

ABSTRACT
Protamine, first isolated from salmon fish sperm and now produced through recombinant biotechnology, is an antidote that neutralizes the anticoagulant properties of heparin. Protamine function is based on the capacity to dissociate the heparin–antithrombin III (AT III) complex (an important link that promotes blood fluidification by inhibiting coagulation), forming the inactive heparin–protamine complex. Protamine has itself dose-dependent anticoagulant properties: It interferes with coagulation factors and platelet function; it stimulates fibrinolysis; it can lead to thrombocytopenia and reduction in thrombin-related platelet aggregation; it decreases platelet response to thrombin receptor agonist in a dose-dependent manner. In this review, we will focus on protamine and its interaction with heparin. Notably, protamine is able to antagonize not only unfractionated heparin (UFH) but also low molecular weight heparins to various degrees. Protamine-allergic and anaphylactoid systemic reactions may affect up to 1 in 10 people and should be prevented and treated early.
Keywords: Activated clotting time, bleeding, cardiac anesthesia, cardiopulmonary bypass, coagulation, heparin, protamine
INTRODUCTION
Protamine and heparin play pivotal roles in medicine, especially in the cardiac surgery setting. Protamines are small, nuclear, arginine-rich, basic, positively charged proteins consisting of 32 amino acids, involved in compact folding and stabilization of sperm deoxyribonucleic acid (DNA),[1] and are a common antidote for heparin, a potent anticoagulant.
Protamine was first isolated from salmon fish sperm and is now produced through recombinant biotechnology. It is available in a sulfate or chloride formulation. The former replaced hexadimethrine bromide (Polybrene®), an earlier cationic agent used as the initial heparin reversal agent during the early stages of cardiac surgery, since investigations conducted in the 1960s, indicated that hexadimethrine bromide doses that exceeded their therapeutic range might lead to kidney failure. The latter type was described as being the most resistant to break down by peptidases. The ability to neutralize heparin was first described at the beginning of the twentieth century.[2]
It is noteworthy that protamine also interferes with coagulation factors, specifically the conversion of prothrombin to thrombin, which is involved in platelet function and can stimulate fibrinolysis. Therefore, protamine can cause dose-dependent thrombocytopenia, reduction in thrombin-related platelet aggregation, and a decreased platelet response to thrombin receptor agonists. Because of its strongly positive charge, protamine sulfate or hydrochloride has a higher affinity for heparin than antithrombin III (AT III) and is able to dissociate the heparin–AT III complex, forming an inactive heparin–protamine complex [Figure 1]. It must be administered by intravenous route.
Figure 1.
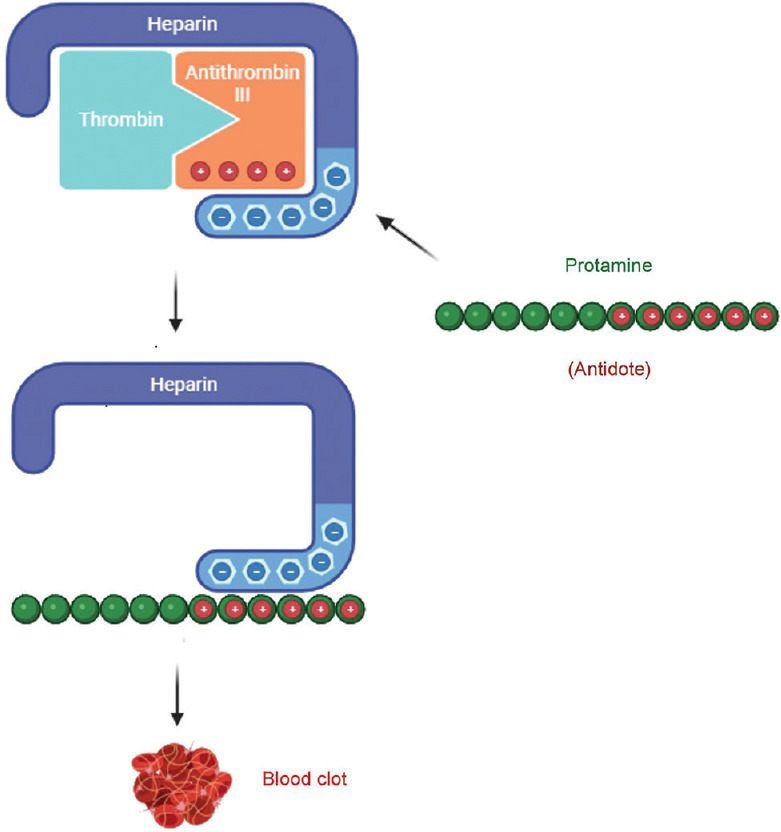
Heparin has an overall high negative charge and can bind with the antithrombin III (AT III)-positive lysine amino acid or with the positive protamine antidote
Furthermore, while the protamine–heparin interaction is well documented and often considered “just” a straightforward ionic interaction, emerging research hints at more intricate molecular dynamics at play, suggesting that there may be additional layers to their actions.
The present review examines the established understanding of protamine and heparin, delves into their multifaceted interactions, and underscores potential scientific knowledge gaps in this field. Of note, unless otherwise specified in the present work, when making reference to “heparin” we intend “unfractionated heparin” (UFH).
Protamine adverse reactions and unforeseen consequences
Protamine administration can lead to systemic reactions. The antigen–antibody response to protamine sulfate results in a type I anaphylactic reaction, ranging from hemodynamic instability, such as transient hypotension and tachycardia to fatal cardiovascular collapse, especially in cardiac surgery settings. Notably, given the high density of histamine-secreting mast cells or basophils in mucosal tissue of both the airways and lungs, the ability of protamine to trigger histamine release in this context was investigated, though in vitro studies failed to demonstrate such an effect at the standard dose commonly administered in clinical settings.[3]
Protamine may also induce IgE-independent anaphylactic and anaphylactoid reactions, causing bradycardia, hypotension, and pulmonary vasoconstriction, leading to pulmonary hypertension and right ventricular dysfunction, two potentially life-threatening clinical complications following the protamine-induced anaphylactic reaction.
Pulmonary hypertension is a potentially life-threatening pathology. Besides chronic conditions related to left heart disease, there are acute reactions due to sudden vasoconstriction of pulmonary arteries caused, for example, by polycations, toxic substances, clots in pulmonary circulation, inflammatory diseases, renal failure, and asbestosis. Hence, preliminary evidence derived from animal models suggests that pretreatment with phosphodiesterase inhibitors (e.g. aminophylline and pentoxifylline) may exhibit a protective effect by attenuating the increase in pulmonary artery pressure and lung weight gain resulting from protamine administration.[4]
Anaphylactic reactions are more common in insulin-dependent diabetic patients due to protamine inclusion in some insulin medical products, such as recombinant human zinc–protamine–insulin (whose absorption and onset of action are delayed by the addition of protamine and zinc, which leads to crystal formation), and in patients with fish protein allergy. Anaphylactic reactions and hemodynamic disturbances are overlapping manifestations of the same pathology, often difficult to discriminate[5,6] [Table 1].
