

Abstract
Background
Recent evidences showed that resection of lung tumor post-targeted therapy has shown progression-free survival (PFS) benefits in initially unresectable patients. The aim of this study is to evaluate pathologic findings of resected lung tumor samples in patients who have undergone prior epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor (TKI) treatment, and also to assess the prognostic factors related to outcomes after resection.
Methods
The deidentified data of non-small cell lung cancer (NSCLC) patients admitted to seven university hospitals affiliated with the Catholic University of Korea were obtained from the Clinical Data Warehouse (CDW) database. Among screened patients, 40 individuals who had previously undergone targeted therapies and later received surgical resection of a primary lung tumor were evaluated for the study.
Results
All 40 patients were diagnosed with adenocarcinoma. Of these, 36 with EGFR mutations received prior EGFR TKI treatment. Only one postoperative complication, atrial fibrillation, was observed. At the time of resection, 19 patients showed primary lung tumor size regressing or unchanged, while 21 patients showed primary lung tumor regrowth or new lesions being developed before the resection. The group with no programmed death-ligand 1 (PD-L1) expression from resected samples showed significantly better post-resection PFS when compared to the other group (P=0.01). In the Model II multivariate analysis for post-resection PFS, PD-L1 detection from the resected sample was significantly associated with PFS [P=0.03; hazard ratio (HR) =5.465; 95% confidence interval (CI): 1.200–24.885]. Furthermore, an increase in PD-L1 expression compared to the baseline value was associated with an increasing lung tumor burden at the time of resection (P=0.03).
Conclusions
Resected specimen following targeted therapy can provide valuable clinical information that can be used to predict the prognosis of patients with initially unresectable NSCLC.
Keywords: Salvage surgery, adenocarcinoma, resection, epidermal growth factor receptor (EGFR), targeted therapy
Highlight box.
Key findings
• This study examined patients with initially unresectable non-small cell lung cancer (NSCLC) adenocarcinoma treated with targeted therapy, followed by surgery. Findings show minimal post-surgery complications, with programmed death-ligand 1 (PD-L1) negativity in resected samples indicating improved post-surgery progression-free survival (PFS).
• The study also identifies PD-L1 expression in resected samples as an independent predictor of PFS outcomes, and links longer epidermal growth factor receptor tyrosine kinase inhibitor (TKI) treatment duration (>12 months) and spread through air spaces to the detection of the T790M mutation.
What is known and what is new?
• Prior research has highlighted the benefits of lung tumor resection post-targeted therapy in enhancing PFS for initially unresectable NSCLC patients.
• PD-L1 expression, as determined by SP263 and 22C3 assays from the resected sample acquired after initial TKI treatment, was markedly different between groups with increasing and regressing/stable tumor burden at tumor resection. Notably, the group with increasing tumor burden showed a significantly higher percentage of patients with PD-L1 expression of 1% or more.
• Multivariate analyses highlighted the importance of several prognostic factors for PFS and overall survival post-resection. Notably, PD-L1 expression from resected was significant factors in these analyses.
What is the implication, and what should change now?
• In cases of initially unresectable NSCLC with a targetable mutation, considering later resection for a lung mass that has been downstaged after a response to targeted therapy, or resection of a regrowing lung mass, may provide valuable pathologic information for planning subsequent treatments.
Introduction
In patients with driver mutations such as epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) mutations, targeted therapies are used for unresectable, advanced, and metastatic non-small cell lung cancer (NSCLC) (1). For patients who show downstaging of lung cancer following targeted therapy, resection of lung tumor can be considered (2). There are advantages to salvage surgery in patients who underwent targeted therapy for initially unresectable NSCLC in terms of progression-free survival (PFS) (2,3).
However, another approach to lung tumor resection in initially unresectable NSCLC deserves attention. In patients with initially unresectable NSCLC with driver mutations, the lung tumor may regrow after a certain duration of sustained treatment response to targeted therapy, or new lung tumoral lesion may develop. In clinical settings where a pulmonary tumor regrows following initial treatment, performing resection of the regrown tumor serves two purposes. Firstly, it allows the acquisition of a sufficient amount of biopsy sample, which is vital for further molecular and histopathological analysis (4). Secondly, this surgical intervention helps reduce the tumor burden (5).
Furthermore, it would be clinically significant to assess the findings provided by surgically resected samples: the changes in the tumor microenvironment from the time of diagnosis to post-tyrosine kinase inhibitor (TKI) treatment, and the differences in resected tumor samples between patients whose primary tumors have decreased in size vs. those whose tumors have increased at the time of resection. Moreover, resected tumor samples after initial targeted therapy can provide valuable information for predicting outcomes after the resection.
The aim of this study is to evaluate the clinical value of pathologic findings of resected lung tumor samples in patients who have undergone prior EGFR and ALK TKI treatment, and also to assess the prognostic factors related to outcomes after resection. We present this article in accordance with the REMARK reporting checklist (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-215/rc).
Methods
Patient selection and data collection
The deidentified data of NSCLC patients admitted to seven university hospitals affiliated with the Catholic University of Korea were obtained from the Clinical Data Warehouse (CDW) database. A total of 369 patients who underwent lobectomy and targeted therapies including gefitinib, erlotinib, afatinib, dacomitinib, lazertinib, osimertinib, alectinib, lorlatinib, brigatinib, and crizotinib were screened for study eligibility. To ensure uniformity, patient inclusion and exclusion criteria were applied at a single time point using the CDW in order to minimize potential bias associated with an extended recruitment period. Among these patients, 40 individuals who had previously undergone targeted therapies and later received surgical resection of a primary lung tumor were evaluated for the study (Figure 1).
Figure 1.
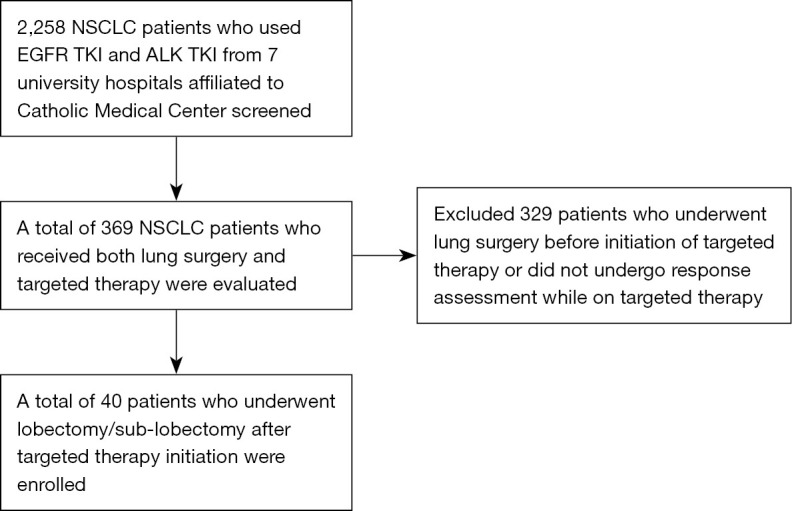
Flow diagram illustrating the selection process of patients for the study. NSCLC, non-small cell lung cancer; EGFR, epidermal growth factor receptor; ALK, anaplastic lymphoma kinase; TKI, tyrosine kinase inhibitor.
