

Abstract
Pediatric carpal fractures are rare and often difficult to detect. This paper reviews the current literature on pediatric non-scaphoid carpal fractures, with a case report of a lunate fracture associated with a distal radius and ulnar styloid fracture, managed nonoperatively in a 12-year-old boy. There is lack of consensus regarding the management of these fractures due to the low number of reported cases. A frequent lack of long-term follow-up limits our understanding of the outcomes, but good outcomes have been reported for both nonoperative and operative management. This case report brings attention to the current time period for the definition of delayed union in pediatric carpal fractures, and emphasizes the need for prolonged follow-up for the detection of delayed complications leading to functional impairment.
Keywords: Pediatrics, Lunate bone, Carpal bones, Closed fractures, Ununited fractures
INTRODUCTION
Pediatric carpal fractures are clinically rare due to anatomical factors and diagnostic challenges. The carpal bones develop via secondary ossification, meaning that at birth, the ossification centers are surrounded by spherical growth plates, which act as protective barriers against injury. The lunate has no calcification until after the age of 2 years. As a child reaches adolescence, the critical bone to cartilage ratio is attained, resulting in an increased risk of carpal bone fractures. These injuries are difficult to detect due to the low sensitivity of radiographs in the cartilaginous immature skeleton, potential obscuration with physeal lines, and incompletely ossified carpal bones; therefore, subtle pathology may be easily missed. Furthermore, this particular patient group may struggle to express and localize pain, and may be difficult to examine.
Pediatric carpal fractures are commonly seen in combination with other fractures or dislocations [1,2], particularly distal radius fractures; therefore, the initial assessment requires a thorough review for secondary injuries. Damage to pediatric bones, particularly around the physeal plates and growth centers, may have long-term consequences with the potential for delayed complications [3]. The most appropriate management pathway in pediatric patients remains elusive, as does the understanding of the long-term sequalae of carpal delayed unions or nonunions in this cohort, due to their rarity.
This paper reviews the current literature on pediatric carpal fractures, utilizing our own case report as an example of delayed complications after nonoperative management. It highlights the need for long-term follow-up and vigilance for possible complications resulting from injury to the immature bones.
CASE REPORT
A 12-year-old boy presented following a fall onto his dominant hand from his bicycle with a closed right wrist injury (Figs. 1, 2). Radiographs demonstrated a dorsally displaced Salter-Harris type III fracture of the distal radius associated with a displaced lunate (equivalent to type IV in the Teisen classification) and ulnar styloid fracture. The patient complained of reduced sensation and “tingling” in the median nerve territory; however, the motor power remained Medical Research Council grade 5 in all muscle groups. The wrist was placed in a dorsal back-slab, after which computed tomography (CT) scanning further delineated the fracture pattern.
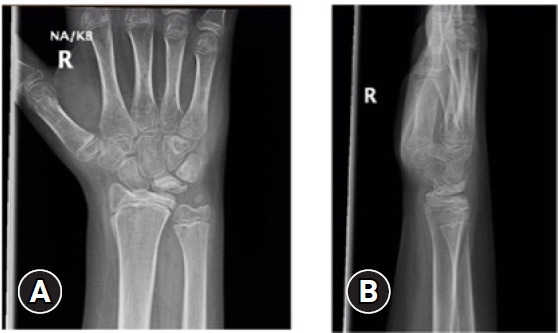
Fig. 1.

Wrist x-ray images at presentation. Salter-Harris III fracture of distal radius dorsally displaced, ulnar styloid fracture, and lunate fracture. (A) Anteroposterior view. (B) Lateral view.
Fig. 2.
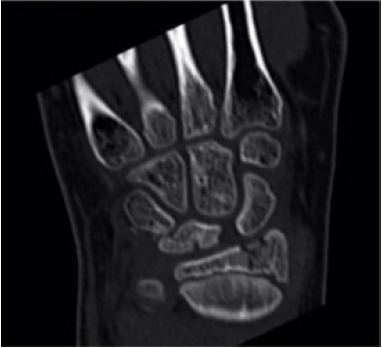
Coronal computed tomography image of wrist confirming distal radius and lunate fracture.
The following morning, the patient underwent manipulation under anesthesia with reapplication of a dorsal plaster as demonstrated in Fig. 3. Satisfactory reduction of the distal radius fracture was achieved; however, the lunate and ulnar styloid fractures remained displaced. Sensation started to return to normal the next day, but it did not settle completely.
Fig. 3.

