

Abstract
Aim
The aim of this current case series is to propose various design modifications of the conventional distal shoe space maintainers in relation to complex clinical scenarios.
Background
Primary dentition plays a significant role in preserving space for underlying unerupted permanent teeth; early childhood caries (ECC) is a serious public health problem in both developing and developed countries, and it is often left untreated. Its consequences can have an immediate and long-term impact on the child's quality of life and overall health. Premature loss of primary dentition can result in loss of arch length, thereby hampering the eruption of the succeedaneous tooth, which can further lead to malalignment, crowding, rotation, and impaction of the permanent teeth. Space maintainers are advocated in cases where extraction of primary molars is inevitable. In the early loss of the second primary molar, a distal-shoe space maintainer is advocated to guide the eruption, as well as prevent mesial migration of the first permanent molar (FPM) during the eruption. In clinical scenarios where multiple losses of deciduous molars occur bilaterally, obtaining adequate anchorage is questionable and futile. The following clinical modifications, however, are useful in overcoming the problems related to the same. The following case series intends to project various modifications of distal shoes in complex scenarios.
Case description
Various modifications of the distal shoe have been proposed in our current case series. The appliances were adjusted individually on a case-to-case basis depending on the clinical scenario. A 1-year clinical follow-up was carried out on all the patients.
Conclusion
All the clinical modifications were successful in guiding the eruption of a FPM; there were no complications during any follow-up visit.
Clinical significance
In cases where the traditional design is not indicated, certain modifications in distal shoes by adding new components to the appliance will allow the appliance to be placed and the space to be maintained effectively. Along with this, reinforcement of parents and the child for oral hygiene maintenance will maintain the remaining healthy tooth structure and increase the success of treatment.
How to cite this article
Gunjal PY, Chauhan RS, Tirupathi S, et al. Guidance of Erupting First Permanent Molar in Complex Clinical Scenarios: A Case Series. Int J Clin Pediatr Dent 2024;17(3):362–367.
Keywords: Children, Guidance for eruption, Modified distal shoe, Space maintenance
Background
Primary dentition is extremely crucial; not only does it influence a child's growth and development in terms of speech, chewing, appearance, and the prevention of bad habits, but it also influences the eruption of permanent teeth.1 Early childhood caries (ECC) is one of the most common causes of primary tooth loss.2 Premature loss of the second deciduous molar prior to the eruption of the first permanent molar (FPM) presents a complex challenge for the pediatric dentist.3 It is extremely beneficial to hold space to allow teeth to erupt and prevent space loss. FPM active eruption begins at 4.5 years of age and continues until they reach full occlusal contact, which occurs at 6.5–7 years of age. The earlier the tooth loss, the more difficult the space management problem. Due to the eruption path of the maxillary arch, there is no need for a distal shoe appliance. The distal surface of the deciduous molar provides guidance for the eruption of the FPM in the mandibular arch; its premature loss results in severe space loss and tipped position as a result of the permanent molar's mesial eruption pathway.4 Davenport described that, due to the early loss of primary second molars, there is a loss of space. Premature loss of deciduous second molars accounts for approximately 70% of space loss and misalignment of permanent teeth.5 Premature loss of the deciduous second molar can result in space loss and mesial tipping of the FPM; hence, it concluded that it had a greater impact on the sagittal molar relationship.6
In this situation, the distal shoe is the space maintainer of choice to prevent space loss. Willett introduced the first distal shoe space maintainer with distal extension in 1929, covering both the first and the second primary molar and the canine teeth together in a casting; it was a unilateral, rigid, nonfunctional appliance having L-shaped intraalveolar extension. However, there were certain shortcomings that led to further modifications in the appliance as the design can be used in unilateral loss of the second deciduous molar, and due to narrow contact of the intraalveolar extension to erupt the permanent molar, the FPM is rotated Roche replaced the distal extension accompanied by a V-shaped intraalveolar extension in 1942. The V shape's larger surface area aided in preventing rotation.
The aim of the current case series is to describe various modifications of distal shoes in complex clinical scenarios.
Case Description
Bilateral Loss of Second Deciduous Molar
Independent Distal Shoe-bilateral
Case 1: A 5-year-old boy was referred to the Department of Pedodontics and Preventive Dentistry, Dr D Y Patil Dental College & Hospital, Dr D Y Patil Vidyapeeth (Deemed to be University), Pune, Maharashtra, India, with pain and recurrent abscess formation in both sides second deciduous lower molars as the chief complaints. Second molars had to be extracted, according to clinical and radiographic examinations. First, primary molars were treated with pulpectomy followed by a stainless steel crown. Banding was done on both crowns, followed by impression taking; the band was transferred on the impression, and casts were obtained. Measurement for the horizontal arm and the intraalveolar extension was calculated with the help of radiovisography (RVG). A 19-gauge stainless steel wire was used to fabricate the appliance. Two separate units of the modified distal shoe with U loops on buccal and lingual arms and V-shaped intraalveolar extension with solder flowed in between as intraalveolar projection were fabricated and soldered to the band. The process of flowing the solder was done after soldering the wire component to the band or the crown. The “V” shaped extension was placed over a plaster block so that the solder material would be held in between the “V.” Cementation of one appliance was done, and after a gap of 6 days, extraction on the other side was performed, and the appliance was cemented. A gap was given in order to avoid bilateral nerve block and also allow healing on one side. The patient was followed up for 12 months, and the FPM was seen to be erupting without rotation or tipping. Further, after the eruption of both the permanent molars, the band and loop, followed by the lingual arch, will be placed after the eruption of the permanent lower anterior (Figs 123).
Fig. 1:

