The questionnaire comprises 18 items, each comprising two components: an evaluation of the frequency of NSSI and the extent of physical harm inflicted. The frequency of NSSI was assessed using a 4-point scale (0, none; 1, one time; 2, two to four times; and 3, five or more times), and the degree of bodily harm was evaluated using a 5-point scale (0, none; 1, mild; 2, moderate; 3, severe; and 4, very severe). The score for each entry was determined by multiplying the frequency of NSSI by the degree of somatic damage. The scores for all 18 entries were then added together to obtain a total scale score. A larger scale score indicates a greater severity of the child’s NSSI. The Cronbach’s alpha coefficient for the scale in this study was 0.73. Confirmatory factor analysis revealed fit indices of χ2/df=2.53, RMSEA=0.04, GFI=0.97, NFI=0.85, RFI=0.83, IFI=0.90, and CFI=0.90.
Ethics statement
The study was performed according to the ethical standards in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Following China’s circular on the issuance of measures for ethical review of life science and medical research involving human beings, informed consent was obtained from each subject and his/her parents and/or guardians for this study. Entrusted by Yantai Vocational College of Culture and Tourism, the medical ethics committee of Yantai Affiliated Hospital of Binzhou Medical University reviewed and approved this study (application number: 20230915070).
Statistical analyses
The database was created using SPSS 23.0 software (IBM Corp., Armonk, NY, USA). A descriptive analysis was conducted, followed by an independent samples t-test to compare the means of the data. Harman’s single-factor test was employed to assess the presence of homogeneity bias in the data. Additionally, Pearson product-moment correlation analysis was utilized to examine the correlation between the variables. The structural equation modeling (SEM) was performed using AMOS 24.0 software (IBM Corp., Armonk, NY, USA). The mediation effects test utilized bias-corrected nonparametric percentile bootstrap estimation with 5,000 random sample repetitions. The 95% confidence interval does not contain 0, indicating that the mediating effect is significant.
RESULTS
Common method bias
Harman’s single-factor test yielded 19 factors with eigenvalues exceeding one through unrotated principal component factor analysis. The first factor contributed 17.45% to the cumulative variance, falling below the recommended critical criterion of 40%. As a result, this study can confidently dismiss any significant homoscedasticity bias issues.
The basics of childhood trauma and NSSI
As per the literature, 56 the minimum values required for the five subscales are as follows: EA ≥13, PA ≥10, SA ≥8, EN ≥15, and PN ≥10. Individuals who met any of the above have concomitant childhood trauma. In this study, a sample of 1,270 individuals was examined. Among them, 48.50% (616) reported no childhood trauma, 17.32% (220) reported experiencing EA, 24.65% (313) suffered PA, 10.79% (137) experienced SA, 24.25% (308) experienced EN, and 31.89% (405) experienced PN.
In this study, 58.43% (742) of participants reported not engaging in NSSI, while 41.57% (528) reported committing at least one or more self-injurious behaviors. There was no significant difference in NSSI between males (4.20±7.70) and females (4.29±7.79), t (1268)=-2.03, p=0.839. NSSI was substantially higher in the group that experienced childhood trauma (5.87±9.09) compared to the group that did not (2.53±5.51), t (1268)=-7.97, p<0.001.
Descriptive statistics and correlation analysis
Pearson’s product-difference correlation analyses (Table 1) revealed that childhood trauma had a positive correlation with alexithymia and its dimensions (r ranging from 0.28 to 0.36, all p<0.01), with rumination and its dimensions (r ranging from 0.24 to 0.37, all p<0.01, and with NSSI (r=0.27, p<0.01). Alexithymia had a positive correlation with rumination and its dimensions (r ranging from 0.25 to 0.34, all p<0.01) and also showed a positive correlation with NSSI (r=0.21, p<0.01). A positive correlation (r=0.23, p<0.01) was observed between rumination and NSSI.
Table 1.