Intraoperative fluoroscopy demonstrating reduction of distal radius.
Ten days postoperation, radiographs demonstrated maintained reduction of the distal radius (Fig. 4); therefore, the patient was switched to a lightweight cast for 5 further weeks. At 7 weeks, radiographs demonstrated satisfactory union of the distal radius but no signs of healing of the ulnar styloid or lunate fractures. The median nerve sensory symptoms had completely resolved. The cast was removed, and range of motion exercises began. The wrist was initially stiff, with no tenderness to palpation over the distal radius, ulnar or lunate and movements were pain-free. The patient and parents declined physiotherapy input.
Fig. 4.
Wrist x-ray images at 6 weeks, demonstrating union of distal radius fracture with no evidence of healing of lunate and ulnar styloid fractures. (A) Anteroposterior view. (B) Lateral view.
Eight weeks postinjury, magnetic resonance imaging demonstrated a nonunited fracture of the lunate without signs of avascular necrosis (Fig. 5). At 6 months the patient had no symptoms, with a full, pain-free range of motion at the wrist, without tenderness. The patient returned to sports without any functional deficit. Radiographs were deemed unnecessary due to the absence of any symptoms.
Fig. 5.
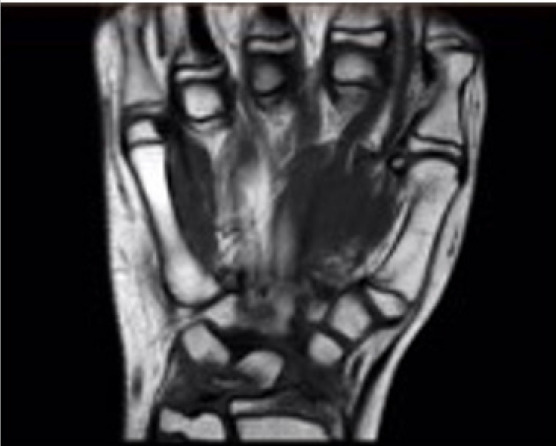
Coronal magnetic resonance imaging of the wrist confirming no evidence of healing of lunate fracture.
Three years following the injury, the patient developed pain in the ipsilateral wrist. His Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire score was 8.3 and his Mayo Wrist Score was 90, with moderate pain in the arm and hand, mild difficulty during recreational activities requiring force or impact through bone, and slight limitation to social activities. His range of movement was limited in flexion and extension compared to the noninjured side. Pronation and supination were unaffected. These results are demonstrated in Table 1.
Table 1.
Range of movement in the noninjured limb versus the injured limb, 3 years after injury
| Movement | Range of movement (°) |
|
|---|---|---|
| Left (noninjured) | Right (injured) | |
| Flexion | 85 | 75 |
| Extension | 70 | 60 |
| Pronation | 90 | 90 |
| Supination | 90 | 90 |
Radiographs revealed abnormal posttraumatic morphology (Fig. 6): partial closure of the distal radial physeal plate or posttraumatic bony bridging with evidence of distal radius growth arrest resulting in a (new) positive ulnar variance.
Fig. 6.

Wrist x-ray images showing early closure of the distal radial growth plate and consequent ulnar variance. (A) Anteroposterior view. (B) Lateral view.
It should be noted that the case we present was additionally complex due to the presence of a concomitant distal radius fracture. The standard management of distal radius fractures was described by Carson et al. in 2006, who stated that “fractures of the distal radial physis … heal quickly … requiring only 3 to 4 weeks of immobilization” [4,5]. In addition, the evidence suggests that 4 to 8 weeks of immobilization is appropriate for conservative scaphoid fracture management [4,6]. There is very sparse further research available to recommend how to manage other carpal fractures in the pediatric population; therefore, we used this evidence. Furthermore, a clinical examination is preferred to a radiographic evaluation in young children with hand and wrist injuries for two reasons: (1) reducing exposure of the patient to ionizing radiation; and (2) incomplete ossification of the carpal bones, which makes fracture assessment difficult on plain radiographs. Thus, we provided immobilization until clinical union (i.e., the absence of pain at the fracture site on palpation, stressing of the fracture, or during range of motion exercises).
Ethics statement
Informed consent for publication of the research details and clinical images was obtained from the patient.
