

Abstract
For assessing health‐related quality of life in patients with chronic wounds, the Wound‐QoL questionnaire has been developed. Two different versions exist: the Wound‐QoL‐17 and the Wound‐QoL‐14. For international and cross‐cultural comparisons, it is necessary to demonstrate psychometric properties in an international study. Therefore, the aim of this study was to test both questionnaires in a European sample, using item response theory (IRT). Participants were recruited in eight European countries. Item characteristic curves (ICC), item information curves (IIC) and differential item functioning (DIF) were calculated. In both questionnaires, ICCs for most items were well‐ordered and sufficiently distinct. For items, in which adjacent response categories were not sufficiently distinct, response options were merged. IICs showed that items on sleep and on pain, on worries as well as on day‐to‐day and leisure activities had considerably high informational value. In the Wound‐QoL‐14, the item on social activities showed DIFs regarding the country and age. The same applied for the Wound‐QoL‐17, in which also the item on stairs showed DIFs regarding age. Our study showed comparable results across both versions of the Wound‐QoL. We established a new scoring method, which could be applied in international research projects. For clinical practice, the original scoring can be maintained.
Keywords: chronic wounds, health‐related quality of life, IRT, item response theory, Wound‐QoL
1. INTRODUCTION
Chronic wounds are ulcers that do not heal within timely manner. Reasons for delayed healing may consist of insufficient treatment of the underlying cause (e.g., venous insufficiency) and/or impeding factors such as oedema or necrosis. 1 , 2 , 3 Around 1.67 per 1000 people are affected by chronic wounds. 4 Especially in ageing societies as the European Union, 5 chronic wounds are a rising issue due to increased prevalence in people above the age of 65 years. 6 For the individual patient, a chronic wound is a burdensome condition, which can cause physical strain, such as wound pain, odour and exudate, and psychological burden, such as sleep disturbances, anxiety and depression. 7 All of this can lead to restrictions in everyday activities 8 and social participation 9 as well as to financial impairments. 8
These impacts on physical, mental, social and everyday life aspects are covered by the well‐established multidimensional construct of health‐related quality of life (HRQoL). The evaluation of HRQoL during treatment is crucial in both clinical trials as well as in routine care. 10 Regulatory authorities have established the measurement of HRQoL as an endpoint in treatment benefit assessment. 11 In routine care, assessing HRQoL enforces incorporating the patient's voice in treatment decisions, setting priorities and monitoring changes over time. 12
HRQoL is a patient‐reported outcome that is assessed using standardized questionnaires. Such questionnaires need to be tested for psychometric properties to prove that they are valid and reliable. For assessing the psychometric properties of a questionnaire, two different approaches can be applied: classical test theory (CTT) and item response theory (IRT). While CTT assumes that the observed score of a test is composed of the true score of a person and measurement errors, IRT models try to plot observable item responses on an underlying construct, the latent trait. 13 Therefore, CTT analyses focus on the average or sum scores and are therefore highly dependent on the sample, while IRT analyses consider a respondent's probability of choosing a distinct response option and can be applied to any population. 14 As in IRT all items are calibrated on the underlying latent trait, 15 scores can be predicted even if responders do not complete every single item.
The Wound‐QoL is a wound‐specific HRQoL questionnaire frequently used in research and clinical practice. It has been developed in 2014 based on three longer questionnaires 8 and encompasses 17 items (Wound‐QoL‐17). The questionnaire has been translated into various languages. The psychometric properties have mainly been analysed using CTT (e.g., 16 , 17 , 18 , 19 , 20 ), showing that the Wound‐QoL is a well‐accepted instrument with mainly good psychometric properties. A recent study by Stülpnagel and colleagues 21 analysed the Wound‐QoL‐17 using both CTT and IRT shedding light on additional statistical aspects. Thereupon, the authors revised the questionnaire based on statistical information and clinical expertise. In this revision, three items were deleted due to low discrimination between response options, low information value for the respective subscale or difficulties in clinical practice and cross‐cultural comparisons. Additionally, slight changes in the scale construction have been established as one item represents aspects of two different subscales. This resulted in an additional short version including 14 items (Wound‐QoL‐14). This study was the first international study using IRT to analyse the Wound‐QoL properties including 1185 patients from six different countries. However, the results were mainly influenced by the US American population, which accounted for more than half of the study sample, and no differences between subgroups were studied.
The aim of the present study was to analyse psychometric properties of both Wound‐QoL‐17 and Wound‐QoL‐14 in a European sample, using IRT. This IRT approach gives insights into patients' response behaviour individually and between subgroups, which shall contribute to the use of these instruments in international and cross‐cultural research and clinical practice.
2. METHODS
This study was approved by the ethics committee of the Medical Association of Hamburg (Ethikkommission der Ärztekammer Hamburg) in June 2019 (PV7029). In participating countries, secondary ethics votes were obtained from the local ethics committees. This article was drafted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist for observational cross‐sectional studies.