Descriptive statistics and correlation analysis for variables and dimensions (r, N=1,270)
| M±SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Emotional abuse | 8.21±4.23 | 1 | ||||||||||||||
| 2. Physical abuse | 7.52±3.38 | 0.45** | 1 | |||||||||||||
| 3. Sexual abuse | 5.77±1.77 | 0.29** | 0.35** | 1 | ||||||||||||
| 4. Emotional neglect | 10.11±5.61 | 0.41** | 0.42** | 0.27** | 1 | |||||||||||
| 5. Physical neglect | 8.23±3.86 | 0.42** | 0.46** | 0.32** | 0.52** | 1 | ||||||||||
| 6. Childhood trauma | 39.84±13.92 | 0.73** | 0.72** | 0.50** | 0.81** | 0.77** | 1 | |||||||||
| 7. Difficulty in identifying feelings | 17.29±7.63 | 0.23** | 0.26** | 0.01 | 0.28** | 0.19** | 0.30** | 1 | ||||||||
| 8. Difficulty in describing feelings | 13.22±5.26 | 0.22** | 0.24** | 0.03 | 0.25** | 0.19** | 0.28** | 0.58** | 1 | |||||||
| 9. Externally oriented thinking | 19.87±7.93 | 0.22** | 0.25** | -0.003 | 0.24** | 0.20** | 0.28** | 0.42** | 0.44** | 1 | ||||||
| 10. Alexithymia | 50.38±16.82 | 0.27** | 0.31** | 0.01 | 0.32** | 0.24** | 0.36** | 0.84** | 0.78** | 0.80** | 1 | |||||
| 11. Symptom rumination | 24.05±8.86 | 0.26** | 0.24** | 0.21** | 0.27** | 0.27** | 0.35** | 0.27** | 0.24** | 0.26** | 0.32** | 1 | ||||
| 12. Reflective pondering | 9.75±3.81 | 0.18** | 0.20** | 0.18** | 0.15** | 0.19** | 0.24** | 0.22** | 0.18** | 0.19** | 0.25** | 0.53** | 1 | |||
| 13. Brooding | 10.78±3.95 | 0.23** | 0.17** | 0.14** | 0.21** | 0.24** | 0.28** | 0.22** | 0.20** | 0.20** | 0.26** | 0.48** | 0.49** | 1 | ||
| 14. Rumination | 44.58±13.87 | 0.28** | 0.26** | 0.23** | 0.27** | 0.30** | 0.37** | 0.29** | 0.26** | 0.27** | 0.34** | 0.92** | 0.75** | 0.73** | 1 | |
| 15. NSSI | 4.25±7.75 | 0.25** | 0.27** | -0.02 | 0.21** | 0.18** | 0.27** | 0.28** | 0.20** | 0.04 | 0.21** | 0.20** | 0.19** | 0.17** | 0.23** | 1 |
p<0.01.
M, mean; SD, standard deviation; NSSI, non-suicidal self-injury
Chain-mediated effects of alexithymia, rumination
The SEM was constructed using the statistical software AMOS 24.0 to investigate the relationship between the four variables of childhood trauma, alexithymia, rumination, and NSSI. The item-packing approach was employed in the statistical analysis procedure. The model fit indicators, including χ2/df=4.89, RMSEA=0.06, GFI=0.97, NFI=0.93, RFI=0.91, IFI=0.94, and CFI=0.94, satisfy the criteria for acceptable values of fit indicators. It suggests that the model and data fit are within acceptable limits.
The model showing the relationship between the variables is displayed in Figure 2, and every path coefficient (all p<0.01) is significant. Not only did childhood trauma predict NSSI directly, but it also did so indirectly through rumination and alexithymia, respectively; additionally, the chain-mediated effects of rumination and alexithymia predicted NSSI indirectly.
Figure 2.

Chain-mediated model of alexithymia and rumination between childhood trauma and NSSI. **p<0.01; ***p<0.001. NSSI, non-suicidal self-injury.
The mediation effect was tested using the bootstrap method, which involved conducting 5,000 sampling iterations. The study showed that in the three pathways of childhood trauma → alexithymia → NSSI, childhood trauma → rumination → NSSI, and childhood trauma → alexithymia → rumination → NSSI, none of the 95% confidence intervals of the mediation effect values contained the value of 0. This indicates that the mediation effect was statistically significant in all three pathways. In addition, the 95% confidence interval for the direct impact of childhood trauma on NSSI did not include the value of 0, indicating a significant direct effect. Alexithymia and rumination were identified as partial mediators in the association between childhood trauma and NSSI, respectively. The effect value of alexithymia was measured to be 0.07, contributing approximately 20.00% of the total effect. The effect value of rumination was measured to be 0.04, contributing to 11.43% of the total effect. Furthermore, the association was mediated by the combination of alexithymia and rumination, with an effect value of 0.02, explaining 5.71% of the total effect (see Table 2 for more information).
Table 2.