Table 1.
Protamine-allergic and anaphylactoid reactions (including severe anaphylactoid reactions, with IgE-independent mechanism): risk factors, clinical manifestations, and therapeutic options
| Risk factors | Clinical manifestations | Therapeutic options |
|---|---|---|
| Fish protein allergy | Common side effects (may affect up to 1 in 10 people) | Treat symptoms |
| Diabetic patients in zinc–protamine–insulin treatment | -Urticaria | Fluids |
| Rate of infusion | - Angioedema | Vasoconstrictors |
| Prior exposure to protamine (only for protamine chloride) | - Skin and mucous reaction | Antihistaminic |
| Vasectomy (may have circulating anti-protamine antibodies) | - Severe hypotension | Corticosteroids (hydrocortisone) |
| - Bronchospasm | ||
| -Heat or flushing feeling | ||
| Rare side effects (may affect up to one person in 1000) | ||
| -Anaphylactic shock | ||
| - Acute pulmonary hypertension (with or without right ventricular failure or pulmonary edema) | ||
| -Bradycardia | ||
| - Dyspnea | ||
| - Nausea | ||
| - Vomiting | ||
| - Modest and reversible thrombocytopenia |
When allergic reactions manifesting with urticaria or mild blood pressure occur, protamine infusion should be stopped, and standard symptomatic management should be followed. If, instead, patients exhibit potentially life-threatening conditions indicative of anaphylaxis (e.g., vasodilatory shock and acute cardiopulmonary dysfunction), it is recommended to administer medical treatment (e.g,. epinephrine administration) along with resuscitative measures and/or cardiopulmonary life support.[7] When refractory shock occurs instead, mechanical circulatory support (MCS) devices, including venoarterial extracorporeal membrane oxygenation or reinstitution of cardiopulmonary bypass (CPB), can be implemented.[8]
Calculating the optimal protamine dose
Protamine is routinely administered to overcome the anticoagulant properties of heparin, forming an ionic complex without any anticlotting activity.
Historically, protamine has been given at a 1:1 ratio, relative to the initial or even total dose of heparin previously administered. Furthermore, an additional protamine dose may be administered, aiming to restore homeostasis and reduce microvascular bleeding, rather than entering toward a vicious circle of “more protamine, more bleeding.”
Notably, current guidelines do not recommend protamine dose adjustments either in specific patient populations (i.e., the elderly and children) or in patients with renal or hepatic impairment.
The hemostasis management system (HMS) allows individualized heparin dose titration based on a dose–response test, which results in a tailored and often decreased protamine dose.
An observational study by De Simone et al.[9] showed that a 1:1 protamine-to-heparin ratio is usually not necessary and HMS can lower the total protamine administered thanks to residual heparin measurements at the end of CPB. Although larger studies are needed to clarify the optimal protamine-to-heparin ratio in cardiac surgery, a reasonable approach could be to set a protamine-to-heparin ratio lower than the traditional 1:1 ratio while waiting for further studies. Moreover, residual blood heparin measurement with HMS devices could help to titrate the protamine dose more accurately.
Noteworthy, a single-center, prospective, observational study by Taneja et al.[10] in a cohort of 28 patients undergoing on-pump cardiac surgery concluded that a 0.5 protamine:cumulative heparin ratio was able to neutralize heparin in >90% of patients.
The algorithmic protamine dosing for reversal of heparin after cardiopulmonary bypass (PRODOSE) trial, a recent original investigation by Miles et al.,[11] sought to compare a customized mathematical model for calculating protamine dosage in a cohort of 228 low bleeding risk patients undergoing on-pump cardiac surgery against the conventional fixed dose ratio (1 mg of protamine per 100 IU of heparin). The authors reported that the utilization of this mathematical model led to improvements in point-of-care (POC) coagulation measurements and a notable 36.6% reduction in protamine administration. Employing mathematical models based on heparin clearance can be safely adopted for protamine dosing, in line with previous pharmacokinetic models developed to determine optimal protamine dosing after therapeutic anticoagulation for CPB.[12,13] Such findings further strengthen the hypothesis that dosing protamine according to the commonly used 1:1 fixed dose ratio is probably excessive in this population, though further research with a focus on clinical outcomes and a population at a higher risk of bleeding is warranted.
The potential consequences when excessive protamine is administered to antagonize heparin are hence to be considered as well. Protamine, having inherent anticoagulant properties, can exacerbate bleeding, a phenomenon known as “paradoxical anticoagulation.” Notably, such anticoagulant properties of protamine rely on its pleiotropic effects. First, reduced platelet function is driven by decreased thrombin generation,[14] inhibition of glycoprotein Ib–von Willebrand factor (GPIb–vWF) activity,[15] and a decreased platelet responsiveness to thrombin receptor agonist peptide.[16] Second, reduced clot strength coupled with a shortened time to lysis results in enhanced fibrinolysis.[17] Lastly, reduced generation or activation of coagulation factors (i.e., thrombin and factors V, VII, and VIII) results in inhibition of coagulation.[18,19,20] This multifactorial mechanism leads to overall impaired platelet function, interference with coagulation factors, and stimulation of clot breakdown, ultimately responsible for the occurrence of bleeding complications [Figure 2].[21] This begs the question of the optimal strategy for heparin antagonism. As described by Suelzu et al.,[22] a protamine dose of 1 mg for every 100 units of administered heparin (1:1 ratio) to reverse residual heparin activity following off-pump coronary artery bypass may be higher than necessary, leading to potential postoperative disruptions in hemostasis. They observed that two-thirds of the total calculated dose of protamine was able to reverse the heparin anticoagulant effect (complete heparin reversal with a 1:0.67 heparin-to-protamine ratio). Additionally, a protamine dose up to a 1:1 ratio seemed to prolong the clotting time; in fact, infusion of the remaining total calculated protamine dose led to significant clotting time elongation. They did not observe modifications in clot firmness. Furthermore, in normothermic conditions (i.e. off-pump coronary artery bypass graft (OPCABG)) compared with hypothermia (i.e., on-pump CABG), the expected reduction in heparin concentration could be higher because of faster heparin turnover.[23]
Figure 2.
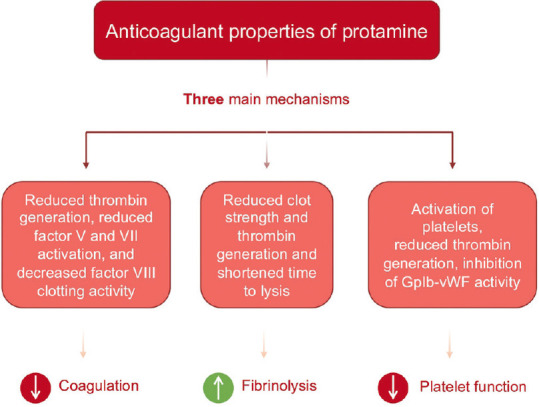
Summary of the three main mechanisms underlying the anticoagulant properties of protamine. GPIb–vWF: glycoprotein Ib–von Willebrand factor
Overdosing protamine leads to an anticoagulant effect and bleeding complications, due to platelet dysfunction, inhibition of glycoprotein Ib–vWF, serine protease activity, and increased fibrinolysis.[23]
Despotis et al.[24] demonstrated that a reduction in the protamine-to-heparin ratio decreased postoperative bleeding and the amount of fresh-frozen plasma and platelet administration after CPB.
