

Abstract
Background
Equitable geographical distribution of health resources, such as hospital beds, is fundamental in ensuring public accessibility to healthcare services. This study examines the distribution of hospital beds across Saudi Arabia's 20 health regions.
Methods
A secondary data analysis was conducted using the 2022 Saudi Ministry of Health Statistical Yearbook. The study focused on calculating the hospital beds-per-1,000-people ratio across Saudi Arabia's 20 health regions. The analysis involved comparing regional bed distributions using the Gini index and Lorenz curve to assess the distribution of hospital beds.
Results
The national average beds-per-1,000-people ratio was 2.43, serving a population of approximately 32.2 million. The calculated mean Gini index for bed distribution was 0.15, which indicates a relatively equitable distribution. Further analysis revealed some regional disparities, with health regions like Makkah and Jeddah displaying critically low bed-to-population ratios. In contrast, others like Al-Jouf and the Northern region reported higher ratios. The study also identified the need for an additional 17,062 beds to meet international standards of 2.9 beds per 1,000 people.
Conclusions
The findings revealed a national average beds-per-1,000-people ratio of 2.43, with some regional disparities. The study highlights the critical need for targeted healthcare planning and policy interventions to address the uneven distribution of hospital beds across Saudi Arabia.
Trial registration
Not applicable.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12913-024-11391-4.
Keywords: Hospital beds to population ratio, Hospital beds, Healthcare access, Regional disparities, Healthcare infrastructure, Regional distribution, Saudi Arabia
Background
The equitable geographical distribution of health resources, such as hospital beds, is fundamental in ensuring public accessibility to healthcare services [1]. The spatial allocation of health resources significantly influences the ability of individuals to receive medical care, particularly within their geographic location [2]. Achieving equity in health resource allocation is believed to be among the significant challenges facing healthcare worldwide [3]. Geographical access to healthcare services plays a crucial role in minimizing health inequalities [4]. Studies have shown that inequalities in the geographical distribution of health resources and services can significantly worsen disparities in healthcare outcomes and quality of life. For instance, a study conducted in Saudi Arabia suggested that regional differences in healthcare access and health resources can exacerbate socioeconomic inequalities in the prevalence of non-communicable diseases, potentially widening the gap between the rich and the poor in the country [5]. Similarly, in China, a reduction in the maternal mortality ratio was observed following the country's expansion of hospital beds and improvements in the equitable geographical distribution of these beds [6].
In the realm of global healthcare infrastructure, the hospital beds-per-1,000-population ratio serves as a key indicator of resource availability. In 2020, Saudi Arabia's ratio stood at 2.2, reflecting its position within the international spectrum of healthcare provisioning (Fig. 1) [7–9]. While this figure trails behind Japan, which boasts a leading ratio of 12.6, and the substantial resources of the European Union and China, each with a ratio of 5.0, it remains competitive when assessed against the global average of 2.9. However, Saudi Arabia outpaces the Middle East and North Africa (MENA) region's average of 1.5, underscoring its relatively more substantial healthcare infrastructure.
Fig. 1.

Comparative analysis of hospital bed availability (beds-per-1,000-People) in selected countries for 2020
In Saudi Arabia, the expansion of hospital bed resources has been rapid and significant. From just 9,000 beds in 1970, the number grew to over 72,000 by 2017, spread across 487 facilities, and reaching over 78,000 by 2022 across 493 facilities [7, 10, 11]. Despite growth in the ratio of hospital beds per 1,000 people in 2022, it remains below the global average of about 2.9 (Table 1). Projections indicate that an additional 10,200 beds will be needed by 2025 to maintain the current ratio [7, 10]. Additionally, the increasing prevalence of non-communicable diseases (NCDs) and an aging population in Saudi Arabia significantly impact the healthcare system, particularly in terms of hospital bed distribution. Chronic conditions such as heart disease, diabetes, and cancer are more common with lifestyle changes and aging, necessitating prolonged medical care, thereby increasing the demand for hospital beds [12].