Mediating effects of alexithymia, rumination on the association between childhood trauma and NSSI
| Effect | Path | Standardized parameter estimates | SE | Bias-corrected 95% CI | Percentage of effect |
|---|---|---|---|---|---|
| Direct | Childhood trauma→NSSI | 0.22 | 0.05 | 0.13–0.32 | 62.86 |
| Indirect | Childhood trauma→alexithymia→NSSI | 0.07 | 0.02 | 0.04–0.11 | 20.00 |
| Childhood trauma→rumination→NSSI | 0.04 | 0.02 | 0.01–0.08 | 11.43 | |
| Childhood trauma→alexithymia→rumination→NSSI | 0.02 | 0.01 | 0.00–0.03 | 5.71 | |
| Total indirect | - | 0.13 | 0.03 | 0.09–0.18 | 37.14 |
| Total | - | 0.35 | 0.04 | 0.27–0.43 | 100.00 |
NSSI, non-suicidal self-injury; SE, standard error; CI, confidence interval
DISCUSSION
The study found that the prevalence of PN was the highest among the group of adolescents surveyed, followed by PA, EN, EA, and SA. These findings align with earlier studies [12]. Contrary to previous research [14], there was no significant difference between males and females regarding NSSI. This lack of difference may be attributed to variations in how NSSI was measured. In our study, we assessed the extent of NSSI by considering both the frequency of self-injury and the severity of bodily harm. The sample that had undergone childhood trauma had elevated levels of NSSI in comparison to the ones that did not suffer childhood trauma, aligns with prior research. 37 This indicates that a heightened propensity for NSSI later in life is associated with childhood trauma.
The two-by-two significant correlations between childhood trauma, alexithymia, rumination, and NSSI are aligned with previous studies [61,62], and the results of the correlation analyses tentatively support subsequent tests of mediating effects. The conclusion that SA and NSSI do not correlate significantly aligns with the findings of a meta-analysis on the topic [63]. SA is unlikely to impact the development or continuation of NSSI significantly. This could be attributed to the fact that children who have experienced SA often encounter additional obstacles when it comes to reporting their experiences [64]. SA was not associated with alexithymia or any of its dimensions. The findings of this investigation align with one previous study [36], but contradict the majority of other studies [65,66]. The present study does not currently offer an explanation for this inconsistency. The absence of a correlation between EOT and NSSI indicates that the connection between alexithymia and NSSI is primarily influenced by DIF and DDF. When individuals are incapable of identifying (DIF) and describing (DDF) their feelings, NSSI may manifest as dysfunctional tactics and maladaptive attempts to handle or manage feelings of negativity. In contrast, EOT individuals are inclined to regulate emotions by indirectly damaging the body (e.g., alcohol consumption) rather than by directly damaging the body (e.g., NSSI) [67,68].
Childhood trauma directly predicts NSSI in adolescents. Childhood trauma is believed to be the origin of various psychopathologies [69,70]. Reports indicate that trauma, particularly trauma experienced during childhood, can significantly influence an individual’s self-sense in a manner that is both self-destructive and re-traumatizing [15]. In other words, these people will attach themselves to the traumatic experience and reproduce it through self-injurious behaviors such as violence against their bodies. The function of NSSI in reducing physiologic arousal and re-experiencing symptoms has been well-studied [71]. Studies of ecological transient assessments of affective experiences before and after NSSI have shown that negative affect increases before NSSI, peaks during participation, and fades [72]. To summarize, there is increasing data indicating that NSSI has a significant role in mitigating the immediate negative consequences of childhood trauma [73].
Through the mediating effect of alexithymia, childhood trauma also impacts the risk of NSSI in adolescents. Studies in biological sciences indicate that childhood maltreatment may decrease the size of the hippocampus, a brain region responsible for emotional processing. This reduction in hippocampal volume is thought to play a role in the development of alexithymia in persons who have experienced abuse during childhood [74] Similarly, Yates [75], based on Kohut’s [76] psychodynamic theory, states that trauma in the early parenting environment either leads to the development of impaired tension-regulating mechanisms or strong emotional tendencies in children. Individuals with alexithymia significantly increase the likelihood of NSSI due to their diminished sensitivity to emotional stimuli and inability to regulate their emotions [67]. Additionally, abuse impedes children’s ability to verbally communicate their feels, compelling them to employ non-verbal coping mechanisms as a means of processing the trauma [77]. The inability to recognize or name emotions, as well as experiencing feelings of being overwhelmed, may lead abused children to express emotions physically [77]. NSSI may be a compensatory nonverbal strategy for disrupting feelings of psychological numbness and/or avoiding and managing strong, seemingly uncontrollable emotions [17].
Childhood trauma can also indirectly influence adolescents’ NSSI through the mediating role of rumination. Trauma theory, incompleteness theory, and secrecy theory related to rumination all emphasize traumatic events as the driving force behind rumination [44]. Childhood trauma, especially trauma that has not been adequately discussed and catharticized, is closely related to rumination [78]. Childhood trauma leads to the deterioration of an individual’s cognitive structure, which in turn triggers a rumination process that facilitates the reprocessing of the traumatic experience [44]. Individuals who ruminate are preoccupied with their internal states (e.g., over-indulging in recurrent thoughts about negative childhood experiences and negative emotions) rather than taking positive action to solve problems or employing distraction to cope with stressors [38]. Rumination repeatedly directs attention to negative emotions, creating a cycle or cascade of negative emotions and further rumination [79]. In order to escape the intense emotions (emotional cascades) that arise from the rumination cycle, individuals may need more extreme forms of distraction (e.g., NSSI) in order to divert attention away from intrusive rumination and overwhelming emotions [79].