However, protamine excess and related clinical significance in terms of bleeding constitute an open question.
Previous studies described platelet function impairment with a higher ratio of protamine. Particularly, Gertler and coauthors demonstrated how protamine addition worsens platelet function.[22,25,26]
Cell salvage
Reinfusion of recovered, filtered, and heparin-washed blood plays a role in CPB-induced coagulation impairment. Cell salvage is often used to avoid blood transfusions, with a reduction in transfusion cost. In cardiac surgery, heparin plays a crucial role in prolonging the activated clotting time. Blood salvaged following CPB is often thought to contain residual heparin, leading to concern among surgeons about its use due to its increased risk of bleeding, especially within the microcirculation, when reinfusion exceeds 18.5% of the total blood volume.[27]
Many studies argue this assumption, claiming that recovered blood has minimal heparin activity, even in procedures requiring complete anticoagulation.[28,29]
Wang et al., in a meta-analysis, underline that cell salvage may be beneficial if used for residual and/or spilled blood or during the entire operative period. Conversely, cell salvage seems to have an irrelevant effect on blood conservation in cardiotomy-suctioned blood during extracorporeal circulation, rather than increasing plasma transfusion.[30]
Protamine alternatives: not only andexanet alfa?
Although protamine is approved as a reversal agent for heparin, a drug shortage coupled with potentially life-threatening hypersensitivity reactions (i.e., anaphylaxis, antibody (IgE) formation, catastrophic pulmonary vasoconstriction, and direct complement activation) following administration in patients at risk of reactions urged the scientific community to investigate possible alternatives.
Andexanet alfa, originally created as an antidote for rivaroxaban and apixaban, showed in vitro almost complete heparin reversal in a dose-dependent manner and regression of the heparin effect on activated partial thromboplastin time, thrombin time, and factor Xa activity. However, the use of andexanet to antagonize heparin or low molecular weight heparin (LMWH) has not been evaluated yet in in vivo settings and is not recommended. Therefore, andexanet before heparinization, for example, during surgery, should be avoided, as off-label use before surgery seems to induce refractoriness to heparin. Notably, this product is very expensive.[31]
Though not currently available for clinical use, other agents potentially suitable as alternatives to protamine for anticoagulation reversal include hexadimethrine, recombinant platelet factor 4 (PF4), heparinase, and universal heparin reversal agent (UHRA), a potent neutralizer of all types of heparin with no effect on clot morphology.
Furthermore, in recent years, a novel small molecule interacting non-covalently through charge–charge interactions with both UFH and LMWH (namely ciraparantag) has been developed. Preliminary studies conducted in animal models using different anticoagulants suggest that ciraparantag shows considerable promise in minimizing blood loss. As a result, its potential as a reversal agent for direct oral anticoagulants (DOACs) is currently under investigation. Whether administered intravenously before or after a bleeding injury, ciraparantag consistently displayed a noteworthy decrease in blood loss at peak concentrations of the anticoagulant. Its ease of administration and prolonged functional half-life position it as a promising choice for potential application in situations with a heightened risk of bleeding (e.g., cardiac surgery). However, it is undeniable that additional large-scale clinical trials are needed to further validate these initial findings and ultimately integrate them into routine clinical practice.[32]
Protamine during polypharmacy and drug incompatibility
Given the increasing prevalence of polypharmacy in both operating rooms and intensive care units (ICUs), it is essential to thoroughly assess the potential for drug incompatibility. Undesirable outcomes (i.e., drug precipitation at the administration port) can result in the formation of harmful compounds or inactive complexes, leading to adverse effects or a lack of therapeutic efficacy. Lamontagne et al.[33] documented a case in which large globules were observed after propofol and protamine were concurrently administered through the same infusion line, causing the separation of oil and aqueous phases. Several years later, Gupta et al.[34] reported a case of physical incompatibility between protamine and ceftriaxone sodium, an antibiotic used prophylactically in cardiac surgery after separation from CPB. This incompatibility resulted in precipitation, with the resulting mixture needing discharge. Further investigations are needed to ascertain whether such precipitates can form toxic complexes or compromise the effectiveness of protamine.
Remarkably, there are currently no further known or described instances of protamine engaging in additional harmful interactions with other medications.
Heparin
In 1918, Emmett Holt and William Howell accidentally discovered an anticoagulant called heparphosphatide at Johns Hopkins Hospital in Baltimore. The new water-soluble anticoagulant phosphatide was found in abundance in the canine liver tissue. The first intravenous heparin was produced in 1936 when the first human trials of heparin were conducted and Connaught’s heparin was confirmed to be a safe, easily available, and effective blood anticoagulant. Heparin performs anticoagulant functions only in the presence of a plasma component named “heparin cofactor.” The connection between heparin cofactor and antithrombin (AT) goes back to the 1950s, when it was pointed out that heparin catalyzes AT activity. Activated AT inhibits thrombin (factor IIa) and factor X. Four generations of heparin are currently available: UFH, derived from bovine lung or gut, or from porcine intestinal mucosa; LMWH, second-generation heparin derived from depolymerization of UFH; ultra (U) LMWH, third-generation heparin, which includes chemical products; and fourth-generation heparin, modified with bioengineering techniques. Nowadays, some of the first three heparin generations have been approved by the US Food and Drug Administration (FDA) and are available for clinical use: Among these are UFH prepared from porcine intestine, several LMWHs (derived from porcine UFH), and ULMWH Arixtra® (fondaparinux).
Generally, pharmaceutical processes can be split into five steps, but the heparin-specific production cycle is patent protected and not available.[35]
Heparin is used for many purposes, including cardiac and vascular procedures, thrombosis and thromboembolism prophylaxis and treatment, atrial fibrillation with embolization, treatment of acute and chronic consumptive coagulopathies (disseminated intravascular coagulation (DIC)), and dialysis procedures.
Heparin administration is commonly based on actual body weight, a reasonable option for achieving adequate anticoagulation, yet individual response to heparin is variable. After hundred years of heparin usage, its pharmacokinetic and pharmacodynamic properties remain incompletely understood. Regorda et al.[36] suggest a mathematical model combining pharmacokinetic and pharmacodynamic properties to predict activated clotting time (ACT) during CPB following heparin administration, aiming to optimize heparin dosage and ACT value. Despite the great variability and heterogeneity of heparin activity where an individualized approach seems reasonable, clinical studies to confirm its utility are needed.