2.1. Study design and participants
This was a European study aiming to recruit participants in 10 European countries with 50 included patients per country, which can be considered adequate for assessing structural validity in the total sample according to the COnsensus‐based Standards for the selection of health Measurement Instruments (COSMIN). 22 Prior to study start, two project partners were not able to continue participation in this project, which resulted in eight participating countries (Austria, Lithuania, Netherlands, Poland, Slovakia, Spain, Switzerland, Ukraine). Patients were included if they were at least 18 years of age, had a chronic wound and were able to understand and complete the questionnaire in the respective local language. All participants gave written informed consent. The number of approached participants and the characteristics of non‐participants have not been assessed.
Patients were recruited during routine visits in ambulatory clinics between October 2020 and November 2021. Both patients and treating clinicians completed a questionnaire. Patients provided information about sociodemographic characteristics (e.g., age, gender) and completed the Wound‐QoL‐17. Clinicians reported wound characteristics.
2.2. Measures
Patients completed the Wound‐QoL‐17 as primary endpoint. From the Wound‐QoL‐17, the scales of the Wound‐QoL‐14 can also be calculated. The questionnaire contains 17 items with a 5‐point Likert scale ranging from 0 (not at all) to 4 (very much). If a minimum of 75% of items are answered by the patient, a total score (arithmetic mean) can be calculated from all items. In the same way, three subscales (body: items 1–5; psyche: items 6–10; everyday life: items 11–16) can be calculated; item 17 is not included in a subscale. For the Wound‐QoL‐14, the total score is the arithmetic mean of the 14 items included (without items on knocking [item 10], stairs [item 12] and finances [item 17]). The subscales can be calculated similarly (body: items 1–4; psyche: items 6–9; everyday life: items 11, 13–16), while the item on treatment (item 5) is not included in any subscale.
Grouping variables for differential item functioning (DIF) analysis were age (≤70, >70), gender (male, female), country (Austria, Lithuania, Netherlands, Poland, Slovakia, Spain, Switzerland, Ukraine) and type of wound (leg ulcer, diabetic foot ulcer, other).
2.3. Statistical analysis
We used descriptive statistics for sociodemographic and wound characteristics (absolute and relative frequencies for categorical variables, mean and standard deviation for continuous variables). Missing data were not imputed.
Both Wound‐QoL‐17 and Wound‐QoL‐14 were analysed using IRT. Assumptions of IRT are unidimensionality, local independence, monotonicity and item invariance. 13 Unidimensionality and local independence were analysed based on CTT: Unidimensionality was tested using confirmatory factor analysis (CFA). Model fit of the CFA was assessed using the Root Mean Square Error of Approximation (RSMEA), the Standardized Root Mean Square Residual (SRMR), the Comparative Fit Index (CFI) and the Tucker‐Lewis Index (TLI). We consider an acceptable model fit of the CFA, when RMSEA is below 0.08, SRMR is below 0.1, CFI is above 0.90 23 , 24 and TLI is above 0.90. 25 In the case that CFA model fit was not acceptable, we considered inter‐item correlations for model improvement. Local independence was tested by correlation of residuals between items, with r < 0.25 showing local independence. 14 Monotonicity and item invariance were tested within the IRT model: Monotonicity means that individuals with higher trait level score higher on the items; hence, smoothly increasing operating characteristics curve confirm monotonicity. 14 Item invariance means that items function comparably across different populations, which was tested using DIF.
The IRT model chosen to analyse the data was an unconstrained graded response model (GRM) as it was assumed that all items have different discrimination parameter and as the item responses of the Wound‐QoL can be considered ordinal. 26
We analysed the data, calculated on every dimension separately, using item characteristic curves (ICC), item information curves (IIC) and DIF analysis.
ICCs display a person's chance to tick one of the response options for each item depending on the latent trait level of the person (i.e., the underlying characteristics, such as physical HRQoL). Steep ICC curves of each response category are desirable as these display higher discrimination between different latent trait levels. These are displayed by high discrimination values and hierarchically ordered difficulty values. 14 Discrimination values reflect the ability to differentiate between individuals (i.e., between people with low and high levels of HRQoL impairments). A difficulty value (also called categorical threshold) is the point where two adjacent categories cut each other: Below this threshold, it is more likely that respondents tick the lower response category; above this, it is more likely that they tick the higher response category. In the present study, in the case that ICCs of adjacent response options were not distinct enough (e.g., overlapping peaks of two curves), we merged these categories so that curves of response options are clearly distinct. To compare scores of the original scoring (five response options for each item) and the scoring with merged response options, we computed (sub‐)scale scores according to both scoring options and plotted in scatterplots. For the merged scoring version, we used mean scores of the merged response options (e.g., merged response options 2 [‘moderately’] and 3 [‘quite a lot’] were scored as 2.5; merged response options 1 [‘a little’], 2 [‘moderately’] and 3 [‘quite a lot’] were scored as 2).