Table 1.
Five-year overview of hospital bed capacity in KSA (2018–2022)
| YEAR | POPULATION | TOTAL BEDS | BEDS-PER-1,000-PEOPLE |
|---|---|---|---|
| 2017 | 29,647,968 | 72,000 | 2.4 |
| 2018 | 30,196,281 | 75,225 | 2.5 |
| 2019 | 30,063,799 | 76,988 | 2.6 |
| 2020 | 31,552,510 | 78,596 | 2.5 |
| 2021 | 30,784,383 | 77,224 | 2.5 |
| 2022 | 32,175,224 | 78,440 | 2.4 |
Optimizing the geographic allocation of hospital beds is essential. International experiences, such as in Sweden, have shown that reductions in bed capacity can lead to increased mortality and healthcare costs [13, 14]. Although Saudi Arabia's healthcare system is favorably positioned regionally regarding hospital beds per population, it still has room for growth when juxtaposed with global healthcare leaders. Studies indicate that resources are moderately equitably distributed at the country's administrative level; however, significant regional variations exist in hospital beds' distribution, with urban areas generally being better provisioned than rural ones. Thus, this study aims to assess the equity of beds distribution across the 20 health regions in Saudi Arabia using the most recent available data (2022). Highlighting regional disparities in bed distribution in the country is crucial for identifying gaps and understanding which health regions are being left behind. Additionally, by offering a comprehensive overview of the current state of hospital bed distribution, the findings of this study can facilitate the implementation of appropriate and effective interventions and contribute to the ongoing discourse on healthcare equity and resource allocation in Saudi Arabia.
Methods
In this study, a secondary data analysis was conducted to examine and compare the geographical distribution of hospital beds across the 20 health regions of Saudi Arabia. The primary objective was to assess the bed distribution metrics using the most recent statistics available for the year 2022. This approach was chosen to provide an up-to-date and comprehensive overview of the country's current state of hospital bed allocation.
The data for this analysis was sourced from the Saudi Ministry of Health (MOH) Statistical Yearbook, a highly regarded and authoritative source for health-related statistics in Saudi Arabia [9]. This Yearbook compiles a wide range of health indicators and infrastructure statistics for each of the country's governed areas, making it an ideal source for this study. The bed counts extracted from the Yearbook represented the total number of hospital beds available across all hospitals in Saudi Arabia, as reported to the MOH at the end of the year.
Alongside the hospital bed data, population estimates for each of the 20 health regions of Saudi Arabia were also obtained from the demographic section of the MOH Statistical Yearbook. These figures result from mid-year population projections produced through collaborative methodologies between the MOH and other national statistical bodies. Using these population estimates was crucial for calculating a key metric of this study: the number of beds per 1,000 people. This metric serves as a standardized measure for comparing the availability of hospital beds across different regions, irrespective of their varying population sizes.
Results
The detailed analysis of the 2022 data on hospital bed distribution in the Kingdom of Saudi Arabia (KSA) reveals significant insights into the healthcare infrastructure across its 20 regions (Table 2). The country, with a total of 78,440 hospital beds serving a population of approximately 32.2 million, achieves an average beds-per-1,000-people ratio of 2.4. While indicative of the overall healthcare capacity, this figure masks considerable regional disparities.
Table 2.