Measuring AT III at every stage: A necessity or not
AT III is a serine protease inhibitor, known for its crucial role as an anticoagulant and anti-inflammatory agent. Heparin presence can enhance 1.000-fold the anticoagulant activity of AT III, while theoretically compromising its anti-inflammatory capacity. Heparin administration can potentially change the available quantity of AT III, as the thrombin—AT III reaction is equilateral.[37] In suspected heparin-resistant patients, the administration of increased doses of heparin is an option but could induce excessive consumption of AT III. One plausible strategy might be to determine the AT III level before and after every surgical intervention. The cost-effectiveness is open to debate as AT III dosing could be expensive. Some advantages of this strategy may be preventing large doses of unnecessary heparin and preserving anti-inflammatory AT III properties and early diagnosis of possible heparin resistance.[38]
Heparin-allergic and anaphylactoid reactions
The most common allergic reaction to heparin is a cell-mediated delayed type IV hypersensitivity reaction, clinically characterized by skin necrosis, including pruritic erythematous plaques or maculae. Immediate type I allergic reaction (IgE-mediated) is rare. The risk factors of LMWH-induced skin reactions (more frequently in females than in males) include a duration of therapy longer than 9 days and body mass index higher than 25. Due to its rarity, there are no standardized protocols to follow in cases of heparin allergy.[39] [Table 2]
Table 2.
Heparin-allergic and anaphylactoid reactions (most of them rare)[39]
| Clinical manifestations | Therapeutic options | |
|---|---|---|
| Heparin-induced anaphylactic and anaphylactoid reactions | ||
| Oversulfated chondroitin sulfate (OSCS) heparin-induced anaphylaxis (contact system activation with increase in vasoactive kinins or bradykinin) | Severe hypotension and laryngeal edema | Corticosteroids Epinephrine or norepinephrine |
| Heparin-induced anaphylactoid reaction as a consequence of heparin-induced thrombocytopenia (HIT), mediated by an immune reaction | Fever or chills Hypertension “pseudo-pulmonary embolism” | Stop heparin Continue with direct thrombin inhibitors if anticoagulation is required: argatroban, bivalirudin, danaparoid, or fondaparinux |
| Patients previously exposed to heparin can have circulating “HIT antibodies” defined as circulating antiplatelet factor 4 (PF4) antibodies, which can lead to platelet activation | Fever, acute respiratory distress, hypotension, thrombosis, and low platelet count (Interestingly, thrombocytopenia increases the risk of bleeding, not reducing the risk of thrombosis) | Stop heparin Continue with direct thrombin inhibitors if anticoagulation is required: argatroban, bivalirudin, danaparoid, or fondaparinux |
| Heparin-allergic reactions (Majority of patients are negative for an intradermal test and can undergo heparin administration) | ||
| Cell-mediated delayed type IV hypersensitivity reaction | Skin necrosis Pruritic erythematous plaques or maculae | Due to their rarity, no specific protocols are specified in the literature. Use standard algorithms |
| Immediate type I allergic reaction (IgE-mediated, rare) | Urticaria Angioedema Bronchospasm Severe anaphylactic shock | Due to their rarity, no specific protocols are specified in the literature. Use standard algorithms |
Size matters (LMWH and protamine)
Over the past years, LMWH progressively substituted UFH in clinical practice, but protamine has remained the same. Neutralization capacity varies according to certain factors: Some studies demonstrated reduced capacity caused by molecular weight and degree of sulfation, suggesting greater affinity of protamine for high molecular weight molecules. Shroeder et al.[40] investigated the molecular weight influence on LMWH neutralization by protamine [Table 3].
Table 3.
Protamine neutralization profile of unfractionated heparin (UFH) and various low molecular weight heparin (LMWH)
| Anti-IIa neutralization | Anti-Xa neutralization | |
|---|---|---|
| UFH | > 95% | 97% |
| Dalteparin | >93% | 59% |
| Tinzaparin | >96% | 81% |
| Enoxaparin | >87% | 46% |
| Fondaparinux | 5% |
They concluded that sulfation does not have the same importance as molecular weight; however, marked variation in protamine neutralization capacity cannot be attributed to one single factor. In this study, using the traditional 1:1 heparin-to-protamine dose, only anti-IIa activity resulted in inhibition contrary to anti-Xa activity. LMWH, a peptide fragment derived from protamine enzymatic digestion, could be a promising solution.[41] Many papers have been published since its initial discovery in 1999: The results showed that low molecular weight protamine could neutralize the anticoagulant properties of heparin and LMWH. Besides its effect as heparin or LMWH antagonist, low molecular weight protamine has capacity to delay insulin absorption, forming insoluble complexes, a less toxic long-lasting insulin product than conventional neutral protamine Hagedorn (NPH) insulin for diabetic control.
Of note, 1 mg of protamine sulfate will neutralize approximately 100 anti-Xa units of an LMWH (i.e. 60 mg of protamine to neutralize 6000 IU of enoxaparin). This dose will depend on the timing of LMWH administration, considering the specific half-life of the culprit molecule. For instance, if 1 mg of enoxaparin was administered, the protamine dose needed to revert it would be 1 mg or 0.5 mg if the former was administered earlier or later than 8 hours, respectively. Protamine reversal may not be required if enoxaparin was administered >12 hours before. Furthermore, as the protamine half-life is 7 minutes and the LMWH half-life is in the range of 4–7 hours, a second, delayed dose of protamine might be administered to achieve better reversal.
Target ACT
In 2018, the Society of Thoracic Surgeons (STS), the Society of Cardiovascular Anesthesiologists (SCA), and the American Society of ExtraCorporeal Technology (AmSECT) published clinical practice guidelines for anticoagulation during CPB. The seventeen suggestions have evidence B or C, and therefore, we are still using the target ACT of 400–480 seconds without the level of evidence “A.” ACT has several limitations resulting in low heparin specificity: Platelet low count and dysfunction, coagulation deficiency (including coagulation factor deficiency), hypothermia, surgery effect, ongoing therapies, and hemodilution may influence the ACT result, simulating adequate heparinization and predisposing to adverse events.[42]
Miles et al.[43] published results from the first Global Cardiopulmonary Bypass Survey. These data represent practice in Europe, North America, Australia or New Zealand, and South America. The ACT considered safe to start CPB in the different regions was generally between 400 and 500 seconds. A small percentage of respondents prefer an ACT above or below that value.
These results evidence some differences in anticoagulation procedures between different regions, and the reasons are unclear.
ACT assessment: arterial or venous blood sampling
Variability has been reported during the ACT measurement. Various studies hypothesize different ACT values resulting from arterial or venous samples.[44,45,46] Differences have been attributed to the heparin presence in arterial line flushing solution, to sampling blood from heparin-coated catheters, to viscosity, or to oxygen tension in arterial blood. Whatever the cause, there is variability in ACT measurement after heparinization and further studies are needed.[47]
Timing and modalities of heparin administration before CPB
Nowadays, CPB is performed approximately 1 million times per year (in Europe and the USA combined) and relies on modulation of the coagulation system through heparin. To allow the patient’s blood to flow into the CPB circuit, an anticoagulant must be administered.