Bilateral decayed primary molars preoperative
Fig. 2:

Bilateral independent crown and loop (1-month visit)
Fig. 3:

Bilateral independent crown and loop (10-month visit)
Bilateral Distal Shoe Appliance
Case 2: A 5-year-old boy came with the chief complaints of food lodgement in the lower left and right side. Clinical and radiographic examinations revealed that the first and second molars on the left side and the first molar on the right side needed to be extracted. After extraction of the first and second molar on the left side, there was not enough anchorage that could be obtained from the canine because of insufficient abutments caused by multiple deciduous molar loss on the lower left side, a modification of the distal shoe appliance was advocated. A distal shoe with a bilateral design was planned. Banding was performed on the canine and first primary molar; an impression was taken, and the cast was poured. The modified distal shoe was fabricated with 19-gauge wire and connected with an anteriorly placed lingual wire component, which was placed 1 mm ahead of the deciduous anterior so as to prevent hindrance in the eruption of permanent anterior teeth. Also, a supporting wire connection, lingual and buccal wire, was placed on the left side of the appliance to support the long arms. Also, two “U” loops at the horizontal arm and one broad “V” with solder flowed in between as intraalveolar projection that provided ease to adjust the appliance during cementation, providing great fusibility to adjust a bilateral single unit appliance. All the components were soldered, and a single unit bilateral distal shoe was fabricated and cemented; the patient was followed up for 9 months (Figs 4567).
Fig. 4:

Bilateral decayed primary molars preoperative
Fig. 5:
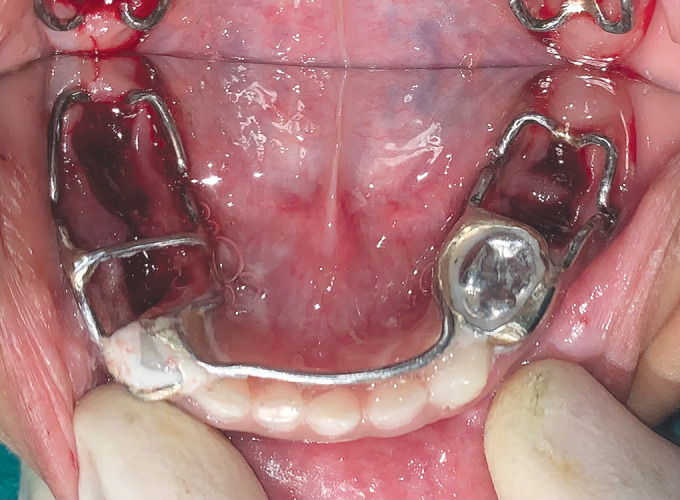
Bilateral fused distal shoe appliance immediate postextraction
Fig. 6:
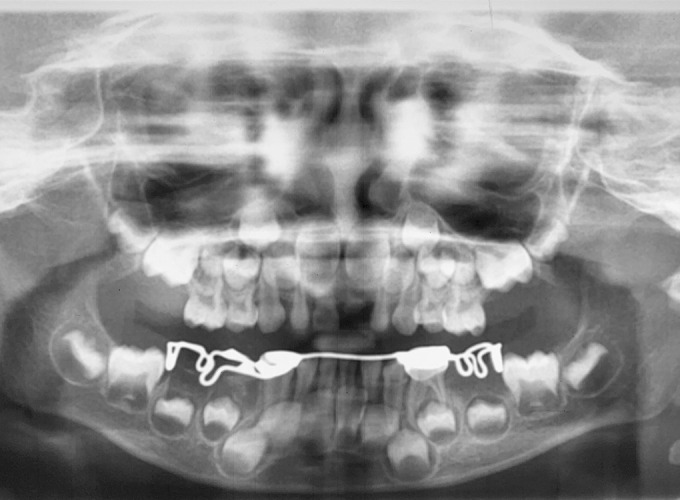
Orthopantomogram showing bilateral fused distal shoe appliance
Fig. 7:

Bilateral fused distal shoe appliance (1-year visit)
Premature Loss of Second Deciduous Molar Unilaterally
Case 3: A 5-year-old girl came with the chief complaint of food lodgement on the lower right side of the jaw. On clinical and radiographic examination, the tooth was planned for pulpectomy. Access opening and biomechanical preparation were done, and intracanal medicament was given. Further, the patient did not continue the treatment. After 3 months, the patient again reported to the department with a complaint of pain; on radiographic examination, resorption was noted, and there was a bone loss in the furcal region. Thus, extraction with a second deciduous molar followed by placement of a modified distal shoe was planned. The first primary molar was restored with type 9 glass ionomer cement (GIC). As the first primary molar needed to be restored with a crown, the crown selection was made, the alginate impression was taken, and the crown was transferred onto the immersion. The distal shoe was soldered to the crown. The patient was followed up for 6 months, and during the follow-up period, it was observed that the FPM was erupting upright (Figs 8910).
Fig. 8:

Unilateral crown and distal shoe immediate delivery
Fig. 9:
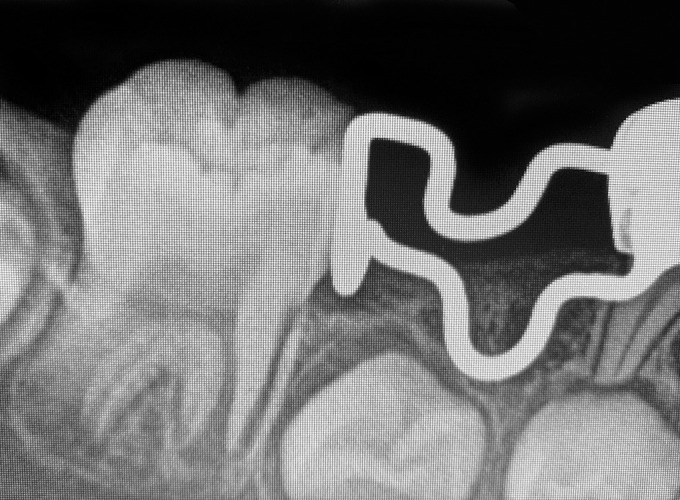
Intraoral periapical radiograph of the unilateral crown and distal shoe
Fig. 10:
Unilateral crown and distal shoe (1-year visit)
Case 4: A 5-year-old girl came with the chief complaints of pain in the deciduous right mandibular second molar. The patient's medical history was nonspecific. Clinical and radiographic examinations revealed that the mandibular second primary molars were bound to fail any other treatment and had to be extracted. The first molar had smooth surface caries and needed to be restored with restorative material and a stainless steel crown, so a distal shoe with the crown was planned. Alginate impressions were made, and the cast was poured; space was made for the intraalveolar extension by scraping the area on the cast. Measurements for intraalveolar extension were done with the help of a digital X-ray, extending up to the mesial surface of the first permanent molar and 1 mm below the mesial marginal ridge. Appliance fabrication was done with 19-gauge wire, and the design was modified with a broad contact area with a broad “V” with solder flowed in between as intraalveolar projection and “U” loop buccally and lingually were fabricated, which will make appliance adjustment possible. The appliance was cemented with type 1 luting GIC. The patient is followed up for 9 months, and after the eruption of FPM, a reverse band and loop were placed (Figs 11121314).
Fig. 11:

Unilateral crown and distal shoe immediate delivery
Fig. 12:

Intraoral periapical radiograph of the unilateral crown and distal shoe
Fig. 13:

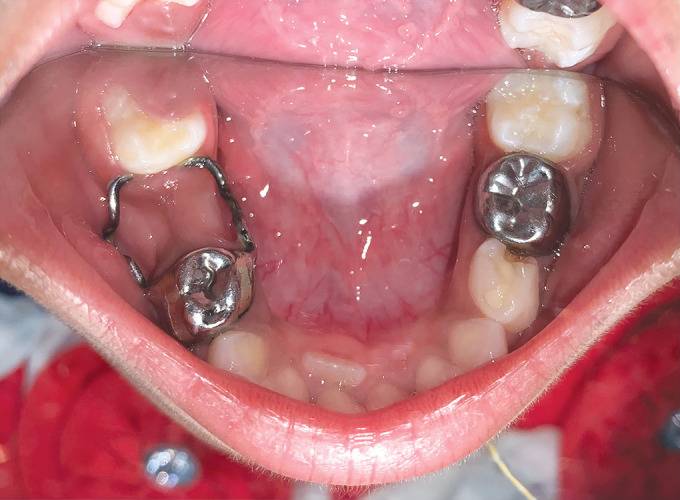
Unilateral crown and distal shoe (10-month visit)
Fig. 14:

Unilateral crown and distal shoe (16-month visit)
Discussion
The deciduous second molar guides the eruption of the permanent first molar. Pediatric dentists have always found it difficult to prevent space loss due to the premature loss of primary second molars. Many designs of guiding appliances are proposed, the most common being the Willet's appliance. Croll, in 1980, developed an appliance with a crown and a half-loop buccally for clinical situations where the FPM partially erupted. Carrol and Jones 1982 designed acrylic pressure ridge extraalveolar acrylic pressure appliance. Garcia-Godoy, in 1983, modified the conventional appliance by making U loops on the buccal and lingual arms of the distal shoe, which made the appliance semi-adjustable. Brill, in 2002, developed a chairside fabricated and adjustable distal shoe.7 Willet's appliance is unable to provide broad contacts and cannot be used in premature loss of multiple deciduous molars. Thus, where there is bilateral loss of mandibular second primary molars, modification is necessary. Dhindsa and Pandit modified the appliance design with a lingual holding arch to support the distal shoe of the bilateral designee and maintain the integrity of the lower dental arch in the event of insufficient abutments.8 Gujjar et al., on the contrary, placed the lingual component far lingually to avoid impeding the eruption of permanent mandibular incisors.9 As Willet's design is often unable to provide broad contact, strength and stability, the modified design was planned to increase flexibility and broaden the contact area by “V” shaped intraalveolar extension with solder flowed in between as intraalveolar projection and prevent dislodgement. Contrary to the conventional design, in the present design, the extended length of intraalveolar extension prevented the slipping during eruption. “U” loops distributed the stresses from the permanent first molar during an active eruption at the buccal and lingual arms of the horizontal component. In some clinical situations, conventional designs cannot be used and must be modified to meet the needs of the patient.
In our case, instead of a prefabricated distal shoe, we have incorporated “U” loops on the horizontal arm on the lingual and buccal arm of the appliance to facilitate adjustment during placement. For the second case, the conventional design of the distal shoe was not advocated as a result of multiple lower primary molar losses. If we had given distal shoes by banding the canine alone unilaterally, the appliance's stability would have been a major issue. Thus, the modified design was planned. The canine was banded with band material; it was experienced that the banding of the canine causes discomfort to the gingiva as the band needs to be custom-made and consumes more time. The modified design was able to maintain the mesiodistal dimension of the space without any compromise to the stability or cooperation of the patient. Bilateral appliances may obstruct the eruption of permanent mandibular incisors during their eruption. The lingual arch was kept as lingual as possible without interfering with the positioning of the tongue, and a close watch was performed on the eruption of permanent mandibular incisors both radiographically and clinically. During the follow-up period, it was observed that the child had difficulty eating food and maintaining oral hygiene. The supporting wire, which was soldered on the left side to support the long arms, was dislodged, though the appliance further showed to be stable and have enough strength.
Various modifications have been made to adapt according to clinical situations. In our case 4, a unilateral distal show along with crown was fabricated with two “U” loops at the horizontal arm that provided ease to adjust the appliance during cementation and one broad “V” with solder flowed in between as intraalveolar projection to provide a border contact that can prevent rotation of the FPM. Crown was given as the first primary molar had smooth surface caries, and only the band would not provide sufficient strength. On the day of cementation, the second primary molar was extracted, and the appliance was cemented with type 1 luting GIC. The position of the distal intraalveolar arm was conformed to radiographically. The intraalveolar extension was placed 1 mm below the mesial marginal ridge of the FPM. The patient was followed up until the eruption of FPM; the appliance was successfully maintained until the period of removal when the molar was visible intraorally; the distal shoe was removed and replaced with the reverse band and loop appliance. During the follow-up period, the patient was informed about the importance of oral hygiene maintenance. Oral prophylaxis was done on follow-up visits. The patient initially complained of discomfort due to appliance and difficulty in chewing food. Further, on regular follow-up, the patient reported less discomfort. On examination, the molars seem to be erupting in an upright position, indicating the success of the appliance. When planning for such a complex type of appliance, follow-up with the patient is very important to evaluate the eruption of FPM and the tooth bud of permanent premolar to prevent hindrance to the tooth bud. Also, the maintenance of oral hygiene is very important to prevent infection or gingivitis that can be caused by the banding of teeth and intraalveolar extension. The function of mastication cannot be restored when this type of appliance is used, but space is successfully maintained, and the FPM molars are guided for eruption in the position without deviation.
Clinical Significance
In cases where the traditional design is not indicated, certain modifications in distal shoes by adding new components to the appliance will allow the appliance to be placed and the space to be maintained effectively. Along with this, reinforcement of parents and the child for oral hygiene maintenance will maintain the remaining healthy tooth structure and increase the success of treatment. The modified distal shoe appliances are more stable and stronger, are well tolerated by the child, and meet all of the criteria for a proper space maintainer. It is a valuable tool for pediatric dentists who must decide whether to extract a primary first and second molar prior to the eruption of the FPM. Regular patient follow-ups, on the contrary, are critical for the success of this type of complex appliance.
Orcid
Pranjali Y Gunjal https://orcid.org/0000-0002-9431-5841
Sunnypriyatham Tirupathi https://orcid.org/0000-0002-2593-0090
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Paglia L. Does breastfeeding increase risk of early childhood caries? Eur J Paediatr Dent. 2015;16(3):173. [PubMed] [Google Scholar]
- 2.Dye BA, Hsu KL, Afful J. Prevalence and measurement of dental caries in young children. Pediatr Dent. 2015;37(3):200–216. [PubMed] [Google Scholar]
- 3.Gandhi JM, Gurunathan D. Short- and long-term dental arch spatial changes following premature loss of primary molars: a systematic review. J Indian Soc Pedod Prev Dent. 2022;40(3):239–245. doi: 10.4103/jisppd.jisppd_230_22. [DOI] [PubMed] [Google Scholar]
- 4.Aldowsari MK, Alsaidan M, Alaqil M, et al. Ectopic eruption of first permanent molars for pediatric patients attended King Saud University, Riyadh, Saudi Arabia: a radiographic study. Clin Cosmet Investig Dent. 2021;13:325–333. doi: 10.2147/CCIDE.S320441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bindayel NA. Clinical evaluation of short term space variation following premature loss of primary second molar, at early permanent dentition stage. Saudi Dent J. 2019;31(3):311–315. doi: 10.1016/j.sdentj.2019.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barbería E, Lucavechi T, Cárdenas D, et al. Free-end space maintainers: design, utilization and advantages. J Clin Pediatr Dent. 2006;31(1):5–8. doi: 10.17796/jcpd.31.1.p87112173240x80m. [DOI] [PubMed] [Google Scholar]
- 7.Brill WA. The distal shoe space maintainer chairside fabrication and clinical performance. Pediatr Dent. 2002;24(6):561–565. [PubMed] [Google Scholar]
- 8.Dhindsa A, Pandit IK. Modified Willet's appliance for bilateral loss of multiple deciduous molars: a case report. J Indian Soc Pedod Prev Dent. 2008;26(3):132–135. doi: 10.4103/0970-4388.43196. [DOI] [PubMed] [Google Scholar]
- 9.Gujjar KR, Indushekar KR, Amith HV, et al. Modified distal shoe appliance–fabrication and clinical performance. J Dent Child (Chic) 2012;79(3):185–188. [PubMed] [Google Scholar]