

Abstract
Androgen deprivation therapy (ADT) forms the cornerstone of treatment in locally-advanced and metastatic prostate cancer (PCa). Since the growth hormone-insulin like growth factor (GH-IGF-1) axis has been implicated in prostate tumorigenesis, we aimed to evaluate the association between IGF-1 and its binding proteins on outcomes in men with metastatic PCa treated with ADT, with or without docetaxel (D). We analyzed serum samples for IGF-1 and its family proteins from baseline, 6 months post-randomization and at the time of progression in men enrolled to receive ADT +/− D in the phase 3 CHAARTED trial. The key outcomes were time to development of castrate-resistant prostate cancer and overall survival (OS). 560 patients had samples available for analysis. At 6 months, significant increases in IGF-BP1 (mean Δ+27.4%, p=0.033), IGF-BP 3 (mean Δ +10.3%, p<0.001) and IGF-BP4 (mean Δ +31.1%, p<0.001) were seen in the ADT+D group, while the ADT group showed an increase in IGF-BP3 (mean Δ +5.5%, p=0.015). A higher IGF-1:IGF-BP1 ratio at baseline and after 6 months was associated with improved OS in both the ADT (baseline: HR=0.77, p=0.026; 6 months: HR=0.83, p=0.036) and ADT+D groups (baseline: HR=0.78, p=0.04; 6 months: HR=0.81, p=0.018). Patients with a log10IGF-1:IGF-BP1 ratio >1.3 at baseline had improved OS when meta-analyzed with data from a prior cohort (HR=0.71). Higher baseline and 6-month IGF-1:IGF-BP1 ratio was associated with better OS. Further exploration of the IGF-1 axis will be important to assess its role as a predictive biomarker and to target this axis in therapeutic trials.
Keywords: Androgen deprivation therapy, chemotherapy, metabolism, IGF-1, IGF-BP1
INTRODUCTION
Androgen deprivation therapy (ADT) (i.e. testosterone suppression) either medically, with LHRH and GnRH agonists or antagonists, or surgically, with bilateral orchiectomy, forms the cornerstone of management of advanced prostate cancer (PCa). In men with metastatic disease, ADT is typically continued indefinitely, with duration of therapy lasting up to several years based on data from contemporary clinical trials.(Sweeney et al., 2015, James et al., 2017, Davis et al., 2019) The natural history of advanced PCa is development of castrate-resistance (CRPC) after an initial clinical and biochemical response to ADT in most patients.
There is a large body of evidence suggesting that the growth hormone-insulin like growth factor 1 (GH-IGF-1) axis is involved in the development of a variety of solid cancers, including PCa.(Pollak, 2012) Preclinical data has shown that IGF-1 stimulates growth of PCa cell lines via activation of the MAPK and PI3K pathways.(DiGiovanni et al., 2000) Epidemiologic data have demonstrated an association between higher circulating IGF-1 levels and an increased risk of incident PCa.(Qian and Huo, 2020) Similarly, patients with acromegaly have a higher risk of developing prostate enlargement and PCa, with some data showing increased PCa mortality.(Watts et al., 2020) We have previously shown that increased serum concentrations of IGF-BP1 at baseline are associated with shorter time to CRPC and poorer OS in men receiving ADT for metastatic PCa.(Sharma et al., 2014a) Despite these data implicating an important role for IGF-1 signaling in PCa, clinical trials evaluating IGF-1R antagonists have not demonstrated a significant survival benefit in men receiving ADT for metastatic PCa, although these men were not enrolled based on levels of serum IGF-1 or those of its binding proteins at baseline.(Yu et al., 2015, Barata et al., 2018)
Systematic study of the prognostic impact of baseline (pre-ADT) levels of circulating members of the IGF family in men receiving ADT for metastatic PCa as well as how these markers change during ADT is lacking. The former would be helpful in identifying PCa patients whose cancer may behave aggressively, and who may therefore potentially benefit from upfront treatment intensification beyond ADT alone.(Riaz et al., 2023) Similarly, changes in these biomarkers could provide insights into the biologic underpinnings of IGF-mediated disease. In this regard, we evaluated serum concentrations of members of the IGF family at baseline, 6 months into therapy, and at progression in men receiving ADT, with or without docetaxel, on the ECOG-ACRIN E3805 CHAARTED trial (NCT00309985). This seminal trial demonstrated a significant OS benefit with addition of upfront docetaxel chemotherapy to ADT in men with mHSPC who had a high volume of metastatic disease.(Sweeney et al., 2015, Kyriakopoulos et al., 2018) The secondary analyses presented here provided an ideal opportunity to assess the impact of these biomarkers on the role of development of CRPC and OS.
PATIENTS AND METHODS
Study design and participants
The CHAARTED trial enrolled patients with metastatic PCa (either arising de novo or after prior local therapy, in a synchronous or metachronous fashion) and randomized them 1:1 to either ADT alone or ADT with 6 cycles of docetaxel (given every 3 weeks). A total of 790 patients were enrolled between 2006–2012 across centers in the United States. The trial demonstrated a significant benefit in OS – the primary endpoint – with the addition of upfront docetaxel to ADT, with the benefit most evident in men with high-volume metastatic PCa (i.e. 4 or more bone lesions with ≥1 outside the axial skeleton, and/or presence of visceral lesions).(Sweeney et al., 2015, Kyriakopoulos et al., 2018)
The study group used for this analysis comprised of trial patients who had serum samples available at one or more of the following time points: (i) baseline (before or within 28 days of starting ADT +/− docetaxel), (ii) after 6 months of therapy with ADT +/− docetaxel, and (iii) at the time of progression on therapy with ADT +/− docetaxel.
Procedures
Baseline clinical and demographic data at ADT +/− docetaxel initiation, including age, PSA, BMI, extent of metastases (high versus low, per CHAARTED volume criteria) and synchronous versus metachronous presentation of metastatic disease, were collected. The key outcomes captured included time to development of castrate-resistant prostate cancer (TT-CRPC) and overall survival (OS). The Fichorova laboratory at Brigham & Women’s Hospital assessed serum biomarker levels as previously described.(Sharma et al., 2014a, Sharma et al., 2014b) IGF-1 and IGF-R1 were measured by ELISA (R&D Systems, Minneapolis, MN), and IGF-BP1, IGF-BP3, and IGF-BP4 were measured by a Luminex 3-plex (R&D Systems Bio-Techne, Minneapolis, MN). Samples were collected from patients enrolled in CHAARTED who provided consent for collection and storage of blood for future studies. The Dana-Farber/Harvard Cancer Center Institutional Review Board reviewed and approved the work conducted as part of this manuscript with waiver of consent (#16–137).
Statistical analyses
Serum biomarker levels were measured as continuous variables. Paired Wilcoxon signed rank test was performed to test the change in serum biomarker levels between baseline and 6 months, and between 6 months and at progression. For each serum biomarker, Cox proportional hazards models were used to examine the association between biomarker levels and time-to-event outcomes (TT-CRPC and OS). For the association between 6-month biomarker levels and time-to-event outcomes, patients with events occurring before the 6-month time point were excluded. To fit the Cox model, biomarkers with skewed distributions (IGF-BP1) were first logged (base 10). Biomarker levels were then standardized by subtracting the mean and divided by the standard deviation for each biomarker across time points. The ratio of biomarkers IGF-1 and IGF-BP1 was calculated using the natural scale and then logged (natural log) before fitting the Cox model. Ratios were evaluated in an attempt to normalize IGF-1 to IGF-BP1 levels given the interplay between the two proteins. Meta-analysis was performed using the fixed-effects method with inverse-variance weights.
RESULTS
Baseline characteristics
Overall, 560 patients (of the 790 enrolled in the trial) had samples available for analysis at baseline, after 6 months of therapy and/or at time of progression, and these patients formed the analytical cohort (Table 1). 72 patients had samples available at all 3 timepoints. Men randomized to ADT and docetaxel (ADT+D) were slightly older than those receiving ADT alone (median: 64 vs. 62 years, p=0.037), but there were no other major differences in disease or patient characteristics between the two groups. There were also no major differences in baseline characteristics between our analytical cohort (n=560) and the remaining 230 men enrolled whose samples were not available, with the exception of a higher proportion of patients with ECOG performance status of 0 in the analytical cohort (Supplementary Table 1).