Administering heparin before CPB and reversing it with protamine at the end of CPB are key moments in the operating room: Coordination among anesthesiologists, surgeons, perfusionists, and nurses is mandatory, and speaking out loud and clear is common so that everyone is aware of what is happening. Heparin is usually administered through the central venous line, followed by proper flushing.
A single bolus of heparin (low cost, quick onset, and easy reversal), at a standard dose of 300 IU/Kg of body weight (equal to 3 mg per kg), is administered to achieve an ACT greater than 480 sec. The starting dose is 300 units per kg and is calculated based on either lean or actual body weight. Shlensky et al.[48] found no differences in bleeding among three different groups of patients (nonobese, obese, and morbidly obese) and concluded that heparin dose based on actual body weight is safe and effective. Additionally, the CPB circuit is usually primed with additional heparin as per the center routine.
When discontinuing extracorporeal circulation, it is necessary to antagonize the effects of heparin.
Heparin antagonization
A protamine dose is administered in a 1:1 ratio to the administered heparin. In this way, the given amount of protamine is always more than necessary. Some physicians may even consider a total administered dose of heparin rather than an initial bolus dose. This is even more serious. The goal is to return to the basal ACT, not to the normal ACT. The normal ACT range is 70–120 sec, while the therapeutic range for anticoagulation is 150–600 sec. (however, ranges vary according to test device and therapy choice). ACT higher than the baseline value does not mean there is still circulating heparin, as much as lower ACT does not mean a total absence of heparin. Considering that the ACT test is influenced by multiple variables, such as temperature, coagulation factor deficiency, hemodilution, and ongoing therapies, as shown by Despotis et al.,[49] it correlates poorly with the heparin level in cardiac surgery [Table 4].
Table 4.
Heparin-suggested dose and activated clotting time (ACT) target in several cardiac and cardiovascular interventions
| Setting | Dose | ACT target |
|---|---|---|
| Cardiac surgery | 300 U/Kg bolus | ACT target >480 sec. |
| Cardiac surgery: off-pump coronary artery bypass graft | 150 U/Kg bolus | ACT target >320 sec. |
| Vascular procedures | 100 U/Kg bolus + adjustments | ACT target >250 sec. |
| Percutaneous interventions | 100 U/Kg bolus + adjustments | ACT target >250 sec. |
| -Transcatheter aortic valve replacement (TAVR) | ACT target 250–300 sec. | |
| - Elective coronary procedures | ||
| - Ventricular tachycardia ablation | ||
| Percutaneous interventions involving the left atrium (e.g., atrial fibrillation ablation, Mitraclip®, and left atrial appendage closure) and tricuspid percutaneous repair (e.g., Triclip®) | 100 U/Kg bolus+adjustments | ACT target>300 sec. |
| Extracorporeal membrane oxygenation (ECMO): wide variability among centers and different ECMO configurations and flows | 7.5–20.0 U/kg/h | ACT 180–200 sec. aPTT 40–60 sec. aPTT 60–80 sec. ACT + POC test |
| Impella® | ACT 160–180 sec. | |
| Intra-aortic balloon pump (IABP) | Manufacturers do not consider anticoagulation mandatory, especially if 1:1 assistance Reasonable to start iv heparin if care >24h or a ratio <1:1 is expected | aPTT ratio target >2 |
Heparin for mechanical assist devices, the controversy continues
A safe anticoagulant strategy during the use of mechanical assist devices is paramount, as more and more MCS is being used every day around the world. Fisser C. et al.[50] reported >50% incidence of cannula-related venous thrombosis after removal of veno-venous extracorporeal membrane oxygenation (VV-ECMO), due to reduced systemic anticoagulation; on the contrary, excessive anticoagulation may lead to bleeding with devastating consequences.
To monitor patients during mechanical support, depending on the center, there are preferences and habits in monitoring coagulation. Traditional coagulation tests are used: PT, activated partial thromboplaastin clotting time (aPTT), and anti-factor Xa levels. POC tests (i.e., thromboelastometry and thromboelastography) and platelet aggregometry are whole-blood coagulation tests, which should guarantee the therapeutic range of antithrombotic medications, recognize patients at risk of thrombotic or hemorrhagic complications, and help in the control of bleeding complications.[51] However, aPTT is not reliable due to a high degree of variability from one laboratory to another, from one reagent to another, and even from intrinsic factors, such as inflammation, low fibrinogen, and vWF, which may cause inaccurate results. The anti-Xa chromogenic assay is not available everywhere and is not routinely used to measure heparin activity, as it is indicated only in specific clinical situations and must be carefully interpreted.
ECMO in and outside the ICU
There is no consensus on the dose of anticoagulation and subsequent monitoring during ECMO. Extracorporeal Life Support Organization (ELSO) guidelines for anticoagulation during ECMO consider a wide range for initial heparin infusion (7.5–20.0 units/kg/h),[52] despite not much indication for monitoring. The ACT range suggested in ECMO is 180–200 sec, but this value has shown a poor correlation with the heparin level.[53,54]
Because of these concerns, many centers decided to develop their own heparin protocol for ECMO, commonly targeted to aPTT range between 40–60 and 60–80 sec, respectively, in patients with high and low bleeding risk. Ranucci et al. suggested a diagnostic–therapeutic algorithm, combining ACT and viscoelastic tests.[55,56]
Impella and Intra-Aortic Balloon Pump (IABP)
According to the manufacturer, the ACT target is 160–180 sec and no recommendation is available for using aPTT,[57] although many centers utilize aPTT with no significant differences from ACT.[58] The purge solution may help to find the “sweet spot” for anticoagulation and might even be sufficient; the recommendation is to adjust the dextrose concentration in the purge solution.
Nowadays, systemic anticoagulation is typically used, aiming for a target aPTT ratio of 2; great attention is needed with IABP at 1:3 mode.[59]
EVIDENCE GAPS AND FUTURE PERSPECTIVES
While we have a clear understanding of the biological and biochemical interactions between heparin and protamine, there are still numerous unanswered questions regarding their practical implications. One such question pertains to the management of patients with spontaneously high basal ACT values, such as those exceeding 220 seconds. It remains uncertain whether the goal should be to reach the target ACT or to focus on the difference between the normal values and the target ACT. To monitor anticoagulation produced by heparin when basal aPTT is prolonged (i.e., low factor VIII), another method should be used. Plasma anti-Xa assay, for example, is a functional test used to monitor patients treated with UFH, LMWH, and DOAC for anti-Xa activity.
Further questions remain open in the management of patients requiring periprocedural anticoagulation. In patients who are on dual antiplatelet therapy, the target periprocedural ACT levels are a matter of debate.[60]
Also, the management of patients requiring extracorporeal cardiopulmonary resuscitation is uncertain due to the common unbalance between the coagulation cascade and fibrinolytic system during cardiac arrest and cardiopulmonary resuscitation.