2022 Distribution of hospital beds per 1,000 people across regions in Saudi Arabia
| Rank | Region | Population | Beds | Beds-per-1,000-people |
|---|---|---|---|---|
| 1 | Al-Jouf | 333,189 | 1,360 | 4.1 |
| 2 | Northern | 358,989 | 1,460 | 4.1 |
| 3 | Najran | 570,698 | 1,947 | 3.4 |
| 4 | Hafr Al-Baten | 437,822 | 1,469 | 3.4 |
| 5 | Tabouk | 889,914 | 2,884 | 3.2 |
| 6 | Ha`il | 685,571 | 2,211 | 3.2 |
| 7 | Ta`if | 1,275,200 | 4,053 | 3.2 |
| 8 | Qurayyat | 165,804 | 490 | 3.0 |
| 9 | Al-Bahah | 465,779 | 1,325 | 2.8 |
| 10 | Al -Ahsa | 1,199,375 | 3,306 | 2.8 |
| 11 | Eastern | 3,202,857 | 8,591 | 2.7 |
| 12 | Qaseem | 1,397,187 | 3,710 | 2.7 |
| 13 | Riyadh | 8,153,488 | 20,457 | 2.5 |
| 14 | Bishah | 380,622 | 920 | 2.4 |
| 15 | Medinah | 2,105,376 | 5,013 | 2.4 |
| 16 | Aseer | 1,782,856 | 4,237 | 2.4 |
| 17 | Jazan | 1,535,152 | 2,753 | 1.8 |
| 18 | Jeddah | 4,623,940 | 8,244 | 1.8 |
| 19 | Makkah | 2,308,801 | 3,610 | 1.6 |
| 20 | Qunfudah | 302,597 | 400 | 1.3 |
| Total = 32,175,220 | Total = 78,440 | KSA average = 2.4 | ||
Regarding regional distribution, Al-Jouf and the Northern region stand out with the highest beds-per-1,000-people ratios, both at 4.1 (Fig. 2). This ratio suggests a sound healthcare infrastructure in these regions, especially considering their respective populations of 333,189 and 358,989. On the other end of the spectrum, Qunfudah, Makkah, and Jeddah exhibit the lowest ratios. This starkly contrasts with the national average, highlighting a significant shortfall in hospital bed availability.
Fig. 2.

The 2022 Hospital beds-per-1,000-people regional distribution in KSA
The region of Riyadh, home to the largest population in the KSA at over 8.1 million, maintains a bed-to-population ratio of 2.5, supported by 20,457 hospital beds. The Eastern region, with a population of 3.2 million, offers 8,591 beds, translating to a ratio of 2.7. In contrast, Jeddah, despite its considerable population of 4.6 million, achieves a lower ratio of 1.8 with 8,244 beds, underscoring a disparity in bed availability compared to other populous regions.
A closer comparative analysis across the regions against the national bed ratio paints a picture of inequality. Approximately half of the regions surpass the national average in bed-to-population ratio, while the other half fall below this benchmark. Notably, the regions in the lowest quartile exhibit significantly lower ratios, ranging from 1.3 to 1.8, which is considerably below the national average, underscoring the uneven distribution of healthcare resources across the KSA.
Analysis of hospital bed distribution equity in Saudi Arabia
The distribution of hospital beds per 1,000 people across various regions in Saudi Arabia reveals a relatively equitable allocation, as indicated by a Gini coefficient of approximately 0.1505. The Lorenz curve for this data set (Fig. 3) illustrates the distribution pattern, plotting the cumulative share of hospital beds against the cumulative share of regions.
Fig. 3.
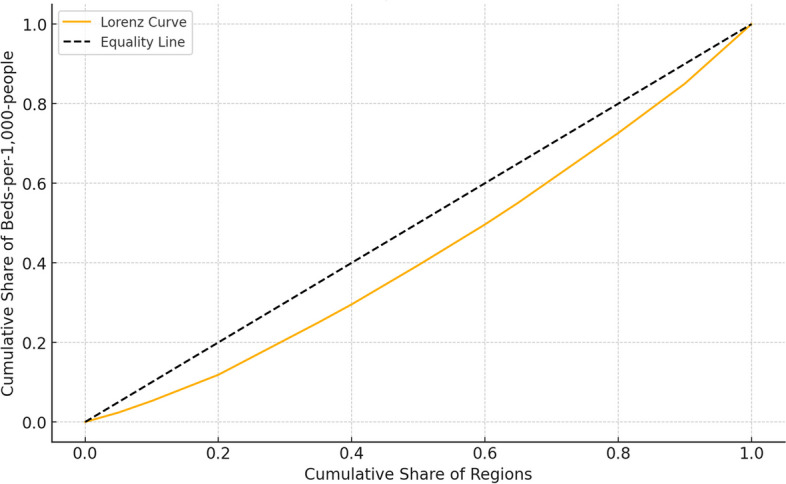
Lorenz Curve for the Distribution of Hospital Beds per 1,000 People in Saudi Arabia
The curve's proximity to the line of equality suggests minimal disparity in the distribution of hospital beds. This relatively low Gini coefficient implies that most regions have a comparable number of hospital beds relative to their population, promoting equitable access to healthcare services across the country.