The primary endpoint was postoperative overall survival (OS), defined as the time between surgical resection and death or censoring. The secondary endpoint was postoperative PFS, defined as the time between surgical resection and disease progression.
Patients were grouped according to change in lung tumors between initiation of prior targeted therapy and resection of pulmonary tumor. Non-progressive disease group comprises patients whose lung tumors have either regressed or remained stable before surgical resection. Tumor progression group includes patients who experienced tumor regrowth after an initial response to treatment or developed new tumoral lung lesions. Tumor regression was defined as when the primary lung tumor shrinks by more than 30% compared to its size before starting TKI treatment. Tumor regrowth is when the tumor grows by more than 20% compared to the computed tomography (CT) scan just before the surgery, in comparison to the one taken right before that.
Tumor, node, metastasis (TNM) staging and pathologic typing
The TNM staging of lung cancer followed the American Joint Committee on Cancer (AJCC) 8th edition guidelines (6). For pathological typing, the 2015 World Health Organization (WHO) classification was utilized (7,8).
Longest diameter of resected tumor
The longest diameter was measured for the resected lung tumor sample. In cases where multiple tumors were resected, the longest diameter was recorded for the largest tumor. For the survival analysis, patients were stratified based on whether the longest diameter of their largest tumor exceeded 3 cm (9).
T790M mutation
Among 36 patients with EGFR mutations at diagnosis, we checked whether the T790M mutation was detected from the resected samples after the prior TKI treatment, either by routine polymerase chain reaction (PCR) methods or next-generation sequencing (NGS) (10,11).
Statistical analysis
For the comparison of clinical parameters between groups, the chi-squared test was used for categorical variables, and the Mann-Whitney test was used for continuous variables. Logistic regression was performed to identify factors associated with the T790M mutation at the time of resection, and multivariate analysis was not performed due to the small number of patients and the risk of overfitting.
For survival analysis, the Kaplan-Meier method was employed, with differences between groups assessed using the log-rank test. Cox regression analysis was conducted to determine associations with postoperative PFS and OS. Two models were used for multivariate analysis. Model I included factors with a P value <0.10 in univariate analysis, and Model II incorporated factors enrolled in Model I analysis, while excluding factors related to metastasis burden at diagnosis. Age and gender were included in the multivariate analysis as fundamental demographic parameters. All P values were two-sided, and a threshold of P<0.05 was set to indicate statistical significance in the multivariate analyses. IBM SPSS Statistics 22 (Armonk, NY, USA) was utilized for all statistical analyses.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Institutional Review Board of Catholic Medical Center, Korea (Nos. 2023-0661-0001 and SC23WIS0035). Informed consent was waived due to the retrospective study design.
Results
Clinical characteristics of study patients
All 40 patients were diagnosed with adenocarcinoma. Of these, 36 (90.0%) with EGFR mutations received prior EGFR TKI treatment, while 4 (10.0%) with ALK mutations received ALK TKI treatment. At the time of TKI initiation, 31 patients (77.5%) were staged as IV and 9 (22.5%) were staged as III (Table 1). Salvage surgery was performed in 18 patients (45.0%), and 22 (55.0%) underwent resection of regrowing masses for biopsy purposes. At the time of resection, tumor burden was unchanged in 7 patients (17.5%), significantly regressing in 12 patients (30.0%), and increasing in 21 patients (52.5%). Among the 28 patients with EGFR mutations from resected tumor specimens, 9 (32.1%) exhibited the T790M mutation. Only one postoperative complication, atrial fibrillation, was observed, and there was no postoperative mortality (Table 2).
Table 1. Clinical characteristic of overall patients.
| Clinical parameters | Value |
|---|---|
| Total number | 40 |
| Sex (female), n (%) | 28 (70.0) |
| Age (years), median [range] | 61.5 [40–82] |
| Pathologic type, n | |
| Adenocarcinoma | 40 (only type studied) |
| Driver mutations, n (%) | |
| EGFR mutation | 36 (90.0) |
| 19 deletion | 22 (61.1) |
| 21 L858R | 12 (33.3) |
| Subtype not available | 2 (5.6) |
| ALK translocation | 4 (10.0) |
| PD-L1 expression (at diagnosis) SP263 (n=27), n (%) | |
| 0% | 12 (30.0) |
| 1–9% | 5 (12.5) |
| 10–49% | 5 (12.5) |
| 0–99% | 5 (12.5) |
| Clinical stage at diagnosis, n (%) | |
| Stage I–II | 3 (7.5) |
| Stage III | 12 (30.0) |
| Stage IV | 25 (62.5) |
| Smoking history, n (%) | |
| Never smoker | 28 (70.0) |
| Ever smoker | 12 (30.0) |
| Targeted therapy prior to surgery†, n (%) | |
| Afatinib | 20 (50.0) |
| Alectinib | 3 (7.5) |
| Brigatinib | 1 (2.5) |
| Dacomitinib | 1 (2.5) |
| Erlotinib | 5 (12.5) |
| Gefitinib | 3 (7.5) |
| Lazertinib | 1 (2.5) |
| Osimertinib | 7 (17.5) |
| Duration of prior TKI treatment (months), median [range] | 18.0 [2.6–68.6] |
| Clinical stage at initiation of TKI, n (%) | |
| Stage III | 9 (22.5) |
| Stage IV | 31 (77.5) |
| Clinical stage at resection, n (%) | |
| Stage II | 1 (2.5) |
| Stage III | 9 (22.5) |
| Stage IV | 29 (72.5) |
| Downstaged (TNM 8th), n (%) | 3 (7.5) |
| Unchanged (TNM 8th), n (%) | 34 (85.0) |
| Upstaged (TNM 8th), n (%) | 2 (5.0) |
| ECOG at resection, n (%) | |
| 0 | 28 (70.0) |
| 1 | 10 (25.0) |
| 2 | 2 (5.0) |
†, one patient had undergone two targeted therapy regimens before resection. EGFR, epidermal growth factor receptor; ALK, anaplastic lymphoma kinase; PD-L1, programmed death-ligand 1; TKI, tyrosine kinase inhibitor; TNM, tumor, node, metastasis; ECOG, Eastern Cooperative Oncology Group.