Patients with coagulation disorders who undergo surgery requiring anticoagulation have a high risk of bleeding complications and represent a challenge for perioperative physicians. Preexisting coagulopathies include heparin-induced thrombocytopenia, factor XII deficiency, AT III deficiency, idiopathic thrombocytopenic purpura, hemophilia, cancer, protein S deficiency, and drug-induced platelet inhibition.[61]
In this context, the integration of pharmacogenomic insights into clinical decision-making empowers healthcare providers to customize anticoagulation therapy for individual patients within the wider realm of personalized medicine.[62] Such a tailored approach ultimately optimizes dosing regimens, mitigates the risk of adverse events, and enhances treatment outcomes.
Comprehensive screening is essential before procedures requiring anticoagulation, mainly to rule out any disease potentially leading to serious complications. A review of the patient’s medical history and coagulation profile is of paramount importance.
CONCLUSIONS
Although protamine and heparin have long been indispensable in medical procedures, particularly in cardiac anesthesia, it is clear that our comprehension of these drugs remains far from exhaustive.
Protamine cannot in fact be defined as a procoagulant, as it is an antidote that might itself act as an anticoagulant if administered to a patient not previously exposed to heparin or if the dosage is too high with respect to the heparin dose. The 1:1 protamine-to-heparin ratio administration to reverse the heparin effects in cardiac surgery is probably an obsolete practice, and studies are required to better address this issue. To avoid the vicious circle of “more protamine, more bleeding,” one option is to use the “HMS,” which results in a decreased and tailored protamine dose, while an alternative is to administer two-thirds of the standard calculated dose of protamine. Protamine has frequent systemic side effects, which can be mitigated by a very slow administration. Notably, protamine also partially reverts the anticoagulant effect of LMWHs. At the moment, there is no pharmacological alternative to protamine as andexanet alfa is extremely expensive and never used in clinical practice and other molecules being developed are confined to use in animal models so far. Conducting more in-depth investigations into their molecular processes, latent roles, and individual variances holds the potential to transform our approach to surgeries, the management of anticoagulation in artificial cardiac assist devices, anticoagulation therapies across diverse clinical scenarios, and treatments for various diseases. Recognizing the existing knowledge gaps and fostering research driven by curiosity will undoubtedly open doors to intriguing breakthroughs in the realm of anticoagulation therapies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Balhorn R. The protamine family of sperm nuclear proteins. Genome Biol. 2007;8:227. doi: 10.1186/gb-2007-8-9-227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Waldschmidt-Leitz E, Stadler P, Steigerwaldt F. Über blutgerinnung, hemmung und beschleunigung. Z Physik Chem. 1929;183:39. [Google Scholar]
- 3.Levy JH, Faraj BA, Zaidan JR, Camp VM. Effects of protamine on histamine release from human lung. Agents Actions. 1989;28:70–2. doi: 10.1007/BF02022982. [DOI] [PubMed] [Google Scholar]
- 4.Hsu K, Wang D, Shen CY, Chiang CH. Protamine-induced acute lung injury and the protective effect of agents that increase cAMP. Proc Natl Sci Counc Repub China B. 1993;17:57–61. [PubMed] [Google Scholar]
- 5.Nybo M, Madsen JS. Serious anaphylactic reactions due to protamine sulfate: A systematic literature review. Basic Clin Pharmacol Toxicol. 2008;103:192–6. doi: 10.1111/j.1742-7843.2008.00274.x. [DOI] [PubMed] [Google Scholar]
- 6.Boer C, Meesters MI, Veerhoek D, Vonk ABA. Anticoagulant and side-effects of protamine in cardiac surgery: A narrative review. Br J Anaesth. 2018;120:914–27. doi: 10.1016/j.bja.2018.01.023. [DOI] [PubMed] [Google Scholar]
- 7.Tacquard C, Iba T, Levy JH. Perioperative anaphylaxis. Anesthesiology. 2023;138:100–10. doi: 10.1097/ALN.0000000000004419. [DOI] [PubMed] [Google Scholar]
- 8.Levy JH, Adkinson NF., Jr Anaphylaxis during cardiac surgery: Implications for clinicians. Anesth Analg. 2008;106:392–403. doi: 10.1213/ane.0b013e3181602e0d. [DOI] [PubMed] [Google Scholar]
- 9.De Simone F, Nardelli P, Licheri M, Frau G, Redaelli MB, Monaco F, et al. Less is more: We are administering too much protamine in cardiac surgery. Ann Card Anaesth. 2021;24:178–82. doi: 10.4103/aca.ACA_26_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Taneja R, Szoke DJ, Hynes Z, Jones PM. Minimum protamine dose required to neutralize heparin in cardiac surgery: A single-centre, prospective, observational cohort study. Can J Anaesth. 2023;70:219227. doi: 10.1007/s12630-022-02364-4. [DOI] [PubMed] [Google Scholar]
- 11.Miles LF, Burt C, Arrowsmith J, McKie MA, Villar SS, Govender P, et al. Optimal protamine dosing after cardiopulmonary bypass: The PRODOSE adaptive randomised controlled trial. PLoS Med. 2021;18:e1003658. doi: 10.1371/journal.pmed.1003658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Miles LF, Marchiori P, Falter F. Pilot validation of an individualised pharmacokinetic algorithm for protamine dosing after systemic heparinisation for cardiopulmonary bypass. Perfusion. 2017;32:481–8. doi: 10.1177/0267659117695881. [DOI] [PubMed] [Google Scholar]
- 13.Meesters MI, Veerhoek D, de Jong JR, Boer C. A Pharmacokinetic model for protamine dosing after cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 2016;30:1190–5. doi: 10.1053/j.jvca.2016.04.021. [DOI] [PubMed] [Google Scholar]
- 14.Jacques LB. A study of the toxicity of the protamine, salmine. Br J Pharmacol Chemother. 1949;4:135–44. doi: 10.1111/j.1476-5381.1949.tb00526.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barstad RM, Stephens RW, Hamers MJ, Sakariassen KS. Protamine sulphate inhibits platelet membrane glycoprotein Ib-von Willebrand factor activity. Thromb Haemost. 2000;83:334–7. [PubMed] [Google Scholar]