Indirectly, via the chain-mediated effects of alexithymia and rumination, childhood trauma influences adolescents’ NSSI. Previous research has shown that alexithymia and rumination are typical factors of NSSI [62]. Individuals with alexithymia may engage in more repetitive and analytical thinking about external affective goals due to significant deficits in identifying and describing internal emotional states and relatively little information available to guide behavior in an emotional context [80]. In addition, people with alexithymia have difficulty facing trauma and integrating emotions associated with traumatic events because they cannot identify and describe emotions. When individuals can no longer pursue important goals, they can only chew on the goal event again in their minds, i.e., by regurgitating to reduce the gap between the status quo and the goal [81].
Research significance, limitations, and future directions
The current research elucidated the trajectory from childhood trauma, a distant risk factor, to NSSI and the potential mechanisms of alexithymia and rumination, which were proximal risk factors that underlie this trajectory. The construction of the chain mediation model was crucial for deepening and expanding the understanding of the connection between childhood trauma and individuals’ disordered behaviors. Moreover, the study extends the integrated theoretical model of the development and maintenance of self-injury and provides empirical data to support the early identification and intervention of NSSI. There is no doubt that childhood trauma is an early risk factor for NSSI, and focused screening of this population is needed. In addition, assessing an individual’s level of alexithymia and rumination can help in the early identification and intervention of NSSI among adolescents. Interventions based on mindfulness have been shown to help increase emotional clarity and internal sense awareness and help reduce rumination [82-84]. Mindfulness training may be an effective method to improve NSSI in adolescents.
There are certain constraints associated with this study. Initially, the assessment of childhood trauma levels was dependent on the recollections provided by adolescents, who may have limited ability to recall instances of maltreatment that took place during infancy or early childhood. There was a possibility that they may either downplay or exaggerate the extent of their physical and mental abuse. Furthermore, it should be noted that the samples used in this study were derived from nonclinical sources. Consequently, the implications and conclusions drawn from this research may not be applicable to the clinical context. Validation of future studies could be conducted on clinical participants. Furthermore, the chain mediation model utilized in the study was inherently cross-sectional, hence restricting the evaluation of causal linkages between variables. Prospective longitudinal data is necessary for future studies to provide causal explanations between childhood trauma, alexithymia, rumination, and NSSI.
Acknowledgments
The author thanks the generous contributions of the research participants and the staff who assisted with data collection during the study.
Footnotes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The author has no potential conflicts of interest to disclose.
Funding Statement
The study was supported by grants from the Shandong Province Social Science Foundation (23DJYJ16).
REFERENCES
- 1.Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6:339–363. doi: 10.1146/annurev.clinpsy.121208.131258. [DOI] [PubMed] [Google Scholar]
- 2.Plener PL, Kaess M, Schmahl C, Pollak S, Fegert JM, Brown RC. Non-suicidal self-injury in adolescents. Dtsch Arztebl Int. 2018;115:23–30. doi: 10.3238/arztebl.2018.0023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ghinea D, Edinger A, Parzer P, Koenig J, Resch F, Kaess M. Non-suicidal self-injury disorder as a stand-alone diagnosis in a consecutive help-seeking sample of adolescents. J Affect Disord. 2020;274:1122–1125. doi: 10.1016/j.jad.2020.06.009. [DOI] [PubMed] [Google Scholar]
- 4.Kiekens G, Hasking P, Boyes M, Claes L, Mortier P, Auerbach RP, et al. The associations between non-suicidal self-injury and first onset suicidal thoughts and behaviors. J Affect Disord. 2018;239:171–179. doi: 10.1016/j.jad.2018.06.033. [DOI] [PubMed] [Google Scholar]