Table 2. Detailed surgical outcomes and pathological features in lung cancer resections.
| Parameters | Value (n=40) |
|---|---|
| Objective of the surgery, n (%) | |
| Curative resection | 18 (45.0) |
| Resection of new/increasing lesion | 21 (52.5) |
| Biopsy purpose only | 1 (2.5) |
| Surgery type, n (%) | |
| Lobectomy | 19 (47.5) |
| Sublobectomy | 21 (52.5) |
| Postoperative complication, n (%) | 1 (2.5) |
| Postoperative mortality, n (%) | 0 (0.0) |
| Diameter of the resected mass (cm), median (range) | 2.3 (0.8–6.4) |
| Differentiation level (n=37), n (%) | |
| Well | 1 (2.7) |
| Moderate | 20 (54.1) |
| Poor | 16 (43.2) |
| STAS (n=30), n (%) | |
| None | 19 (63.3) |
| Present | 11 (36.7) |
| Pleural invasion (n=38), n (%) | |
| None | 25 (65.8) |
| PL1 | 6 (15.8) |
| PL2 | 5 (13.2) |
| PL3 | 2 (5.3) |
| Treatment change after resection† (n=39), n (%) | |
| No systemic treatment | 2 (5.1) |
| Resume same systemic treatment regimen | 12 (30.8) |
| Change to other systemic treatment | 25 (64.1) |
†, this parameter is assessed only in patients with regarding data. STAS, spread through air spaces; PL1, pleural invasion level 1; PL2, pleural invasion level 2; PL3, pleural invasion level 3.
Comparison between groups stratified by change in primary lung tumor at the resection
At the time of resection, 19 patients showed primary lung tumor size regressing or unchanged, while 21 patients showed primary lung tumor regrowth or new lesions being developed before the resection. Figure 2 presents CT images at timepoints before and after resection for a patient whose primary lung tumor size regressed at the time of resection. Figure 3 displays CT images of a patient whose primary lung tumor showed regrowth after an initial period of response to TKI therapy. The tumor progression group had a significantly higher percentage of stage IV cancer at the time of diagnosis and at the time of TKI initiation (P=0.01 and P=0.02, respectively). Median duration of prior TKI treatment duration was longer for the regrowth group, with statistical significance (P=0.044).
Figure 2.

Sequential chest CT images showing changes before and after surgical resection in a patient with primary lung tumor regression. (A) Baseline imaging showing primary tumor in the RML at initiation of afatinib treatment. (B) Decreased size of the RML mass observed after 6 months of afatinib therapy before surgical resection. (C) VATS RML lobectomy and MLND. (D) CT image obtained 3 months post-lobectomy showing the tumor located in RML removed and post-surgical changes. CT, computed tomography; RML, right middle lobe; VATS, video-assisted thoracoscopic surgery; MLND, mediastinal lymph node dissection.
Figure 3.

Chest CT images from a patient with tumor regrowth after initial response to TKI therapy. (A) Initial chest CT revealing a tumor in the LLL at the start of afatinib treatment (red arrow). (B) Image showing increase in size of the LLL tumor 24 months post-afatinib initiation (red arrow). (C) VATS wedge resection of the LLL tumor and mediastinal lymph node sampling. (D) CT image obtained 3 months following the wedge resection (red arrow). CT, computed tomography; TKI, tyrosine kinase inhibitor; LLL, left lower lobe; VATS, video-assisted thoracoscopic surgery.
Non-progressive disease group showed a higher percentage of downstaged patients (15.8% vs. 0.0%), but this was not statistically significant (P=0.08). Programmed death-ligand 1 (PD-L1) expression from both the SP263 and 22C3 assays were checked at time of diagnosis and from the resected samples. At the time of diagnosis, PD-L1 expression from both SP263 and 22C3 showed no significant difference between the groups. PD-L1 expression as shown by SP263 from resected samples showed significant difference. The tumor progression group showed a higher percentage of patients who expressed 1% or more (92.3% vs. 21.4%, P<0.001). By 22C3, the proportion of patients with PD-L1 expression equal to or more than 1% was also higher for the tumor progression group, but was not statistically significant (P=0.09).
The non-progressive disease group had a higher percentage of patients who showed viable tumor cell less than 10% from the resected sample (15.4% vs. 0.0%) compared to the tumor progression group, but no statistical significance was shown. When survival outcomes were compared between the two groups, there was no significant difference in duration of post-resection PFS and OS rate. The non-progressive disease group demonstrated a tendency toward a higher 6-month PFS rate compared to the tumor progression group (84.2% vs. 57.1%, P=0.06), although this was not statistically significant (Table 3).
Table 3. Comparison of clinical characteristics between groups stratified by changes in lung tumor at resection.