- 16.Ammar T, Fisher CF. The effects of heparinase 1 and protamine on platelet reactivity. Anesthesiology. 1997;86:1382–6. doi: 10.1097/00000542-199706000-00021. [DOI] [PubMed] [Google Scholar]
- 17.Matsuo T, Shanberge JN, Matsuo O. Effect of protamine sulfate on antithrombin III activity. Clin Chim Acta. 1983;131:233–8. doi: 10.1016/0009-8981(83)90092-x. [DOI] [PubMed] [Google Scholar]
- 18.Cobel-Geard RJ, Hassouna HI. Interaction of protamine sulfate with thrombin. Am J Hematol. 1983;14:227–33. doi: 10.1002/ajh.2830140304. [DOI] [PubMed] [Google Scholar]
- 19.Ni Ainle F, Preston RJ, Jenkins PV, Nel HJ, Johnson JA, Smith OP, White B, Fallon PG, O’Donnell JS. Protamine sulfate down-regulates thrombin generation by inhibiting factor V activation. Blood. 2009;114:1658–65. doi: 10.1182/blood-2009-05-222109. [DOI] [PubMed] [Google Scholar]
- 20.Chu AJ, Wang ZG, Raicu M, Beydoun S, Ramos N. Protamine inhibits tissue factor-initiated extrinsic coagulation. Br J Haematol. 2001;115:392–9. doi: 10.1046/j.1365-2141.2001.03100.x. [DOI] [PubMed] [Google Scholar]
- 21.Meesters MI, Veerhoek D, de Lange F, de Vries JW, de Jong JR, Romijn JW, et al. Effect of high or low protamine dosing on postoperative bleeding following heparin anticoagulation in cardiac surgery. A randomised clinical trial. Thromb Haemost. 2016;116:251–61. doi: 10.1160/TH16-02-0117. [DOI] [PubMed] [Google Scholar]
- 22.Suelzu S, Cossu A, Pala G, Portoghese M, Columbanu V, Sales G, et al. Impact of different dosage of protamine on heparin reversal during off-pump coronary artery bypass: A clinical study. Heart Lung Vessel. 2015;7:238–45. [PMC free article] [PubMed] [Google Scholar]
- 23.Griffin MJ, Rinder HM, Smith BR, Tracey JB, Kriz NS, Li CK, et al. The effects of heparin, protamine, and heparin/protamine reversal on platelet function under conditions of arterial shear stress. Anesth Analg. 2001;93:20–7. doi: 10.1097/00000539-200107000-00005. [DOI] [PubMed] [Google Scholar]
- 24.Despotis GJ, Joist JH, Hogue CW, Jr, Alsoufiev A, Kater K, Goodnough LT, et al. The impact of heparin concentration and activated clotting time monitoring on blood conservation. A prospective, randomized evaluation in patients undergoing cardiac operation. J Thorac Cardiovasc Surg. 1995;110:46–54. doi: 10.1016/S0022-5223(05)80008-X. [DOI] [PubMed] [Google Scholar]
- 25.Gertler R, Wiesner G, Tassani-Prell P, Braun SL, Martin K. Are the point-of-care diagnostics MULTIPLATE and ROTEM valid in the setting of high concentrations of heparin and its reversal with protamine? J Cardiothorac Vasc Anesth. 2011;25:981–6. doi: 10.1053/j.jvca.2010.11.020. [DOI] [PubMed] [Google Scholar]
- 26.Carr ME, Carr SL. At high heparin concentrations, protamine concentrations which reverse heparin anticoagulant effects are insufficient to reverse anti-platelet effects. Thrombosis Res. 1994;75:617–30. doi: 10.1016/0049-3848(94)90174-0. [DOI] [PubMed] [Google Scholar]
- 27.Son K, Yamada T, Tarao K, Kitamura Y, Okazaki J, Sato Y, et al. Effects of cardiac surgery and salvaged blood transfusion on coagulation function assessed by thromboelastometry. J Cardiothorac Vasc Anesth. 2020;34:2375–82. doi: 10.1053/j.jvca.2020.02.009. [DOI] [PubMed] [Google Scholar]
- 28.Tamura T, Waters JH, Nishiwaki K. Heparin concentration in cell salvage during heparinization: A pilot study. Nagoya J Med Sci. 2020;82:449–55. doi: 10.18999/nagjms.82.3.449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.DeAndrade D, Waters JH, Triulzi DJ, Alarcon L, Wisniewski MK, Dyga R, et al. Very low rate of patient-related adverse events associated with the use of intraoperative cell salvage. Transfusion. 2016;56:2768–72. doi: 10.1111/trf.13791. [DOI] [PubMed] [Google Scholar]
- 30.Wang G, Bainbridge D, Martin J, Cheng D. The efficacy of an intraoperative cell saver during cardiac surgery: A meta-analysis of randomized trials. Anesth Analg. 2009;109:320–30. doi: 10.1213/ane.0b013e3181aa084c. [DOI] [PubMed] [Google Scholar]
- 31.Maneno JN, Ness GL. Andexanet Alfa, the possible alternative to protamine for reversal of unfractionated heparin. Ann Parmacother. 2021;55:261–4. doi: 10.1177/1060028020943160. [DOI] [PubMed] [Google Scholar]
- 32.Ansell J, Laulicht BE, Bakhru SH, Burnett A, Jiang X, Chen L, et al. Ciraparantag, an anticoagulant reversal drug: Mechanism of action, pharmacokinetics, and reversal of anticoagulants. Blood. 2021;137:115–25. doi: 10.1182/blood.2020007116. [DOI] [PubMed] [Google Scholar]
- 33.Lamontagne C, Brouillette D, Hardy JF. Incompatibility of propofol emulsion with anesthetic drugs. Anesthesiology. 1998;89:1609. doi: 10.1097/00000542-199812000-00066. [DOI] [PubMed] [Google Scholar]
- 34.Gupta D, Soori R. Physical incompatibility between protamine sulfate and ceftriaxone sodium. J Cardiothorac Vasc Anesth. 2017;31:e50–1. doi: 10.1053/j.jvca.2017.01.001. [DOI] [PubMed] [Google Scholar]
- 35.Baytas SN, Linhardt RJ. Advances in the preparation and synthesis of heparin and related products. Drug Discov Today. 2020;25:2095–109. doi: 10.1016/j.drudis.2020.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Regorda F, Vigoni E, Pesenti G, Pieri M, Belletti A, Manca D, et al. Physiologically-based pharmacokinetic and pharmacodynamic modeling of unfractionated heparin to predict activated clotting time. Comput Aided Chem Eng. 2020;48:703–8. [Google Scholar]
- 37.Ranucci M. Antithrombin III Key factor in extracorporeal circulation. Minerva Anestesiol. 2002;68:454–7. [PubMed] [Google Scholar]
- 38.Ranucci M, Isgrò G, Cazzaniga A, Ditta A, Boncilli A, Cotza M, et al. Different patterns of eparine resistance: Therapeutic implications. Perfusion. 2002;17:199–204. doi: 10.1191/0267659102pf562oa. [DOI] [PubMed] [Google Scholar]
- 39.Warkentin TE, Greinacher A. Heparin-induced anaphylactic and anaphylactoid reactions: Two distinct but overlapping syndromes. Expert Opin Drug Saf. 2009;8:129–44. doi: 10.1517/14740330902778180. [DOI] [PubMed] [Google Scholar]