The summed‐up ICCs of all response categories of an item display the IICs of this item. The higher the curves of an item in the IIC, the more information this item provides in the respective dimension; flat curves provide low informational value to the dimension. 14
The analysis of DIF was used to compare between subgroups. In DIF analysis, the sample is divided into reference and focal groups to check whether response probabilities depend solely on their latent trait level or also on their membership to the respective subgroup. 27 , 28 , 29 DIFs can be either uniform (i.e., differences are the same across all latent trait levels) or non‐uniform (i.e., differences vary across the latent trait bet). 30 As detection criterion for DIF, Χ 2 with α = 0.01 has been used. 31
Data management and description of patient characteristics were conducted using SPSS version 27.0 (IBM Corp, Armonk, NY). For statistical analysis, R version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria) was used. In R, the lavaan package was used for the CFA, 32 the ltm package to conduct the GRM 33 and the lordif package for the DIF analysis. 31
3. RESULTS
3.1. Patient characteristics
A total of 305 patients (Table 1) participated in the study (mean age: 68.5 years, SD 13.9; 52.8% male). The most frequent types of wounds were leg ulcers (49.2%), followed by diabetic foot ulcers (23.9%) and other ulcers (19.3%).
TABLE 1.
Patient characteristics.
| Characteristic | Total (n = 305) | Austria (n = 51) | Lithuania (n = 50) | Netherlands (n = 37) | Poland (n = 50) | Slovakia (n = 41) | Spain (n = 21) | Switzerland (n = 13) | Ukraine (n = 42) |
|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Gender | |||||||||
| Male | 161 (52.8) | 37 (72.5) | 20 (40.0) | 21 (56.8) | 21 (42.0) | 21 (51.2) | 12 (57.1) | 10 (76.9) | 19 (45.2) |
| Female | 143 (46.9) | 14 (27.5) | 30 (60.0) | 16 (43.2) | 28 (56.0) | 20 (48.8) | 9 (42.9) | 3 (23.1) | 23 (54.8) |
| Missing | 1 (0.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Age group | |||||||||
| ≤70 years | 155 (50.8) | 33 (64.7) | 23 (46.0) | 16 (43.2) | 24 (48.0) | 18 (43.9) | 8 (38.1) | 6 (46.2) | 27 (64.3) |
| >70 years | 147 (48.2) | 18 (35.3) | 27 (54.0) | 21 (56.8) | 25 (50.0) | 22 (53.7) | 13 (61.9) | 7 (53.8) | 14 (33.3) |
| Missing | 3 (1.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.0) | 1 (2.4) | 0 (0.0) | 0 (0.0) | 1 (2.4) |
| Type of wound | |||||||||
| Leg ulcer | 150 (49.2) | 14 (27.5) | 36 (72.0) | 11 (29.7) | 25 (50.0) | 5 (12.2) | 13 (61.9) | 7 (53.8) | 39 (92.9) |
| Diabetic foot ulcer | 73 (23.9) | 23 (45.1) | 13 (26.0) | 14 (37.8) | 1 (2.0) | 19 (46.3) | 0 (0.0) | 1 (7.7) | 2 (4.8) |
| Other | 59 (19.3) | 11 (21.6) | 1 (2.0) | 6 (16.2) | 23 (46.0) | 7 (17.1) | 6 (28.6) | 5 (38.5) | 0 (0.0) |
| Missing | 23 (7.5) | 3 (5.9) | 0 (0.0) | 0 (0.0) | 1 (2.0) | 10 (24.4) | 2 (9.5) | 0 (0.0) | 1 (2.4) |
3.2. Statistical assumptions
Bifactorial CFA was conducted according to the proposed models of the Wound‐QoL‐17 and the Wound‐QoL‐14, each showing three subdomains and one item loading directly on the total score. As the models showed partly acceptable and partly insufficient model fit parameters, we additionally considered the strongest inter‐item correlations: We found that correlations between items 2 (odour) and 3 (exudate), items 11 (moving) and 12 (stairs), and items 14 (leisure activities) and 15 (social activities) in the Wound‐QoL‐17 model and items 2 (odour) and 3 (exudate), and items 14 (leisure activities) and 15 (social activities) in the Wound‐QoL‐14 model improved the model fit indices. These models showed acceptable to good results (Wound‐QoL‐17: RMSEA = 0.069, CFI = 0.951, TLI = 0.941, SRMR = 0.051; Wound‐QoL‐14: RMSEA = 0.076, CFI = 0.953, TLI = 0.941, SRMR = 0.051). Unidimensionality, local independence and monotonicity were given.