| Parameters | Non-progressive disease group | Tumor progression group | P value |
|---|---|---|---|
| Number | 19 | 21 | |
| Clinical stage at diagnosis, n (%) | 0.01 | ||
| Stage I–II | 1 (5.3) | 2 (9.5) | |
| Stage III | 10 (52.6) | 2 (9.5) | |
| Stage IV | 8 (42.1) | 17 (81.0) | |
| Duration of prior TKI treatment (months), median (range) | 10.5 (2.6–67.8) | 20.1 (3.5–68.6) | 0.044 |
| Clinical stage at initiation of TKI, n (%) | 0.02 | ||
| Stage III | 7 (36.8) | 2 (9.6) | |
| Stage IV | 12 (63.2) | 19 (90.5) | |
| Clinical stage at resection, n (%) | 0.07 | ||
| Stage II | 1 (5.3) | 0 (0.0) | |
| Stage III | 7 (36.8) | 2 (10.0) | |
| Stage IV | 11 (57.9) | 18 (90.0) | |
| Change of cancer stage between TKI initiation and later resection (TNM), n (%) | 0.08 | ||
| Downstaged | 3 (15.8) | 0 (0.0) | |
| Unchanged | 16 (84.2) | 18 (90.0) | |
| Upstaged | 0 (0.0) | 2 (10.0) | |
| Tumor differentiation level from resected sample (n=37), n (%) | n=18 | n=19 | 0.49 |
| Well | 0 (0.0) | 1 (5.3) | |
| Moderate | 11 (61.1) | 9 (47.4) | |
| Poor | 7 (38.9) | 9 (47.4) | |
| Lymphovascular invasion† (n=37), n (%) | n=18 | n=19 | 0.94 |
| None | 5 (27.8) | 6 (30.0) | |
| Lymphatic | 5 (27.8) | 4 (20.0) | |
| Vascular | 2 (11.1) | 2 (10.0) | |
| Both | 6 (33.3) | 8 (40.0) | |
| T790M mutation at resection (n=36), n/total (%) | 4/16 (25.0) | 7/20 (35.0) | 0.58 |
| PD-L1 SP263, diagnosis (n=27) , n (%) | n=14 | n=13 | 0.55 |
| 0% | 7 (50.0) | 5 (38.5) | |
| ≥1% | 7 (50.0) | 8 (61.5) | |
| PD-L1 22C3 at diagnosis (n=24), n (%) | n=14 | n=10 | 0.24 |
| 0% | 5 (35.7) | 6 (60.0) | |
| ≥1% | 9 (64.3) | 4 (40.0) | |
| PD-L1 SP263, resected sample (n=27), n (%) | n=14 | n=13 | <0.001 |
| 0% | 11 (78.6) | 1 (7.7) | |
| ≥1% | 3 (21.4) | 12 (92.3) | |
| PD-L1 22C3, resected sample (n=24), n (%) | n=13 | n=11 | 0.09 |
| 0% | 8 (61.5) | 3 (27.3) | |
| ≥1% | 5 (38.5) | 8 (72.7) | |
| Viable tumor cell from resected sample (n=25), n (%) | 0.16 | ||
| ≤10% | 2 (15.4) | 0 (0.0) | |
| >10% | 11 (84.6) | 12 (100.0) | |
| PFS and postoperative survival, n/total (%) | |||
| 6-month PFS rate (n=40) | 16/19 (84.2) | 12/21 (57.1) | 0.06 |
| 1-year PFS rate (n=39) | 13/19 (68.4) | 10/20 (50.0) | 0.24 |
| 18-month PFS rate (n=30) | 5/11 (45.5) | 8/19 (42.1) | 0.86 |
| 1-year postoperative survival rate | 18/18 (100.0) | 15/17 (88.2) | 0.13 |
| 2-year postoperative survival rate | 4/5 (80.0) | 10/14 (71.4) | 0.71 |
†, this parameter is assessed only in patients with regarding data. TKI, tyrosine kinase inhibitor; TNM, tumor, node, metastasis; PD-L1, programmed death-ligand 1; PFS, progression-free survival.
PD-L1 expression and survival
There were 27 patients with available PD-L1 (SP263) data from the resected samples. Among them, 15 patients exhibited PD-L1 expression of one percent or higher, while PD-L1 expression was not detected in the resected samples of 12 patients. From the Kaplan-Meier graph analysis, the group who showed no PD-L1 expression showed significantly better post-resection PFS when compared to the other group (P=0.007), while the median survival was not reached for the prior group and was 4.5 months for the latter group (Figure 4A). When post-resection OS was compared, a significant statistical difference was not seen (P=0.08) (Figure 4B). Six-month PFS rate was significantly better for the group without PD-L1 expression than the other group (90.9% vs. 53.3%, P=0.02), while the 1-year PFS rate did not show a significant difference (P=0.09).
Figure 4.

Comparison of post-resection survival outcomes based on PD-L1 expression, analyzed using different assays. (A) Comparison of post-resection PFS between patients with no PD-L1 expression and those with PD-L1 expression, analyzed using the SP263 assay. (B) Comparison of post-resection OS in patients with no PD-L1 expression vs. those with PD-L1 expression, analyzed using the SP263 assay. (C) Analysis of post-resection PFS in patients with no PD-L1 expression compared to those with PD-L1 expression, based on the 22C3 assay. (D) Assessment of post-resection OS in patients with no PD-L1 expression vs. those with PD-L1 expression, based on the 22C3 assay. PD-L1, programmed death-ligand 1; PFS, progression-free survival; OS, overall survival.
There were 24 patients with available PD-L1 (22C3) data from the resected samples. Among them, 13 patients exhibited PD-L1 expression of one percent or higher, while PD-L1 expression was absent in the resected samples of 11 patients. The group with PD-L1 expression (22C3) demonstrated a shorter median post-resection PFS (10.6 months) compared to those without PD-L1 expression (28.3 months), although the difference was not statistically significant (P=0.10) (Figure 4C) and no significant difference between the two groups in post resection OS was found (P=0.35) (Figure 4D).
T790M mutation
Among the 36 patients with EGFR mutations, prevalence of the T790M mutation was 27.5% at the time of resection.
Logistic regression was performed to assess association with the T790M mutation at the time of resection. Among the various parameters, prior EGFR TKI longer than 12 months and presence of spread through air spaces (STAS) from the resected samples showed significant association with the T790M mutation (Table 4, Figure 5).
Table 4. Correlation of T790M mutation with clinicopathologic parameters at resection in EGFR-mutated cases (n=36).
| Parameters | OR (95% CI) | P value |
|---|---|---|
| Tumor burden change at resection: regrowth vs. all others | 1.615 (0.376–6.940) | 0.52 |
| EGFR mutation subtype | 0.525 (0.119–2.312) | 0.39 |
| Lobectomy vs. sub-lobectomy | 4.875 (0.872–27.262) | 0.07 |
| Lymph node dissection during resection | 0.314 (0.069–1.433) | 0.14 |
| Objective of resection (curative vs. biopsy only) | 3.152 (0.668–14.862) | 0.15 |
| Tumor differentiation level of resected sample (poorly differentiated vs. others) | 0.686 (0.155–3.036) | 0.62 |
| Presence of STAS | 10.5 (1.496–73.673) | 0.02 |
| Pleural invasion (yes or no) | 0.132 (0.013–1.308) | 0.08 |
| Primary tumor size at resection (≥3 cm) | 0.118 (0.013–1.074) | 0.058 |
| Resected sample PD-L1 ≥1% (SP263) | 0.444 (0.060–3.285) | 0.43 |
| Resected sample PD-L1 ≥1% (22C3) | 0.656 (0.108–4.003) | 0.65 |
| Prior EGFR TKI >12 months | 9.231 (1.023–83.331) | 0.048 |
| Gender | 1.037 (0.212–5.077) | 0.96 |
EGFR, epidermal growth factor receptor; OR, odds ratio; CI, confidence interval; STAS, spread through air spaces; PD-L1, programmed death-ligand 1; TKI, tyrosine kinase inhibitor.
Figure 5.

Forrest plot depicting the association between the T790M mutation in resected samples and various clinical parameters. EGFR, epidermal growth factor receptor; STAS, spread through air spaces; PD-L1, programmed death-ligand 1; TKI, tyrosine kinase inhibitor; OR, odds ratio; CI, confidence interval.