- 40.Schroeder M, Hogwood J, Gray E, Mulloy B, Hackett AM, Johansen KB. Protamine neutralisation of low molecular weight heparins and their oligosaccharide components. Anal Bioanal Chem. 2011;399:763–71. doi: 10.1007/s00216-010-4220-8. [DOI] [PubMed] [Google Scholar]
- 41.Chang LC, Lee HF, Yang Z, Yang VC. Low molecular weight protamine (LMWP) as nontoxic heparin/low molecular weight heparin antidote (I): Preparation and characterization. AAPS PharmSci. 2001;3:E17. doi: 10.1208/ps030317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Shore-Lesserson L, Baker RA, Ferraris VA, Greilich PE, Fitzgerald D, Roman P, et al. The society of thoracic surgeons, the society of cardiovascular anesthesiologists, and the American Society of ExtraCorporeal Technology: Clinical practice guidelines-anticoagulation during cardiopulmonary bypass. Ann Thorac Surg. 2018;105:650–62. doi: 10.1016/j.athoracsur.2017.09.061. [DOI] [PubMed] [Google Scholar]
- 43.Miles LF, Coulson TG, Galhardo C, Falter F. Pump priming practices and anticoagulation in cardiac surgery: Results from the global cardiopulmonary bypass survey. Anesth Analg. 2017;125:1871–7. doi: 10.1213/ANE.0000000000002052. [DOI] [PubMed] [Google Scholar]
- 44.Pesola GR, Johnson A, Pesola DA. Percutaneous transluminal coronary angioplasty: Comparison of arterial vs. venous activated clotting time. Cathet Cardiovasc Diagn. 1996;37:140–4. doi: 10.1002/(SICI)1097-0304(199602)37:2<140::AID-CCD7>3.0.CO;2-D. [DOI] [PubMed] [Google Scholar]
- 45.Rath B, Bennett DH. Monitoring the effect of heparin by measurement of activated clotting time during and after percutaneous transluminal coronary angioplasty. Br Heart J. 1990;63:18–21. doi: 10.1136/hrt.63.1.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Zisman E, Rosenberg B, Katz Y, Ziser K. A comparison between arterial and venous-sampled activated clotting time measurements. Isr J Med Sci. 1997;33:786–8. [PubMed] [Google Scholar]
- 47.Leyvi G, Zhuravlev I, Inyang A, Ziser A. Arterial versus venous sampling for activated coagulation time measurements during cardiac surgery: A comparative study. J Cardiothorac Vasc Anesth. 2004;18:573–80. doi: 10.1053/j.jvca.2004.07.006. [DOI] [PubMed] [Google Scholar]
- 48.Shlensky JA, Thurber KM, O’xMeara JG. Unfractionated heparin infusion for treatment of venous thromboembolism based on actual body weight without dose capping. Vasc Med. 2020;25:47–54. doi: 10.1177/1358863X19875813. [DOI] [PubMed] [Google Scholar]
- 49.Despotis GJ, Summerfield AL, Joist JH, Goodnough LT, Santoro SA, Spitznagel E, et al. Comparison of activated coagulation time and whole blood heparin measurements with laboratory plasma anti-Xa heparin concentration in patients having cardiac operations. J Thorac Cardiovasc Surg. 1994;108:1076–82. [PubMed] [Google Scholar]
- 50.Fisser C, Reichenbächer C, Müller T. Incidence and risk factors for cannula-related venous thrombosis after venovenous extracorporeal membrane oxygenation in adult patients with acute respiratory failure. Crit Care Med. 2019;47:e332–9. doi: 10.1097/CCM.0000000000003650. [DOI] [PubMed] [Google Scholar]
- 51.Bercovitz RS. An introduction to point-of-care testing in extracorporeal circulation and LVADs. Hematology Am Soc Hematol Educ Program. 2018;2018:516–21. doi: 10.1182/asheducation-2018.1.516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Organization ECLS. ELSO anticoagulation Guideline. The Extracorporeal Life Support Organization (ELSO) Ann Arbor: Organization ECLS. 2014:2–17. [Google Scholar]
- 53.Lawson DS, Walczak R, Lawson AF, Shearer IR, Ing R, Schulman S, et al. North American neonatal extracorporeal membrane oxygenation (ECMO) devices: 2002 survey results. J Extra Corpor Technol. 2004;36:16–21. [PubMed] [Google Scholar]
- 54.Atallah S, Liebl M, Fitousis K, Bostan F, Masud F. Evaluation of the activated clotting time and activated partial thromboplastin time for the monitoring of heparin in adult extracorporeal membrane oxygenation patients. Perfusion. 2014;29:456–61. doi: 10.1177/0267659114524264. [DOI] [PubMed] [Google Scholar]
- 55.Ranucci M, Baryshnikova E, Cotza M, Carboni G, Isgrò G, Carlucci C, et al. Group for the Surgical and Clinical Outcome Research (SCORE). Coagulation monitoring in postcardiotomy ECMO: Conventional tests, point-of-care, or both? Minerva Anestesiol. 2016;82:858–66. [PubMed] [Google Scholar]
- 56.Sklar MC, Sy E, Lequier L, Fan E, Fan E, Kanji HD. Anticoagulation practices during venovenous extracorporeal membrane oxygenation for respiratory failure. A systematic review. Ann Am Thorac Soc. 2016;13:2242–50. doi: 10.1513/AnnalsATS.201605-364SR. [DOI] [PubMed] [Google Scholar]
- 57.Succar L, Sulaica EM, Donahue KR, Wanat MA. Management of anticoagulation with Impella®percutaneous ventricular assist devices and review of new literature. J Thromb Thrombolysis. 2019;48:284–91. doi: 10.1007/s11239-019-01837-6. [DOI] [PubMed] [Google Scholar]
- 58.Fitousis K, Klasek R, Mason PE, Masud F. Evaluation of a pharmacy managed heparin protocol for extracorporeal membrane oxygenation patients. Perfusion. 2017;32:238–44. doi: 10.1177/0267659116678057. [DOI] [PubMed] [Google Scholar]
- 59.Ferguson JJ, 3rd, Cohen M, Freedman RJ, Jr, Stone GW, Miller MF, Joseph DL, et al. The current practice of intra-aortic balloon counterpulsation: Results from the Benchmark Registry. J Am Coll Cardiol. 2001;38:1456–62. doi: 10.1016/s0735-1097(01)01553-4. [DOI] [PubMed] [Google Scholar]
- 60.Karlsson M, Hannuksela M, Appelblad M, Hällgren O, Johagen D, Wahba A, et al. Cardiopulmonary bypass and dual antiplatelet therapy: A strategy to minimise transfusions and blood loss. Perfusion. 2020;35:236–45. doi: 10.1177/0267659119867005. [DOI] [PubMed] [Google Scholar]
- 61.De Bois W, Liu J, Lee L, Girardi L, Ko W, Tortolani A, et al. Cardiopulmonary bypass in patients with pre-existing coagulopathy. J Extra Corpor Technol. 2005;37:15–22. [PMC free article] [PubMed] [Google Scholar]
- 62.Relling MV, Evans WE. Pharmacogenomics in the clinic. Nature. 2015;526:343–50. doi: 10.1038/nature15817. [DOI] [PMC free article] [PubMed] [Google Scholar]