DISCUSSION
The lunate’s anatomical position and surrounding structures may explain why lunate fractures are often associated with other bony and soft tissue injuries, and may result in instability and pain. The lunate is the central carpal bone in the proximal row, and its position makes it difficult to view radiographically as there is significant overlap with other carpals on many radiographic views [7]. It is crescent-shaped, with a convex articular facet facing the radius, and a concave single or dual articular surface distally, facing the capitate. Along with the triquetrum and scaphoid, the lunate forms the distal articular surface of the radiocarpal joint and it articulates with the triangular fibrocartilage complex. Multiple ligamentous attachments of the lunate, including the scapholunate and lunotriquetral ligaments, indicate dislocation as an inherently severe injury. One proposed mechanism of lunate fracture is direct axial compression, driving the capitate into the lunate. There are few evidence-supported risk factors for lunate fractures, but one appears to be positive ulnar variance [8].
Adult lunate fractures are categorized using the Teisen classification system, based on the anatomic orientation of fracture patterns [9]; however, these do not provide prognostic value. They can be recognized by disruption of the radius-lunate-capitate axis on a lateral radiograph (normal axis demonstrated in Fig. 7), if it is not clear on the anteroposterior view [10].
Fig. 7.

Demonstrating the radius-lunate-capitate view on a lateral anatomically normal x-ray.
In adults, the lunate is mainly covered in cartilage, and it is therefore relatively insensate [11]. Its vascular supply is often twofold, with dorsal and palmar surfaces supplied by the radiocarpal and intercarpal arch; however, 20% of all lunates have a single-vessel supply [12]. This means that missed lunate fractures may lead to avascular necrosis and resulting chronic pain, which is termed Kienböck disease [13]. Only one case report [14] thus far has documented the progression of a pediatric lunate fracture to Kienböck disease, with unclear original pathology. However, there may be reporting bias regarding this possibility due to a lack of thorough follow-up.
Pediatric fractures involve a growth plate in 15% to 30% of cases [15], often at the distal radius. The most commonly fractured carpal bone in children is the scaphoid, with an incidence of 0.4% of all pediatric fractures [16]. Of carpal bone fractures, scaphoid fractures are the most common (73.5%), followed by triquetral fractures (18.0%), with lunate fractures making up a significantly smaller proportion of the total (0.5%) [9].
Pediatric lunate fractures are rare, and as a result, little high-level evidence has been published. The evidence found in a literature search is presented in Table 2 [14,17–27]. Current management is often based on case series and reports of other carpal fractures, often in adult populations.
Table 2.
Case reports of pediatric carpal fractures (excluding scaphoid fractures)
| Study | Carpal | Displacement | Age (yr) | Sex | Detection | Imaging | Mechanism of injury | Management | Outcome | X-ray finding | Range of motion |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Adler and Shaftan [17] (1962) | Capitate | None | 17 | Male | Immediate | X-ray | Fall | C | Union | Full | |
| Young [18] (1986) | Capitate | None | 10 | Male | Immediate | X-ray | Fall (from 2 m) | C | 3 mo | Union | Full |
| Gibbon and Jackson [19] (1989) | Capitate | None | 9 | Male | Delay of 24 day | X-ray | FOOSH | C | 3.5 wk | Sclerosis | - |
| Wulff and Schmidt [20] (1998) | Capitate | None | 13 | Female | Immediate | - | MTC | C | 6 wk | Union | - |
| Wulff and Schmidt [20] (1998) | Triquetrum | None | 12 | Female | Immediate | - | Fall (from 1 m) | C | 4 wk | Union | - |
| Wulff and Schmidt [20] (1998) | Trapezoid | None | 14 | Female | Immediate | - | MTC | C | 4 wk | Union | - |
| Wulff and Schmidt [20] (1998) | Hamate | None | 16 | Male | Immediate | - | MTC | C | 3 wk | Union | - |
| Sawant and Miller [21] (2000) | Capitate | - | 12 | Male | Delay of 24 hr | X-ray | MTC | S | 3 yr | Union | Flexion 70° (vs. 90°) Extension 85° (95°), Normal grip strength |
| Ferlic et al. [14] (2003) | Lunate | None | 13 | Male | Delayed presentation (6 months) | X-ray + MRI | Nontraumatic | S | 30 mo | Union | Flexion, 68°, Extension 45° |
| Kuniyoshi et al. [22] (2005) | Capitate | None | 6 | Male | Delayed presentation (3 months) | X-ray + MRI | Wrist caught in iron gates | C | 14 mo | Union | Full |
| Horras et al. [23] (2012) | Triquetrum | Yes | 14 | Male | Immediate | MRI | FOOSH | C | 6 wk | Union | Full |
| Cooney and Stuart [24] (2013) | Capitate | Minimal | 16 | Male | Delayed presentation (2 months) | X-ray + CT | FOOSH | C + delayed S + bone graft | 18 wka) | Delayed union post-ORIF | - |
| Hurni et al. [25] (2015) | Pisiform | Yes | 11 | Male | Immediate | CT | MTC | S | 3 mo | Union | Full |
| Covelli et al. [26] (2018) | Pisiform | Yes | 13 | Male | Delayed presentation (3 months) | MRI | Nontraumatic | C | No mention of follow-up | - | |
| Rodriguez-Alejandro et al. [27] (2021) | Hamate | None | 12 | Male | Delayed presentation (3 months) | MRI | Hitting ball with a baseball bat | S | Excision of hook of hamate after nonunion detected | Nonunion (excised hook of hamate) | Full |
C, conservative; FOOSH, fall on an outstretched hand; MTC, motor traffic collision; S, surgical; MRI, magnetic resonance imaging; CT, computed tomography; ORIF, open reduction and internal fixation.