Among the patients with EGFR mutations, PFS was compared between the groups stratified by whether the T790M mutation was detected. PFS was significantly different between the groups (Figure 6A) (P=0.01). Median PFS was 65.1 months in the T790M-positive group, while median PFS was 12.5 months in the group without the T790M mutation. When postresection OS was compared, no statistical significance was present (Figure 6B) (P=0.06), despite a positive trend toward the T790M-positive group.
Figure 6.

Comparison of clinical outcomes between groups stratified by presence of T790M mutation. (A) Analysis of PFS among patients with EGFR mutations, stratified by the presence or absence of the T790M mutation. (B) Comparison of post-resection OS between patients with and without the T790M mutation. Although not statistically significant (P=0.054), a trend favored the T790M-positive group. PFS, progression-free survival; EGFR, epidermal growth factor receptor; OS, overall survival.
Other pathologic parameters
When patients were stratified by the differentiation level of the resected tumor sample, those with poorly differentiated tumors showed significantly worse PFS compared to those with well or moderately differentiated tumors (P=0.02). However, no statistically significant difference was observed in postoperative OS between the groups (P=0.08) (Figure 7A,7B).
Figure 7.

Comparison of clinical outcome between groups stratified by tumor differentiation level from resected samples. (A) Comparison of PFS in patients with poorly differentiated tumors vs. those with well or moderately differentiated tumors, showing significantly worse PFS in the former group (P=0.02). (B) Analysis of postoperative survival across different tumor differentiation levels, revealing no statistically significant difference (P=0.08). PFS, progression-free survival.
NGS data
NGS performed on resected samples from 22 patients revealed various genetic alterations. The most prevalent mutation was TP53, found in 11 patients, accounting for 50% of the patients with NGS data. EGFR exon 19 deletions were present in 9 patients (40.9%), while the EGFR L858R mutation was identified in 6 patients (27.3%). The T790M mutation was detected in 5 patients, accounting 22.7%. EML4-ALK fusions and MET amplifications were each observed in 3 patients, each constituting around 13.6% of the cases (Table S1).
Analyses for prognostic factors for PFS and OS
Post-resection PFS
In the univariate analysis, brain metastasis at diagnosis [P=0.008; hazard ratio (HR) =4.122; 95% confidence interval (CI): 1.450–11.721], liver metastasis at diagnosis (P=0.043; HR =3.817; 95% CI: 1.042–13.986), differentiation level of cancer cells from the resected samples (poorly differentiated vs. others) (P=0.02; HR =2.834; 95% CI: 1.148–6.996), lymphovascular invasion (P=0.047 for reference value), and PD-L1 expression from resected samples (≥1% from 22C3 or SP263) (P=0.03; HR =4.239; 95% CI: 1.200–14.972) showed significant associations with post-resection PFS.
In the Model I multivariate analysis, which included age, gender, brain metastases, liver metastases at diagnosis, cancer differentiation level, presence of pleural invasion from the resected sample, lymphovascular invasion, and PD-L1 detection from the resected sample, none of the factors showed a significant association. In the Model II multivariate analysis, only PD-L1 detection from the resected sample demonstrated a significant association with PFS (P=0.03; HR =5.465; 95% CI: 1.200–24.885) (Table 5).
Table 5. Association with post-resection PFS.
| Parameters | Univariate | Multivariate (Model I) | Multivariate (Model II) | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |||
| Age (years) | 1.005 (0.968–1.043) | 0.80 | 1.067 (0.993–1.146) | 0.08 | 1.045 (0.990–1.103) | 0.11 | ||
| Gender (male vs. female) | 0.813 (0.330–1.999) | 0.65 | 0.812 (0.159–4.145) | 0.80 | 0.527 (0.135–2.064) | 0.36 | ||
| Smoking (never vs. ever) | 1.128 (0.458–2.779) | 0.79 | ||||||
| Brain metastasis at diagnosis (present vs. absent) | 4.122 (1.450–11.721) | 0.008 | 4.221 (0.475–37.512) | 0.20 | ||||
| Bone metastasis at diagnosis (present vs. absent) | 1.856 (0.536–6.425) | 0.33 | ||||||
| Liver metastasis at diagnosis (present vs. absent) | 3.817 (1.042–13.986) | 0.043 | 2.785 (0.233–33.234) | 0.42 | ||||
| Tumor burden change at resection: regrowth vs. other patterns (unchanged and regressing) | 1.686 (0.693–4.112) | 0.25 | ||||||
| Earlier clinical stages (II & III) vs. IV at resection | 2.079 (0.599–7.218) | 0.25 | ||||||
| Lobectomy vs. sub-lobectomy | 1.309 (0.530–3.236) | 0.56 | ||||||
| Lymph node dissection during resection (performed vs. not performed) | 0.754 (0.318–1.787) | 0.52 | ||||||
| Complete resection (R0 vs. R1–2) | 2.695 (0.722–10.061) | 0.14 | ||||||
| Tumor differentiation level of resection sample (poorly differentiated vs. others) | 2.834 (1.148–6.996) | 0.02 | 1.408 (0.207–9.586) | 0.73 | ||||
| STAS (presence vs. absence) | 0.710 (0.255–1.975) | 0.51 | ||||||
| Pleural invasion from resected sample (presence vs. absence) | 2.864 (1.146–7.161) | 0.02 | 1.458 (0.281–7.568) | 0.65 | 2.493 (0.607–10.237) | 0.21 | ||
| Lymphovascular invasion | ||||||||
| None | 1 | 0.047 | 1 | 0.46 | 1 | 0.66 | ||
| Lymphatic/vascular only | 0.363 (0.106–1.245) | 0.11 | 2.156 (0.246–18.883) | 0.49 | 1.546 (0.260–9.180) | 0.63 | ||
| Both | 1.631 (0.609–4.372) | 0.33 | 4.996 (0.378–66.021) | 0.22 | 2.728 (0.316–23.537) | 0.36 | ||
| Primary tumor size at resection (≥3 vs. <3 cm) | 1.626 (0.679–3.894) | 0.28 | ||||||
| Resected sample PD-L1 ≥1% vs. <1% (positive from 22C3 or SP263) | 4.239 (1.200–14.972) | 0.03 | 4.055 (0.775–21.223) | 0.10 | 5.465 (1.200–24.885) | 0.03 | ||
| Prior TKI treatment duration (continuous) | 1.011 (0.990–1.032) | 0.29 | ||||||
| Preoperative performance ECOG 0 | 1 | 0.55 | ||||||
| ECOG 1 | 1.710 (0.641–4.563) | 0.28 | ||||||
| ECOG 2 | 0.914 (0.118–7.074) | 0.93 | ||||||
Model I included factors with a P value <0.10; Model II incorporated factors enrolled in Model I analysis, while excluding factors regarding metastasis burden at diagnosis. PFS, progression-free survival; HR, hazard ratio; CI, confidence interval; STAS, spread through air spaces; PD-L1, programmed death-ligand 1; TKI, tyrosine kinase inhibitor; ECOG, Eastern Cooperative Oncology Group.