Healthcare infrastructure enhancement: bed availability projection
To examine Saudi Arabia's healthcare infrastructure against global standards [7], with a minimum of 2.9 hospital beds per 1,000 people, an analysis was conducted to determine the necessary increase in bed numbers.
As of 2022, the total number of beds count stands at 78,440; however, to meet the international bed-to-population ratio, an additional 17,062 beds are required to reach a revised total of 79,628. Table 3 delineates the regional distribution of current bed counts and identifies the additional beds needed for each region to achieve the 2.9 beds-per-1,000-people ratio. Notably, eight regions already exceed this standard and require no extra beds, reflecting their well-equipped healthcare facilities.
Table 3.
Bed allocation to meet international standards across regions
| REGION | 2022 TOTAL BEDS | TOTAL BEDS NEEDED TO ACHIEVE THE 2.9 BEDS-PER-1,000-PEOPLE RATIO DISTRIBUTED AMONG 12 REGIONS |
|---|---|---|
| AL-JOUF | 1,360 | 0 |
| NORTHERN | 1,460 | 0 |
| NAJRAN | 1,947 | 0 |
| HAFR AL-BATEN | 1,469 | 0 |
| TABOUK | 2,884 | 0 |
| HA'IL | 2,211 | 0 |
| TA'IF | 4,053 | 0 |
| QURAYYAT | 490 | 0 |
| AL-BAHAH | 1,325 | 26 |
| AL -AHSA | 3,306 | 172 |
| EASTERN | 8,591 | 697 |
| QASEEM | 3,710 | 342 |
| RIYADH | 20,457 | 3,188 |
| BISHAH | 920 | 184 |
| MEDINAH | 5,013 | 1,093 |
| ASEER | 4,237 | 933 |
| JAZAN | 2,753 | 1,699 |
| JEDDAH | 8,244 | 5,165 |
| MAKKAH | 3,610 | 3,086 |
| QUNFUDAH | 400 | 478 |
| Total = 78,440 | Total = 17,062 beds |
Discussion
To our knowledge, this is the first study evaluating the equity in hospital bed distribution relative to population size across the 20 health regions in 2022 in Saudi Arabia. When calculating the Gini coefficient, the overall bed distributions seem to be somehow equitable among different regions. However, a picture of inequality emerges when comparing the 20 health regions against the national bed ratio. Approximately half of the regions surpass the national average in bed-to-population ratio, while the other half fall below this benchmark. Notably, the regions in the lowest quartile exhibit significantly lower ratios, ranging from 1.3 to 1.8, underscoring the uneven geographical distribution of hospital beds across the KSA. We have also projected the need for an additional 17,062 beds to meet international standards of 2.9 beds per 1,000 population.