3.3. IRT analysis
The ICCs of the Wound‐QoL‐17 (Figure 1) were well‐ordered and sufficiently distinct across all five response options for items 1 (pain), 4 (sleep), 5 (treatment), 8 (worries), 9 (worsening), 11 (moving), 13 (day‐to‐day activities) and 15 (social activities). In the other items, adjacent response categories were not sufficiently distinct. Namely, at least one response option was less likely to be chosen than the others across the whole latent trait (see Supplement 1). Therefore, response options ‘moderately’ and ‘quite a lot’ were merged in items 3 (exudate), 6 (unhappiness), 7 (frustration), 12 (stairs), 14 (leisure activities) and 16 (dependence). In items 2 (odour) and 10 (knocking), response options ‘a little’, ‘moderately’ and ‘quite a lot’ were merged. Item 17 (finances) did not have an ICC as this item is not part of any dimension.
FIGURE 1.
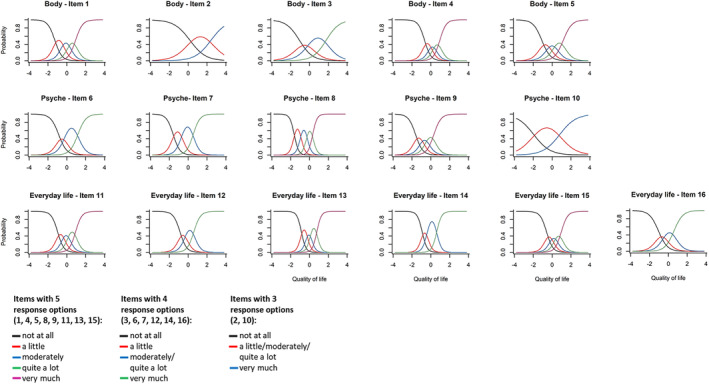
Item characteristic curves of the Wound‐QoL‐17 for all items in the subscales body, psyche and everyday life using merged response options.
In the Wound‐QoL‐14 (Figure 2), the ICCs of all items showed the same patterns as in the Wound‐QoL‐17; while four items did not have any ICCs due to not being assigned to any dimension (item 5 [treatment]) or due to exclusion from the questionnaire (items 10 [knocking], 12 [stairs] and 17 [finances]).
FIGURE 2.
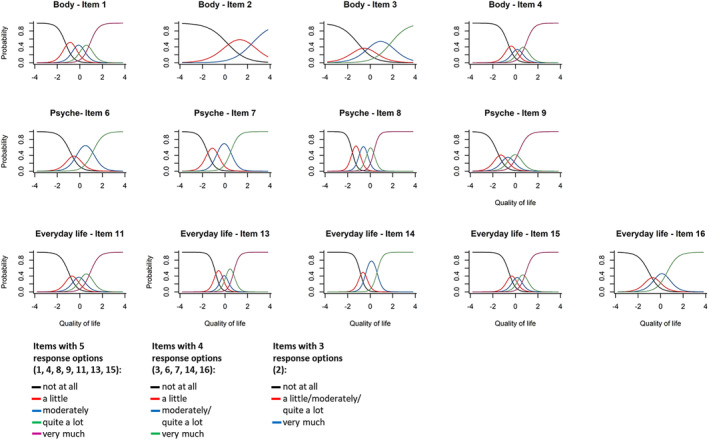
Item characteristic curves of the Wound‐QoL‐14 for all items in the subscales body, psyche and everyday life using merged response options.
Discrimination values and difficulty values were calculated for both Wound‐QoL‐17 and Wound‐QoL‐14 in the newly established models with merged categories. Results can be seen in Supplement 2.
For both Wound‐QoL‐17 and Wound‐QoL‐14, (sub‐)scale scores were calculated using the original scoring and the scoring using merged response options and compared using scatterplots (Figures 3 and 4). These scatterplots showed comparable results using both scoring versions.
FIGURE 3.
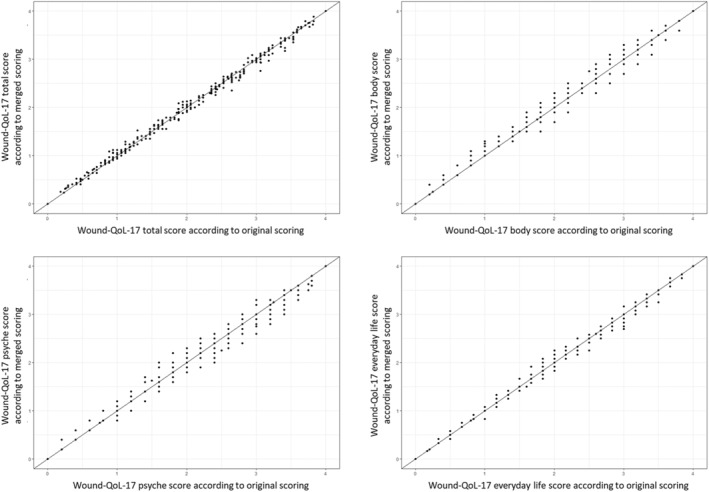
Scatterplots comparing Wound‐QoL‐17 scales using original scoring and scoring using merged response options.
FIGURE 4.