Post-resection OS
In the univariate analysis, liver metastasis at diagnosis was the only factor that showed a significant association (P=0.01; HR =10.445; 95% CI: 1.736–62.86). In both Model I and Model II multivariate analyses for OS, no factor demonstrated an independently significant association with post-resection OS (Table 6).
Table 6. Association with post-resection OS.
| Parameters | Univariate | Multivariate (Model I) | Multivariate (Model II) | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |||
| Age (years) | 1.039 (0.973–1.109) | 0.25 | 1.038 (0.950–1.134) | 0.41 | 1.011 (0.942–1.087) | 0.75 | ||
| Gender (male vs. female) | 0.449 (0.100–2.011) | 0.30 | 1.008 (0.104–9.803) | >0.99 | 0.600 (0.082–4.401) | 0.62 | ||
| Smoking (never vs. ever) | 0.357 (0.043–2.974) | 0.34 | ||||||
| Preoperative performance ECOG 0 | 1 | 0.07 | 1 | 0.37 | 1 | 0.10 | ||
| ECOG 1 | 7.076 (1.282–39.068) | 0.03 | 3.946 (0.572–27.237) | 0.16 | 6.870 (1.204–39.206) | 0.03 | ||
| ECOG 2 | 7.129 (0.639–79.533) | 0.11 | 3.111 (0.166–58.281) | 0.45 | 3.709 (0.209–65.967) | 0.37 | ||
| Brain metastasis at diagnosis (present vs. absent) | 1.098 (0.131–9.194) | 0.93 | ||||||
| Bone metastasis at diagnosis (present vs. absent) | 1.498 (0.179–12.509) | 0.71 | ||||||
| Liver metastasis at diagnosis (present vs. absent) | 10.445 (0.1736–62.86) | 0.01 | 7.026 (0.696–70.903) | 0.10 | ||||
| Tumor burden change at resection: regrowth vs. other patterns (unchanged and regressing) | 4.678 (0.553–39.578) | 0.16 | ||||||
| Earlier clinical stages (II & III) vs. IV at resection | 30.206 (NA) | 0.42 | ||||||
| Lobectomy vs sub-lobectomy | 0.452 (0.099–2.067) | 0.31 | ||||||
| Lymph node dissection during resection (performed vs. not performed) | 1.643 (0.317–8.520) | 0.55 | ||||||
| Complete resection (R0 vs. R1–2) | 1.952 (0.217–17.58) | 0.55 | ||||||
| Tumor differentiation level of resection sample (poorly differentiated vs. others) | 5.696 (0.635–51.054) | 0.12 | ||||||
| STAS (presence vs. absence) | 1.267 (0.211–7.595) | 0.80 | ||||||
| Pleural invasion from resected sample (presence vs. absence) | 3.441 (0.675–17.539) | 0.14 | ||||||
| Lymphovascular invasion | ||||||||
| None | 1 | 0.79 | ||||||
| Lymphatic/vascular only | 0.879 (0.124–6.253) | 0.90 | ||||||
| Both | 1.579 (0.262–9.511) | 0.62 | ||||||
| Primary tumor size at resection (≥3 vs. <3 cm) | 1.781 (0.393–8.068) | 0.45 | ||||||
| Resected sample PD-L1 ≥1% vs. <1% (positive from 22C3 or SP263) | 44.202 (NA) | 0.32 | ||||||
| Prior TKI treatment duration (continuous) | 1.002 (0.961–1.044) | 0.94 | ||||||
Model I included factors with a P value <0.10; Model II incorporated factors enrolled in Model I analysis, while excluding factors regarding metastasis burden at diagnosis. OS, overall survival; HR, hazard ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; NA, not available; STAS, spread through air spaces; PD-L1, programmed death-ligand 1; TKI, tyrosine kinase inhibitor.
Comparison of changes in PD-L1 expression at diagnosis and resection across groups stratified by changes in primary tumor burden
There were 15 patients with paired data for the 22C3 assay and 19 patients with paired data for the SP263 assay, obtained both at the time of diagnosis and from the resected sample. In the disease progression group, where lung tumors showed regrowth or new lung tumor lesions developed at the time of resection, the proportion of patients with increase in PD-L1 (22C3) expression was significantly higher compared to the non-progressive disease group (67% vs. 11%, P=0.03) as shown in Figure 8A.
Figure 8.

Correlation between change in lung tumoral burden at resection and increase in PD-L1 expression. (A) In the disease progression group, where lung tumors showed regrowth or new lung tumor lesions developed at the time of resection, the proportion of patients with increase in PD-L1 (22C3) expression was significantly higher compared to the non-progressive disease group (67% vs. 11%, P=0.03). (B) Additionally, the disease progression group showed a higher proportion of patients with elevated PD-L1 (SP263) expression compared to the non-progressive disease group (44% vs. 10%), although this difference was not statistically significant (P=0.09). PD-L1, programmed death-ligand 1.
Additionally, the disease progression group showed a higher proportion of patients with elevated PD-L1 (SP263) expression compared to the non-progressive disease group (44% vs. 10%), although this difference was not statistically significant (P=0.09), as illustrated in Figure 8B.
Comparison of PFS and OS rates between groups stratified by various factors
Tumor differentiation level of resected sample
In the analysis of survival outcomes stratified by tumor differentiation level, there were a statistically significant difference in 6-month PFS rates and 2-year OS rates between patients with well and moderate differentiation compared to those with poor differentiation (P=0.046 and P=0.03, respectively). Specifically, patients with well and moderate differentiation exhibited a 6-month PFS rate of 85.7%, significantly higher than the 56.3% observed in patients with poor differentiation. Additionally, while the 2-year OS rate was 100% in the well and moderate differentiation group, it was significantly lower in the poor differentiation group at 55.6% (Table S2).
Resection status (R0 vs. R 1–2)
Further stratification by resection status (Table S3) showed no statistically significant differences in PFS or OS between patients with no residual tumor (R0) and those with microscopic or gross residual disease (R1–2) at most time points. Group with R0 resection showed tendency of superior higher PFS rates, but no statistical significance was present.