- 5.Griep SK, MacKinnon DF. Does nonsuicidal self-injury predict later suicidal attempts? A review of studies. Arch Suicide Res. 2022;26:428–446. doi: 10.1080/13811118.2020.1822244. [DOI] [PubMed] [Google Scholar]
- 6.Plener PL, Schumacher TS, Munz LM, Groschwitz RC. The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Personal Disord Emot Dysregul. 2015;2:2. doi: 10.1186/s40479-014-0024-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lim KS, Wong CH, McIntyre RS, Wang J, Zhang Z, Tran BX, et al. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: a meta-analysis. Int J Environ Res Public Health. 2019;16:4581. doi: 10.3390/ijerph16224581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thumfart KM, Jawaid A, Bright K, Flachsmann M, Mansuy IM. Epigenetics of childhood trauma: long term sequelae and potential for treatment. Neurosci Biobehav Rev. 2022;132:1049–1066. doi: 10.1016/j.neubiorev.2021.10.042. [DOI] [PubMed] [Google Scholar]
- 9.Xueqian X, Zhenyu H. [A review of psychosocial mediating factors between childhood trauma and non-suicidal self-injury in adolescents] Chin Ment Health J. 2022;36:1079–1083. Chinese. [Google Scholar]
- 10.Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury. Curr Dir Psychol Sci. 2009;18:78–83. doi: 10.1111/j.1467-8721.2009.01613.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. 1994;151:1132–1136. doi: 10.1176/ajp.151.8.1132. [DOI] [PubMed] [Google Scholar]
- 12.Wang L, Cheng H, Qu Y, Zhang Y, Cui Q, Zou H. The prevalence of child maltreatment among Chinese primary and middle school students: a systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. 2020;55:1105–1119. doi: 10.1007/s00127-020-01916-7. [DOI] [PubMed] [Google Scholar]
- 13.Brown RC, Heines S, Witt A, Braehler E, Fegert JM, Harsch D, et al. The impact of child maltreatment on non-suicidal self-injury: data from a representative sample of the general population. BMC Psychiatry. 2018;18:181. doi: 10.1186/s12888-018-1754-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wang YJ, Li X, Ng CH, Xu DW, Hu S, Yuan TF. Risk factors for non-suicidal self-injury (NSSI) in adolescents: a meta-analysis. EClinicalMedicine. 2022;46:101350. doi: 10.1016/j.eclinm.2022.101350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.van der Kolk BA. The compulsion to repeat the trauma. Re-enactment, revictimization, and masochism. Psychiatr Clin North Am. 1989;12:389–411. [PubMed] [Google Scholar]
- 16.Finkelhor D, Browne A. The traumatic impact of child sexual abuse: a conceptualization. Am J Orthopsychiatry. 1985;55:530–541. doi: 10.1111/j.1939-0025.1985.tb02703.x. [DOI] [PubMed] [Google Scholar]
- 17.Yates TM. In: Understanding nonsuicidal self-injury: origins, assessment, and treatment. Nock MK, editor. Washington: American Psychological Association; 2009. Developmental pathways from child maltreatment to non-suicidal self-injury; pp. 117–137. [Google Scholar]
- 18.Smith NB, Kouros CD, Meuret AE. The role of trauma symptoms in nonsuicidal self-injury. Trauma Violence Abuse. 2014;15:41–56. doi: 10.1177/1524838013496332. [DOI] [PubMed] [Google Scholar]
- 19.Gross JJ. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol. 1998;2:271–299. [Google Scholar]
- 20.Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. 2004;26:41–54. [Google Scholar]
- 21.Gross JJ. Emotion regulation: current status and future prospects. Psychol Inq. 2015;26:1–26. [Google Scholar]
- 22.Preece D, Becerra R, Allan A, Robinson K, Dandy J. Establishing the theoretical components of alexithymia via factor analysis: introduction and validation of the attention-appraisal model of alexithymia. Pers Individ Differ. 2017;119:341–352. [Google Scholar]
- 23.Sifneos PE. The prevalence of ‘alexithymic’ characteristics in psychosomatic patients. Psychother Psychosom. 1973;22:255–262. doi: 10.1159/000286529. [DOI] [PubMed] [Google Scholar]
- 24.Bagby RM, Parker JD, Taylor GJ. The twenty-item Toronto Alexithymia scale—I. Item selection and cross-validation of the factor structure. J Psychosom Res. 1994;38:23–32. doi: 10.1016/0022-3999(94)90005-1. [DOI] [PubMed] [Google Scholar]
- 25.Frijda NH. The emotions. Cambridge: Cambridge University Press; 1986. [Google Scholar]
- 26.Gross JJ. Emotion regulation: past, present, future. Cogn Emot. 1999;13:551–573. [Google Scholar]
- 27.Gottman JM, DeClaire J. Raising an emotionally intelligent child: the heart of parenting. New York: Simon & Schuster; 1997. [Google Scholar]