Among the 20 health regions, Makkah and Jeddah regions, despite their economic significance, exhibited a substantial deficit in hospital bed numbers per 1000 population and also fell below the national average bed-to-population ratio. For the Makkah region, the study found a ratio of 1.6 hospital beds -per-1,000-people. The region houses 80 primary healthcare centers and 18 hospitals. Although there is no consensus about the "optimal" ratio for primary healthcare centers to population, a study by Alsheddi et al. [15] examining the distribution of primary healthcare centers between 2017 and 2021 found a negative correlation between the number of primary healthcare centers in the region and its population size. It is important to note that Makkah City, at the heart of the Makkah region, presents a challenge on its own for those in charge of enhancing the health of its population [16].The city attracts millions of visitors for religious purposes annually. This influx of tourists might cause surges in demand and put an enormous strain on the healthcare system, such as increasing the occupancy rate of hospital beds [17]. Furthermore, during the pandemic crises, the city was a hot spot for the COVID-19 infection. Studies have shown that in 2020, the city demonstrated the highest prevalence rates, accounting for 49.3% of the total cases in the country [18]. Health resources, including ICU beds, were also found inadequate at that time [16]. Taken together, this indicates that the overall healthcare infrastructure of the region might be insufficient to meet the population's needs, and the distinctive characteristics of Makkah City, in particular, add another layer to the issue. Therefore, a strategic approach is needed to address current resource allocation challenges.
Similarly, we have found that the Jeddah health region exhibited a low bed-to-population ratio, underscoring a significant shortfall in hospital bed availability. This is of particular concern given that Jeddah city's estimated population growth rate is 3.8 per year, a growing rate surpassing the national average [18]. It is also the second biggest urban city in the country. In addition, as of 2022, the city contains 13 public and 32 private hospitals [9]. It has been indicated that the public sector contributes to 80% of the total bed capacity in the country [19]. This scenario could partly explain the low bed-to-population ratio observed in this study, given the low number of public hospitals in Jeddah. Additionally, the imbalanced growth in the number of beds and population size, particularly in populous health regions, could play a significant role [20]. A further factor that comes into play is urbanization. Alhomaidhi [21] suggests that rapid urbanization in Riyadh city presents challenges in efficiently distributing healthcare services. However, having adequate numbers of hospital beds and the flexibility to use them is crucial to managing any unexpected rise in demand for health services [22].
Similar to the Makkah region, the Jeddah health region also witnesses a notable insufficiency in primary healthcare centers. Geographical access in the region persists as a challenge; some populations within the boundaries of Jeddah city still lack geographical access to healthcare [23]. This observation is confirmed by Alabbasi et al., who reported that the capacity of PHCs in the city of Jeddah is still insufficient to satisfy population demand despite current reforms [24]. Thus, a more nuanced understanding of why inequalities in health resources exist in populous regions/cities such as the Jeddah region is warranted. Also, research on how the geographic presence of primary healthcare facilities influences hospital admission and occupancy rate of hospital beds is essential.
The findings of this study also indicate that among the 20 health regions in Saudi Arabia, Al-Jouf and the Northern region represent the highest beds-per-1,000-people ratios. This can be attributed to the fact that these regions are characterized by a small population size in comparison to other regions. It is important to note that the public sector significantly influences bed rates. For instance, it has been indicated that between 2015 and 2019, some health regions in the country witnessed a significant improvement in hospital bed ratio of more than 13% increase, which was partially explained by investments made in the public sector [20]. This regional variation across the country underscores the need to reassess resource allocation to ensure a more equitable distribution of health resources, particularly bed distribution.
Furthermore, we have not analyzed the bed-to-population ratio separately for the public and private sectors in our study. This is due to the current restructuring of the Saudi healthcare system aimed toward privatization. As part of this transition, the private sector will be responsible for the provision of healthcare to meet the demands of a growing population moving forward [19].
Recommendations for future research
While the paper offers valuable insights into the current state of hospital bed distribution in Saudi Arabia and proposes various strategic recommendations, there are opportunities for furthering this research. Future work could explore longitudinal analyses tracking changes in bed distribution over time. This would provide a sense of the effectiveness of current interventions and where adjustments might be needed. Integrating geographic information systems (GIS) in analyzing the spatial distribution of healthcare facilities could offer more nuanced insights into accessibility issues. Such data could be invaluable for precision policymaking and in the location of new healthcare infrastructure investments.
Ultimately, the study provides a starting point for an ongoing conversation and research into how best to achieve a more equitable distribution of healthcare resources in Saudi Arabia and how to develop a system that adjusts dynamically to the evolving healthcare needs of its population. Future research should continue to capture the complexities of the healthcare system and strive for methodologies that can influence policymaking substantively and sustainably.