Impact of T790M mutation status
The analysis of lung cancer patients stratified by T790M mutation status (Table S4) reveals differences in survival outcomes. Patients with T790M mutation from resected sample showed significantly better PFS rate at 12 months (90.0% vs. 48.0%, P=0.02) and 18 months (87.5% vs. 35.7%, P=0.003) compared to those without the mutation.
Survival outcomes by Eastern Cooperative Oncology Group (ECOG) performance status
When stratified by ECOG performance status prior to resection (Table S5), patients with an ECOG score of 0 demonstrated better 12-month PFS (71.4% vs. 22.2% in ECOG 1 and 50.0% in ECOG 2, P=0.03) and superior 2-year OS (100.0% vs. 33.3% in ECOG 1 and 50.0% in ECOG 2, P=0.008) compared to those with higher ECOG scores.
Pleural invasion and survival
The degree of pleural invasion also significantly influenced survival outcomes (Table S6). Patients with no pleural invasion (PL0) had a higher 6-month PFS rate of 84.05% and 2-year OS rate of 84.6% compared to groups with more extensive invasion (P=0.03 and P=0.04, respectively).
Discussion
This study showed two key findings: that surgical resection of lung tumor after targeted therapy can provide valuable information that can potentially predict future outcomes, and that it is relatively safe.
Most patients enrolled had a targetable EGFR mutation at diagnosis and received EGFR TKI treatment as their initial management. From the resected samples, the T790M mutation detection rate was 27.5% among 36 EGFR mutation-positive patients who underwent primary lung tumor resection. This is lower than the T790M mutation detection rate reported by historical data (12,13). However, it should be taken into account that the majority of the patients still retained treatment response from prior TKI when the resection was performed, suggesting that resistance to treatment has not yet developed in a considerable number of cases. From the logistic regression analysis, it was interesting to see that longer duration of EGFR TKI (TKI duration longer than 12 months) and presence of STAS from the resected sample showed significant association with detection of the T790M mutation. Association with longer duration of prior TKI was also reported in other study (14). STAS was reported as a risk factor for recurrence in primary lung adenocarcinoma and squamous cell carcinoma (15,16). It is questionable if there is a direct molecular or pathological link between the presence of STAS and T790M mutations or if it is a simple coincidence. If this association with the T790M mutation is validated using a larger population of resected samples, we can consider tumor resection in patients who initially had STAS or had undergone EGFR TKI for a long duration.
The study patients with the T790M mutation detected at the time of resection showed significantly better PFS than the EGFR mutation-positive patients without the T790M mutation. Early detection of the T790M mutation is crucial as it allows clinicians to understand the resistance mechanisms in lung cancer patients undergoing TKI treatment, facilitating the selection of more appropriate targeted therapies (17,18). It is important to note that in Korea, third-generation TKIs such as lazertinib and osimertinib were not covered by national health insurance for first-line treatment in EGFR-mutated patients during this period. Consequently, they were more frequently prescribed in the second line or later for advanced NSCLC with the T790M mutation (19-21). This treatment context may have contributed to the observed trend of patients with T790M mutations experiencing higher PFS rates in our study patients.
It was also interesting to see that PD-L1 expression in the resected sample showed a difference between the groups stratified by change in lung tumoral burden at resection (non-progressive disease group vs. tumor progression group). The tumor progression group showed higher proportion of patients with PD-L1 expression from the resected sample. Most of the included patients were positive for EGFR mutations. One meta-analysis that included 991 patients showed that pretreatment PD-L1 expression was associated with shorter PFS (22). However, controversy exists as another study indicated that there is no association between clinical outcomes and post-progression PD-L1 expression (23). Nevertheless, in our study, an increase in PD-L1 expression observed in paired samples was significantly associated with increased tumor burden at the time of resection. In our study, not only did the PD-L1 expression in the resection sample correlate with clinical outcomes, the change in PD-L1 expression relative to baseline also demonstrated a clinical correlation with the response to TKI treatment. Unfortunately, number of patients with paired PD-L1 expression was too small to conclude association with postoperative PFS or OS. The change in PD-L1 expression in EGFR-mutated patients undergoing initial TKI treatment requires validation through larger studies, and its association with other components of the tumor immune microenvironment needs further studies (24).
Under the condition that resection of lung tumors following a period of TKI treatment response in initially unresectable NSCLC improves clinical outcomes, the optimal timing for such interventions remains uncertain. Should we perform the surgery as soon as the primary tumor becomes resectable? Or is it better to wait until the initial systemic chemotherapy effect takes place and plateau of primary tumor regression happens? The other option is to wait until the mass starts to regrow. Our study, limited by its small sample size, cannot provide definitive answers to these questions. When comparing the group that underwent resection after primary tumor stability or regression at the time of resection with the group that underwent resection following tumor regrowth, we observed a trend towards a better 6-month PFS rate in the former group, but no clear superiority in clinical outcomes was evident from our study. However, timing of the resection should be carefully decided by the multidisciplinary team, balancing between the risk of resection and maximization of the efficacy of the surgery.
The objective of resection is particularly important in patients undergoing targeted therapy for initially unresectable NSCLC, and this heavily depends on the clinical situation of the patient. If the patient presents with multiple distant metastases, aggressive and early resection of the primary tumor may not be advisable. However, in cases without distant metastases, active consideration can be given to resecting the primary tumor if there is a response to initial systemic chemotherapy and complete resectability is achieved. Should the primary tumor size increase after an initial response to targeted therapy, resection can be undertaken to identify alternative targetable mutations while also reducing tumor burden. Acquiring a sufficient amount of post-progression sample can provide an opportunity for more tailored therapy, which ultimately contributes to improved outcomes in advanced NSCLC with driver mutations (25).
Present study has several limitations. This is a retrospective study with small sample sizes, but data were sampled from 7 different centers. Despite relatively specific enrollment criteria, heterogeneity still exists in terms of disease burden and clinical circumstances at time of surgery. Although factors such as lympho-vascular invasion and tumor size did not show an association with PFS in our study, the small sample size may limit the ability to detect the true clinical impacts of these factors. A prospective study with a larger sample size and a well-matched control group is necessary for validation.
Conclusions
The findings of this study suggest that lung tumor resection following targeted therapy for initially unresectable NSCLC can provide valuable clinical information that can be used to predict the prognosis. Identifying suitable candidates for lung surgery is crucial for optimizing patient outcomes.
Supplementary
The article’s supplementary files as
Acknowledgments
The present study was previously presented in the poster session of ESMO 2023.
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Institutional Review Board of Catholic Medical Center, Korea (Nos. 2023-0661-0001 and SC23WIS0035). Informed consent was waived due to the retrospective study design.
