

Abstract
Objective:
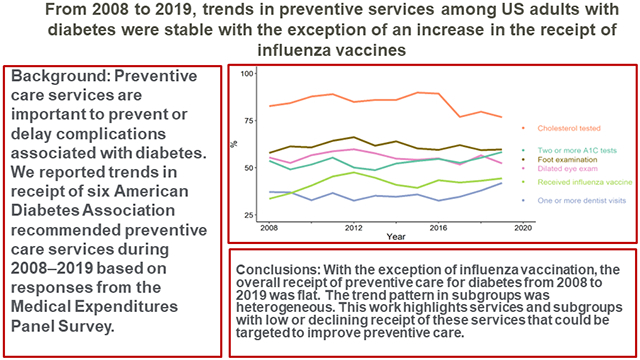
Preventive care services are important to prevent or delay complications associated with diabetes. We reported trends in receipt of six American Diabetes Association recommended preventive care services during 2008–2020.
Research Design and Methods:
We used 2008–2020 data from the cross-sectional Medical Expenditures Panel Survey to calculate the proportion of U.S. adults ≥18 years of age with diagnosed diabetes that reported receiving preventive care services, overall and by subpopulation (n = 25,616). We used Joinpoint regression to identify trends during 2008–2019. The six services completed in the past year included ≥1 dental examination, dilated eye examination, foot examination, ≥2 A1C tests, cholesterol test, and receipt of an influenza vaccine.
Results:
From 2008–2020, proportions of U.S. adults with diabetes receiving any individual preventive care service ranged from 32.6% to 89.9%. From 2008–2019, overall trends in preventive services among these adults were flat except for an increase in influenza vaccination (average annual percent change: 2.6% [95% CI: 1.1%, 4.2%]). Trend analysis of subgroups was heterogeneous: influenza vaccination and A1C testing showed improvements among several subgroups, while cholesterol testing (45-64 year age, < high school education, Medicaid insurance) and dental visits (uninsured) declined. In 2020, 8.2% (4.5%, 11.9%) of those with diabetes received none of the recommended preventive care services.
Conclusions:
Other than influenza vaccination, we observed no improvement in preventive care service utilization among U.S. adults with diabetes. These data highlight services and specific subgroups that could be targeted to improve preventive care among adults with diabetes.
Keywords: preventive services, Medical Expenditure Panel Survey, trends, joinpoint
Graphical Abstract
Twitter Summary:
We report trends of six recommended preventive care services from 2008 – 2020. Other than flu vaccination, we saw no improvement in preventive care service utilization for US adults with diabetes.
Introduction
Diabetes is a chronic disease that affects 11.3% of the adult population, or 37.1 million adults, in the United States (1). Diabetes is also costly: total direct and indirect costs in 2017 were estimated at $327 billion (2). The prevalence of diabetes in the U.S. is expected to increase to 60.6 million adults by the year 2060 (3). Incidence of diabetes peaked in the U.S. at 8.5 cases per 1,000 in 2008 and 2009 and has fallen since to 5.1 cases per 1,000 in 2021 (4,5). While rates of newly diagnosed cases of diabetes have decreased, rates of hospitalization with diabetes as the primary diagnosis have been increasing since the year 2000 by about 2.5% per year (6).
Complications of diabetes include both microvascular (retinopathy, neuropathy, and diabetic nephropathy) and macrovascular complications (coronary artery disease, peripheral arterial disease, and stroke) (7,8). Access to preventive services to control glycemia, lipids, and blood pressure and the early identification of diabetic retinopathy and foot lesions is important to minimize diabetes-related complications and reduce rates of hospitalization (7,9,10). Other studies have reported on trends in receipt of some preventive services in the 2000s using data from various surveys, such as the Behavioral Risk Factor Surveillance System (BRFSS) and the National Health and Nutrition Examination Survey (NHANES) (11-15). To our knowledge, the proportion and trend of receipt of preventive services addressed in the Medical Expenditure Panel Survey (MEPS) has not been reported. Analysis of MEPS data provides advantages over other surveys, as it is nationally representative and available yearly. Meanwhile, NHANES is not annual and has smaller sample sizes; BRFSS is administered at the state level, and the diabetes module is not available in every state in every year. We reported the proportion of and trends in the receipt of six preventive care services recommended by the American Diabetes Association (ADA) overall and among subgroups (7). These data are valuable for identifying groups that may be under-utilizing health care services, examining any effects the start of the COVID-19 pandemic may have had on receipt of these services, and providing benchmarks for future studies.