Sclerosis only; delayed ORIF + bone grafting to union, 38 weeks postfixation union + wrist flexion to 80°, wrist extension to 60°.
Nonunion of pediatric carpal fractures is extremely rare, with the first reported nonunion of a pediatric scaphoid fracture described by Southcott and Rosman [28] in 1977. Despite their scarcity in the literature, more recently, Rodriguez-Alejandro et al. [27] reported the case of a hook of hamate nonunion in a 12-year-old baseball player. This case likely resulted in nonunion due to repeated misdiagnoses on sequential plain radiographs by multiple healthcare professionals. The definitive and successful management involves surgical excision of the hook of hamate. That case report described a full return of function and no patient complaints 2 years after operation.
Previous case reports have demonstrated good long-term results from both nonoperative and operative management of pediatric carpal fractures, but the length of follow-up has often been a limitation. Most reports only have a 3-year follow-up, which may not be sufficient to understand the long-term consequences of these injuries.
A case report by Bhatnagar et al. [29] highlighted a good clinical outcome following nonoperative management of an active 11-year-old boy with multiple carpal fractures. They demonstrated asymptomatic full range of motion of the wrist at a 3-year follow-up, despite CT scanning at this stage showing nonunion of the hamate fracture.
Clarke et al. [30] reported a case of an 11-year-old boy with spontaneous union 2 years following a conservatively managed waist-of-scaphoid fracture. This caused persistent wrist pain between 18 and 24 months, prior to radiographic evidence of union. This may highlight the need to review the pediatric definition of healing timelines when defining delayed union and nonunion in children.
Similarly, there have been good clinical outcomes with operative management. Kamano et al. [31] showed effective results in a child with multiple carpal fractures treated with wire fixation and followed for 29 months. In 2009, Foley and Patel [32] also demonstrated similar outcomes in a 10-year-old boy treated with Kirschner wires for scaphoid, capitate, and triquetrum fractures. In this patient, bone union was achieved and there was pain-free full range of movement of the wrist at a 1-year follow-up. DeCoster et al. [33] also reported initial good clinical outcomes following open reduction with internal fixation of distal radius, scaphoid, lunate, and triquetral fractures with gross displacement in a 10-year-old boy at 1 year, but described delayed abnormal carpal development. Ferlic et al. [14] operatively managed a delayed presentation of Kienböck disease with radial shortening.
There is evidence for management of other carpal injuries, with established protocols for scaphoid nonunion in the pediatric population to be anatomically reduced with stable fixation, with or without bone grafting. The management of other types of carpal nonunion in children, and particularly the lunate, is much less clear. Wyrick et al. [34] advocated for open reduction and internal fixation in all displaced pediatric carpal fractures.
In our case, the patient was nonoperatively managed following the initial reduction of the distal radius fracture. However, the following questions remain: (1) What follow-up time is appropriate for pediatric carpal fractures to identify delayed consequences of injury, and delayed union? (2) Should lunate fixation be performed at the primary operation? (3) Is lunate nonunion detrimental to wrist function and does it cause chronic pain? (4) Should delayed open reduction with internal fixation, with or without bone grafting, be performed simply to achieve union or only in the presence of symptoms?