Limitations
While providing valuable insights into the distribution of hospital beds across Saudi Arabia, this study is subject to certain limitations. Firstly, the reliance on secondary data from the Saudi Ministry of Health (MOH) Statistical Yearbook 2022 means that the findings depend on this data's accuracy and comprehensiveness. While the MOH Yearbook is a reputable source, the data may not capture real-time changes or the nuances of bed availability, such as the distinction between different types of hospital beds (e.g., general vs. intensive care units).
Another limitation is the study's focus on quantitative data, which overlooks qualitative aspects such as patient satisfaction, quality of care, and the actual utilization of hospital beds. These factors are crucial in understanding the effectiveness of healthcare services and the true impact of bed distribution on patient outcomes.
Additionally, the study does not account for the distribution of other healthcare resources like medical staff, equipment, and facilities, which are integral to the overall healthcare delivery system. The availability of hospital beds is just one aspect of healthcare infrastructure, and a comprehensive assessment requires a broader view of resource allocation. Lastly, the study's scope is limited to 2022, providing a snapshot rather than a longitudinal perspective. Trends in bed distribution over time and the impact of recent healthcare reforms and investments are beyond the scope of this analysis.
Conclusion
The findings of this study underscore a critical juncture in the evolution of Saudi Arabia's healthcare system, marked by the challenge of balancing the rapid development of healthcare infrastructure with the equitable distribution of resources. The findings revealed a national average beds-per-1,000-people ratio of 2.43, with some regional disparities. Health regions such as Al-Jouf and the Northern region exhibited higher ratios, indicating a robust healthcare infrastructure. The observed regional disparities in hospital bed availability, particularly in populous regions like Makkah and Jeddah, highlight a significant gap in meeting the healthcare needs of the entire population. This imbalance not only reflects on the current state of healthcare accessibility but also raises concerns about the system's preparedness to handle the increasing burden of non-communicable diseases and the needs of an aging population. The study's insights into these disparities are instrumental in guiding future healthcare policies and strategies, aligning with the ambitious goals of Saudi Vision 2030.
Supplementary Information
Authors’ contributions
Waleed Kattan was responsible for conceiving the presented idea and making a substantial contribution to the concept of the article, acquisition, and analysis of the data. Noor Alshareef has contributed to the interpretation of data for the article and for revising it critically for important intellectual content. All authors edited, reviewed, and approved the final manuscript.
Funding
This research received no external funding.
Availability of data and materials
The datasets generated and analyzed during the current study are available in supplementary files. The data are provided in two Excel files:1.2022 MOH data_Ch1_Demographics.xlsx: This file contains demographic data relevant to the study, including population statistics and other pertinent demographic information.2.2022 MOH data_Ch2_Resources.xlsx: This file includes data on healthcare resources, such as the distribution of hospital beds and other medical facilities across various regions.The data supporting the findings of this study are derived from publicly available sources. The analysis was based on data obtained from the Saudi Ministry of Health (MOH) Statistical Yearbook 2022. This dataset provides detailed information on the distribution of hospital beds across the administrative regions of Saudi Arabia. The MOH Statistical Yearbook 2022 is accessible online at the Saudi Ministry of Health's official website: https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Pan J, Shallcross D. Geographic distribution of hospital beds throughout China: a county-level econometric analysis. Int J Equity Health. 2016;15:179. 10.1186/s12939-016-0467-9. 10.1186/s12939-016-0467-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rice N, Smith PC. Ethics and geographical equity in health care. J Med Ethics. 2001;27(4):256–61. 10.1136/jme.27.4.256. 10.1136/jme.27.4.256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Omrani-Khoo H, Lotfi F, Safari H, Zargar Balaye Jame S, Moghri J, Shafii M. Equity in distribution of health care resources; assessment of need and access, using three practical indicators. Iran J Public Health. 2013;42(11):1299–308. [PMC free article] [PubMed] [Google Scholar]
- 4.A rethink on measuring health inequalities using the Gini Coefficient - UQ eSpace. https://espace.library.uq.edu.au/view/UQ:352576. Accessed 21 July 2024.