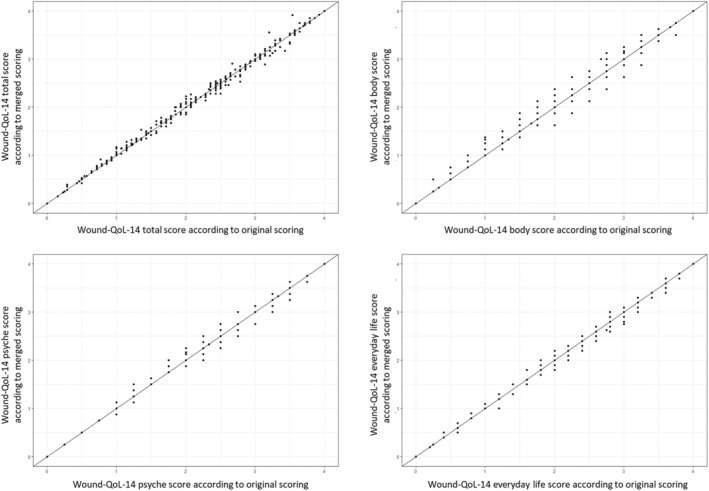
Scatterplots comparing Wound‐QoL‐14 scales using original scoring and scoring using merged response options.
The IICs in the Wound‐QoL‐17 (Figure 5) show that item 4 (sleep) had the highest informational value for the body subscale, followed by item 1 (pain), items 2 (odour) and 3 (exudate) provided only little information. In the psyche subscale, item 8 (worries) had by far the highest informational value, whereas item 10 (knocking) had almost no informational value. In the everyday life subscale, item 13 (day‐top‐day activities) had the highest informational value; item 16 (dependence) had the lowest informational value.
FIGURE 5.
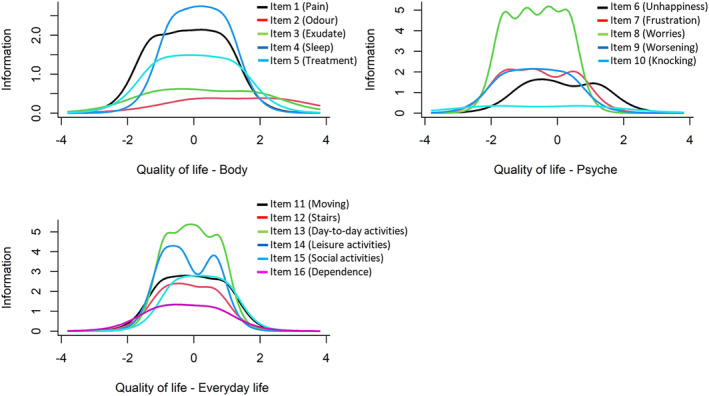
Item information curves of the subscales body, psyche and everyday life of the Wound‐QoL‐17.
IIC results of the Wound‐QoL‐14 (Figure 6) were similar to those of the Wound‐QoL‐17. Items 1 (pain) and 4 (sleep) had the highest informational value for the body subscale. Items 2 (odour) and 3 (exudate) gave only little information to the score of the body subscale. In the psyche subscale, item 8 (worries) had by far the highest informational value. In the everyday life subscale, items 13 (day‐to‐day activities) and 14 (leisure activities) had both the highest informational value.
FIGURE 6.
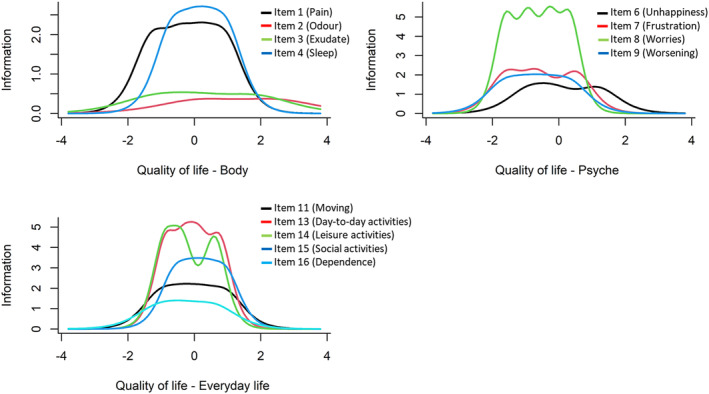
Item information curves of the subscales body, psyche and everyday life of the Wound‐QoL‐14.
DIF analysis showed no DIFs in the body and psyche subscales of the Wound‐QoL‐17. In the everyday life subscale, item 15 (social activities) showed uniform DIFs regarding the country and age, while item 12 (stairs) showed non‐uniform DIFs only regarding age. No DIFs were detected regarding gender and type of wound.
In the Wound‐QoL‐14, only item 15 (social activities) showed uniform DIFs regarding country and age.
4. DISCUSSION
This study examined the psychometric properties of the Wound‐QoL‐17 and the Wound‐QoL‐14 in a European sample using IRT analysis. It showed comparable results across both questionnaire versions and confirmed that items excluded in the shortened version were those, which posed issues in their statistical performance according to IRT analyses. In this study, we established a new scoring method for the questionnaires, namely merging response categories for several items.