CONCLUSIONS
Pediatric carpal fractures are rare and easily missed, and their long-term impact remains unknown. A high index of suspicion is required in order to make an accurate diagnosis and ensure that occult injuries are not missed. No evidence exists regarding the specific management of pediatric lunate fractures, and good outcomes have been reported in both operatively and nonoperatively managed cases. The rate of Kienböck disease is unclear in the pediatric population. We present a case of nonoperative management based on the patient’s symptoms. Although successful in the short to mid-term, this has resulted in some limitation of function after 3 years. We are still unable to comment on the long-term prognosis of this injury, but will continue to follow his progress. If a nonoperative approach is to be taken, we recommend immobilization in a cast for a minimum of 4 weeks and a maximum of 8 weeks.
Footnotes
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for this study.
Author contributions
Conceptualization: all authors; Formal analysis: all authors; Methodology: al authors; Project administration: all authors; Visualization: all authors; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.
REFERENCES
- 1.Goddard N. Carpal fractures in children. Clin Orthop Relat Res. 2005;(432):73–6. doi: 10.1097/01.blo.0000156003.24374.ab. [DOI] [PubMed] [Google Scholar]
- 2.Vigler M, Aviles A, Lee SK. Carpal fractures excluding the scaphoid. Hand Clin. 2006;22:501–16. doi: 10.1016/j.hcl.2006.07.007. [DOI] [PubMed] [Google Scholar]
- 3.Nellans KW, Chung KC. Pediatric hand fractures. Hand Clin. 2013;29:569–78. doi: 10.1016/j.hcl.2013.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Woolridge DP, Kilgore K. Pediatric upper extremity injuries. Pediatr Clin North Am. 2006;53:41–67. doi: 10.1016/j.pcl.2005.10.003. [DOI] [PubMed] [Google Scholar]
- 5.Bochang C, Jie Y, Zhigang W, Weigl D, Bar-On E, Katz K. Immobilisation of forearm fractures in children. J Bone Joint Surg Br. 2005;87:994–6. doi: 10.1302/0301-620X.87B7.15774. [DOI] [PubMed] [Google Scholar]
- 6.Vahvanen V, Westerlund M. Fracture of the carpal scaphoid in children: a clinical and roentgenological study of 108 cases. Acta Orthop Scand. 1980;51:909–13. doi: 10.3109/17453678008990893. [DOI] [PubMed] [Google Scholar]
- 7.Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJ. MDCT and radiography of wrist fractures: radiographic sensitivity and fracture patterns. AJR Am J Roentgenol. 2008;190:10–6. doi: 10.2214/AJR.07.2699. [DOI] [PubMed] [Google Scholar]
- 8.Titus SJ, Deitche WS. In: The sports medicine resource manual. Seidenberg PH, Beutler AI, editors. Saunders; 2008. Chapter 18: wrist and hand fractures. [Google Scholar]
- 9.Teisen H, Hjarbaek J. Classification of fresh fractures of the lunate. J Hand Surg Br. 1988;13:458–62. doi: 10.1016/0266-7681_88_90180-5. [DOI] [PubMed] [Google Scholar]
- 10.Kannikeswaran N, Sethuraman U. Lunate and perilunate dislocations. Pediatr Emerg Care. 2010;26:921–4. doi: 10.1097/PEC.0b013e3181fe915b. [DOI] [PubMed] [Google Scholar]
- 11.Cooney WP. The wrist: diagnosis and operative treatment. 2nd ed. Lippincott Williams & Wilkins; 2010. [Google Scholar]
- 12.Kaewlai R, Avery LL, Asrani AV, Abujudeh HH, Sacknoff R, Novelline RA. Multidetector CT of carpal injuries: anatomy, fractures, and fracture-dislocations. Radiographics. 2008;28:1771–84. doi: 10.1148/rg.286085511. [DOI] [PubMed] [Google Scholar]
- 13.Bedel C, Coskun G, Turkoglu S. Avascular necrosis of lunate bone: Kienbock disease. J Surg Med. 2018;2:387–8. [Google Scholar]
- 14.Ferlic RJ, Lee DH, Lopez-Ben RR. Pediatric Kienböck’s disease: case report and review of the literature. Clin Orthop Relat Res. 2003;(408):237–44. doi: 10.1097/00003086-200303000-00031. [DOI] [PubMed] [Google Scholar]