Table 1 –
Baseline characteristics of the analytical cohort
| Total (n=560) | ADT+D (n=283) | ADT (n=277) | p | |
|---|---|---|---|---|
| Age, median (range) | 63 (36–91) | 64 (36–88) | 62 (39–91) | 0.037 |
| Race (%) | 0.155 | |||
| White | 481 (86) | 250 (88) | 231 (83) | |
| Black | 52 (9) | 25 (9) | 27 (10) | |
| Asian | 9 (2) | 3 (1) | 6 (2) | |
| Unknown | 18 (3) | 5 (2) | 13 (5) | |
| ECOG PS (%) | 0.621 | |||
| 0 | 406 (73) | 204 (72) | 202 (73) | |
| 1 | 147 (26) | 77 (27) | 70 (25) | |
| 2 | 6 (1) | 2 (1) | 4 (1) | |
| Missing | 1 | 0 | 1 | |
| Baseline PSA, ng/mL, median (IQR) | 51 (12–277) | 51 (12–237) | 50 (13–311) | 0.445 |
| Gleason score (%) | 0.692 | |||
| 4–6 | 36 (7) | 19 (8) | 17 (7) | |
| 7 | 129 (26) | 68 (27) | 61 (25) | |
| 8 | 99 (20) | 53 (21) | 46 (19) | |
| 9–10 | 237 (47) | 113 (45) | 124 (50) | |
| Missing | 59 | 30 | 29 | |
| High-volume disease (%) | 352 (63) | 181 (64) | 171 (62) | 0.601 |
| Visceral metastasis (%) | 89 (25) | 40 (22) | 49 (29) | 0.177 |
| Prior local therapy (%) | 0.975 | |||
| None | 395 (71) | 201 (71) | 194 (70) | |
| RP | 117 (21) | 59 (21) | 58 (21) | |
| RT | 47 (8) | 23 (8) | 24 (9) | |
| Unknown/missing | 1 | 0 | 1 |
Abbreviations: ADT = androgen deprivation therapy; D = docetaxel; PS = performance status; RP = radical prostatectomy; RT = radiotherapy; PSA = prostate specific antigen’ IQR = interquartile range
Changes between baseline, 6 months and progression
Figure 1 shows boxplots of changes in markers between baseline, 6 months of therapy and progression in patients receiving ADT alone (Figure 1A, 1C) and ADT+D (Figure 1B, 1D). Significant increases in IGF-BP1 (mean Δ +27.4%, p=0.033), IGF-BP 3 (mean Δ +10.3%, p<0.001) and IGF-BP4 (mean Δ +31.1%, p<0.001) were seen in the ADT+D group, with an increase in IGF-BP3 (mean Δ +5.5%, p=0.015) also seen in the ADT group in the first 6 months. Numerical data for these changes in markers are provided in Supplementary Table 2. These trends were also particularly seen in patients with high-volume disease in both the ADT and ADT+D group (Supplementary Table 3).