Research Design and Methods
Data Source
We used data from the 2008 – 2020 MEPS, a household survey of U.S. noninstitutionalized populations administered and maintained by the Agency for Healthcare Research and Quality since 1996 (16). The set of households surveyed for MEPS is a subsample of those surveyed in the National Health Interview Survey (NHIS). We chose the years 2008 to 2020 due to consistency of questions related to preventive care during that time period starting in 2008. Data from MEPS were collected through a combination of computer-assisted personal interviewing and pencil-and-paper surveys. In 2020, the computer-assisted personal interviews were changed from in-person to phone interviews due to the COVID-19 pandemic. MEPS provides national and regional estimates of health care use, expenditures, sources of payment and health insurance coverage. This survey also contains information on patient demographics, socioeconomic characteristics, and, via the Diabetes Care Survey (DCS), information on diabetes preventive care services. The DCS is a self-administered paper-and-pencil questionnaire that is mailed to MEPS respondents who indicate that they have been told by a doctor or health care professional that they have diabetes. In this analysis, we used data from the full-year consolidated MEPS files for adults with diagnosed diabetes that responded to the DCS survey (n = 25,616). Response rates for the DCS survey ranged from 92.4% in 2008 to 57.1% in 2020.
Outcome Measures
Among respondents with self-reported diagnosed diabetes, we selected six preventive care variables that were available in the data from 2008 to 2020. These variables are based on self-reported receipt in a given year (17): ≥1 dental examination (derived from total number of reported dental care visits), a dilated eye examination, a foot examination by a healthcare provider, ≥2 A1C tests, a blood cholesterol test, and an influenza vaccine. Respondents were asked about receiving each of these services in a given year (e.g., “Did you receive an influenza vaccine in 2013?”). We also created binary variables classifying adults with diabetes who received none of the recommended preventive care services or all of the recommended services, although these results were presented only for the overall population due the unreliability of estimates of some sub-populations in some years (18).
Analysis
Our analysis accounts for the complex survey design used, including clustering and stratification, using the weights provided for the DCS (16). Reported values were age-adjusted using the direct method, standardized to the 2000 U.S. population grouped by ages 18 – 44, 45 – 64, 65 – 74, and ≥75 years. We presented these estimates for the overall population, as well as stratified by self-reported characteristics of age, sex, race and ethnicity, highest degree of education, type of health insurance, and the ratio of family income to the poverty line (poverty income ratio). We used the package gtsummary in R Statistical Software (v4.2.1) to calculate estimates (19,20).
Medical care utilization decreased as a result of the COVID-19 pandemic starting in early 2020 (21). We excluded 2020 from the trend analysis because of the decreased medical care utilization associated with the COVID-19 pandemic. However, we presented the estimated proportions for 2020 in the results to show how the onset of the pandemic affected the reported receipt of preventive services. Trends were analyzed using Joinpoint Command Line Software (22) with R via the R package nih.joinpoint (23). The Joinpoint software was used to fit a weighted least-squares regression model to the estimated proportions on the linear scale. A maximum of three joinpoints were searched for using the Grid search algorithm. As few as two observed time points were allowed between line segment. Joinpoint regression uses permutation tests to detect statistically significant changes at a pre-specified alpha of 0.05 in direction or magnitude of trends (24). The Joinpoint software also provided estimates of the annual percent change (APC), or slope, for each trend segment and the average annual percent change (AAPC), or overall slope, for the entire trend. The test of significance for APC is an asymptotic t-test. Due to the omnibus nature of the permutation test used to identify Joinpoint years and the use of all the data in identifying those years, the permutation tests are more powerful (24). In some cases, Joinpoint years are identified but the corresponding intervals for the APC will overlap zero due to this power difference.
Data and Resource Availability
The datasets generated during and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Results
All values pertaining to individual preventive practices presented here, as well as those that are not described, can be found in Supplemental Table 1. Figures 1 and 2 display trends, overall and by subgroup.
Figure 1—

Age-adjusted trends in proportions of U.S. adults with diagnosed diabetes overall and by subgroup who reported receiving recommended medical examinations from 2008 to 2019. The dashed black line is the overall trend, while dots represent percentages for 2020. Data from 2020 were not included in the trend analysis.
Figure 2—

Age-adjusted trends in proportions of U.S. adults with diagnosed diabetes overall and by subgroup who reported receiving recommended lab tests and vaccinations. The dashed black line is the overall trend, while dots represent percentages for 2020. Data from 2020 were not included in the trend analysis.
Dilated Eye Exam
The overall proportion receiving dilated eye exams was stable during 2008–2019 (Table 1, Figure 1). This proportion averaged 55.5% (95% CI: 54.0%, 57.0%) over this period. Similarly, for males, we observed stable trends from 2008 to 2011 but a significant decrease after 2011 (APC −1.6% [−2.9%, −0.3%]) (Figure 1). Uninsured adults with diabetes had average annual increase from 2008 to 2019 in the receipt of dilated eye exams of 3.3% (0.1%, 6.6%) (Figure 1). Adults with diabetes in the highest income group (poverty income ratio > 400%) had a flat trend in dilated eye examinations until 2013, after which the proportion significantly decreased (APC −3.8% [−6.8%, −0.7%]).
Table 1—
Age-adjusted trends in proportions of U.S. adults with diagnosed diabetes that report receiving recommended care services - at least one dental visit, one dilated eye exam, one foot exam, two or more A1C tests, cholesterol level tested, and receiving an influenza vaccine.
| Preventive service |
Average (SE)* |
2008 (SE) |
2009 (SE) |
2010 (SE) |
2011 (SE) |
2012 (SE) |
2013 (SE) |
2014 (SE) |
2015 (SE) |
2016 (SE) |
2017 (SE) |
2018 (SE) |
2019 (SE) |
2020 (SE) |
Percent Change (95% CI)*,† |
Joinpoint Year‡ |
APC (95% CI)*,§ |
AAPC (95% CI)*,∥ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cholesterol tested | 84.4 (1.3) | 82.7 (1.9) | 84.3 (1.8) | 87.8 (1.3) | 89.0 (1.4) | 84.9 (1.6) | 85.9 (1.7) | 85.9 (1.8) | 89.9 (1.5) | 89.3 (1.6) | 77.0 (1.8) | 79.7 (1.7) | 76.8 (2.6) | 71.1 (3.1) | −7.1 (−14.5, 0.4) | −0.7 (−1.6, 0.2) | −0.7 (−1.6, 0.2) | |
| Received influenza vaccine | 41.8 (1.1) | 33.6 (1.8) | 36.5 (2.2) | 40.5 (1.9) | 45.4 (2.1) | 47.6 (2.1) | 44.7 (2.4) | 41.0 (2.3) | 39.4 (2.0) | 43.4 (2.3) | 42.2 (2.1) | 43.1 (2.2) | 44.4 (2.7) | 42.5 (2.8) | 32.4 (11.3, 53.5) | 2012, 2015 | 9.2 (6.9, 11.6), −6.0 (−12.1, 0.6), 2.9 (0.7, 5.1) | 2.6 (1.1, 4.2) |
| One or more dentist visits | 35.7 (0.7) | 37.2 (2.0) | 37.0 (2.2) | 32.8 (2.0) | 36.6 (2.4) | 32.6 (1.8) | 35.1 (2.0) | 34.6 (2.1) | 35.9 (2.0) | 32.6 (2.1) | 34.6 (2.2) | 37.9 (2.3) | 41.9 (2.7) | 32.7 (2.9) | 12.9 (−5.6, 31.3) | 2017 | −0.7 (−2.2, 0.9), 11.6 (−6.1, 32.7) | 1.4 (−1.4, 4.3) |
| Two or more A1C tests | 53.0 (0.8) | 53.7 (2.3) | 49.1 (2.3) | 51.7 (2.0) | 55.4 (2.0) | 50.1 (2.3) | 48.8 (2.2) | 52.3 (2.1) | 53.6 (2.2) | 54.7 (2.1) | 52.7 (2.0) | 55.3 (2.5) | 58.3 (2.5) | 59.3 (3.0) | 8.7 (−4.3, 21.7) | 0.8 (−0.1, 1.7) | 0.8 (−0.1, 1.7) | |
| Dilated eye exam | 55.5 (0.7) | 55.5 (2.1) | 52.6 (2.3) | 56.6 (2.1) | 58.8 (2.4) | 59.8 (2.1) | 57.7 (2.2) | 54.8 (2.1) | 54.3 (2.1) | 55.0 (2.1) | 51.7 (2.2) | 56.6 (2.4) | 52.3 (3.0) | 49.7 (2.9) | −5.7 (−18.2, 6.9) | −0.4 (−1.3, 0.4) | −0.4 (−1.3, 0.4) | |
| Foot examination | 61.4 (0.7) | 57.9 (2.4) | 61.3 (2.2) | 60.8 (2.0) | 64.3 (1.8) | 66.2 (2.0) | 61.7 (2.4) | 64.0 (2.2) | 60.3 (2.1) | 59.5 (2.2) | 62.0 (1.9) | 59.4 (2.5) | 59.7 (2.5) | 54.4 (2.9) | 3.2 (−8.5, 14.9) | 2011 | 3.5 (−1.1, 8.4), −1.1 (−2.1, −0.1) | 0.2 (−1.0, 1.4) |
Values in these columns were estimated excluding data from 2020.
Percent change: the percent change in the proportion from 2008 to 2019.
Years identified as Joinpoint years.
Annual percent change: the slope of the line in each period demarcated by a Joinpoint year. If two Joinpoint years are identified, there will be three different annual percent changes. Joinpoint years are identified by permutation test, whereas the test of significance for APC is an asymptotic t-test. Due to the omnibus nature of the permutation test and the use of all the data in identifying the Joinpoints, the permutation tests are more powerful. In some cases, Joinpoint years are identified but the corresponding intervals for the APC will overlap zero due to this power difference.
Average annual percent change: the slope of the line over the entire study period.
Foot Exam
The average proportion of U.S. adults with diabetes receiving a foot exam over the study period was 61.4% (95% CI: 60.0%, 62.8%) (Table 1). The trend for foot exams for the overall adult population with diabetes was flat until 2011, after which it decreased (APC −1.1% [−2.1%, −0.1%], Table 1, Figure 1). We found an increase in foot exams among adults with diabetes age 65–74 years until 2014 (APC 1.9% [0.5%, 3.4%]), and the trend was flat thereafter (Figure 1).
One or More Dentist Visits
The trend for dentist visits for the overall adult population with diabetes was stable over the study period, averaging 35.7% (34.2%, 37.2%) (Table 1). Adults age 65–74 and ≥75 years had average annual percent increases of 3.1% (2.1%, 4.1%) and 1.4% (0.1%, 2.7%), respectively. Non-Hispanic White adults with diabetes had an average annual percent increase of 1.8% (0.5%, 3.1%). Among those with private insurance, we found decreasing proportions visiting the dentist during 2008–2015 (APC −2.6% [−4.3%, −0.9%]), followed by an increase after 2015 (APC 5.6% [1.4%, 9.9%]. The trends for adults with diabetes in the poverty income ratio group < 100% and those with a high school education had multiple changes upward and downward during the study period.
Cholesterol Testing
During 2008–2019, we found no significant change in the percentage of adults with diabetes who received cholesterol tests, which averaged 84.4% (95% CI: 81.8%, 87.0%) during this period (Table 1). For adults age 45–64 years, cholesterol testing was flat from 2008 to 2015 and showed a significant decrease starting in 2016 (APC −4.8% [−7.3%, −2.4%], AAPC −1.3% [−2.0%, −0.6%]). We found significant decreases starting in 2016 in the percentage of males (APC −6.9% [−11.7%, −1.8%]) and adults with less than a high school education (APC −10.4% [−15.8%, −4.6%], AAPC −2.3% [−3.8%, −0.6%]) who received cholesterol testing. Adults with Medicaid had an AAPC of −2.3% (−3.6%, −1.0%).