Unidimensionality of the single subscales of both Wound‐QoL versions was confirmed by the CFA. In contrast to the previous publication, 21 additional inter‐item correlations were included in model of the Wound‐QoL. Our results propose correlations within distinct subscales, which are also contextually conclusive: Odour (item 2) and exudate (item 3) are not necessarily present in all patients experiencing physical strain, but both aspects often co‐exist. The ability to move about (item 11) and the ability to climb stairs (item 12) are also closely linked to each other and might be more related with each other than with the other items of the everyday life subscale, which are more activity‐related. Similarly, the items on leisure activities (item 14) and activities with others (item 15) are closely linked in terms of wording and content.
Similarly to the study by Stülpnagel and colleagues, 21 the ICCs in this study show good discrimination between the response options for around half of the items. Items with critical ICCs most often showed problems with the middle category or with both the middle and the second highest categories. In these items, a 5‐point Likert scale might be too graduated. Therefore, we merged adjacent response options that showed insufficient discrimination. We propose to conduct this merging only in the process of score computation but to keep the five response options in the questionnaire. As one of the main aims of the Wound‐QoL development was to provide short and easy‐to‐understand instruments, we assume that the uniformity of response options contribute to the acceptance of this questionnaire.
The IICs show that, as in a previous study, 21 the informative value of the items related to one subscale differed widely: while there were one or two items with relatively high informative value for each subscale, other items had comparatively low informative value. Items on odour and exudate had remarkably low values, which might indicate that the character of the body scale is less reflective (where all items are indicators of the same unidimensional construct) but rather formative (where each item represents a distinct aspect of a composite construct). 34 Another item with low informative values was item 10 (knocking), which was deleted in the shortened Wound‐QoL‐14.
DIF analysis showed only few differences between subgroups. Age‐related DIFs in the Wound‐QoL‐17 might be explained by the fact that climbing stairs (item 12) and activities with others (item 15) are more restricted in older patients anyways regardless of the impact of the wound. Possible reasons for country‐related DIFs in item 15 on activities with others might be cultural differences in the understanding of spending time together. DIFs have been analysed for single items, which are embedded in multi‐item scales in the Wound‐QoL. We assume these DIFs to have marginal impact on the respective subscales and the global scale, especially in the Wound‐QoL‐14 in which one of these items has been removed. The aspects covered in the items with DIF are meaningful to patients with chronic wounds and therefore important in the context of HRQoL. For such items with important content for the construct but with subgroup differences, individual responses should be compared within the respective group. 28
This study confirms that with the development of the Wound‐QoL‐14, 21 items were deleted that posed some issue in the light of IRT analysis. This applied especially to item 10 (knocking) showing flat ICCs and low informative value in the IIC and to item 12 (stairs) showing difficulties with the middle and second highest response options and age‐related DIFs. Additionally, item 5 (treatment) was excluded from the subscales, which had low informative value for the body subscale.
This study has several strengths. First, it examines the Wound‐QoL questionnaires with IRT, which is a method rarely used for the Wound‐QoL and, hence, giving new insights into its psychometrics. Existing studies were either country‐specific 35 or highly influenced by the data of one country accounting for more than half of the patients in the data set. 21 This is the first European study assessing the Wound‐QoL characteristics including data from eight countries. For the first time, it assesses DIF in the Wound‐QoL and shows only few differences regarding age or country. Few country‐specific differences support the use of the questionnaires in international studies and clinical practice. We analysed the data for both Wound‐QoL‐17 and Wound‐QoL‐14, which allowed for detailed comparison between both questionnaire versions.
Limitations of this study were the reduced number of participating countries and participants compared with the study protocol. This resulted in less evenly distributed participants per country than expected and limits generalizability of the results; however, not a single country accounted for more than a sixth of the total sample. In the CFA, we adapted the pre‐existing models by adding three (Wound‐QoL‐17) and two (Wound‐QoL‐14) inter‐item correlations. Even though these correlations were added to the original model, they are conclusive and justifiable in terms of content. As IRT requires unidimensionality, in the multidimensional construct of HRQoL, only subscales can be considered. Therefore, one item per Wound‐QoL version could not be tested in our analysis.
In conclusion, this study confirms the validity of both the Wound‐QoL‐17 and the Wound‐QoL‐14 and shows comparable results across both Wound‐QoL versions. The newly established scoring method for the questionnaires could be applied in research projects and especially in international studies. For clinical practice, the application of the original scoring can be maintained as simplicity and manageability of the scoring is crucial in routine practice where time and resources are scarce. The scatterplots visualizing the new and the original scoring algorithms support the comparability of both scoring methods.
FUNDING INFORMATION
This study has been partly funded by the European Academy of Dermatology and Venereology (EADV).
CONFLICT OF INTEREST STATEMENT
TMJ, VK, SV, LR, PC, MJ, CVM, SA, MB and ECM have no relevant financial or non‐financial interests to disclose. AR has been a consultant or speaker for AbbVie, Bioderma, Boehringer Ingelheim, Celgene, Chema Elektromet, Eli Lilly, Galderma, Janssen, Leo Pharma, Medac, Menlo Therapeutics, Novartis, Pierre‐Fabre, Sandoz and Trevi Therapeutics; and principal investigator or subinvestigator in clinical trials sponsored by Abbvie, Alvotech, Amgen, AnaptysBio, Argenx, Biothera, BMS, Celgene, Celltrion, Dermira, Galderma, Inflarx, Janssen, Kiniksa, Kymab, Leo Pharma, Novartis, Pfizer, Trevi Therapeutics, UCB. KS participated in clinical trials as subinvestigator sponsored by Amgen, Anaptys, Almirall, Celltrion, Galderma, Kiniksa, Novartis, Trevi Therapeutics and was an invited speaker by Medac and Novartis. MA has received fees for consulting and/or lectures and/or studies from the following companies: 3 M Medica, AOK Bundesverband, Bayer Healthcare, Beiersdorf, Birken, Bode, B. Braun, BSNmedical/Essity, BVmed, Coloplast, DAK, Diabet concept, Gerromed, GlaxoSmithKline, Johnson & Johnson, Lohmann & Rauscher, medi, Medovent, Mölnlycke, Smith & Nephew, Schülke & Mayr, Söring, Sorbion, Systagenix, Uluru, Urgo. Project proposal has been submitted by MA. CB is project lead of the HAQOL study, which has been partly funded by the EADV.
Supporting information
Data S1. Supporting Information.
ACKNOWLEDGEMENTS
The authors thank the Scientific Communication Team of the IVDP, in particular Sara Tiedemann and Mario Gehoff, for copy editing. We acknowledge financial support from the Open Access Publication Fund of UKE ‐ Universitätsklinikum Hamburg‐Eppendorf and DFG – German Research Foundation. Open Access funding enabled and organized by Projekt DEAL.
Janke TM, Kozon V, Valiukeviciene S, et al. Assessing health‐related quality of life using the Wound‐QoL‐17 and the Wound‐QoL‐14—Results of the cross‐sectional European HAQOL study using item response theory. Int Wound J. 2024;21(8):e70009. doi: 10.1111/iwj.70009
DATA AVAILABILITY STATEMENT
Data are available on reasonable request from the corresponding author.
REFERENCES
- 1. Dissemond J, Bültemann A, Gerber V, Jäger B, Münter C, Kröger K. Definitionen für die Wundbehandlung. Hautarzt. 2016;67:265‐266. [DOI] [PubMed] [Google Scholar]
- 2. Lazarus GS, Cooper DM, Knighton DR, et al. Definitions and guidelines for assessment of wounds and evaluation of healing. Wound Repair Regen. 1994;2(3):165‐170. [DOI] [PubMed] [Google Scholar]
- 3. Werdin F, Tenenhaus M, Rennekampff H‐O. Chronic wound care. Lancet. 2008;372(9653):1860‐1862. [DOI] [PubMed] [Google Scholar]
- 4. Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: systematic review and meta‐analysis of observational studies. Ann Epidemiol. 2019;29:8‐15. [DOI] [PubMed] [Google Scholar]
- 5. European Commission . The 2018 Ageing Report. Publication Office of the European Union; 2018. [Google Scholar]
- 6. Olsson M, Järbrink K, Divakar U, et al. The humanistic and economic burden of chronic wounds: a systematic review. Wound Repair Regen. 2019;27(1):114‐125. [DOI] [PubMed] [Google Scholar]
- 7. Edwards H, Finlayson K, Skerman H, et al. Identification of symptom clusters in patients with chronic venous leg ulcers. J Pain Symptom Manage. 2014;47(5):867‐875. [DOI] [PubMed] [Google Scholar]
- 8. Blome C, Baade K, Debus ES, Price P, Augustin M. The ‘Wound‐QoL’: a short questionnaire measuring quality of life in patients with chronic wounds based on three established disease‐specific instruments. Wound Repair Regen. 2014;22(4):504‐514. [DOI] [PubMed] [Google Scholar]
- 9. Klein TM, Andrees V, Kirsten N, Protz K, Augustin M, Blome C. Social participation of people with chronic wounds: a systematic review. Int Wound J. 2021;18(3):287‐311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Black N, Burke L, Forrest CB, et al. Patient‐reported outcomes: pathways to better health, better services, and better societies. Qual Life Res. 2016;25(5):1103‐1112. [DOI] [PubMed] [Google Scholar]
- 11. U.S. Food and Drug Administration . Guidance for industry. Patient‐reported outcome measures: use in medical product development to support labeling claims. 2009. https://www.fda.gov/media/77832/download [DOI] [PMC free article] [PubMed]
- 12. Greenhalgh J, Gooding K, Gibbons E, et al. How do patient reported outcome measures (PROMs) support clinician‐patient communication and patient care? A realist synthesis. J Patient Rep Outcomes. 2018;2:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Champlain AF d. A primer on classical test theory and item response theory for assessments in medical education. Med Educ. 2010;44(1):109‐117. [DOI] [PubMed] [Google Scholar]
- 14. Fayers PM, Machin D, Quality of life . The Assessment, Analysis and Reporting of Patient‐Reported Outcomes. 3rd ed. John Wiley & Sons Ltd; 2016. [Google Scholar]
- 15. Edelen MO, Reeve BB. Applying item response theory (IRT) modeling to questionnaire development, evaluation, and refinement. Qual Life Res. 2007;16(Suppl 1):5‐18. [DOI] [PubMed] [Google Scholar]
- 16. Amesz SF, Klein TM, Meulendijks AM, et al. A translation and preliminary validation of the Dutch wound‐QoL questionnaire. BMC Dermatol. 2020;20(1):5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Fagerdahl A‐M, Bergström G. Translation and validation of a wound‐specific, quality‐of‐life instrument (the Wound‐QoL) in a Swedish population. Ostomy Wound Manage. 2018;64(5):40‐46. [PubMed] [Google Scholar]
- 18. Knudsen JT, Johansen CW, Hansen AØ, Eshoj HR. The Danish wound‐quality of life (Wound‐QoL) questionnaire: translation and psychometric properties. Wound Repair Regen. 2021;29(6):973‐984. [DOI] [PubMed] [Google Scholar]
- 19. Gamus A, Kaufman H, Keren E, Brandin G, Peles D, Chodick G. Validation of ‘Wound QoL’ Hebrew version disease‐specific questionnaire for patients with lower extremity ulcerations. Int Wound J. 2018;15(4):600‐604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Janke TM, Kozon V, Valiukeviciene S, et al. Validation of the Wound‐QoL‐17 and the wound‐QoL‐14 in a European sample of 305 patients with chronic wounds. Int Wound J. 2023;21(3):e14505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Stülpnagel CC v, Da Silva N, Augustin M, et al. Assessing the quality of life of people with chronic wounds by using the cross‐culturally valid and revised Wound‐QoL questionnaire. Wound Repair Regen. 2021;29(3):452‐459. [DOI] [PubMed] [Google Scholar]
- 22. Mokkink LB, Prinsen CA, Patrick DL, et al. COSMIN study design checklist for patient‐reported outcome measurement instruments. 2019. https://www.cosmin.nl/wp-content/uploads/COSMIN-study-designing-checklist_final.pdf
- 23. Harrington D. Confirmatory Factor Analysis. Oxford University Press, Inc.; 2009. [Google Scholar]
- 24. Kline RB. Principles and Practice of Structural Equation Modeling. 4th ed. Guilford Press; 2016. [Google Scholar]
- 25. Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychol Bull. 1980;88(3):588‐606. [Google Scholar]
- 26. Samejima F. Estimation of latent ability using a response pattern estimation of latent ability using a response pattern of graded scores. ETS Res Bull Ser. 1968;1968(1):1‐169. [Google Scholar]
- 27. Reise SP, Widaman KF, Pugh RH. Confirmatory factor analysis and item response theory: two approaches for exploring measurement invariance. Psychol Bull. 1993;114(3):552‐566. [DOI] [PubMed] [Google Scholar]
- 28. Chen W‐H, Revicki D. Differential item functioning (DIF). In: Michalos AC, ed. Encyclopedia of Quality of Life and Well‐Being Research. Dordrecht Springer; 2014:1611‐1614. [Google Scholar]
- 29. Nugent WR. Understanding DIF and DTF: description, methods, and implications for social work research. JSSWR. 2017;8(2):305‐334. [Google Scholar]
- 30. Berger M, Tutz G. Detection of uniform and nonuniform differential item functioning by item‐focused trees. J Educ Behav Stat. 2016;41(6):559‐592. [Google Scholar]
- 31. Choi SW, Gibbons LE, Crane PK. Lordif: an R package for detecting differential item functioning using iterative hybrid ordinal logistic regression/item response theory and Monte Carlo simulations. J Stat Softw. 2011;39(8):1‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Rosseel Y. Lavaan: an R package for structural equation modeling. J Stat Softw. 2012;48(2):1‐36. [Google Scholar]
- 33. Rizopoulos D. Ltm: an R package for latent variable modelling and item response theory analyses. J Stat Softw. 2006;17(5):1‐25. [Google Scholar]
- 34. de Vet HCW, Terwee CB, Mokkink LB, Knol DL. Measurement in medicine: A practical guide. 10th ed. Cambridge University Press; 2018. [Google Scholar]
- 35. Sommer R, von Stülpnagel CC, Fife CE, et al. Development and psychometric evaluation of the U.S. English wound‐QoL questionnaire to assess health‐related quality of life in people with chronic wounds. Wound Repair Regen. 2020;28(5):609‐616. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Supporting Information.
Data Availability Statement
Data are available on reasonable request from the corresponding author.