- 15.Mizuta T, Benson WM, Foster BK, Paterson DC, Morris LL. Statistical analysis of the incidence of physeal injuries. J Pediatr Orthop. 1987;7:518–23. doi: 10.1097/01241398-198709000-00003. [DOI] [PubMed] [Google Scholar]
- 16.Faouzi HM. Scaphoid fracture associated with distal radius fracture in children: a case report. Chin J Traumatol. 2009;12:187–8. [PubMed] [Google Scholar]
- 17.Adler JB, Shaftan GW. Fractures of the capitate. J Bone Joint Surg Am. 1962;44:1537–47. [PubMed] [Google Scholar]
- 18.Young TB. Isolated fracture of the capitate in a 10-year-old boy. Injury. 1986;17:133–4. doi: 10.1016/s0020-1383(86)80014-6. [DOI] [PubMed] [Google Scholar]
- 19.Gibbon WW, Jackson A. An isolated capitate fracture in a 9-year-old boy. Br J Radiol. 1989;62:487–8. doi: 10.1259/0007-1285-62-737-487. [DOI] [PubMed] [Google Scholar]
- 20.Wulff RN, Schmidt TL. Carpal fractures in children. J Pediatr Orthop. 1998;18:462–5. [PubMed] [Google Scholar]
- 21.Sawant M, Miller J. Scaphocapitate syndrome in an adolescent. J Hand Surg Am. 2000;25:1096–9. doi: 10.1053/jhsu.2000.18494. [DOI] [PubMed] [Google Scholar]
- 22.Kuniyoshi K, Toh S, Nishikawa S, Kudo S, Ogawa T, Pegoli L. Long-term follow-up of a malunited, isolated fracture of the capitate in a 6-year-old boy. J Pediatr Orthop B. 2005;14:46–50. doi: 10.1097/01202412-200501000-00008. [DOI] [PubMed] [Google Scholar]
- 23.Horras N, Barthlen W, Wildbrett P. A rare case of an isolated triquetrum body fracture in a 14-year-old boy. Afr J Paediatr Surg. 2012;9:157–8. doi: 10.4103/0189-6725.99405. [DOI] [PubMed] [Google Scholar]
- 24.Cooney AD, Stuart PR. Symptomatic nonunion of an isolated capitate fracture in an adolescent. J Hand Surg Eur Vol 2013;38:565–7. [DOI] [PubMed] [Google Scholar]
- 25.Hurni Y, Fusetti C, de Rosa V. Fracture dislocation of the pisiform bone in children: a case report and review of the literature. J Pediatr Orthop B. 2015;24:556–60. doi: 10.1097/BPB.0000000000000210. [DOI] [PubMed] [Google Scholar]
- 26.Covelli J, Schallert EK, Kan JH, Pederson WC. Hamate-pisiform coalition complicated by fracture in a pediatric patient. Radiol Case Rep. 13. Vol. 13. Netherlands: 2018. pp. 1163–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rodriguez-Alejandro OE, Olivella G, Torres-Lugo NJ, Echegaray GJ, Ramirez N, Foy-Parrilla CA. Non-union in a hook of hamate fracture of a skeletally immature baseball player. Trauma Case Rep. 2021;35:100523. doi: 10.1016/j.tcr.2021.100523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Southcott R, Rosman MA. Non-union of carpal scaphoid fractures in children. J Bone Joint Surg Br. 1977;59:20–3. doi: 10.1302/0301-620X.59B1.321463. [DOI] [PubMed] [Google Scholar]
- 29.Bhatnagar G, Crone D, Ahmed H. Paediatric multiple carpal fractures: a case report. Inj Extra. 2008;39:247–9. [Google Scholar]
- 30.Clarke JV, Ramjug SD, Barnes SJ. Established scaphoid nonunion progressing to spontaneous union in a child. Inj Extra. 2006;37:170–1. [Google Scholar]
- 31.Kamano M, Fukushima K, Honda Y. Multiple carpal bone fractures in an eleven-year-old. J Orthop Trauma. 1998;12:445–8. doi: 10.1097/00005131-199808000-00017. [DOI] [PubMed] [Google Scholar]
- 32.Foley K, Patel S. Fractures of the scaphoid, capitate and triquetrum in a child: a case report. J Orthop Surg (Hong Kong) 2012;20:103–4. doi: 10.1177/230949901202000121. [DOI] [PubMed] [Google Scholar]
- 33.DeCoster TA, Faherty S, Morris AL. Case report: pediatric carpal fracture dislocation. J Orthop Trauma. 1994;8:76–8. doi: 10.1097/00005131-199402000-00017. [DOI] [PubMed] [Google Scholar]
- 34.Wyrick JD, Youse BD, Kiefhaber TR. Scapholunate ligament repair and capsulodesis for the treatment of static scapholunate dissociation. J Hand Surg Br. 1998;23:776–80. doi: 10.1016/s0266-7681(98)80095-8. [DOI] [PubMed] [Google Scholar]