Figure 1: Changes in markers between baseline and 6 months (1A, 1B), and between 6 months to progression (1C, 1D) in the ADT and ADT+D groups.
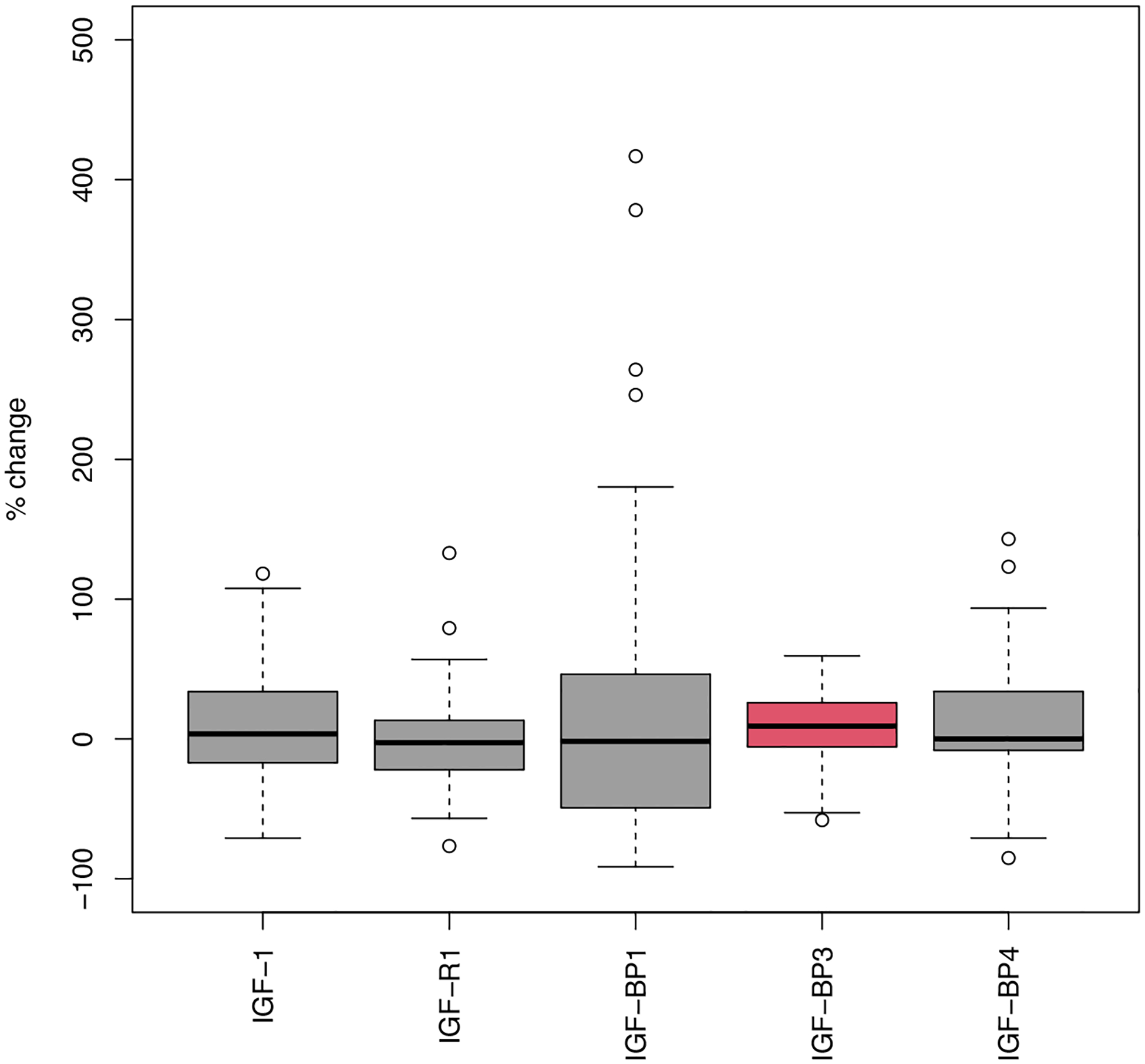
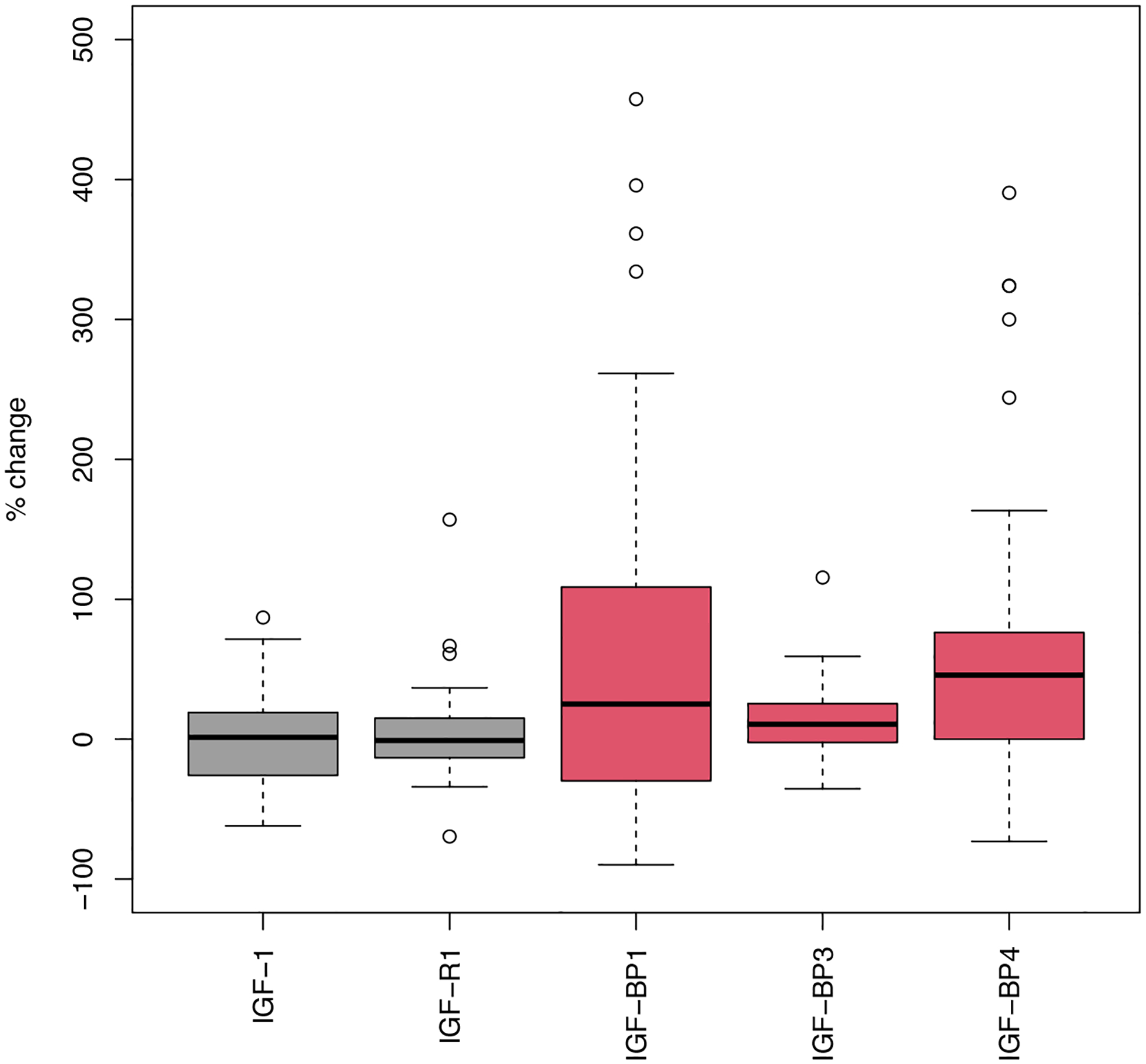
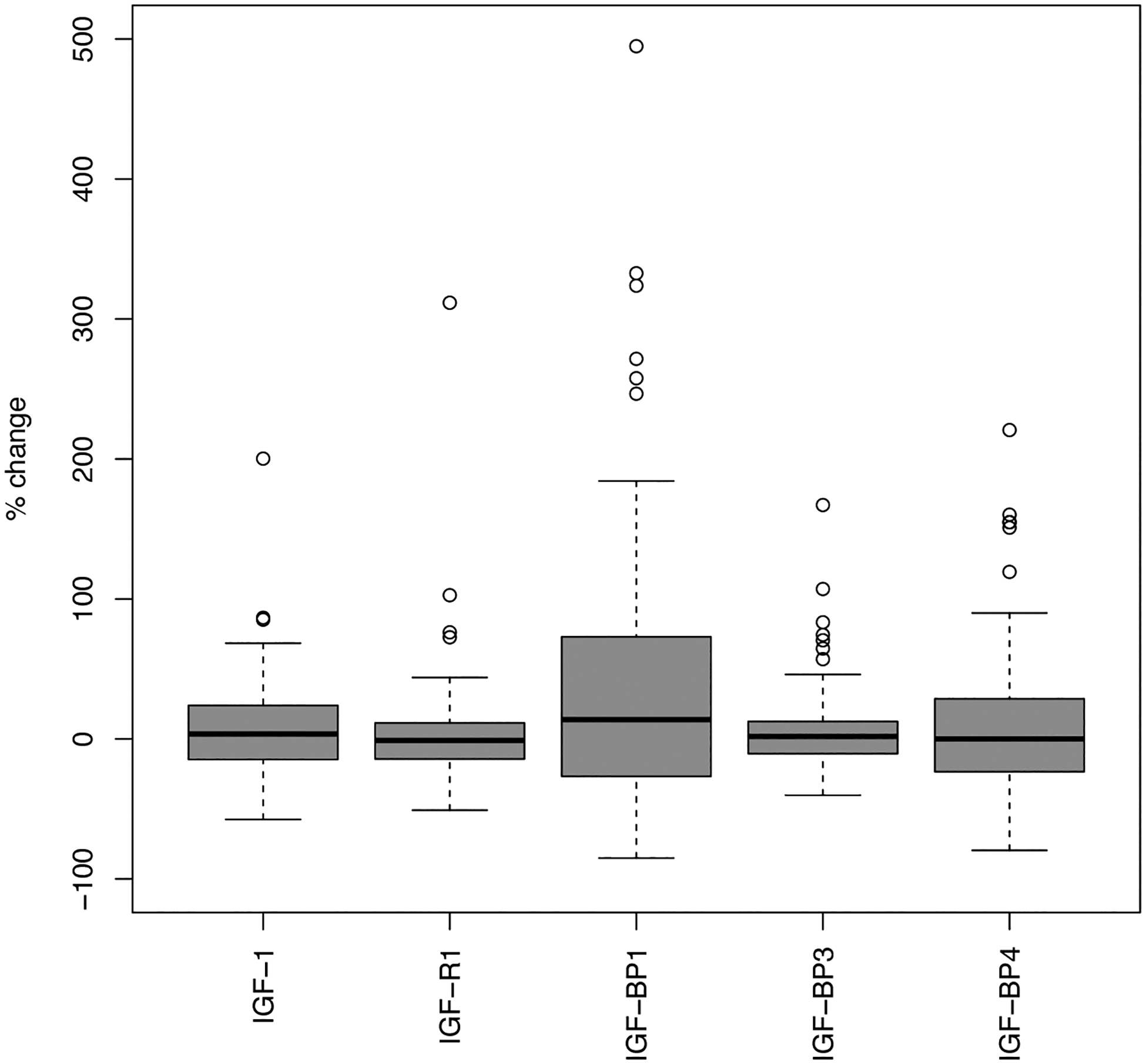
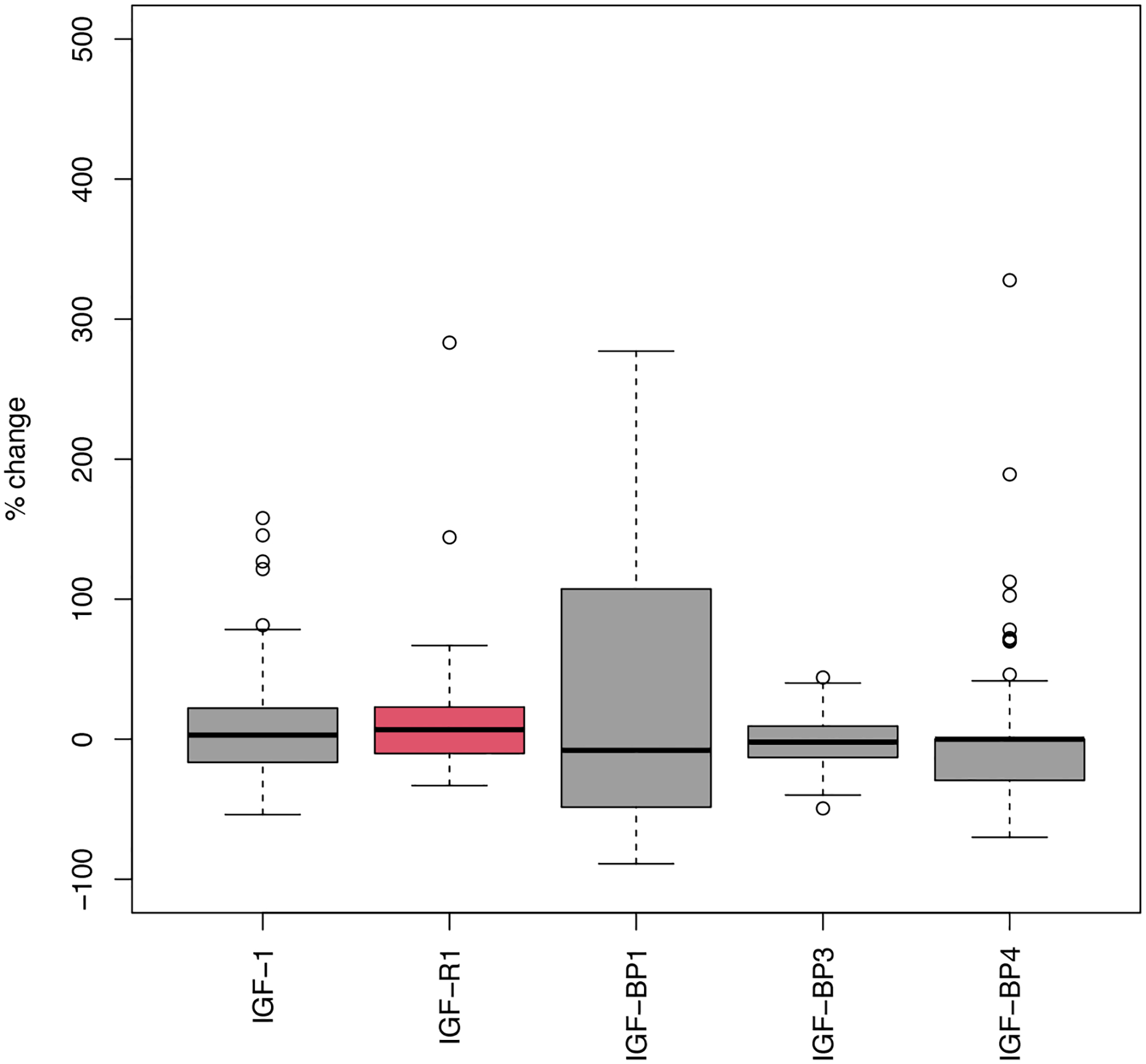
Red indicates significant p-value (<0.05). For the baseline and 6 month comparison, a total of 67 and 75 patients in the ADT and ADT+D groups respectively had serum samples available at both timepoints. For the 6 month and progression comparison, 67 and 73 patients in the ADT and ADT+D groups respectively had samples available at both timepoints. Abbreviations: ADT = androgen deprivation therapy; D = docetaxel.
Between 6 months and progression, there were no significant changes in any of the markers in the ADT group, while IGF-R1 levels (mean Δ +10.0%, p=0.020) increased significantly in the ADT+D group (Supplementary Table 4).
Prognostic impact of baseline IGF-1 system
The associations between continuous baseline marker levels and TT-CRPC and OS on univariable analysis, for each treatment arm, are shown in Table 2. Higher baseline levels of IGF-BP4 were associated with shorter TT-CRPC (HR=1.32, p=0.011) and poorer OS (HR=1.34, p=0.017) in patients receiving ADT, as well as ADT+D (time to CRPC: HR=1.36, p=0.020; OS: HR=1.48, p=0.006). A higher IGF-1:IGF-BP1 ratio was associated with improved OS in patients receiving ADT (HR=0.77, p=0.026) as well as ADT+D (HR=0.78, p=0.047). Higher IGF-BP1 was also associated with poorer OS (HR=1.27, p=0.045) amongst patients receiving ADT but not ADT+D (HR=1.23, p=0.124), while higher IGF-R1 was also associated with worse OS in patients receiving ADT (HR=1.36, p=0.013).