- 28.Sroufe LA. Emotional development: the organization of emotional life in the early years (1st ed) Cambridge: Cambridge University Press; 1995. [Google Scholar]
- 29.van der Kolk BA, Fisler RE. Childhood abuse and neglect and loss of self-regulation. Bull Menninger Clin. 1994;58:145–168. [PubMed] [Google Scholar]
- 30.Feyzioğlu A, Taşlıoğlu Sayıner AC, Özçelik D, Tarımtay Altun F, Budak EN. The mediating role of early maladaptive schemas in the relationship between early childhood trauma and alexithymia. Curr Psychol. 2023;42:17851–17861. [Google Scholar]
- 31.Ditzer J, Wong EY, Modi RN, Behnke M, Gross JJ, Talmon A. Child maltreatment and alexithymia: a meta-analytic review. Psychol Bull. 2023;149:311–329. doi: 10.1037/bul0000391. [DOI] [PubMed] [Google Scholar]
- 32.Gould F, Clarke J, Heim C, Harvey PD, Majer M, Nemeroff CB. The effects of child abuse and neglect on cognitive functioning in adulthood. J Psychiatr Res. 2012;46:500–506. doi: 10.1016/j.jpsychires.2012.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McKenzie KC, Gross JJ. Nonsuicidal self-injury: an emotion regulation perspective. Psychopathology. 2014;47:207–219. doi: 10.1159/000358097. [DOI] [PubMed] [Google Scholar]
- 34.Hasking P, Whitlock J, Voon D, Rose A. A cognitive-emotional model of NSSI: using emotion regulation and cognitive processes to explain why people self-injure. Cogn Emot. 2017;31:1543–1556. doi: 10.1080/02699931.2016.1241219. [DOI] [PubMed] [Google Scholar]
- 35.Iskric A, Ceniti AK, Bergmans Y, McInerney S, Rizvi SJ. Alexithymia and self-harm: a review of nonsuicidal self-injury, suicidal ideation, and suicide attempts. Psychiatry Res. 2020;288:112920. doi: 10.1016/j.psychres.2020.112920. [DOI] [PubMed] [Google Scholar]
- 36.Paivio SC, McCulloch CR. Alexithymia as a mediator between childhood trauma and self-injurious behaviors. Child Abuse Negl. 2004;28:339–354. doi: 10.1016/j.chiabu.2003.11.018. [DOI] [PubMed] [Google Scholar]
- 37.Swannell S, Martin G, Page A, Hasking P, Hazell P, Taylor A, et al. Child maltreatment, subsequent non-suicidal self-injury and the mediating roles of dissociation, alexithymia and self-blame. Child Abuse Negl. 2012;36:572–584. doi: 10.1016/j.chiabu.2012.05.005. [DOI] [PubMed] [Google Scholar]
- 38.Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol. 1991;100:569–582. doi: 10.1037//0021-843x.100.4.569. [DOI] [PubMed] [Google Scholar]
- 39.Gold DB, Wegner DM. Origins of ruminative thought: trauma, incompleteness, nondisclosure, and suppression. J Appl Soc Psychol. 1995;25:1245–1261. [Google Scholar]
- 40.Nolen‐Hoeksema S. In: Depressive rumination: nature, theory and treatment. Papageorgiou C, Wells A, editors. Chichester: John Wiley & Sons; 2023. The response styles theory (1st ed) pp. 105–123. [Google Scholar]
- 41.Hansen M, Armour C, Wittmann L, Elklit A, Shevlin M. Is there a common pathway to developing ASD and PTSD symptoms? J Anxiety Disord. 2014;28:865–872. doi: 10.1016/j.janxdis.2014.09.019. [DOI] [PubMed] [Google Scholar]
- 42.Jaeger J, Lindblom KM, Parker-Guilbert K, Zoellner LA. Trauma narratives: it’s what you say, not how you say it. Psychol Trauma. 2014;6:473–481. doi: 10.1037/a0035239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kim JS, Jin MJ, Jung W, Hahn SW, Lee SH. Rumination as a mediator between childhood trauma and adulthood depression/anxiety in nonclinical participants. Front Psychol. 2017;8:1597. doi: 10.3389/fpsyg.2017.01597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Erduran Tekin Ö, Şirin A. Rumination mediates the relationship between childhood traumas with cognitive defusion, acceptance, and emotion regulation: a qualitative and quantitative study. J Rat-Emo Cognitive-Behav Ther. 2023;41:810–837. doi: 10.1007/s10942-023-00503-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Watkins ER, Roberts H. Reflecting on rumination: consequences, causes, mechanisms and treatment of rumination. Behav Res Ther. 2020;127:103573. doi: 10.1016/j.brat.2020.103573. [DOI] [PubMed] [Google Scholar]
- 46.Coleman SE, Dunlop BJ, Hartley S, Taylor PJ. The relationship between rumination and NSSI: a systematic review and meta-analysis. Br J Clin Psychol. 2022;61:405–443. doi: 10.1111/bjc.12350. [DOI] [PubMed] [Google Scholar]