Influenza Vaccine
From 2008 to 2019, receipt of influenza vaccines increased at an AAPC of 2.6% (1.1%, 4.2%) (Table 1, Figure 2). The average proportion of adults with diabetes receiving an influenza vaccine over the study period was 41.8% (39.6%, 44.0%). Specifically, we noted significant increases during 2008 – 2012 (APC 9.2% [6.9%, 11.6%], AAPC 2.6% [1.1%, 4.2%]), and after 2015 (APC 2.9% [0.7%, 5.1%]) (Table 1). The influenza vaccine trend for non-Hispanic White adults followed a similar pattern (AAPC 3.7% [1.5%, 5.9%]), although only the period from 2008 to 2012 had a significant increase (APC 12.2% [8.9%, 15.7%]). Receipt of influenza vaccines increased among females over the entire study period (AAPC 2.0% [0.4%, 3.7%]). Adult males, adults in the poverty income ratio group 200%–399% and >400%, and adults with private insurance showed an increase in the receipt of influenza vaccines in the early part of the study period, but flat thereafter. Receipt of influenza vaccines increased slightly for adults on Medicare (AAPC 1.0% [0.1%, 1.9%]).
A1C Tests
We observed no significant changes in the overall trend in the proportion of adults receiving two or more A1C tests in a year, which averaged 53.0% (95% CI: 51.4%, 54.5%) over the study period (Table 1). Proportions increased annually by 1.2% (0.6%, 1.7%), 1.8% (0.8%, 2.9%), and 2.2% (0.7%, 3.8%) for those age 45–64, 65–74, and ≥75 years, respectively. We also found increases in A1C testing for Hispanic adults (AAPC 6.8% [2.0%, 11.8%] ), non-Hispanic White adults (AAPC 1.2% [0.5%, 1.9%]), those with Medicare only (AAPC 1.6% [0.4%, 2.9%]), and those in the highest poverty income ratio group (> 400%) (AAPC 1.1% [0.5%, 1.8%]).
Aggregate Preventive Care Services
For both adults with diabetes that reported receiving none of the six recommended preventive services and adults reporting receiving all of them, trends were flat from 2008 to 2019 (zero services: 3.1% [95% CI: −4.5%, 11.3%]; all services: 1.4% [−0.9%, 3.7%]; Supplemental Table 2). In 2008, 5.1% (2.7%, 7.5%) of adults with diabetes reported receiving none of the six recommended care services (Supplemental Table 2). In 2019, this estimate was 6.1% (3.7%, 8.5%) and in 2020 it was 8.2% (4.5%, 11.9%; Supplemental Table 2). The percentage of adults that reported receiving all six preventive services in 2008 was 7.1% (4.5%, 9.6%), 10.8% (7.4%, 14.1%) in 2019 and 7.9% (5.3%, 10.5%) in 2020 (Supplemental Table 2).
Comparisons Among Subgroups
The youngest adults (18–44 years) often reported lower rates of dilated eye exams, foot exams, cholesterol testing, and influenza vaccination. Uninsured adults often reported the lowest rates of preventive care for dilated eye exams, foot exams, cholesterol testing, and A1C testing. Adults with less than a high school education were less likely to visit the dentist in most years, although they were only statistically significantly less likely to visit the dentist in 2008–2010, 2013–2014, and 2020.
Discussion
Influenza vaccination was the only preventive service that increased significantly during 2008–2019 overall. Among most subgroups, influenza vaccine uptake, A1C testing, and dental visits tended to improve. However, foot exams, cholesterol testing, and dental visits among the uninsured tended to decline. The passing of the Affordable Care Act (ACA) in 2010 and subsequent Medicaid expansion has been seen as a mechanism to increase the receipt of preventive services (12); however, we found no significant change over time in five out of the six preventive care services for the overall U.S. adult population with diagnosed diabetes from 2008 to 2019. While the passing of the ACA led to an increase in the number of adults with diagnosed and undiagnosed diabetes who have health insurance, and an increase in their access to health care (25,26), detecting corresponding increases in the receipt of preventive care has proved more elusive. As of 2019, 6.1% of adults with diabetes had not received any of the six preventive services, and this percentage was 8.2% in 2020 during the onset of the COVID-19 pandemic. Continued monitoring will help to understand the extent to which the pandemic interrupted preventive care service utilization.