- 5.Al-Hanawi MK. Socioeconomic determinants and inequalities in the prevalence of non-communicable diseases in Saudi Arabia. Int J Equity Health. 2021;20:174. 10.1186/s12939-021-01510-6. 10.1186/s12939-021-01510-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tian F, Pan J. Hospital bed supply and inequality as determinants of maternal mortality in China between 2004 and 2016. Int J Equity Health. 2021;20(1):51. 10.1186/s12939-021-01391-9. 10.1186/s12939-021-01391-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.The World Bank. Hospital beds (per 1000 people). The World Bank Data. https://ourworldindata.org/grapher/hospital-beds-per-1000-people. Published 2022. Accessed November 29, 2023. - Google Search. https://www.google.com/search?q=The+World+Bank.+Hospital+beds+(per+1000+people).+The+World+Bank+Data.+https%3A%2F%2Fourworldindata.org%2Fgrapher%2Fhospital-beds-per-1000-people.+Published+2022.+Accessed+November+29%2C+2023.&rlz=1C5CHFA_enUS811US811&oq=The+World+Bank.+Hospital+beds+(per+1000+people).+The+World+Bank+Data.+https%3A%2F%2Fourworldindata.org%2Fgrapher%2Fhospital-beds-per-1000-people.+Published+2022.+Accessed+November+29%2C+2023.&gs_lcrp=EgZjaHJvbWUyBggAEEUYOTIGCAEQRRhA0gEHMzcyajBqN6gCALACAA&sourceid=chrome&ie=UTF-8. Accessed 22 July 2024.
- 8.OECD. Health at a Glance: Europe 2022: State of Health in the EU Cycle. Organisation for Economic Co-operation and Development; 2022. https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-europe-2022_507433b0-en. Accessed 22 July 2024.
- 9.MOH. MOH. MOH Statistical Yearbook - 2022. MOH.GOV.SA. https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx. Published 2022. - Google Search. https://www.google.com/search?q=MOH.+MOH+Statistical+Yearbook+-+2022.+MOH.GOV.SA.+https%3A%2F%2Fwww.moh.gov.sa%2Fen%2FMinistry%2FStatistics%2Fbook%2FPages%2Fdefault.aspx.+Published+2022.&rlz=1C5CHFA_enUS811US811&oq=MOH.+MOH+Statistical+Yearbook+-+2022.+MOH.GOV.SA.+https%3A%2F%2Fwww.moh.gov.sa%2Fen%2FMinistry%2FStatistics%2Fbook%2FPages%2Fdefault.aspx.+Published+2022.&gs_lcrp=EgZjaHJvbWUyBggAEEUYOTIGCAEQRRg80gEIMTYzMWowajeoAgCwAgA&sourceid=chrome&ie=UTF-8. Accessed 22 July 2024.