Table 2 –
Associations between continuous baseline marker levels and TT-CRPC and OS
| Marker* | TT-CRPC | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| ADT (N=116) | ADT+D (N=117) | ADT (N=116) | ADT+D (N=117) | |||||
| HR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P | |
| IGF-1 | 0.96 (0.77–1.20) | 0.723 | 0.95 (0.73–1.24) | 0.702 | 0.92 (0.70–1.20) | 0.520 | 0.91 (0.68–1.22) | 0.527 |
| IGF-R1 | 1.11 (0.91–1.36) | 0.288 | 1.18 (0.83–1.67) | 0.365 | 1.36 (1.07–1.73) | 0.013 | 1.22 (0.82–1.82) | 0.335 |
| IGF-BP1 | 1.09 (0.88–1.35) | 0.423 | 1.15 (0.90–1.47) | 0.262 | 1.27 (1.01–1.61) | 0.045 | 1.23 (0.95–1.60) | 0.124 |
| IGF-BP3 | 0.96 (0.75–1.23) | 0.738 | 1.10 (0.88–1.38) | 0.406 | 0.89 (0.66–1.19) | 0.427 | 1.04 (0.80–1.37) | 0.760 |
| IGF-BP4 | 1.32 (1.07–1.64) | 0.011 | 1.36 (1.05–1.75) | 0.020 | 1.34 (1.05–1.70) | 0.017 | 1.48 (1.12–1.95) | 0.006 |
| IGF-1/IGF-BP1* | 0.92 (0.75–1.12) | 0.384 | 0.85 (0.68–1.08) | 0.179 | 0.77 (0.62–0.97) | 0.026 | 0.78 (0.61–1.00) | 0.047 |
Abbreviations: HR = hazard ratio; ADT = androgen deprivation therapy; D = docetaxel; TT-CRPC = time to castrate-resistant prostate cancer; OS = overall survival
natural log of the ratio
Prognostic impact of 6-month IGF-1 system
Similar findings to baseline were seen when analyzing marker levels at 6 months and their associations with outcomes (Table 3). Higher levels of IGF-BP1 at 6 months were associated with poorer OS in patients receiving ADT (HR=1.27, p=0.014) and ADT+D (HR=1.30, p=0.013), while improved OS was seen in those with higher IGF-1:IGF-BP1 ratios at 6 months in patients receiving ADT alone (HR=0.83, p=0.036) and ADT+D (HR=0.81, p=0.018). Higher IGF-BP3 at 6 months was associated with improved OS in patients receiving ADT (HR=0.80, p=0.038) while higher IGF-BP4 levels at this timepoint were associated with poorer OS in those receiving ADT+D (HR=1.28, p=0.008).
Table 3 –
Associations between continuous marker levels at 6 months and TT-CRPC and OS
| Marker | TT-CRPC | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| ADT (N=164) | ADT+D (N=212) | ADT (N=199) | ADT+D (N=224) | |||||
| HR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P | HR (95% CI) | P | |
| IGF-1 | 1.07 (0.90–1.28) | 0.440 | 1.15 (0.95–1.40) | 0.139 | 1.06 (0.87–1.30) | 0.551 | 1.04 (0.83–1.30) | 0.757 |
| IGF-R1 | 0.98 (0.79–1.21) | 0.821 | 1.24 (0.96–1.59) | 0.095 | 1.22 (0.96–1.54) | 0.100 | 1.31 (0.99–1.74) | 0.056 |
| IGF-BP1 | 1.09 (0.91–1.30) | 0.360 | 1.06 (0.88–1.27) | 0.562 | 1.27 (1.05–1.54) | 0.014 | 1.30 (1.06–1.59) | 0.013 |
| IGF-BP3 | 0.91 (0.76–1.09) | 0.312 | 1.11 (0.96–1.30) | 0.167 | 0.80 (0.64–0.99) | 0.038 | 1.03 (0.86–1.23) | 0.734 |
| IGF-BP4 | 1.03 (0.84–1.26) | 0.804 | 1.13 (0.96–1.33) | 0.155 | 1.14 (0.90–1.43) | 0.277 | 1.28 (1.07–1.54) | 0.008 |
| IGF-1/IGF-BP1* | 0.95 (0.81–1.12) | 0.550 | 1.00 (0.85–1.17) | 0.973 | 0.83 (0.70–0.99) | 0.036 | 0.81 (0.68–0.96) | 0.018 |
Abbreviations: HR = hazard ratio; ADT = androgen deprivation therapy; D = docetaxel; TT-CRPC = time to castrate-resistant prostate cancer; OS = overall survival
natural log of the ratio
Prognostic impact of baseline IGF-1:IGF-BP1 ratio by tertile
Finally, we specifically assessed IGF-1:IGF-BP1 ratio by tertile and associations with TT-CRPC and OS. Across both the ADT and ADT+D groups, those in the upper two tertiles of IGF-1:IGF-BP1 ratio (i.e. ≥1.53) had significantly longer TT-CRPC (HR=0.73 [95% CI 0.53–1.00], p=0.046) and improved OS (HR=0.68 [0.48–0.98], p=0.035) compared to those in the lowest tertile (Figure 2). These trends were consistent when the ADT and ADT+D groups were analyzed separately (Supplementary Figure 1).
Figure 2: Kaplan-Meier curves of TT-CRPC (2A) and OS (2B) stratified by IGF-1:IGF-BP1 ratio tertile (lowest [T1] vs. upper two [T2/3]).
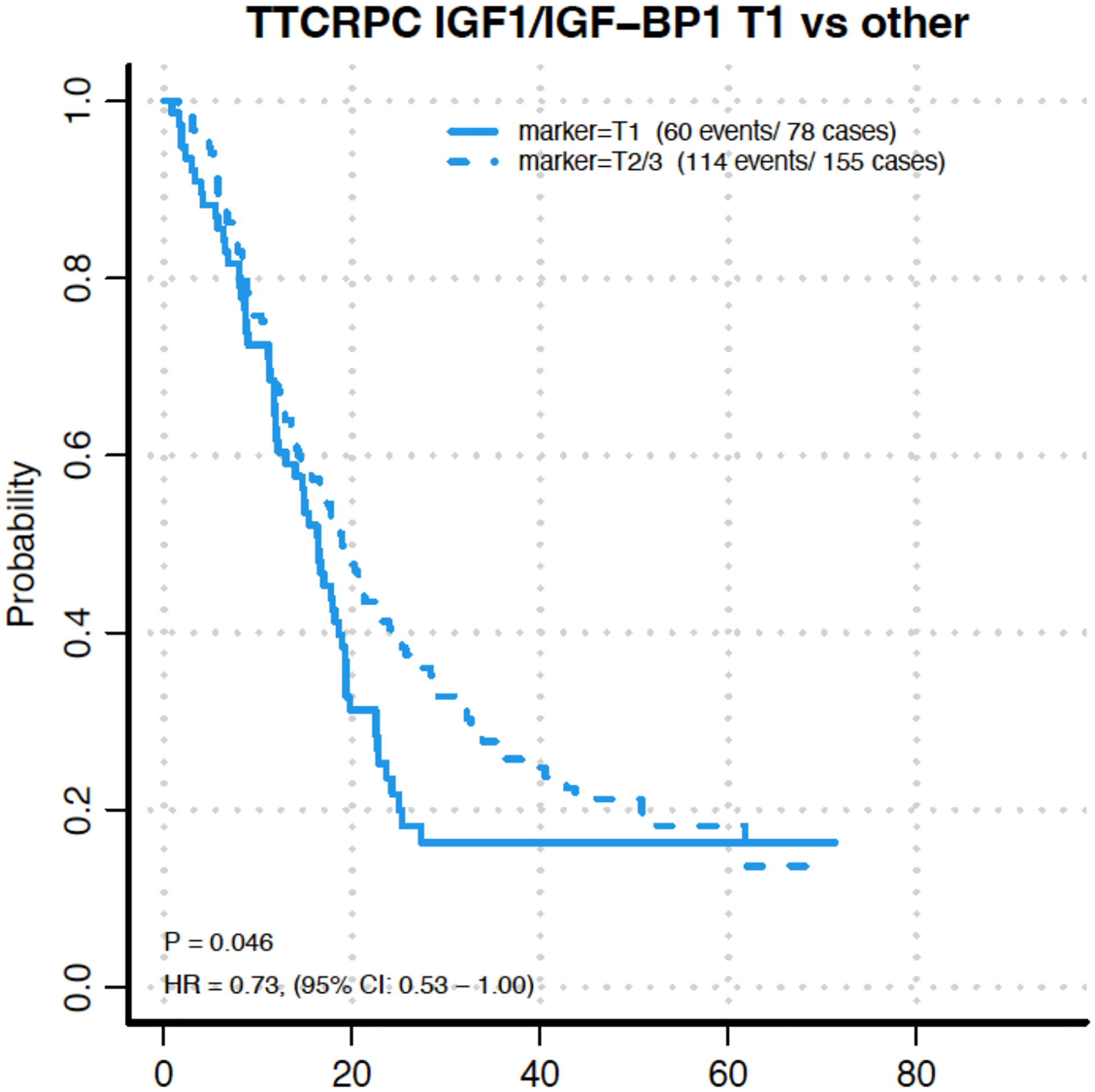
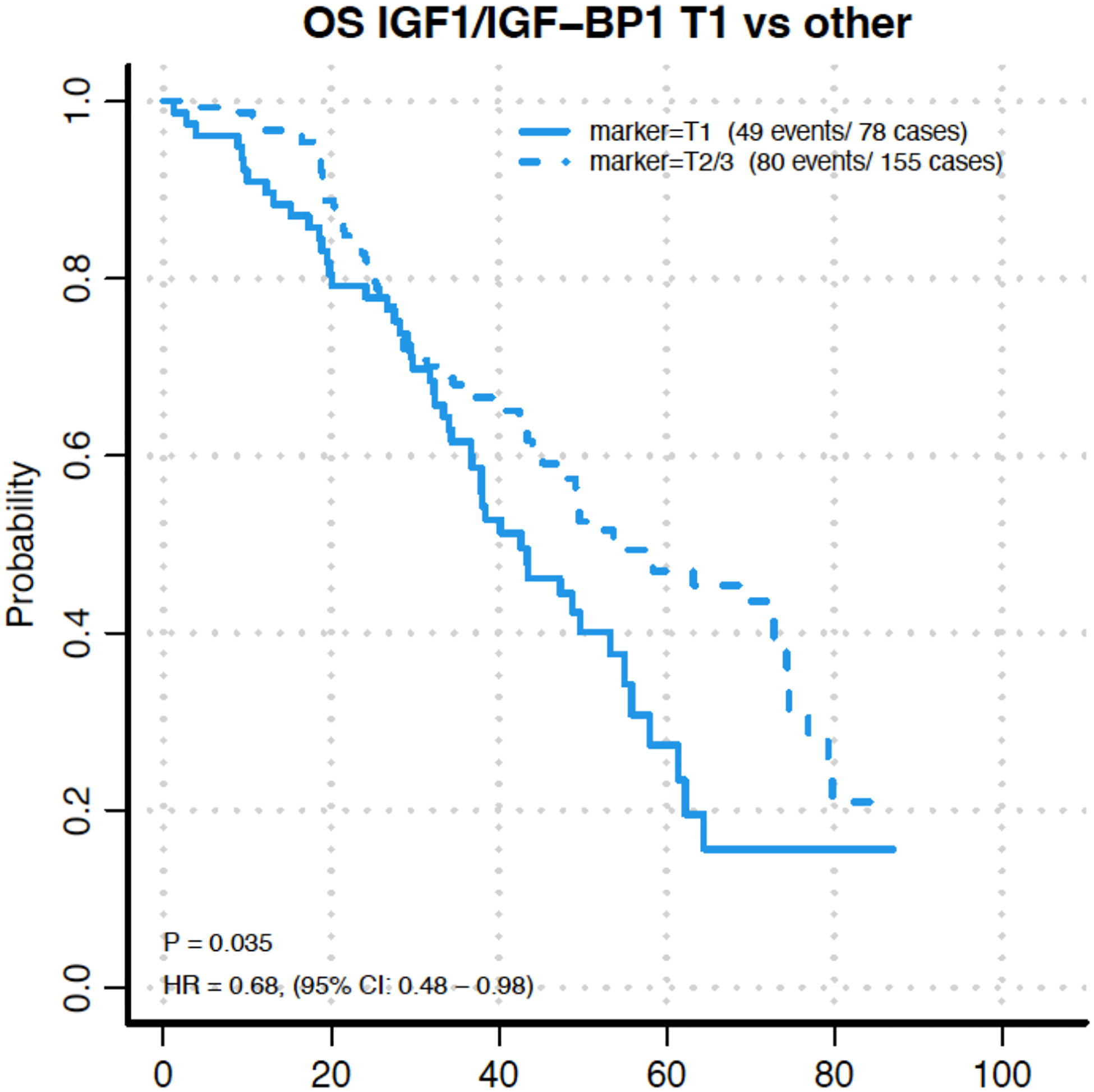
Abbreviations: TT-CRPC = time to castrate-resistant prostate cancer; OS = overall survival.
We additionally performed a meta-analysis combining our cohort with the previously reported data from our group(Sharma et al., 2014a) to evaluate the prognostic impact of IGF-1:IGF-BP1 tertile. When using the same tertile cut-point of 1.3 on the log10 scale for IGF-1:IGF-BP1 ratio from the prior study,(Sharma et al., 2014a) patients with a ratio of >1.3 at baseline had improved OS on meta-analysis (HR=0.71 [0.48–1.05]), with the hazard ratios from our data (E3805) and the prior study being almost identical (0.72 and 0.70 respectively, Figure 3).
Figure 3: Meta-analysis of impact of baseline IGF-1:IGF-BP1 ratio (<1.3 or ≥1.3 on log10 scale) on OS utilizing data from Sharma et al (Ref 5) and CHAARTED ADT cohorts (E3805).
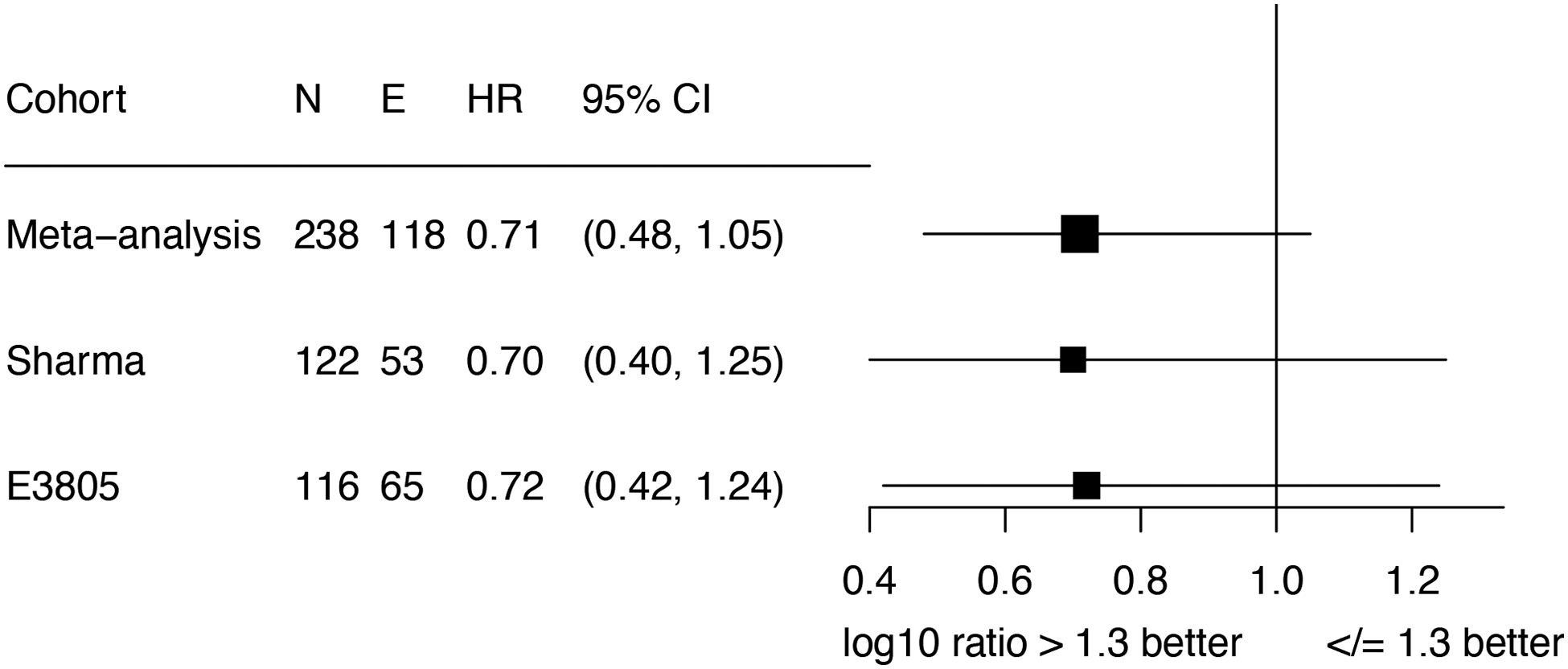
Abbreviations: HR = hazard ratio; E = events; CI = confidence interval. Meta-analysis was performed using the fixed effects method.
DISCUSSION
In this correlative analysis of the CHAARTED trial, we noted significant increases in IGF-BP1, IGF-BP3 and IGF-BP4 in the first 6 months of therapy in patients who received ADT and docetaxel, with IGF-BP3 levels increasing in the first 6 months in the ADT group. Baseline IGF-BP4 levels were prognostic for TT-CRPC and OS in both the ADT and ADT+D groups, while baseline IGF-BP1 was prognostic for OS amongst men receiving ADT, but not ADT+D. Notably, the baseline IGF-1:IGF-BP1 ratio was prognostic in both groups with a higher ratio being associated with improved outcomes. Intriguingly, we also validated that a log10 IGF-1:IGF-BP1 ratio >1.3 at baseline was prognostic for OS. These findings add to the literature on the IGF axis and outcomes in prostate cancer, and ours is the first study to evaluate these associations within the context of a large, phase 3 clinical trial as well as in patients receiving chemohormonal therapy and not ADT alone.
The relationship between the IGF peptides (IGF-1 and IGF-2) and IGF-BPs is complex.(Pollak, 2012) IGF-1 and IGF-2 bind to the IGF receptor family, with IGF-R1 signaling known to stimulate nuclear translocation of the androgen receptor (AR) and thereby promoting AR signaling.(Wu et al., 2006) The IGF peptides have a short life span in the circulation unless bound to IGF-BPs, which prolong the circulating half-life of IGFs and regulate their movement into tissues, and IGF-BPs may themselves stimulate cell growth through their own receptors.(Durai et al., 2006) Our finding that higher IGF-BP1 levels at baseline was prognostic for poorer OS among patients receiving ADT validates prior work in a retrospective cohort.(Sharma et al., 2014a) The lack of association between IGF-BP1 and OS in the ADT+D cohort may be due to the impact of docetaxel, which was shown to significantly improve outcomes when added to ADT in upfront treatment of mHSPC in the CHAARTED trial,(Sweeney et al., 2015) and therefore may abrogate any detrimental impact of IGF signaling via the AR.
Moreover, it is important to note that our results pertaining to the prognostic impact of baseline IGF-1:IGF-BP1 ratio by tertile are almost identical to that reported previously by our group when we evaluated marker levels in an observational cohort of mHSPC patients receiving ADT alone.(Sharma et al., 2014a) Our meta-analysis of tertile results at baseline confirmed almost identical hazard ratios for OS, with such cross-validation in different cohorts being extremely rare in biomarker work. Moreover, the prognostic impact of IGF-1:IGF-BP-1 ratio seemed stronger in patients receiving ADT alone. Further evaluation of this easily available blood-based biomarker as a means to select patients for treatment is therefore warranted, potentially to identify patients with mHSPC who most benefit from intensification of therapy, including with docetaxel and/or a novel hormonal agent in addition to ADT.(Smith et al., 2022, Fizazi et al., 2022) Additionally, this could be used to guide targeting of the IGF-R in mHSPC, particularly in patients who may have an inadequate PSA response to initial therapy since there is good data that patients with PSA >0.1 or >0.2 after ~6 months of ADT+D(Harshman et al., 2018) or ADT + abiraterone(Matsubara et al., 2020) have poorer survival. While previous efforts at targeting the IGF axis in PCa were not promising,(Yu et al., 2015, Barata et al., 2018) a biomarker-directed strategy (i.e. those with a low IGF1:IGFB1 ratio) may bear more fruit, given that elevated IGF-BP1 and lower IGF-1/IGF-BP1 ratios at 6 months were associated with poorer OS in both the ADT and ADT+D groups in our analyses.
The mechanism behind IGF-BP levels leading to poorer outcomes is unclear. It is possible that higher IGF-BP1 (and IGF-BP4) levels reflect greater transport of bound IGF peptides to tissues, including prostate cancer cells, thereby leading to increased IGF-R signaling and promoting tumor proliferation.(Pollak, 2012) However, we also found higher IGF-1:IGF-BP1 ratio was prognostic for a better OS and thus may reflect more IGF-1 levels potentially being more tightly bound to IGF-BPs with less free IGF-1 being delivered to tissue to support cancer cell survival. Alternatively, the higher ratio could mean higher free IGF-1 levels that are subject to degradation in the circulation, with less IGF-1 therefore delivered to tissues. Interestingly, while baseline IGF-1:IGF-BP1 ratio was prognostic for better OS in men receiving ADT+D, the levels of IGF-BP1 alone were not associated with OS in this group, suggesting that the balance between the levels of ligand and binding protein may be more important than the levels of either alone in determining extent of IGF-1 delivering and subsequent IGF-R signaling.
Though our analyses utilized correlative blood samples from men enrolled on a prospective clinical trial and was able to provide comparisons in markers between ADT and ADT+D, there are limitations that must be acknowledged. A limited number of patients (37 and 29 in the ADT and ADT+D groups respectively) had blood available at all 3 timepoints (baseline, 6 months and progression) which impeded our ability to track changes in these markers on an individual patient level. Furthermore, fasting blood samples were not required and it is possible that levels of some markers may be affected by food intake. We were unable to measure levels of IGF-BP2, which has shown prognostic value in an androgen-dependent manner in patients with localized prostate cancer,(Inman et al., 2005) due to constraints with adding this marker to a multiplex panel. Finally, baseline marker levels were drawn either before or within 28 days of starting ADT or ADT+D, and therefore may not reflect a true “baseline” value in those patients in whom it was drawn after starting therapy. However, complete testosterone suppression takes 2–4 weeks after starting ADT and it is likely that marker levels measured up to 28 days after starting therapy may not have a major impact on “baseline” values. We also acknowledge that the prognostic associations are based on descriptive univariate analyses with no correction for multiple testing since our goal was to report data to inform future evaluations to assess for reproducibility and therefore, our findings should be viewed as hypothesis-generating. As such, our work will guide the prospective biomarker analysis plan for evaluations of samples from the ENZAMET study, which evaluated the addition of enzalutamide to ADT (+/− docetaxel) in mHSPC.(Davis et al., 2019)
In summary, we leveraged the phase 3 randomized CHAARTED trial to evaluate serum levels of the IGF family at baseline and during ADT, with or without docetaxel. We validated the prognostic impact of baseline IGF-BP1 and IGF-1:IGF-BP1 ratio in men receiving ADT, while also demonstrating that the IGF-1:IGF-BP1 ratio is prognostic in men who received ADT+D. Additionally, this ratio was prognostic after 6 months of therapy as well in both groups, and the reproducibility of these findings suggest a possible role in using this ratio at baseline and/or after 6 months of therapy to identify patients for treatment intensification in mHSPC.
Supplementary Material
Funding:
Sanofi; NIH, Grant/Award Numbers: R01CA208254 (CJS). This study was coordinated by the ECOG-ACRIN Cancer Research Group (Peter J. O’Dwyer, MD and Mitchell D. Schnall, MD, PhD, Group Co-Chairs) and supported by the National Cancer Institute of the National Institutes of Health under award numbers: U10CA180820, U10CA180794, and UG1CA233180. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosures:
PR – Research funding (to institution): Lilly, Telix; VW – none; RNF – none; BAM – Consulting Fees: Astella, Bayer, Bristol Myers Squibb, Calithera, Dendreon, Exelixis, Ipsen, Pfizer, Seattle Genetics, Consulting Fees (Non-pharmaceutical): Aptitude Health, MJH, Targeted Oncology, OncLive, DAVA Oncology, Curio; Fees to institution: Bristol Myers Squibb, Calithera, Exelixis, Pfizer, Seattle Genetics; XXW – Research funding (to institution): Bristol Myers Squibb; Consulting: Novartis; SB – none; CJS – Research funding (to institution) from Janssen, Astellas, Sanofi, Bayer; Patents; Consulting, or Advisory Role: Sanofi, Janssen, Astellas, Bayer, Genentech/Roche, Pfizer, Lilly; CellCentric, PointBiopharma
REFERENCES
- BARATA P, COONEY M, TYLER A, WRIGHT J, DREICER R & GARCIA JA 2018. A phase 2 study of OSI-906 (linsitinib, an insulin-like growth factor receptor-1 inhibitor) in patients with asymptomatic or mildly symptomatic (non-opioid requiring) metastatic castrate resistant prostate cancer (CRPC). Invest New Drugs, 36, 451–457. [DOI] [PubMed] [Google Scholar]