Two studies that used data from BRFSS found no changes overall in the receipt of preventive care for adults with diabetes resulting from Medicaid expansion between 2014 and 2019 (11,12). Similarly, the majority of subgroups in these studies exhibited no change in or decreased receipt of these six preventive services. The subgroup trends we observed suggest disparities in diabetes care that have been shown in other research. Consistent with our findings, studies using NHANES data for 2005–2018 as well as BRFSS for 2004–2014 both found that younger adults with diabetes were less likely to report receiving various recommended preventive care services (13,27). Additionally, lack of insurance was a barrier to preventive care, as uninsured adults also reported lower rates of preventive care in these studies (13,27). In our study, dental visits decreased over the study period but dilated eye exams increased among the uninsured. Education has also been linked to meeting recommendations for preventive care; adults with lower education consistently report lower rates of prevention (13,15). We found that adults with less than a high school education had decreasing trends in cholesterol testing and frequently were less likely to report visiting the dentist at least once than adults with more education, although this difference was not always statistically significant. Future research may wish to examine those adults with diabetes who reported receiving none of the six preventive care services, and factors contributing to this lack of care. While the confidence intervals for the estimates from 2008 and 2019/2020 overlap, the increase highlights the sustained suboptimal preventive care for a subset of adults with diabetes.
A1C testing and influenza vaccinations were the only two preventive services that showed increases either among the overall population or various subgroups which may be linked with the increase in health care service usage (25). A1C increased among: adults age 45 – 65, 65 – 74, > 75 years, Hispanic adults, non-Hispanic White adults, adults on Medicare only, and adults in the > 400% poverty income ratio group. Influenza vaccination increased among: non-Hispanic White adults, adult females, adult males, adults in the 200% – 399% poverty income ratio group, and adults in the > 400% poverty income ratio group. These services can be administered at the point-of-care during regular physician visits, whereas a dilated eye exam or dental visit require separate appointments. Lack of access to specialists, limited provider acceptance of public insurance options like Medicare, and inadequate care coordination may further complicate access to dilated eye exams or dentist visits and may explain why, for most groups, we observed no change or a decrease in the receipt of these services (15,28,29).
Other studies on trends in preventive care using different data sources report some conflicting findings. A study using NHANES data from 2005 to 2018 found increases in the proportion of adults with diabetes who reported all of the following: having a primary care doctor, receiving an annual check-up with a physician, having had at least two A1C tests in a year, having their cholesterol levels tested, and having an annual foot exam by a doctor (13). However, when evaluated individually, only A1C testing increased, which is similar to our findings. Another study that reported on data from NHANES, NHIS, and BRFSS found that foot exams, influenza vaccinations, and two or more A1C tests in a year increased from 1999 to 2016, although dilated eye exams stayed roughly constant (14). Data from BRFSS showed that adults with diabetes had reported decreasing dentist visits from 2004 to 2014 (27), while patient-reported dilated eye examinations increased briefly following Medicaid expansion in 2014 and then decreased (28). In contrast, a study using NHANES data found that dilated eye exams for adults with diabetes did not increase from 2005 to 2016 (15). A study using NHIS data reported no change in influenza vaccination rates from 2007 to 2018 for the overall population of adults with diabetes (30). Our finding that A1C testing increased is consistent with what has been reported in other studies. Discrepancies with other survey results may be due to differences in how questions are phrased, differences in the population being surveyed and trend analysis of time periods of different length. Caution should be used when interpreting these differences; when possible, trends should be compared over similar and longer time periods (31,32).
Limitations
The responses from MEPS were self-reported which may introduce bias. The study group was also cross-sectional and does not provide insight into how past receipt of preventive services may affect future receipt. In 2013, MEPS implemented efforts to improve collection of complete information by using field interviewers, with the goal of improving under reporting. This effort may have improved data quality after 2014 and could have impacted our trend analyses.
We are unable to identify factors that are causally linked to the changes in trends. Additionally, there has been a steadily declining response rate for both MEPS and DCS. During the studied time period both MEPS and DCS response rates peaked in 2008 at 59.3% and 92.4%, respectively, fell to 39.5% and 65.8%, respectively, in 2019, and fell further to 27.6% and 57.1%, respectively, in 2020. Although weights for these data were adjusted for non-response, the direction of bias due to non-response cannot be known. Furthermore, we were unable to distinguish between type 1 and type 2 diabetes in these data. Because of the greater proportion of type 2 diabetes (90% – 95%), the trends we report likely are more reflective of type 2 diabetes than type 1 diabetes.
Conclusions
In summary, with the exception of influenza vaccination, the overall receipt of preventive care for diabetes from 2008 to 2019 was flat. The trend pattern in subgroups was heterogeneous. This work highlights services and subgroups with low or declining receipt of these services that could be targeted to improve preventive care. Declining trends in preventive care may lead to increased diabetes complications, thereby increasing morbidity as well as cost of diabetes care.
Supplementary Material
Article Highlights.
We reported trends in receipt of six American Diabetes Association recommended preventive care services during 2008–2020.
The preventive services we evaluated were dental examinations, a dilated eye examination, a foot examination by a healthcare provider, ≥2 A1C tests, a blood cholesterol test, and an influenza vaccine.
From 2008 to 2019, overall trends in preventive services among U.S. adults with diabetes were stable except for an increase in the receipt of influenza vaccines.
These data highlight services and specific subgroups that could be targeted to improve preventive care among adults with diabetes.
Footnotes
Conflict of Interest: The authors of this study declare no conflicts of interest.
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
- 1.Centers for Disease Control and Prevention. National diabetes statistics report website [Internet]. Published 2022. [cited 2023 Jan 31]. Available from: https://www.cdc.gov/diabetes/data/statistics-report/index.html [Google Scholar]
- 2.American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care. 2018. Mar 22;41(5):917–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lin J, Thompson TJ, Cheng YJ, Zhuo X, Zhang P, Gregg E, et al. Projection of the future diabetes burden in the United States through 2060. Popul Health Metr. 2018. Jun 15;16(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Centers for Disease Control and Prevention. United States diabetes surveillance system [Internet]. Published 2022. [cited 2023 Jan 31]. Available from: https://gis.cdc.gov/grasp/diabetes/diabetesatlas.html [Google Scholar]
- 5.Magliano DJ, Islam RM, Barr ELM, Gregg EW, Pavkov ME, Harding JL, et al. Trends in incidence of total or type 2 diabetes: Systematic review. BMJ. 2019. Sep 11;l5003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zhang Y, Bullard KM, Imperatore G, Holliday CS, Benoit SR. Proportions and trends of adult hospitalizations with diabetes, United States, 2000-2018. Diabetes Res Clin Pract. 2022. May;187:109862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. Introduction and Methodology: Standards of Care in Diabetes2023. Diabetes Care. 2022. Dec 12;46(Supplement_1):S1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fowler MJ. Microvascular and Macrovascular Complications of Diabetes. Clinical Diabetes. 2008. Apr 1;26(2):77–82. [Google Scholar]
- 9.Kent D, D’Eramo Melkus G, Stuart P“M”W, McKoy JM, Urbanski P, Boren SA, et al. Reducing the Risks of Diabetes Complications Through Diabetes Self-Management Education and Support. Popul Health Manag. 2013. Apr;16(2):74–81. [DOI] [PubMed] [Google Scholar]
- 10.Gregg EW, Li Y, Wang J, Rios Burrows N, Ali MK, Rolka D, et al. Changes in Diabetes-Related Complications in the United States, 19902010. New England Journal of Medicine. 2014. Apr 17;370(16):1514–23. [DOI] [PubMed] [Google Scholar]
- 11.Monnette A, Stoecker C, Nauman E, Shi L. The impact of Medicaid expansion on access to care and preventive care for adults with diabetes and depression. J Diabetes Complications. 2020. Oct;34(10):107663. [DOI] [PubMed] [Google Scholar]
- 12.Luo H, Chen ZA, Xu L, Bell RA. Health care access and receipt of clinical diabetes preventive care for working-age adults With diabetes in states with and without Medicaid expansion: Results from the 2013 and 2015 BRFSS. Journal of Public Health Management and Practice. 2019. Jul;25(4):E34–43. [DOI] [PubMed] [Google Scholar]
- 13.Shin JI, Wang D, Daya N, Grams ME, Golden SH, Rajpathak S, et al. Trends in receipt of American Diabetes Association guideline-recommended care among U.S. adults with diabetes: NHANES 2005-2018. Diabetes Care. 2021. Apr 16;44(6):1300–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fang M. Trends in diabetes management among US adults: 1999-2016. J Gen Intern Med. 2020. Jan 2;35(5):1427–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Eppley SE, Mansberger SL, Ramanathan S, Lowry EA. Characteristics associated with adherence to annual dilated eye examinations among US patients with diagnosed diabetes. Ophthalmology. 2019. Nov;126(11):1492–9. [DOI] [PubMed] [Google Scholar]
- 16.Agency for Healthcare Research and Quality. MEPS HC-224 2020 full year consolidated data file documentation [Internet]. 2022. Available from: https://meps.ahrq.gov/mepsweb/data_stats/download_data_files_detail.jsp?cboPufNumber=HC-224 [Google Scholar]
- 17.American Diabetes Association. Comprehensive medical evaluation and assessment of comorbidities: Standards of Medical Care in Diabetes—2021. Vol. 44, Diabetes Care. 2022. p. S40–52. [DOI] [PubMed] [Google Scholar]
- 18.Parker J, Talih M, Malec DJ, Beresovsky V, Carroll MD, Gonzalez JF, et al. National Center for Health Statistics data presentation standards for proportions. National Center for Health Statistics. Vital Health Stat [Internet]. 2017. [cited 2023 Jun 12];2. Available from: https://www.cdc.gov/nchs/data/series/sr_02/sr02_175.pdf [PubMed] [Google Scholar]
- 19.Sjoberg DD, Whiting K, Curry M, Lavery JA, Larmarange J. Reproducible summary tables with the gtsummary package. The R Journal. 2021;13:570–80. [Google Scholar]
- 20.R Core Team. R: A language and environment for statistical computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2022. Available from: https://www.R-project.org/ [Google Scholar]
- 21.Cantor J, Sood N, Bravata DM, Pera M, Whaley C. The impact of the COVID-19 pandemic and policy response on health care utilization: Evidence from county-level medical claims and cellphone data. J Health Econ. 2022. Mar;82:102581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute. Joinpoint regression program. 2022. [Google Scholar]
- 23.Chaltiel D. Nih.joinpoint: R interface for NIH’s joinpoint regression software [Internet]. 2022. Available from: https://github.com/DanChaltiel/nih.joinpoint/ [Google Scholar]
- 24.Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–51. [DOI] [PubMed] [Google Scholar]
- 25.Myerson R, Romley J, Chiou T, Peters AL, Goldman D. The Affordable Care Act and health insurance coverage among people with diagnosed and undiagnosed diabetes: Data from the National Health and Nutrition Examination Survey. Diabetes Care. 2019. Sep 23;42(11):e179–80. [DOI] [PubMed] [Google Scholar]
- 26.Simon K, Soni A, Cawley J. The impact of health insurance on preventive care and health behaviors: Evidence from the first two years of the ACA Medicaid expansions. Journal of Policy Analysis and Management. 2017. Jan 16;36(2):390–417. [DOI] [PubMed] [Google Scholar]
- 27.Luo H, Bell RA, Wright W, Wu Q, Wu B. Trends in annual dental visits among US dentate adults with and without self-reported diabetes and prediabetes, 2004-2014. The Journal of the American Dental Association. 2018. Jun;149(6):460–9. [DOI] [PubMed] [Google Scholar]
- 28.Chen EM, Armstrong GW, Cox JT, Wu DM, Hoover DR, Del Priore LV, et al. Association of the Affordable Care Act Medicaid expansion with dilated eye examinations among the United States population with diabetes. Ophthalmology. 2020. Jul;127(7):920–8. [DOI] [PubMed] [Google Scholar]
- 29.Fathy C, Patel S, Sternberg P, Kohanim S. Disparities in adherence to screening guidelines for diabetic retinopathy in the United States: A comprehensive review and guide for future directions. Semin Ophthalmol. 2016. Apr 26;31(4):364–77. [DOI] [PubMed] [Google Scholar]
- 30.Hung MC, Lu P, Srivastav A, Cheng YJ, Williams WW. Influenza vaccination coverage among adults with diabetes, United States, 2007–08 through 2017–18 seasons. Vaccine. 2020. Sep;38(42):6545–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cusser S, Helms J, Bahlai CA, Haddad NM. How long do population level field experiments need to be? Utilising data from the 40-year-old LTER network. Ecol Lett. 2021. Feb 22;24(5):1103–11. [DOI] [PubMed] [Google Scholar]
- 32.Bahlai CA, White ER, Perrone JD, Cusser S, Stack Whitney K. The broken window: An algorithm for quantifying and characterizing misleading trajectories in ecological processes. Ecological Informatics. 2021. Sep;64:101336. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.