- 47.Nagy LM, Shanahan ML, Seaford SP. Nonsuicidal self-injury and rumination: a meta-analysis. J Clin Psychol. 2023;79:7–27. doi: 10.1002/jclp.23394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Selby EA, Joiner TE., Jr Cascades of emotion: the emergence of borderline personality disorder from emotional and behavioral dysregulation. Rev Gen Psychol. 2009;13:219–229. doi: 10.1037/a0015687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Valderrama J, Macrynikola N, Miranda R. Early life trauma, suicide ideation, and suicide attempts: the role of rumination and impulsivity. Arch Suicide Res. 2022;26:731–747. doi: 10.1080/13811118.2020.1828208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Andersson H, Aspeqvist E, Dahlström Ö, Svedin CG, Jonsson LS, Landberg Å, et al. Emotional dysregulation and trauma symptoms mediate the relationship between childhood abuse and nonsuicidal self-injury in adolescents. Front Psychiatry. 2022;13:897081. doi: 10.3389/fpsyt.2022.897081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Vine V, Aldao A. Impaired emotional clarity and psychopathology: a transdiagnostic deficit with symptom-specific pathways through emotion regulation. J Soc Clin Psychol. 2014;33:319–342. [Google Scholar]
- 52.Foran HM, O’Leary KD. The role of relationships in understanding the alexithymia–depression link. Eur J Pers. 2013;27:470–480. [Google Scholar]
- 53.Klonsky ED. The functions of self-injury in young adults who cut themselves: clarifying the evidence for affect-regulation. Psychiatry Res. 2009;166:260–268. doi: 10.1016/j.psychres.2008.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Schoemann AM, Boulton AJ, Short SD. Determining power and sample size for simple and complex mediation models. Soc Psychol Pers Sci. 2017;8:379–386. [Google Scholar]
- 55.Bernstein DP, Ahluvalia T, Pogge D, Handelsman L. Validity of the childhood trauma questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry. 1997;36:340–348. doi: 10.1097/00004583-199703000-00012. [DOI] [PubMed] [Google Scholar]
- 56.Zhao X, Zhang Y, Li L, Zhou Y. Evaluation on reliability and validity of Chinese version of childhood trauma questionnaire. Chin J Tissue Eng Res. 2005;9:209–211. [Google Scholar]
- 57.Yi J, Yao S, Zhu X. The Chinese version of the TAS-20: reliability and validity. Chin Ment Health J. 2003;17:763–767. [Google Scholar]
- 58.Han X, Yang HF. Chinese version of Nolen-Hoeksema ruminative responses scale (RRS) used in 912 college students: reliability and validity. Chin J Clin Psychol. 2009;17:550–551. [Google Scholar]
- 59. Zheng Y. [Epidemiologic investigation of self-mutilation behavior among adolescents in Wuhan and its functional model] [dissertation]. Wuhan: Central China Normal University; 2006. Chinese. [Google Scholar]
- 60. Feng Y. [The relation of adolescents’ self-harm behaviors: individual emotion characteristics and family environment factors] [dissertation]. Wuhan: Central China Normal University; 2008. Chinese. [Google Scholar]
- 61.Serafini G, Canepa G, Adavastro G, Nebbia J, Belvederi Murri M, Erbuto D, et al. The relationship between childhood maltreatment and non-suicidal self-injury: a systematic review. Front Psychiatry. 2017;8:149. doi: 10.3389/fpsyt.2017.00149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Borrill J, Fox P, Flynn M, Roger D. Students who self-harm: coping style, rumination and alexithymia. Couns Psychol Q. 2009;22:361–372. [Google Scholar]
- 63.Klonsky ED, Moyer A. Childhood sexual abuse and non-suicidal self-injury: meta-analysis. Br J Psychiatry. 2008;192:166–170. doi: 10.1192/bjp.bp.106.030650. [DOI] [PubMed] [Google Scholar]
- 64.Alaggia R, Collin-Vézina D, Lateef R. Facilitators and barriers to child sexual abuse (CSA) disclosures: a research update (2000-2016) Trauma Violence Abuse. 2019;20:260–283. doi: 10.1177/1524838017697312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Liu H, Wang W, Yang J, Guo F, Yin Z. The effects of alexithymia, experiential avoidance, and childhood sexual abuse on non-suicidal self-injury and suicidal ideation among Chinese college students with a history of childhood sexual abuse. J Affect Disord. 2021;282:272–279. doi: 10.1016/j.jad.2020.12.181. [DOI] [PubMed] [Google Scholar]
- 66.Boisjoli C, Hébert M. Importance of telling the unutterable: alexithymia among sexually abused children. Psychiatry Res. 2020;291:113238. doi: 10.1016/j.psychres.2020.113238. [DOI] [PubMed] [Google Scholar]
- 67.Cerutti R, Zuffianò A, Spensieri V. The role of difficulty in identifying and describing feelings in non-suicidal self-injury behavior (NSSI): associations with perceived attachment quality, stressful life events, and suicidal ideation. Front Psychol. 2018;9:318. doi: 10.3389/fpsyg.2018.00318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Greene D, Boyes M, Hasking P. The associations between alexithymia and both non-suicidal self-injury and risky drinking: a systematic review and meta-analysis. J Affect Disord. 2020;260:140–166. doi: 10.1016/j.jad.2019.08.088. [DOI] [PubMed] [Google Scholar]
- 69.Hetzel MD, McCanne TR. The roles of peritraumatic dissociation, child physical abuse, and child sexual abuse in the development of posttraumatic stress disorder and adult victimization. Child Abuse Negl. 2005;29:915–930. doi: 10.1016/j.chiabu.2004.11.008. [DOI] [PubMed] [Google Scholar]
- 70.Nanni V, Uher R, Danese A. Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: a meta-analysis. Am J Psychiatry. 2012;169:141–151. doi: 10.1176/appi.ajp.2011.11020335. [DOI] [PubMed] [Google Scholar]
- 71.Franklin JC, Hessel ET, Aaron RV, Arthur MS, Heilbron N, Prinstein MJ. The functions of nonsuicidal self-injury: support for cognitive-affective regulation and opponent processes from a novel psychophysiological paradigm. J Abnorm Psychol. 2010;119:850–862. doi: 10.1037/a0020896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Rodríguez-Blanco L, Carballo JJ, Baca-García E. Use of ecological momentary assessment (EMA) in non-suicidal self-injury (NSSI): a systematic review. Psychiatry Res. 2018;263:212–219. doi: 10.1016/j.psychres.2018.02.051. [DOI] [PubMed] [Google Scholar]
- 73.Tatnell R, Hasking P, Lipp OV, Boyes M, Dawkins J. Emotional responding in NSSI: examinations of appraisals of positive and negative emotional stimuli, with and without acute stress. Cogn Emot. 2018;32:1304–1316. doi: 10.1080/02699931.2017.1411785. [DOI] [PubMed] [Google Scholar]
- 74.Teicher MH, Anderson CM, Polcari A. Childhood maltreatment is associated with reduced volume in the hippocampal subfields CA3, dentate gyrus, and subiculum. Proc Natl Acad Sci U S A. 2012;109:E563–E572. doi: 10.1073/pnas.1115396109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Yates TM. The developmental psychopathology of self-injurious behavior: compensatory regulation in posttraumatic adaptation. Clin Psychol Rev. 2004;24:35–74. doi: 10.1016/j.cpr.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 76.Kohut H. The restoration of the self. Chicago: University of Chicago Press; 1977. [Google Scholar]
- 77.van der Kolk BA, Pelcovitz D, Roth S, Mandel FS, McFarlane A, Herman JL. Dissociation, somatization, and affect dysregulation: the complexity of adaptation of trauma. Am J Psychiatry. 1996;153(7 Suppl):83–93. doi: 10.1176/ajp.153.7.83. [DOI] [PubMed] [Google Scholar]
- 78.Pennebaker JW, Susman JR. Disclosure of traumas and psychosomatic processes. Soc Sci Med. 1988;26:327–332. doi: 10.1016/0277-9536(88)90397-8. [DOI] [PubMed] [Google Scholar]
- 79.Selby EA, Anestis MD, Joiner TE. Understanding the relationship between emotional and behavioral dysregulation: emotional cascades. Behav Res Ther. 2008;46:593–611. doi: 10.1016/j.brat.2008.02.002. [DOI] [PubMed] [Google Scholar]
- 80.Di Schiena R, Luminet O, Philippot P. Adaptive and maladaptive rumination in alexithymia and their relation with depressive symptoms. Pers Individ Differ. 2011;50:10–14. [Google Scholar]
- 81.Roberts H, Watkins ER, Wills AJ. Cueing an unresolved personal goal causes persistent ruminative self-focus: an experimental evaluation of control theories of rumination. J Behav Ther Exp Psychiatry. 2013;44:449–455. doi: 10.1016/j.jbtep.2013.05.004. [DOI] [PubMed] [Google Scholar]
- 82.Cooper D, Yap K, Batalha L. Mindfulness-based interventions and their effects on emotional clarity: a systematic review and meta-analysis. J Affect Disord. 2018;235:265–276. doi: 10.1016/j.jad.2018.04.018. [DOI] [PubMed] [Google Scholar]
- 83.Mao L, Li P, Wu Y, Luo L, Hu M. The effectiveness of mindfulness-based interventions for ruminative thinking: a systematic review and meta-analysis of randomized controlled trials. J Affect Disord. 2023;321:83–95. doi: 10.1016/j.jad.2022.10.022. [DOI] [PubMed] [Google Scholar]
- 84.Silveira S, Godara M, Faschinger A, Singer T. Reducing alexithymia and increasing interoceptive awareness: a randomized controlled trial comparing mindfulness with dyadic socio-emotional app-based practice. J Affect Disord. 2023;341:162–169. doi: 10.1016/j.jad.2023.08.093. [DOI] [PubMed] [Google Scholar]