Footnotes
Reporting Checklist: The authors have completed the REMARK reporting checklist. Available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-215/rc
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-215/coif). The authors have no conflicts of interest to declare.
Data Sharing Statement
Available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-215/dss
References
- 1.Lindeman NI, Cagle PT, Beasley MB, et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Mol Diagn 2013;15:415-53. 10.1016/j.jmoldx.2013.03.001 [DOI] [PubMed] [Google Scholar]
- 2.Suzuki S, Asakura K, Okui M, et al. Prognostic factors affecting survival in patients with non-small cell lung cancer treated with salvage surgery after drug therapy: a multi-institutional retrospective study. World J Surg Oncol 2023;21:290. 10.1186/s12957-023-03177-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Li K, Cao X, Ai B, et al. Salvage surgery following downstaging of advanced non-small cell lung cancer by targeted therapy. Thorac Cancer 2021;12:2161-9. 10.1111/1759-7714.14044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ofiara LM, Navasakulpong A, Ezer N, et al. The importance of a satisfactory biopsy for the diagnosis of lung cancer in the era of personalized treatment. Curr Oncol 2012;19:S16-23. 10.3747/co.19.1062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ohtaki Y, Shimizu K, Suzuki H, et al. Salvage surgery for non-small cell lung cancer after tyrosine kinase inhibitor treatment. Lung Cancer 2021;153:108-16. 10.1016/j.lungcan.2020.12.037 [DOI] [PubMed] [Google Scholar]
- 6.Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2016;11:39-51. 10.1016/j.jtho.2015.09.009 [DOI] [PubMed] [Google Scholar]
- 7.Travis WD. The 2015 WHO classification of lung tumors. Pathologe 2014;35 Suppl 2:188. 10.1007/s00292-014-1974-3 [DOI] [PubMed] [Google Scholar]
- 8.Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol 2015;10:1243-60. 10.1097/JTO.0000000000000630 [DOI] [PubMed] [Google Scholar]
- 9.Hung JJ, Jeng WJ, Hsu WH, et al. Prognostic factors in pathological stage IB nonsmall cell lung cancer greater than 3 cm. Eur Respir J 2010;36:1355-61. 10.1183/09031936.00014109 [DOI] [PubMed] [Google Scholar]
- 10.Vaclova T, Grazini U, Ward L, et al. Clinical impact of subclonal EGFR T790M mutations in advanced-stage EGFR-mutant non-small-cell lung cancers. Nat Commun 2021;12:1780. 10.1038/s41467-021-22057-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Masuda T, Miura S, Sato Y, et al. Significance of micro-EGFR T790M mutations on EGFR-tyrosine kinase inhibitor efficacy in non-small cell lung cancer. Sci Rep 2023;13:19729. 10.1038/s41598-023-45337-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bencze E, Bogos K, Kohánka A, et al. EGFR T790M Mutation Detection in Patients With Non-Small Cell Lung Cancer After First Line EGFR TKI Therapy: Summary of Results in a Three-Year Period and a Comparison of Commercially Available Detection Kits. Pathol Oncol Res 2022;28:1610607. 10.3389/pore.2022.1610607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Li W, Qiu T, Guo L, et al. Primary and acquired EGFR T790M-mutant NSCLC patients identified by routine mutation testing show different characteristics but may both respond to osimertinib treatment. Cancer Lett 2018;423:9-15. 10.1016/j.canlet.2018.03.005 [DOI] [PubMed] [Google Scholar]
- 14.Huang YH, Hsu KH, Tseng JS, et al. The Association of Acquired T790M Mutation with Clinical Characteristics after Resistance to First-Line Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor in Lung Adenocarcinoma. Cancer Res Treat 2018;50:1294-303. 10.4143/crt.2017.512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kadota K, Nitadori JI, Sima CS, et al. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J Thorac Oncol 2015;10:806-14. 10.1097/JTO.0000000000000486 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lu S, Tan KS, Kadota K, et al. Spread through Air Spaces (STAS) Is an Independent Predictor of Recurrence and Lung Cancer-Specific Death in Squamous Cell Carcinoma. J Thorac Oncol 2017;12:223-34. 10.1016/j.jtho.2016.09.129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Watanabe M, Kawaguchi T, Isa S, et al. Ultra-Sensitive Detection of the Pretreatment EGFR T790M Mutation in Non-Small Cell Lung Cancer Patients with an EGFR-Activating Mutation Using Droplet Digital PCR. Clin Cancer Res 2015;21:3552-60. 10.1158/1078-0432.CCR-14-2151 [DOI] [PubMed] [Google Scholar]
- 18.Sequist LV, Waltman BA, Dias-Santagata D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med 2011;3:75ra26. 10.1126/scitranslmed.3002003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Park S, Jung HA, Lee SH, et al. Real-world clinical evidence of lazertinib use in acquired EGFR T790M mutated non-small cell lung cancer. Transl Lung Cancer Res 2023;12:1912-22. 10.21037/tlcr-23-160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cho BC, Han JY, Kim SW, et al. A Phase 1/2 Study of Lazertinib 240 mg in Patients With Advanced EGFR T790M-Positive NSCLC After Previous EGFR Tyrosine Kinase Inhibitors. J Thorac Oncol 2022;17:558-67. 10.1016/j.jtho.2021.11.025 [DOI] [PubMed] [Google Scholar]
- 21.Mok TS, Wu Y-L, Ahn M-J, et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N Engl J Med 2017;376:629-40. 10.1056/NEJMoa1612674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Peng Z, Lin H, Zhou K, et al. Predictive value of pretreatment PD-L1 expression in EGFR-mutant non-small cell lung cancer: a meta-analysis. World J Surg Oncol 2021;19:145. 10.1186/s12957-021-02254-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liu J, Itchins M, Nagrial A, et al. Relationship between PD-L1 expression and outcome in EGFR-mutant lung cancer patients treated with EGFR tyrosine kinase inhibitors. Lung Cancer 2021;155:28-33. 10.1016/j.lungcan.2021.03.004 [DOI] [PubMed] [Google Scholar]
- 24.Peng S, Wang R, Zhang X, et al. EGFR-TKI resistance promotes immune escape in lung cancer via increased PD-L1 expression. Mol Cancer 2019;18:165. 10.1186/s12943-019-1073-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Choudhury NJ, Marra A, Sui JSY, et al. Molecular Biomarkers of Disease Outcomes and Mechanisms of Acquired Resistance to First-Line Osimertinib in Advanced EGFR-Mutant Lung Cancers. J Thorac Oncol 2023;18:463-75. 10.1016/j.jtho.2022.11.022 [DOI] [PMC free article] [PubMed] [Google Scholar]