- DAVIS ID, MARTIN AJ, STOCKLER MR, BEGBIE S, CHI KN, CHOWDHURY S, COSKINAS X, FRYDENBERG M, HAGUE WE, HORVATH LG, JOSHUA AM, LAWRENCE NJ, MARX G, MCCAFFREY J, MCDERMOTT R, MCJANNETT M, NORTH SA, PARNIS F, PARULEKAR W, POOK DW, REAUME MN, SANDHU SK, TAN A, TAN TH, THOMSON A, TU E, VERA-BADILLO F, WILLIAMS SG, YIP S, ZHANG AY, ZIELINSKI RR, SWEENEY CJ, INVESTIGATORS, E. T., THE, A., NEW ZEALAND, U. & PROSTATE CANCER TRIALS, G. 2019. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N Engl J Med, 381, 121–131. [DOI] [PubMed] [Google Scholar]
- DIGIOVANNI J, KIGUCHI K, FRIJHOFF A, WILKER E, BOL DK, BELTRAN L, MOATS S, RAMIREZ A, JORCANO J & CONTI C 2000. Deregulated expression of insulin-like growth factor 1 in prostate epithelium leads to neoplasia in transgenic mice. Proc Natl Acad Sci U S A, 97, 3455–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DURAI R, DAVIES M, YANG W, YANG SY, SEIFALIAN A, GOLDSPINK G & WINSLET M 2006. Biology of insulin-like growth factor binding protein-4 and its role in cancer (review). Int J Oncol, 28, 1317–25. [PubMed] [Google Scholar]
- FIZAZI K, FOULON S, CARLES J, ROUBAUD G, MCDERMOTT R, FLECHON A, TOMBAL B, SUPIOT S, BERTHOLD D, RONCHIN P, KACSO G, GRAVIS G, CALABRO F, BERDAH JF, HASBINI A, SILVA M, THIERY-VUILLEMIN A, LATORZEFF I, MOUREY L, LAGUERRE B, ABADIE-LACOURTOISIE S, MARTIN E, EL KOURI C, ESCANDE A, ROSELLO A, MAGNE N, SCHLURMANN F, PRIOU F, CHAND-FOUCHE ME, FREIXA SV, JAMALUDDIN M, RIEGER I, BOSSI A & INVESTIGATORS, P.−. 2022. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet, 399, 1695–1707. [DOI] [PubMed] [Google Scholar]
- HARSHMAN LC, CHEN YH, LIU G, CARDUCCI MA, JARRARD D, DREICER R, HAHN N, GARCIA JA, HUSSAIN M, SHEVRIN D, EISENBERGER M, KOHLI M, PLIMACK ER, COONEY M, VOGELZANG NJ, PICUS J, DIPAOLA R, SWEENEY CJ & INVESTIGATORS, E.-A. 2018. Seven-Month Prostate-Specific Antigen Is Prognostic in Metastatic Hormone-Sensitive Prostate Cancer Treated With Androgen Deprivation With or Without Docetaxel. J Clin Oncol, 36, 376–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- INMAN BA, HAREL F, AUDET JF, MEYER F, DOUVILLE P, FRADET Y & LACOMBE L 2005. Insulin-like growth factor binding protein 2: an androgen-dependent predictor of prostate cancer survival. Eur Urol, 47, 695–702. [DOI] [PubMed] [Google Scholar]
- JAMES ND, DE BONO JS, SPEARS MR, CLARKE NW, MASON MD, DEARNALEY DP, RITCHIE AWS, AMOS CL, GILSON C, JONES RJ, MATHESON D, MILLMAN R, ATTARD G, CHOWDHURY S, CROSS WR, GILLESSEN S, PARKER CC, RUSSELL JM, BERTHOLD DR, BRAWLEY C, ADAB F, AUNG S, BIRTLE AJ, BOWEN J, BROCK S, CHAKRABORTI P, FERGUSON C, GALE J, GRAY E, HINGORANI M, HOSKIN PJ, LESTER JF, MALIK ZI, MCKINNA F, MCPHAIL N, MONEY-KYRLE J, O’SULLIVAN J, PARIKH O, PROTHEROE A, ROBINSON A, SRIHARI NN, THOMAS C, WAGSTAFF J, WYLIE J, ZARKAR A, PARMAR MKB, SYDES MR & INVESTIGATORS, S. 2017. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N Engl J Med, 377, 338–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KYRIAKOPOULOS CE, CHEN YH, CARDUCCI MA, LIU G, JARRARD DF, HAHN NM, SHEVRIN DH, DREICER R, HUSSAIN M, EISENBERGER M, KOHLI M, PLIMACK ER, VOGELZANG NJ, PICUS J, COONEY MM, GARCIA JA, DIPAOLA RS & SWEENEY CJ 2018. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol, 36, 1080–1087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MATSUBARA N, CHI KN, OZGUROGLU M, RODRIGUEZ-ANTOLIN A, FEYERABEND S, FEIN L, ALEKSEEV BY, SULUR G, PROTHEROE A, LI S, MUNDLE S, DE PORRE P, TRAN N & FIZAZI K 2020. Correlation of Prostate-specific Antigen Kinetics with Overall Survival and Radiological Progression-free Survival in Metastatic Castration-sensitive Prostate Cancer Treated with Abiraterone Acetate plus Prednisone or Placebos Added to Androgen Deprivation Therapy: Post Hoc Analysis of Phase 3 LATITUDE Study. Eur Urol, 77, 494–500. [DOI] [PubMed] [Google Scholar]
- POLLAK M 2012. The insulin and insulin-like growth factor receptor family in neoplasia: an update. Nat Rev Cancer, 12, 159–69. [DOI] [PubMed] [Google Scholar]
- QIAN F & HUO D 2020. Circulating Insulin-Like Growth Factor-1 and Risk of Total and 19 Site-Specific Cancers: Cohort Study Analyses from the UK Biobank. Cancer Epidemiol Biomarkers Prev, 29, 2332–2342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- RIAZ IB, NAQVI SAA, HE H, ASGHAR N, SIDDIQI R, LIU H, SINGH P, CHILDS DS, RAVI P, HUSSAIN SA, MURAD MH, BOORJIAN SA, SWEENEY C, VAN ALLEN EM & BRYCE AH 2023. First-line Systemic Treatment Options for Metastatic Castration-Sensitive Prostate Cancer: A Living Systematic Review and Network Meta-analysis. JAMA Oncol. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SHARMA J, GRAY KP, EVAN C, NAKABAYASHI M, FICHOROVA R, RIDER J, MUCCI L, KANTOFF PW & SWEENEY CJ 2014a. Elevated insulin-like growth factor binding protein-1 (IGFBP-1) in men with metastatic prostate cancer starting androgen deprivation therapy (ADT) is associated with shorter time to castration resistance and overall survival. Prostate, 74, 225–34. [DOI] [PubMed] [Google Scholar]
- SHARMA J, GRAY KP, HARSHMAN LC, EVAN C, NAKABAYASHI M, FICHOROVA R, RIDER J, MUCCI L, KANTOFF PW & SWEENEY CJ 2014b. Elevated IL-8, TNF-alpha, and MCP-1 in men with metastatic prostate cancer starting androgen-deprivation therapy (ADT) are associated with shorter time to castration-resistance and overall survival. Prostate, 74, 820–8. [DOI] [PubMed] [Google Scholar]
- SMITH MR, HUSSAIN M, SAAD F, FIZAZI K, STERNBERG CN, CRAWFORD ED, KOPYLTSOV E, PARK CH, ALEKSEEV B, MONTESA-PINO A, YE D, PARNIS F, CRUZ F, TAMMELA TLJ, SUZUKI H, UTRIAINEN T, FU C, UEMURA M, MENDEZ-VIDAL MJ, MAUGHAN BL, JOENSUU H, THIELE S, LI R, KUSS I, TOMBAL B & INVESTIGATORS, A. T. 2022. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med, 386, 1132–1142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SWEENEY CJ, CHEN YH, CARDUCCI M, LIU G, JARRARD DF, EISENBERGER M, WONG YN, HAHN N, KOHLI M, COONEY MM, DREICER R, VOGELZANG NJ, PICUS J, SHEVRIN D, HUSSAIN M, GARCIA JA & DIPAOLA RS 2015. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med, 373, 737–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WATTS EL, GOLDACRE R, KEY TJ, ALLEN NE, TRAVIS RC & PEREZ-CORNAGO A 2020. Hormone-related diseases and prostate cancer: An English national record linkage study. Int J Cancer, 147, 803–810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WU JD, HAUGK K, WOODKE L, NELSON P, COLEMAN I & PLYMATE SR 2006. Interaction of IGF signaling and the androgen receptor in prostate cancer progression. J Cell Biochem, 99, 392–401. [DOI] [PubMed] [Google Scholar]
- YU EY, LI H, HIGANO CS, AGARWAL N, PAL SK, ALVA A, HEATH EI, LAM ET, GUPTA S, LILLY MB, INOUE Y, CHI KN, VOGELZANG NJ, QUINN DI, CHENG HH, PLYMATE SR, HUSSAIN M, TANGEN CM & THOMPSON IM JR. 2015. SWOG S0925: A Randomized Phase II Study of Androgen Deprivation Combined With Cixutumumab Versus Androgen Deprivation Alone in Patients With New Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol, 33, 1601–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.