- 10.Al-Hanawi MK, Khan SA, Al-Borie HM. Healthcare human resource development in Saudi Arabia: emerging challenges and opportunities-a critical review. Public Health Rev. 2019;40:1. 10.1186/s40985-019-0112-4. 10.1186/s40985-019-0112-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.El-Farouk A. Geographical distribution of health resources in the Kingdom of Saudi Arabia : is it equitable? Egypt J Environ Change. 2016;8:4–20. 10.12816/0038449. 10.12816/0038449 [DOI] [Google Scholar]
- 12.Boettiger DC, Lin TK, Almansour M, et al. Projected impact of population aging on non-communicable disease burden and costs in the Kingdom of Saudi Arabia, 2020–2030. BMC Health Serv Res. 2023;23(1):1381. 10.1186/s12913-023-10309-w. 10.1186/s12913-023-10309-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Af Ugglas B, Djärv T, Ljungman PLS, Holzmann MJ. Association between hospital bed occupancy and outcomes in emergency care: a cohort study in Stockholm Region, Sweden, 2012 to 2016. Ann Emerg Med. 2020;76(2):179–90. 10.1016/j.annemergmed.2019.11.009. 10.1016/j.annemergmed.2019.11.009 [DOI] [PubMed] [Google Scholar]
- 14.Siverskog J, Henriksson M. The health cost of reducing hospital bed capacity. Soc Sci Med. 1982;2022(313):115399. 10.1016/j.socscimed.2022.115399. 10.1016/j.socscimed.2022.115399 [DOI] [PubMed] [Google Scholar]
- 15.Al-Sheddi A, Kamel S, Almeshal AS, Assiri AM. Distribution of primary healthcare centers between 2017 and 2021 across Saudi Arabia. Cureus. 15(7):e41932. 10.7759/cureus.41932. [DOI] [PMC free article] [PubMed]
- 16.Arbaein TJ, Alharbi KK, Alfahmi AA, et al. Makkah healthcare cluster response, challenges, and interventions during COVID-19 pandemic: a qualitative study. J Infect Public Health. 2024;17(6):975–85. 10.1016/j.jiph.2024.04.007. 10.1016/j.jiph.2024.04.007 [DOI] [PubMed] [Google Scholar]
- 17.Alrefaei AF, Almaleki D, Alshehrei F, et al. Assessment of health awareness and knowledge toward SARS-CoV-2 and COVID-19 vaccines among residents of Makkah. Saudi Arabia Clin Epidemiol Glob Health. 2022;13:100935. 10.1016/j.cegh.2021.100935. 10.1016/j.cegh.2021.100935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alkhaldy IA. GIS application for modeling covid-19 risk in the Makkah region, Saudi Arabia, based on population and population density. Egypt J Environ Change. 2020;12(2):13–30. 10.21608/ejec.2020.115873 [DOI] [Google Scholar]
- 19.Rahman R. The privatization of health care system in Saudi Arabia. Health Serv Insights. 2020;13:1178632920934497. 10.1177/1178632920934497. 10.1177/1178632920934497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hawsawi T, Abouammoh N. Distribution of hospital beds across Saudi Arabia from 2015 to 2019: a cross-sectional study. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit. 2022;28(1):23–30. 10.26719/emhj.22.003. 10.26719/emhj.22.003 [DOI] [PubMed] [Google Scholar]
- 21.Alhomaidhi A. Geographic distribution of public health hospitals in Riyadh. Saudi Arabia Geogr Bull. 2019;60(1):25–48. [Google Scholar]
- 22.OECD. Hospital beds and occupancy. Published online 2023. https://www.oecd-ilibrary.org/content/component/bdd23022-en.
- 23.Murad A, Faruque F, Naji A, et al. Optimizing health service location in a highly urbanized city: multi criteria decision making and P-Median problem models for public hospitals in Jeddah City, KSA. PLoS ONE. 2024;19(1):e0294819. 10.1371/journal.pone.0294819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Alabbasi KH, Kassim S, Alsharif A, Kruger E, Tennant M. Evaluating population-based geographic access to primary healthcare services in Jeddah second cluster, Saudi Arabia. Int J Med Dev Ctries. 2023;7(11):1460–1460. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated and analyzed during the current study are available in supplementary files. The data are provided in two Excel files:1.2022 MOH data_Ch1_Demographics.xlsx: This file contains demographic data relevant to the study, including population statistics and other pertinent demographic information.2.2022 MOH data_Ch2_Resources.xlsx: This file includes data on healthcare resources, such as the distribution of hospital beds and other medical facilities across various regions.The data supporting the findings of this study are derived from publicly available sources. The analysis was based on data obtained from the Saudi Ministry of Health (MOH) Statistical Yearbook 2022. This dataset provides detailed information on the distribution of hospital beds across the administrative regions of Saudi Arabia. The MOH Statistical Yearbook 2022 is accessible online at the Saudi Ministry of Health's official website: https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx.