

Abstract
Childhood adversity can have detrimental impacts on life course mental and physical health. Timing, nature, severity, and chronicity of adversity are thought to explain much of the variability in health and developmental outcomes among exposed individuals. The current study seeks to characterize heterogeneity in adverse experiences over time at the individual, family, and neighborhood domains in a cohort of predominantly Black children (85% Black and 15% white, 46.2% girls, 67.2% free/reduced lunch in 1st grade), and to examine associations with mental health from 6th grade to age 26. Participants were part of a randomized universal preventive interventions trial in 1st grade with prospective follow-up through early adulthood. Separate models characterized heterogeneity in adversity in elementary, middle, and high schools. Changes in adversity over time and relationships with mental health (anxiety, depression, suicidal behaviors) were investigated using a random-intercept latent transition analysis (RI-LTA). We identified 3-class solutions in early childhood, middle school, and high school. Generally, both a higher and a lower poly-adversity class were observed at each time point, with varying nature of adversity characterized by the third class. RI-LTA indicated prevalent within-individual changes in adverse exposure over time and differential associations with mental health and suicidal behaviors. Results suggest that treating adverse exposures as a static construct may limit the ability to characterize salient variation over time. Identifying complexity in adverse experiences and their relation to health and well-being is key for developing and implementing effective prevention and early intervention efforts to mitigate negative effects through the life course.
Keywords: adversity, suicidal behaviors, mental health, latent variable analysis, longitudinal
INTRODUCTION
Childhood adversity has demonstrated impacts on mental, behavioral, and physical health outcomes (Merrick et al., 2017); however, current literature has not fully elucidated how heterogeneity in adverse exposure over time relate to long-term outcomes. The current study considers a life course framework to assess developmental trajectories of adverse exposure and examine associations between trajectory membership and mental health outcomes through emerging adulthood. Further, the current study relies on a sample of primarily Black children and as such aims to include the experiences of minoritized youth to extend the definition of adverse exposures across key developmental periods.
Childhood adversity encompasses a range of potentially traumatic events, occurring up to the age of 18, including but not limited to physical, sexual, or verbal abuse, witnessing violence, having a parent with a mental illness or substance use disorder, or experiencing neighborhood violence. Childhood adversity is often captured via a count of exposures, which weighs all exposures equally. The most common measure of adverse childhood experiences (ACEs), popularized by Felitti et al (1998), captures ten events across three domains: abuse, neglect, and household function (Felitti et al., 1998). More recently, the conceptualization of adverse exposures has expanded to include bullying, neighborhood safety, foster care, and racism (Cronholm et al., 2015) to better capture negative experiences along multiple socioecological domains. A broader conceptualization of ACEs allows for a more comprehensive framework of exposure to adversity in individual, family, and neighborhood domains.
Data from the nationally representative 2016 National Survey of Children’s Health found that 45% of US children ages 0-17 had at least one ACE, most commonly economic hardship, or parental divorce (Sacks & Murphey, 2018). Other research estimates suggest that by middle childhood, most children are exposed to at least two adversities (O'Connor et al., 2020). Patterns of adversity vary, however, by child race and ethnicity due, in part, to differential exposure to racialized experiences. Black and Hispanic/Latinx youth are more likely to report parental incarceration and living with an adult with a substance use problem (Sacks & Murphey, 2018). Black, non-Hispanic/Latinx youth are more likely to experience the death of a parent or caregiver and are more likely to witness or experience violence in their neighborhood compared to white youth (Sacks & Murphey, 2018; Umberson et al., 2017). Broadly, prior research suggests that Black and economically disadvantaged children are more likely to experience adverse events compared to white or economically advantaged children. Along with understanding how groups of individuals experience childhood adversity, there is a substantial body of research focused on understanding the impact of adverse exposure across development.
Adverse Exposures Across Development
Consistent with a life course framework, there are at least three potential mechanisms by which early experience and exposures influence later health (Dunn et al., 2018). The first proposed mechanism focuses on accumulation of risk, suggesting that exposure to adversity accumulates across the life course, and more exposure to adversity is associated with more negative outcomes regardless of the timing of exposure. The next proposed mechanism suggests the presence of sensitive periods of adverse exposure, which assumes that the timing of exposure across the life course matters more than the cumulative exposure. Finally, the recency mechanism suggests that the impact of adverse exposure is time-limited and that exposure proximal to the outcome of interest has the biggest impact.
Research directly testing proposed mechanisms linking early adversity to later outcomes is limited and somewhat mixed in terms of support for primacy of one mechanism over the other. Dunn and colleagues (2018) found that the best fitting model depended not only on the exposure in question but also on the outcome of interest. These findings also suggested that the recency and accumulation models better fit the data than the sensitive period models, but the developmental window explored was limited, focusing on birth to age eight. In another study, Dunn and colleagues (2019) found that exposures early in childhood (before three years old) lead to the most significant biological changes (Dunn et al., 2019), whereas Andersen and colleagues (2021) suggest that both early childhood and adolescence serve as sensitive periods for the negative impacts of adversity (Andersen et al., 2021). Regardless of specific life course model, much of the research suggests that the type of adversity, the accumulation of burden from adversity, and the timing of adversity are independent factors of consideration and must be explored in future research (Nelson et al., 2020).
Linking Adverse Exposures to Mental Health Outcomes
Exposure to adversity in childhood is associated with increased risk for negative mental health through the life course, specifically depression and anxiety diagnoses and suicide ideation and attempt. A study conducted by Poole and colleagues (2017) found that a count of ACEs significantly predicted depressive symptoms (Poole et al., 2017). Kelifa and colleagues (2020) and Hendrick and colleagues (2021) found similar relationships between number of ACEs and depressive symptoms, suggesting that a greater number of ACES is associated with worse outcomes (Hedrick et al., 2021; Kelifa et al., 2020). Other studies have examined thresholds of adversity. For example, Elmore and Crouch (2020) found an increased risk of anxiety and depression among individuals exposed to four or more ACEs compared to those exposed to fewer than four (Elmore & Crouch, 2020). Thompson and colleagues (2019) examined the longitudinal relationship between exposure to ACEs beginning in 7th grade and suicide ideation and attempt in adulthood. Those with three or more ACEs (of eight ACEs examined) were more than three times more likely to consider suicide or attempt suicide in adulthood compared to those with no ACEs (Thompson et al., 2019).
Most existing studies rely on retrospective reporting of childhood adversity measures collected concurrently with mental health outcomes in adulthood. Retrospective reporting of ACEs, however, introduces recall bias. A smaller number of studies have relied on prospective reports of ACEs. Overall, evidence suggests that there is only a low to moderate correlation between prospective and retrospective reports; retrospective reports, in general, tend to underestimate ACE exposure (Naicker et al., 2021). Moreover, retrospective and prospective reports of ACEs may be differentially related to outcomes. For example, Naicker and colleagues (2021) examined ACEs measured prospectively from ages 5 to 18 and retrospectively at age 22-23. While they found evidence that both prospective and retrospective reporting of four or more ACEs related to poorer mental health, there was a decrease in prevalence of retrospectively reported ACEs compared to those reported prospectively over time in this cohort. Further, female youth were more likely to report fewer retrospective exposure to ACEs than male youth but were similar in their number of ACEs reported prospectively. (Naicker et al., 2021). While there is rigorous and consistent research that suggests exposure to ACES (defined in several different ways) increases risk for negative mental health outcomes (Smith & Pollak, 2021), much remains unknown regarding the timing and variation of adverse exposures in this population and how differential exposure relates to mental health.
Measurement and Methodological Gaps
The original conceptualization of ACEs was proposed by Felitti et al. in their landmark 1998 study (Felitti et al., 1998). This study assessed psychological, physical and sexual abuse, and household dysfunction (e.g., substance abuse, mental illness, mother treated violently, and criminal behavior) using 18 items. Much adversity measurement to date includes dimensions of abuse, household dysfunction and neglect, typically in the form of single binary endorsement variables (Steptoe et al., 2019). While the field has moved to consider a wider range of ACEs (e.g., discrimination, community violence) measurement and assessment tools still largely focus on Felitti’s original dimensions of adversity, which may miss key variation in adverse exposures occurring across socioecological levels (Bethell et al., 2017). Further, despite the burgeoning emphasis on examining how variation in type, timing, and duration of adverse exposures in childhood relate to health outcomes, challenges remain in characterizing the complexity of adversity during and across various developmental stages. This is primarily due to the lack of appropriate measures collected over time in a large enough sample to capture the potential heterogeneity in adverse exposures; such data are rare.
In addition, most existing work has operationalized adverse exposures as a cumulative risk score, without examining how particular types of adversities cluster together (Bethell et al., 2017) or change in nature over time. Recent, albeit fewer, studies have examined how adverse exposures group together and/or have focused on revealing distinct subgroups of adverse exposure patterns (Hajat et al., 2020). Finally, much of the literature on adversity focuses on retrospective reports of childhood experiences (Bethell et al., 2017; Merrick et al., 2018). As a result, there has been less focus on understanding how adversities are distributed over the life course and what the construct of adversity looks like in specific developmental time periods (e.g., are adverse exposures in early childhood similar to adverse exposures in adolescence?).
Current Study
The current study explores links between changes in subjective reports of multi-domain adverse exposures (individual, family, and neighborhood) from childhood to adolescence and their differential association with mental health outcomes. We leverage longitudinal data spanning 20 years in a sample exposed to substantial adversity. Adverse experiences in childhood can have detrimental impacts on life course health; as discussed, variation in the timing, nature, severity, and chronicity of adversity is thought to explain the variability in health and developmental outcomes among those exposed (Nelson et al., 2020). However, few studies have empirically examined this level of complexity, in particular the way adverse exposures change over time and implications for measurement.
To address existing gaps, the current study aims to 1) characterize multi-domain (individual, family, neighborhood) patterns of adverse exposures from childhood to adolescence, leveraging parent report in early childhood and youth self-report in adolescence; 2) examine longitudinal changes in adverse exposures over development across early childhood, middle school, and high school ages to understand stability and/or change in exposures over time; and 3) investigate within-individual pathways by which differing and changing adverse experiences through childhood and adolescence relate to mental health through emerging adulthood (ages 19-26).
We examine the aforementioned gaps using prospective measures of adverse exposures from parents in early childhood and subsequently repeated measures of youth self-report in middle and high school periods. This is important as most of the literature surrounding the impact of ACEs on mental health has focused on retrospective reporting of ACEs (i.e., adults reporting on past childhood exposures) and mental health outcomes also measured concurrently in adulthood (Naicker et al., 2021; Reuben et al., 2016). We also expand on existing methodological frameworks used to examine adverse exposures by leveraging a random-intercept latent transition analysis (RI-LTA) to highlight within-individual changes in exposures over time. RI-LTA models the variation between individuals through random intercepts, akin to the use of random intercepts in other multilevel modeling methods (Muthén & Asparouhov, 2022). By including a random intercept, the between-individual variation is removed from the latent class indicators and resulting transition probabilities from the RI-LTA model represent within-individual change in adverse exposures over time; this provides a clearer picture of how adversity changes and correlates with individuals’ mental health and suicidal behaviors. There are several advantages to using an RI-LTA model over traditional LTA methods. First, a regular LTA model estimates transition probabilities that confound between- and within-individual influences leading to biased transition probability estimates (Muthén & Asparouhov, 2022). Further, the probability of an individual staying in the same class over time is often overestimated in regular LTA models; for a review of the advantages of RI-LTA over a regular LTA model for assessing within-individual changes, see (Muthén & Asparouhov, 2022). While we are interested in how adversity changes over time, and therefore expect the construct of adversity to be non-invariant over time by design, using an RI-LTA model could address some concerns about measurement non-invariance by accounting for between-individual variation in response probabilities for a given latent class indicator. Further, recent work has indicated that longitudinal measurement invariance is not required for LTA models unless the assumption (or imposition) is that latent classes will be similar over time (Nylund-Gibson et al., 2023).
Based on the breadth of literature examining adversity and mental health (e.g., (Gondek et al., 2021; Juwariah et al., 2022), we hypothesize that individuals will have differing patterns of adverse exposures (e.g., heterogeneity in adverse exposures) and that these patterns of adverse exposures will be different in early childhood, middle school and high school ages. Next, we hypothesize that there will be a subset of individuals exposed to chronic and severe adversity across all three developmental periods. Further, we hypothesize that the subset of individuals exposed to chronic and severe adversity will have the greatest risk for negative mental health outcomes (Johnson et al., 2013; Shonkoff et al., 2012). While researchers and practitioners generally acknowledge that adverse exposures are heterogeneous in nature and dynamic through the life course, limited empirical work has incorporated the confluence of type, timing, and duration of adverse exposures in the examination of mental health outcomes. Leveraging existing developmental frameworks (Dunn et al., 2018; Nelson et al., 2020) and empirical work that has examined either type, timing or duration of adversity as it relates to later mental health (Berman et al., 2022; Schroeder et al., 2020) we hypothesize that level of adverse exposures will be stable over time even if the type of exposures change (e.g., those with high levels of adverse exposures early on will also experience high levels of adversity over the course of development, suggesting chronicity) (Dunn et al., 2018).
METHODS
Participants and Procedures
Participants in this study were part of the second-generation Johns Hopkins University Prevention Intervention Research Center’s randomized controlled trial (RCT), which involved a prospective cohort (n=678) of children from nine Baltimore City Public Schools who started first grade in 1993. A randomized block design was employed with three first-grade classrooms in each school randomly assigned to a control of standard setting condition or one of two universal preventive intervention conditions. Both teachers and students were randomly assigned to classrooms. The trial assessed the impact of two universal prevention interventions (as compared to control classrooms), focused on either supporting teacher instructional capacity and classroom behavior management (classroom) or parent-teacher relationships and providing tools to parents for child behavior management and support for child academic achievement (family) (Ialongo et al., 1999). The interventions were provided during the first-grade year only. Both intervention arms aimed to improve achievement and to reduce early aggressive/disruptive behavior in children. Follow-up data collection was conducted annually from grades 1-3 and 6-12, and at ages 19-26 years. The current study includes 580 of the 678 children (85% Black and 15% white, 46.2% girls, 67.2% receiving free/reduced lunch in 1st grade) who had parent-reported adverse exposure in the fall of 1993 (first grade). Children were distributed equally (~33%) into the control and two intervention groups. About 84% of participants had mental health data from 6th grade through age 26.
This research was approved by the Johns Hopkins University Institutional Review Board. Parental consent and youth assent were obtained for youth under the age of 18; written consent was obtained from participants once they reached 18 years of age or older.
Measures
Adverse Exposures.
Adverse exposures (individual, family, neighborhood domains) were collected using parent report of their child’s lifetime adversity in first grade (ages 6-7) and subsequently youth self-report of adverse life events in the past year and neighborhood perceptions in grades 6 to 12. Exposure items were selected based on exploratory and confirmatory factor analyses over grades. These items were then binned into first grade, middle school (grades 6-8) and high school (grades 9-12) to capture heterogeneity in adverse exposures within and across developmental periods.
Elementary School (Parent Report). Adversity and negative life events in 1st grade were assessed through parent reports using items adapted from the life change events indices from the Health and Daily Living Form (Moos et al., 1984). Parent-reported adversity was measured with seven items including parental death, parental divorce or separation, marriage difficulties, financial difficulties, serious mental and physical health problems, and parent substance use, scored from 0 (not at all) to 3 (a lot). Item responses were dichotomized as yes (1-3) vs. no (0).
Grades 6-12 (Youth Self-Report). Youth reported their past year adverse exposures using a modified version of The Life Events Questionnaire Adolescent Version (adapted from (Coddington, 1972)) that included a broader range of adolescent and family-related stressors from: 1) Adolescent Perceived Events Scale (Compas et al., 1985); 2) Adolescent Family Inventory of Life Events and Changes (McCubbin et al., 1985); and 3) Children’s Report of Violence Exposure (Cooley-Quille et al., 1995). Adverse exposures assessed through self-report included whether participants had little contact with parents, got in trouble with the law, had a parent who died, witnessed and/or experienced violence (shot, stabbed, killed) scored as 1=You, 2=Family member or 3=No. Responses were dichotomized as yes (response option “You”) (1) vs. No (0) (response option “No”) to assess youths’ own exposures. Youth also reported on their perceptions of their neighborhood and neighborhood-level adverse exposures (e.g., see kids beat up in the neighborhood, people steal/damage property) using the Neighborhood Environment Scale (Elliott et al., 1985) scored from 1 (not at all true) to 4 (very true). Due to low prevalence estimates in some categories, item responses were collapsed into binary neighborhood variables as yes (2-4) vs. no (1).
Mental Health and Suicidal Behaviors.
Participant mental health and suicidal behavior were assessed by self-report from grade 6 to age 26. Prior available data (e.g., 6-12th grade) on mental health and suicidal behaviors were included to account for diagnoses and/or suicidal behaviors that onset before adulthood.
Anxiety/Depression. Participants reported on any past year diagnosis of anxiety and/or depressive disorder from 6th grade to age 26. A composite anxiety/depression variable was generated with Yes (if ever diagnosed with either anxiety or depressive disorder between grade 6 and age 26) vs. No (never diagnosed with either), based on meeting diagnostic criteria on an adult adaptation of the Computerized Diagnostic Interview Schedule for Children IV (C DISC-IV) (Shaffer et al., 2000) in adolescence and its adult adaptation in young adulthood; the C DISC-IV and its adult adaptation are fully structured interviews that ascertain the presence or absence of major mental health diagnoses consistent with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994).
Suicidal Ideation. Suicidal ideation was captured by the following question in the C DISC-IV and its adult adaptation: “in the last year, did you think seriously about killing yourself”, which was collapsed into Yes (if ever had suicidal thoughts) vs. No (never had suicidal thoughts) between grade 6 and age 26.
Suicide Attempt(s). Participants were also asked on the C DISC-IV and its adult adaptation: “have you ever, in your whole life, tried to kill yourself, or made a suicide attempt”. Suicide attempts were recorded as Yes vs. No.
Covariates.
Covariates measured in the fall of first grade were receiving free/reduced-price school meals (yes/no), child race (Black vs. white), child gender (boy vs. girl), and indicator variables for intervention status (classroom vs. not, family vs. not), all of which were included in all adjusted models.
Overview of Analytic Approach
Descriptive and exploratory analyses (t-tests, χ2 analyses, and Pearson correlation coefficients) were used to summarize and examine adverse exposures over time, mental health correlates, and covariates. Latent mixture modeling, using a 3-step method, was employed to examine changes in adverse exposure from first grade through high school and to examine the influence of within-individual change in adverse exposures on mental health and suicidal behaviors. This approach involves several model runs: 1) unconditional (no covariates) latent class analysis (LCA) to select the appropriate number of latent classes to characterize heterogeneity of adverse exposures in first grade, middle school and high school separately; 2) unconditional latent transition analysis (LTA), which is fit by regressing each latent class variable on the latent variable from the prior time point (e.g., middle school latent class variable Cmiddle school ON first grade latent class variable Cfirst grade); and 3) leveraging posterior class probabilities and most likely latent class membership from the LTA model to fix parameters in subsequent LTA models with covariates and/or distal outcomes to account for measurement error and avoid class shifting when including covariates and/or distal outcomes. Details on each step of latent mixture modeling used are described below.
Missing data in latent mixture models were handled in Mplus using full information maximum likelihood (FIML) estimation (Enders & Bandalos, 2001; Graham, 2009). This approach includes all participants in the analyses (n = 580) regardless of whether they had missing data. For FIML to provide accurate and unbiased parameter estimates, potential causes of missingness should be included within the specified models. Therefore, key covariates (e.g., child gender) were considered. To examine the effect of attrition over time, we compared mental health correlates (e.g., anxiety/depression, suicidal behaviors) for those who were in the analytic sample of 580 compared to the original study sample of 678 who were not included over time; there were no significant differences in prevalence of anxiety/depression diagnoses (8.3% vs. 7.7%), suicide ideation (35.1% vs. 22.2%) or suicide attempt (21.6% vs. 16.7%) between the two samples. Latent mixture analyses were conducted in Mplus 8.4. All other analyses were conducted using Stata Version 16.1 (StataCorp, College Station, TX, USA).
LCA Class Enumeration.
First, separate latent class models (LCA) were used to characterize heterogeneity in adverse exposures in first grade, middle school, and high school. Class enumeration was done separately for each latent class model for first grade, middle school, and high school time points. Mixture models with 1-5 class solutions for first grade and 1-6 class solutions for middle and high school were fit and evaluated. Starting with a 1-class model, classes were added sequentially without covariates and were examined for fit (Nylund et al., 2007). Information criteria [Bayesian Information Criterion (BIC), sample-size adjusted BIC and Akaike Information Criterion (AIC)] were used to determine model fit during class enumeration, with lower values indicating better model fit. Lo–Mendell–Rubin test (LMR), bootstrap likelihood ratio test (BLRT), and associated p values, were examined to assess whether adding an additional class significantly improved the model fit. Final selection of LCA models was based on lowest BIC (or largest decrease in BIC), and significant LMR and BLRT parameters; class specification (entropy) and substantive interpretation of classes were also considered in the selection of the final models (Nylund et al., 2007).
Three-Step Method in Mplus for Latent Transition Models.
Once time-specific LCA models were determined based on the class enumeration process, three unconditional latent transition models (1. regular LTA, 2. RI-LTA with continuous random intercept and 3. RI-LTA with binary random intercept) were estimated and the best fitting model was selected. While the goal of the current study was to examine within-individual changes in adverse exposures over time, a regular LTA model was fit to assess if including a random intercept improved model fit and would be appropriate before moving further. Due to the non-nested nature of the fitted LTA models, the resulting log-likelihood and number of parameters were unable to be compared. Therefore, we relied on BIC, as suggested by Muthen & Asparouhov 2022, and prioritized model parsimony given the existing computational burden of the fitted models. For more detailed information and references to RI-LTA Mplus code, see Muthen & Asparouhov 2022.
From the best fitting LTA model, individuals were assigned to nominal latent classes using posterior class probabilities and most likely latent class membership (logits); logits were obtained from the selected LTA model fit in its entirety (e.g., including random intercepts). This process accounts for measurement error in parameter estimates and helps to avoid class shifting when including covariates and outcomes in subsequent models. For more detailed information on the 3-step method and LTA Mplus code, see Nylund-Gibson et al., 2014. Finally, using the nominal latent classes and logits to fix measurement parameter estimates, covariates (e.g., free/reduced lunch status) and distal outcomes (e.g., depression and/or anxiety diagnosis from 6th grade through emerging adulthood) were included to assess predictors of class membership and how changes in adverse exposures over time relate to mental health through emerging adulthood. Our goal was to test for differences in prevalence of mental health variables across latent classes in high school accounting for transitions in prior waves of data collection (e.g., middle school); therefore, we estimated class-specific prevalence for the mental health variables by regressing the outcome variables on the last latent class variable (high school) (Nylund-Gibson et al., 2019). This study and analysis were not pre-registered, and data are not publicly available. Study materials, data collection protocol, and peer-reviewed studies resulting from the data are available at: https://www.jhsph.edu/research/centers-and-institutes/johns-hopkins-center-for-prevention-and-early-intervention/.
RESULTS
In elementary school, the most prevalent adverse exposure reported was financial difficulties affecting family (56%), with about one-third of children experiencing divorce/separation of parents and 9.5% of children experiencing death of a parent up to age 6. In addition to family-domain adversity (e.g., parents struggled to get a job, little contact with parent) in middle school, 49.1% of youth reported witnessing violence (e.g., someone getting shot, stabbed, or beaten up) and 10.5% reported experiencing such violence themselves. In high school, 66.4% of youth reported witnessing violence and about 21% reported experiencing violence themselves, a notable increase from middle school. Nearly one-third of youth (31%) in high school reported that a close friend died during their high school years. About half of participants reported that kids in their neighborhood get beat up or mugged, that they often see drunk people on the streets and that people in their neighborhood damage or steal each other’s property in both the middle (range 41-47%) and high school years (range 50-53%). Prevalence of depression and/or anxiety diagnoses from 6th grade to emerging adulthood (ages 19-26) was 8.3% with 35.1% of participants reporting having had suicidal ideation and 21.6% reporting attempting suicide in this time period. Table 1 includes prevalence of adverse exposures in each developmental period, mental health and suicidal behaviors, and demographic characteristics.
Table 1.
Prevalence of Adverse Exposures, Mental Health and Suicidal Behaviors and Participant Sociodemographic Characteristics
| Variables | % Experienced |
|---|---|
| Elementary School Adversity (% Yes); n = 580 | |
| Child Experienced Death of a Parent | 9.53 |
| Child Experienced Divorce/Separation of Parents | 32.50 |
| Marriage Difficulties Affected Family | 27.12 |
| Financial Difficulties Affected Family | 56.03 |
| Serious (Physical) Illness Affected Family | 15.17 |
| Mental or Emotional Illness Affected Family | 7.60 |
| Substance Use (tobacco, alcohol and/or other drug problems) Affected Family | 4.84 |
| Middle School Adversity (% Yes); n = 491 | |
| Parent Died | 8.10 |
| Family Member Died (i.e., grandparent) | 26.55 |
| Close Friend Died | 17.76 |
| Parents Struggle to Get a Job or Lost Job | 57.76 |
| Family Evicted | 7.93 |
| Parents Divorced or Separated | 27.59 |
| Little Contact with One Parent | 49.14 |
| Family Member Got in Trouble with the Law | 40.34 |
| You Got in Trouble with the Law | 11.21 |
| Witnessed Violence (shot, stabbed, mugged/beaten up) | 49.14 |
| Experienced Violence (shot, stabbed, mugged/beaten up) | 10.52 |
| Every few weeks some kid in my neighborhood gets beat up or mugged | 42.07 |
| Every few weeks some adult in my neighborhood gets beat up or mugged | 29.14 |
| In the morning or later in the day, I often see drunk people on the street in my neighborhood | 47.59 |
| The people who live in my neighborhood often damage or steal each other’s property | 41.21 |
| High School Adversity; n = 524 | |
| Parent Died | 7.59 |
| Family Member Died (i.e., grandparent) | 29.48 |
| Close Friend Died | 31.03 |
| Parents Struggle to Get a Job or Lost Job | 47.24 |
| Family Evicted | 8.97 |
| Parents Divorced or Separated | 19.31 |
| Little Contact with One Parent | 52.07 |
| Family Member Got in Trouble with the Law | 48.28 |
| You Got in Trouble with the Law | 20.52 |
| Witnessed Violence (shot, stabbed, mugged/beaten up) | 66.38 |
| Experienced Violence (shot, stabbed, mugged/beaten up) | 21.03 |
| Every few weeks some kid in my neighborhood gets beat up or mugged | 50.69 |
| Every few weeks some adult in my neighborhood gets beat up or mugged | 42.24 |
| In the morning or later in the day, I often see drunk people on the street in my neighborhood | 53.97 |
| The people who live in my neighborhood often damage or steal each other’s property | 52.59 |
| Mental Health and Suicidal Behaviors from 6th grade thru age 26 (% Yes); n = 543 | |
| Anxiety/Depression Diagnosis | 8.28 |
| Suicidal Ideation | 35.10 |
| Suicide Attempt | 21.59 |
| Covariates (measured in first grade); n = 580 | |
| Child Race | |
| Black (%) | 85.00 |
| White (%) | 15.00 |
| Child Gender (% Girls) | 46.21 |
| Free/Reduced Lunch (%) | 67.24 |
| Classroom-centered Intervention (%) | 33.97 |
| Family-School Partnership Intervention (%) | 33.62 |
| Control Group (%) | 32.41 |
LCA Class Enumeration and Unconditional Latent Class Findings
Separate three-class models were selected to characterize the heterogeneity in adverse exposures separately in elementary school, middle school, and high school based on fit statistics (i.e., BIC, LMR p-value, BLRT p-value) and substantive interpretability of classes (Table 2). Details on analytic decisions surrounding class enumeration and resultant latent classes are explained below.
Table 2.
Latent Class Analysis (LCA) and Latent Transition Analysis (LTA) Fit Statistics
| Latent Class Enumeration | |||||||
|---|---|---|---|---|---|---|---|
| No. of Classes | Log Likelihood | BIC | SSA-BIC | LMR p -value |
BLRT p- value |
Entropy | Smallest class % (n) |
| First Grade Adverse Exposures | |||||||
| 1 | −2005.56 | 4055.66 | 4033.44 | -- | -- | -- | -- |
| 2 | −1904.68 | 3904.81 | 3857.19 | <.001 | <.001 | .566 | 39.8 (229) |
| 3 | −1890.01 | 3926.38 | 3853.36 | .003 | <.001 | .785 | 9.1 (53) |
| 4 | −1880.84 | 3958.94 | 3860.53 | .300 | .250 | .676 | 4.8 (28) |
| 5 | −1874.95 | 3998.05 | 3874.24 | .073 | 1.00 | .691 | 5.3 (31) |
| Middle School Adverse Exposures | |||||||
| 1 | −3879.89 | 7852.73 | 7805.12 | -- | -- | -- | -- |
| 2 | −3628.74 | 7449.57 | 7351.18 | <.001 | <.001 | .751 | 48.3 (237) |
| 3 | −3570.44 | 7432.11 | 7282.94 | .124 | <.001 | .721 | 22.0 (108) |
| 4 | −3530.00 | 7450.38 | 7250.42 | .034 | <.001 | .699 | 21.6 (106) |
| 5 | −3501.95 | 7493.42 | 7242.67 | .142 | <.001 | .716 | 11.2 (55) |
| 6 | −3479.09 | 7546.84 | 7245.31 | .345 | <.001 | .747 | 5.9 (29) |
| High School Adverse Exposures | |||||||
| 1 | −3893.37 | 7880.67 | 7833.06 | -- | -- | -- | -- |
| 2 | −3523.03 | 7240.17 | 7141.77 | <.001 | <.001 | .797 | 40.3 (211) |
| 3 | −3378.65 | 7051.59 | 6902.40 | <.001 | <.001 | .808 | 33.4 (175) |
| 4 | −3338.82 | 7072.12 | 6872.15 | .022 | <.001 | .753 | 17.5 (92) |
| 5 | −3303.90 | 7102.25 | 6851.48 | .368 | <.001 | .727 | 15.8 (83) |
| 6 | −3277.11 | 7149.05 | 6847.50 | .467 | .013 | .743 | 8.0 (42) |
| Latent Transition Model Fit | # Parameters | ||||||
| 1. Regular LTA | −8796.89 | 18389.14 | 17992.31 | -- | -- | -- | 125 |
| 2. RI-LTA, Binary Intercept | −8796.88 | 19101.80 | 18349.41 | -- | -- | -- | 237 |
| 3. RI-LTA, Continuous Intercept | −8610.71 | 18252.22 | 17737.94 | -- | -- | -- | 162 |
Note. First grade n = 580; Middle School n = 491; High School n = 524
Elementary School Adversity
Fit statistics for the LCA model in first grade indicated that a 3-class model was most appropriate to characterize children’s adverse exposures. Along with BIC values decreasing from the 2-class model to the 3-class model, the addition of the third class significantly improved the model fit as exhibited by significant LMR and BLRT p-values. The distribution of the total sample in each class and the classification probabilities also indicated that a 3-class model optimized class specification. Despite the smallest class comprising only 9.1 % of the sample, considering the fit statistics and substantive interpretations of each class, a 3-class model was ultimately selected. Elementary school adversity classes were as follows: Family Illness and Financial Difficulties (class 1, n = 54, 9.6%), Household Stressors (class 2, n = 132, 23.9%) and Low Adversity (class 3, n = 385, 66.4%) (Figure 1). The Family Illness and Financial Difficulties class was characterized by a high likelihood of parents reporting that their child was exposed to family members with serious physical and/or mental and emotional illnesses and moderate likelihood of exposure to substance use problems. The Household Stressors class was comprised of those who experienced the loss of a caregiver, had changes in household composition (e.g., parents divorced), had financial difficulties, and had the highest likelihood of family members with substance use problems in early childhood. Finally, the Low Adversity class included children who had relatively lower exposure to adversity as compared to the Family Illness and Financial Difficulties and Household Stressors classes.
Figure 1. Composition of Child Adversity Classes in First Grade.
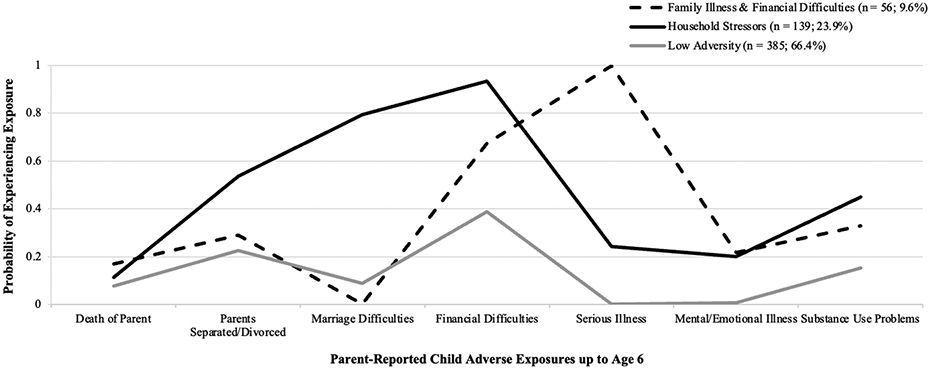
Note. Figure reflects heterogeneity in parent-reported children’s lifetime adversity to age 6 with adverse items listed on the x-axis and probability of experiencing adverse items on the y-axis.
Middle School Adversity
LCA model fit statistics for characterizing middle school adverse exposures indicated that a 3-class model was the best fit. The 3-class model had the lowest BIC values, compared to 1-, 2-,4- and 5-class models. Although the size of the smallest class was comparable for 3- and 4-class models and the LMR p-value was significant in the 4-class model, classification diagnostics (e.g., latent class posterior probabilities, entropy) pointed to a 3-class solution as the optimal fit. Further, substantive interpretation of latent subgroups validated the selection of a 3-class model (e.g., addition of 4th class did not enhance the interpretability of heterogeneity of exposures). Middle school adversity classes were as follows: Moderate Violence & Law Exposure (class 1, n = 261. 45.0%), Negative Neighborhood Perception & Violence Exposure (class 2, n = 217, 37.4%), and High Family Disruption (class 3, n = 102, 17.6%) (Figure 2); law exposure refers to youth directly getting in trouble with the law and/or having a family member get in trouble with the law and violence exposure includes witnessing or directly experiencing violence such as shooting, stabbing, and/or mugging. Over a third of youth (Negative Neighborhood Perception & Violence Exposure class) experienced high levels of adversity ranging from getting in trouble with the law, witnessing and/or experiencing violence (e.g., getting beat up, stabbed, shot) and perceiving their neighborhood as unsafe (e.g., high endorsement of seeing kids and adults getting beat up in neighborhood every few weeks). Youth in the High Family Disruption (17.6%) class reported higher likelihood of their parents losing or struggling to find a job, being evicted from their house, parents getting divorced and losing contact with parents during their middle school years; it is important to note that these youth also perceived their neighborhoods as unsafe. Youth in the Moderate Violence & Law Exposure class (45%) reported multiple types of adverse exposures, predominated by moderate likelihood of violence and law-related adverse exposures, but perceived their neighborhoods as less unsafe relative to the other subgroups of youth.
Figure 2. Composition of Child Adversity Classes in Middle School.

Note. Figure reflects heterogeneity in youth self-report of adverse life events and perceptions of their neighborhoods in grades 6-8. Adverse items are listed on the x-axis and probability of experiencing adverse items on the y-axis.
High School Adversity
For high school adversity, LCA model fit statistics indicated that a 3-class model provided the best fit. The 3-class model had the lowest BIC values, compared to 1-, 2-,4- and 5-class models. LMR and BLRT p-values showed that a 3-class solution significantly improved model fit compared to a 2-class model. Although LMR and BLRT remained significant in the 4-class model, and the size of the smallest class was comparable for the 3- and 4-class models, the statistical (e.g., IC-related fit statistics) and substantive (e.g., conceptual interpretation) criteria together indicated a 3-class solution as the optimal fit. High school adverse exposure classes were: High Poly-Adversity (class 1, n = 100, 17.2%), Negative Neighborhood Perception & Family Disruption (class 2, n = 307, 52.9%), and Moderate Poly-Adversity (class 3, n = 173, 29.3%) (Figure 3). A little over half of youth (52.9%; Negative Neighborhood Perception & Family Disruption class) endorsed items that reflected perceptions of unsafe neighborhood in addition to parents losing or struggling to find a job and losing contact with parents. Those in the High Poly-Adversity class, a smaller proportion of youth (17.2%) relative to the other subgroups, reported high likelihood of adverse exposures across all measured domains including family (e.g., death of parent, family evicted), community/violence (e.g., getting in trouble with the law, getting shot, stabbed and/or beat up during high school period) and neighborhood (e.g., seeing drunk people on streets during the day) exposures. Those in the Moderate Poly-Adversity class (29.3%) reported experiencing multiple domains of adverse exposures but at a lower likelihood of these exposures relative to the other subgroups of youth.
Figure 3. Composition of Child Adversity Classes in High School.

Note. Figure reflects heterogeneity in youth self-report of adverse life events and perceptions of their neighborhoods in grades 9-12. Adverse items are listed on the x-axis and probability of experiencing adverse items on the y-axis.
LTA Model Fitting Results
Three unconditional latent transition models were evaluated to represent changes in adverse exposures across the developmental time periods. Table 2 compares the model fitting results of regular LTA and RI-LTA models (one model examining fit of a binary random intercept and one assessing the fit of a continuous random intercept). Due to the non-nested nature of these LTA models, log likelihood parameters were not used to evaluate model fit. Therefore, BIC was examined and compared across the three LTA models. RI-LTA with a continuous random intercept had the lowest BIC and sample size adjusted BIC (SSA-BIC), compared to a regular LTA model; this indicated that including a continuous random intercept improved model fit compared to a regular LTA and was appropriate to model changes in adverse exposures over time. The RI-LTA model with a binary intercept had the highest BIC as well as the most number of parameters among the three LTA models and was not considered further. Therefore, a RI-LTA model with a continuous random intercept was selected as the best fit to model within-individual changes in adverse exposures over time.
Unconditional Transition Probabilities from RI-LTA modeling
Unconditional (unadjusted) transition probabilities were examined from the RI-LTA with a continuous random intercept. See Table 3 for complete transition probabilities. Selected transition pathways are summarized here. For example, about 47% of children started in the Low Adversity class (class 3) in elementary school and transitioned into the Negative Neighborhood Perception & Violence Exposure class (class 2) in middle school. From there, 23.5% of youth transitioned to the High Poly-Adversity class (class 3) in high school; this is an example of individuals moving from low adverse exposures in early childhood to higher exposure across middle childhood and into adolescence. Next, 52.4% of children who started in the Family Illness & Financial Difficulties class (class 1) in elementary school moved into the Moderate Violence & Law Exposure class (class 1) in middle school, with about 54.9% of those youth transitioning into the Moderate Poly-Adversity class (class 3) in high school; these are the individuals moving from higher adversity in early childhood to moderate likelihood of adversity exposure in middle and high school periods. A third example pathway represents 24.1% of children who started in the Household Stressors class (class 2) in elementary school and transitioned into the High Family Disruption class (class 3) in middle school, with 9.0% of those youth subsequently transitioned to the High Poly-Adversity class (class 1) in high school. This transition pathway represents children with relatively high likelihood of adverse exposures across all three time points of development. Of note, no one transitioned from the Family Illness & Financial Difficulties class in elementary school to the High Family Disruption class in middle school.
Table 3.
Unconditional Transition Probabilities from Random-Intercept Latent Transition Analysis (RI-LTA; with continuous random intercept) Assessing Changes in Adverse Exposures Over Time
| Middle School Adverse Exposures | High School Adverse Exposures | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Class 1: Moderate Violence & Law Exposure (45%) |
Class 2: Negative Neighborhood Perception & Violence Exposure (37.4%) |
Class 3: High Family Disruption (17.6%) |
Class 1: High Poly- Adversity (17.2%) |
Class 2: Negative Neighborhood Perception & Family Disruption (52.9%) |
Class 3: Moderate Poly- Adversity (29.3%) |
||||
| Elementary School Adverse Exposures | Class 1: Family Illness & Financial Difficulties (9.6%) | .524 | .476 | 0.00 | Middle School Adverse Exposures | Class 1: Moderate Violence & Law Exposure (45%) | .144 | .308 | .549 |
| Class 2: Household Stressors (23.9%) | .301 | .458 | .241 | Class 2: Negative Neighborhood Perception & Violence Exposure (37.4%) | .235 | .650 | .116 | ||
| Class 3: Low Adversity (66.4%) | .468 | .289 | .243 | Class 3: High Family Disruption (17.6%) | .090 | .656 | .253 | ||
Note. Percent (%) refers to percent of children/youth in each latent subgroup over time.
Covariate Modeling Results
Logits for the classification probabilities for most likely class membership were extracted from the unconditional RI-LTA, with a continuous random intercept, and used to fix parameter estimates. Then, covariates (e.g., child gender, race, free/reduced lunch) were included to examine predictors of latent adversity class membership in elementary, middle and high schools. Class structure from this model was compared to the unconditional model to ensure that there was no class shifting upon including covariates in the model.
Covariates were unrelated to adverse exposure classes in elementary school. In middle school, youth in the Moderate Violence & Law Exposure class (class 1) were less likely to have received free/reduced lunch in first grade compared to youth in the High Family Disruption class (class 3), OR = .19, z = −2.59, p = .01, 95% CI (confidence interval): .05, .66). Further, in middle school, youth in the Negative Neighborhood Perception & Violence Exposure class (class 2) were less likely to receive free/reduced lunch compared to those in the High Family Disruption class, OR = .22, z = −2.19, p = .03, 95% CI: .05, .85. In addition, youth who were in the Negative Neighborhood Perception & Violence Exposure class in middle school were less likely to be girls than those in the High Family Disruption class, OR = .32, z = −2.68, p = .007, 95% CI: .14, .74; taken together, youth in the High Family Disruption class were more likely to receive free/reduced lunch compared to the other subgroups of youth and more likely to be girls as compared to youth in the Negative Neighborhood & Violence Exposure class. Interestingly, covariates were unrelated to adverse exposure classes in high school and neither classroom nor family interventions were related to adverse class membership over time.
Figure 4 is a visual depiction of the changes in adverse exposures from elementary to high school (left to right) from the fully adjusted RI-LTA, with a continuous random intercept, model. The thickness of the connecting lines across latent adversity classes reflects the transition probabilities after adjusting for child race, gender, free/reduced lunch, and intervention status; thicker lines represent higher probability of transitioning through that pathway. Fully adjusted and unadjusted (unconditional) transition probabilities were comparable; however, in the fully adjusted RI-LTA model with continuous intercept, there were no youth who moved from the Negative Neighborhood Perception & Violence Exposure class in middle school to the Moderate Poly-Adversity class in high school.
Figure 4. Sankey Diagram Reflecting Transition Probabilities from Adjusted RI-LTA Model.

Note. Left of figure: first grade adversity classes, middle of figure: middle school adversity classes, right of figure: high school adversity classes; RI-LTA model was adjusted for child race, gender, free/reduced lunch status and intervention status (~33% control, ~33% classroom-based, ~33% family-school partnership); thicker lines indicate higher transition probability.
Outcome Modeling Results
To explore the association of within-individual adverse exposures over time with mental health and suicidal behaviors from 6th grade through emerging adulthood (age 26), mental health variables were modeled as a distal outcome from the high school latent class, accounting for all prior adversity transitions in separate models. From the covariate-adjusted model with fixed parameter estimates detailed above, mental health and suicidal behaviors were estimated as prevalences (e.g., percent of individuals reporting anxiety/depression diagnosis in a specific transition pathway). Models were adjusted for child gender and race, free/reduced lunch status, and indicator variables for intervention status (classroom vs. not, family vs. not). Full results of within-individual pathways and resultant prevalence of anxiety/depression diagnoses, suicide ideation and suicide attempt from the separate models are presented in Table 4; there were seven transition pathways with no individuals; therefore, results in Table 4 are presented for the remaining 20 latent transition pathways and selected findings are summarized here.
Table 4.
Random Intercept Latent Transition Analysis (RI-LTA; with continuous random intercept) examining Trajectories of Adversity Exposure and Mental Health and Suicidal Behaviors
| Within-Individual Exposure Pathways | Mental Health and Suicidal Behaviors | |||||
|---|---|---|---|---|---|---|
| First Grade Adversity |
Middle School Adversity |
High School Adversity |
Depression/ Anxiety Diagnosis (% yes) |
Suicide Ideation (% yes) |
Suicide Attempt (% yes) |
Number of Individuals in Latent Transition Pathway |
| Family Illness and Financial Difficulties (1) | Moderate Violence & Law Exposure (1) | High Poly-Adversity (1) | 14.9 | 49.1 | 26.3 | 1 |
| Family Illness and Financial Difficulties (1) | Moderate Violence & Law Exposure (1) | Negative Neighborhood & Family Disruption (2) | 12.6 | 41.6 | 33.4 | 14 |
| Family Illness and Financial Difficulties (1) | Moderate Violence & Law Exposure (1) | Mod Poly-Adversity (3) | 3.2 | 6.1 | 16.6 | 18 |
| Family Illness and Financial Difficulties (1) | Neighborhood &Violence Exposure (2) | High Poly-Adversity (1) | 5.2 | 45.2 | 23.7 | 10 |
| Family Illness and Financial Difficulties (1) | Neighborhood &Violence Exposure (2) | Negative Neighborhood & Family Disruption (2) | 3.8 | 19.3 | 20.2 | 13 |
| Family Illness and Financial Difficulties (1) | Neighborhood &Violence Exposure (2) | Mod Poly-Adversity (3) | 0 | |||
| Family Illness and Financial Difficulties (1) | High Family Disruption (3) | High Poly-Adversity (1) | 0 | |||
| Family Illness and Financial Difficulties (1) | High Family Disruption (3) | Negative Neighborhood & Family Disruption (2) | 0 | |||
| Family Illness and Financial Difficulties (1) | High Family Disruption (3) | Mod Poly-Adversity (3) | 0 | |||
| Household Stressors (2) | Moderate Violence & Law Exposure (1) | High Poly-Adversity (1) | 0 | |||
| Household Stressors (2) | Moderate Violence & Law Exposure (1) | Negative Neighborhood & Family Disruption (2) | 6.6 | 13.4 | 22.4 | 3 |
| Household Stressors (2) | Moderate Violence & Law Exposure (1) | Mod Poly-Adversity (3) | 5.6 | 11.9 | 15.4 | 21 |
| Household Stressors (2) | Neighborhood &Violence Exposure (2) | High Poly-Adversity (1) | 16.6 | 36.6 | 32.5 | 17 |
| Household Stressors (2) | Neighborhood &Violence Exposure (2) | Negative Neighborhood & Family Disruption (2) | 3.0 | 12.9 | 16.3 | 59 |
| Household Stressors (2) | Neighborhood &Violence Exposure (2) | Mod Poly-Adversity (3) | 8.6 | 30.4 | 30.9 | 2 |
| Household Stressors (2) | High Family Disruption (3) | High Poly-Adversity (1) | 0 | |||
| Household Stressors (2) | High Family Disruption (3) | Negative Neighborhood & Family Disruption (2) | 2.6 | 14.3 | 25.2 | 28 |
| Household Stressors (2) | High Family Disruption (3) | Mod Poly-Adversity (3) | 7.7 | 16.7 | 26.0 | 9 |
| Low Adversity (3) | Moderate Violence & Law Exposure (1) | High Poly-Adversity (1) | 33.1 | 51.7 | 28.1 | 33 |
| Low Adversity (3) | Moderate Violence & Law Exposure (1) | Negative Neighborhood & Family Disruption (2) | 4.7 | 9.4 | 10.7 | 69 |
| Low Adversity (3) | Moderate Violence & Law Exposure (1) | Mod Poly-Adversity (3) | 6.8 | 16.1 | 20.0 | 102 |
| Low Adversity (3) | Neighborhood &Violence Exposure (2) | High Poly-Adversity (1) | 17.9 | 34.0 | 26.1 | 30 |
| Low Adversity (3) | Neighborhood &Violence Exposure (2) | Negative Neighborhood & Family Disruption (2) | 3.4 | 11.4 | 10.9 | 66 |
| Low Adversity (3) | Neighborhood &Violence Exposure (2) | Mod Poly-Adversity (3) | 0 | |||
| Low Adversity (3) | High Family Disruption (3) | High Poly-Adversity (1) | 38.1 | 38.0 | 33.0 | 1 |
| Low Adversity (3) | High Family Disruption (3) | Negative Neighborhood & Family Disruption (2) | 4.2 | 13.5 | 20.2 | 58 |
| Low Adversity (3) | High Family Disruption (3) | Mod Poly-Adversity (3) | 8.5 | 16.5 | 27.9 | 20 |
Note. Within-individual adverse exposure pathways (transitions in adverse exposures over time; latent class number in parentheses for interpretability) through adolescence listed on the left with resultant prevalence of experiencing mental health outcomes and suicide-related behaviors expressed as percentages (%) on the right. Boxes shaded in gray represent exposure pathways with no individuals based on final class counts and proportions based on most likely latent class pattern the RI-LTA models.
The overall test statistic for depression and/or anxiety disorder diagnosis suggested differences in prevalence of these two diagnoses across classes (Wald test (2) = 12.70, p=0.002). Examination of pairwise comparisons suggested that prevalence of depression and/or anxiety disorder diagnosis significantly differed between the High Poly-Adversity class and the Negative Neighborhood & Family Disruption class (OR = .14, z = −2.88, p = .004) and the Moderate Poly-Adversity class (OR = .24, z = −2.99, p = .003), accounting for covariates and prior waves of adverse exposures; prevalence of anxiety/depression diagnoses were lower among those in the Negative Neighborhood & Family Disruption (3.8%) and Moderate Poly-Adversity (6.6%) classes compared to those in the High Poly-Adversity class (22.3%). There were no differences in the prevalence of an anxiety/depression diagnosis between the Negative Neighborhood & Family Disruption and Moderate Poly-Adversity classes.
Individuals who transitioned from latent classes of Low Adversity in elementary school to High Family Disruption in middle school and subsequently High Poly-Adversity in high school had the highest prevalence of anxiety/depression diagnoses (38.1%). The lowest prevalence of anxiety/depression diagnoses based on outcome modeling was 2.6% corresponding to those who started in the Household Stressors class in elementary school and transitioned into the High Family Disruption class in middle school and then to the Negative Neighborhood & Family Disruption class in high school. Generally, those who ended in the Negative Neighborhood & Family Disruption class had relatively lower prevalence of anxiety/depression diagnosis, irrespective of prior adverse exposures, though prevalences varied (range 2.6% - 12.6%).
The overall Wald test suggested that adversity latent class membership in high school, accounting for prior adverse exposures, was associated with suicide ideation at a trend level (Wald (2) = 5.32, p=0.07). Exploring pairwise comparisons suggested two significant differences across the latent classes. Individuals in the Negative Neighborhood Perception & Family Disruption class and Moderate Poly-Adversity class were less likely to report suicide ideation as compared to those in the High Poly-Adversity class (prevalence of suicide ideation 13.2%, 14.7% and 42.0%, respectively; OR = .38, z=−1.96, p=0.05, and OR = .35, z = −2.27, p = .02 respectively). There was no significant difference when comparing endorsement of suicide ideation between the Negative Neighborhood Perception & Family Disruption and the Moderate Poly-Adversity classes.
Given that over a third of participants (35.1%) overall reported suicidal ideation, and there were significant pairwise comparisons in outcome modeling, within-individual pathways and resultant prevalence of suicide ideation were probed further. The highest prevalence of suicide ideation (78.0%) was seen among those who moved from Family Illness and Financial Difficulties in elementary school to Negative Neighborhood Perception & Violence Exposure in middle school and subsequently to the High Poly-Adversity class in high school. The lowest prevalence of suicide ideation (16.9%) corresponded to those who started in the Low Adversity class in elementary school, had Moderate Violence & Law Exposure in middle school and Moderate Poly-Adversity in high school; this transition pathway represents those who had relatively lower likelihood of adversity across elementary, middle and high schools compared to other subgroups of individuals. Those who ended in the High Poly-Adversity class in high school had an overall higher prevalence of suicide ideation (43.6% - 78%).
The overall Wald test for suicide attempt was not statistically significant (Wald (2) =2.81, p=0.24) and no significant pairwise comparisons were found with suicide attempts and within-individual adverse exposure pathways. In general, the lowest prevalence of suicide attempt was among those who ended in the Negative Neighborhood Perception & Family Disruption class (range 10.7% - 33.4%), however, patterns across time were mixed and interpretation of findings is therefore speculative.
DISCUSSION
Our findings highlight how children are exposed to changing forms of adversity across development that have differential associations with lifecourse mental health. With this, we underscore the need to examine adversity as a dynamic exposure across sensitive periods of development from early childhood through adolescence to understand and characterize variability in both exposures and mental health correlates. Specifically, results indicated distinct subgroups of children who experience varying types and levels of adversity that differ in childhood, middle childhood, and adolescence as evidenced by latent classes of exposure over development.
Three latent classes of adversity were found at each developmental period but varied in composition. In elementary school (up to age 6), children were primarily characterized as experiencing household stressors (24%) including high likelihood of family financial difficulties, parental marriage difficulties and substance use in the household, or low adversity (66.4%), indicating relatively lower adversity. It is important to note here that children in the low adversity class still experienced multiple types of adverse exposures (e.g., family financial difficulties, some substance use in household). Interestingly, a smaller but notable group of children (9.6%) were exposed to living in a household with family members who had serious mental, emotional, and physical illnesses.
A wealth of research indicates the negative impacts of adversity in early childhood on health and development including disruptions to brain structure, physiological stress response/regulation, and cumulative tolls on physical (e.g., cardiovascular disease) and mental health (e.g., depression) through the life course (McLaughlin et al., 2019; Schroeder et al., 2020; Wymbs et al., 2020). Our findings reveal that regardless of adversity latent class in first grade, children experienced disruptions in multiple aspects of family-level stability, including financial difficulties, changes in household composition and/or caregiver stressors (e.g., mental illness) that have implications for their well-being. Safe, stable, and nurturing caregiver relationships are crucial to children’s positive development and well-being, with salience in early childhood (Mercy & Saul, 2009). Potential disruptions and stressors within the family, as evidenced by our latent class findings in elementary school, in turn, can impact social, emotional and cognitive development and mental well-being. As such, examining the heterogeneity in adverse exposures allows for a better understanding of what domains of a child’s environment to bolster with preventive interventions (e.g., intervention following death of a parent focused on reducing socioemotional distress related to grief and enhancing children’s coping strategies) (Pereira et al., 2017).
In middle and high school, we leveraged youth’s self-report of their adverse exposures which, in addition to family exposures (e.g., parent died in past year), also included peer (close friend died), law enforcement (e.g., got in trouble with the law), violence (witnessing and/or experience) and neighborhood (e.g., people damage property/steal in neighborhood) domains of adversity. Heterogeneity in adverse exposures differed between middle and high school as evidenced by dissimilar latent class patterns in each developmental period, despite using the same items to measure adversity. For example, some youth (17.6%) experienced adversity characterized by high likelihood of family disruption such as parents losing or struggling to find a job, being evicted from their home, and parental divorce or loss of contact in middle school. Meanwhile, in high school, about 17% of youth experienced high likelihood of multi-domain adversity and the family disruption class seen in middle school was no longer identified. Even with the use of youth self-report in both middle and high school, we see that the construct of adverse exposures varied over time. Our findings suggest that children experience shifts in their adverse exposures in both the middle and high school periods that could be a product of increased autonomy and changes in peer relationships (Pollmann et al., 2022). In addition, variability of adverse exposures could reflect the change in developmental influences from internal family environments, which predominate in childhood, to broader social and ecological exposures such as different neighborhood characteristics and changing peer groups.
The middle and high school time points encompass middle childhood and adolescence, developmental periods characterized by swift physical, environmental and expectational changes wherein social, emotional, behavioral, and physical competencies are established and honed to support successful transitions into adolescence and adulthood (Laurens et al., 2017). Thus, they can be considered key developmental periods for establishing socioemotional well-being and adaptation, but also corollary to increased risk for future adverse health and well-being (Laurens et al., 2017). As such, examining disruptions in environments in childhood and adolescence can allow for closer examination of exposures that may strongly influence mental health and well-being. Less is known about the role that adversity has on mental health during middle childhood/early adolescence; therefore, our findings motivate future research to continue to parse this. Taken together, we see that youth are exposed not only to multiple, overlapping types of adversity, but also that the exposure patterns vary over time and development.
Interestingly, in middle school, youth in the Negative Neighborhood Perception & Violence Exposure class (37.4%) and those in the Moderate Violence & Law Exposure class (45%) both had somewhat similar levels of adversity exposures in the family and peer domains but differed in their violence exposure (witnessing and/or experiencing) and perceptions of neighborhood safety. Youth who reported lower likelihood of witnessing and/or experiencing violence perceived their neighborhood as safer than youth who had higher violence exposures; this concordance between violence exposure and perception of the neighborhood remained in high school. We see that witnessing violence increased from middle school to high school (49.1% to 66.4% of youth reporting yes to witnessing violence) and experiencing violence more than doubled in prevalence from middle school to high school periods (10.5% to 21%). Large proportions of children in the US are exposed to violence in their homes, schools, and communities, with urban residing Black children at highest risk for exposure (Gollub et al., 2019). There is evidence that exposure to family, peer, and community-level violence exposures, both through witnessing and direct experience, has negative consequences for youth mental health (Foell et al., 2021). By examining exposures separately in both middle school and high school, we can clarify when, and at what level, to target interventions to best support youth. These interventions include, for example, community-based strategies to increase access to extracurricular activities (Bungay & Vella-Burrows, 2013) or media-based interventions to promote socioemotional coping and provide mental health supports (Das et al., 2016).
Our results indicate significant heterogeneity in adverse exposures and changes in latent transition pathways over time. As such, examining changes in exposures over time is a crucial extension to the existing measurement framework used to characterize life course adversity. We find evidence for some children moving from low adversity in elementary school to reporting moderate adversity in middle school and reporting high exposure to adversity in high school. We also see some children experiencing high exposure to family-domain adversity earlier and having lower exposure to adverse experiences in middle and high school. At the same time, some experienced high or low adverse exposures across all time points or particularly high peaks in middle school. Even after accounting for between-youth changes in adversity, we see significant within-person heterogeneity in exposure over time in our sample. There is no single consistent pattern of exposure or change over time, highlighting that exposure to adversity is not equally distributed among youth over time. Taken together, the results signal that adversity is not static or a trait-level characteristic. This suggests that the field should move forward with examining multiple time points to better disentangle sources of adversity and their influence on development and well-being.
Finally, based on prior literature, we know that there is a strong relationship between exposure to adverse and poorer mental health. However, less is known about how the timing, duration, and severity of adverse exposures through the life course relate to adult mental health variability. Findings from the RI-LTA model with mental health correlates illustrated that there is not one pathway of adverse exposures that had the majority proportion of poor mental health; instead, general findings from modeling mental health correlates point to the need for multiple touch points of preventive intervention through development to have a larger impact on mental health and well-being. Methodologically parsing out the within- and between-individual variation in exposure pathways leading to varied mental health correlates allows one to examine the result of specific pathways on individual- and population-level differences in mental health.
Prior research has posited several potential mechanisms through which adversity can impact health and development. While our analysis was not a direct test of each of these potential mechanisms, our findings do add some support for potential sensitive periods in development during which exposure to adversity can be particularly influential. Further, there was support for the recency mechanism, suggesting that the impact of adversity exposure is time-limited and that exposure proximal to the outcome of interest may have the biggest impact (Nelson et al., 2020); generally, across our mental health correlates, those with the most severe adversity exposure during adolescence showed somewhat worse mental health. This was particularly true for the prevalence of anxiety/depression diagnoses and suicide ideation. Likely, the mechanism through which adversity impacts health and development will depend on the way adversity is conceptualized, as well as the particular outcome of interest.
Our findings add knowledge to the adversity exposure literature given the uniqueness of the cohort. This sample was captured from Baltimore City beginning in the early 1990s, a time during which levels of violence in the city as a whole were high. As a result of higher community violence, participants in this cohort were likely exposed to more community and interpersonal violence than average. While these intense adversity exposures provided us with an opportunity to explore these trajectories, our findings may not be generalizable to other populations with less overall burden of adversity exposure. With that being said, this level of adversity exposure is often seen in other urban, underfunded, and racially segregated cities. Our findings may indeed apply to children living in cities with moderate to high levels of community violence.
Our findings also show that there is a certain level of mobility, with some children moving to more positive environments over time. Given that families with lower incomes are typically more mobile than more economically advantaged families (DeLuca & Jang-Trettien, 2020), some prevention programs explicitly target improving the environment in which a child is living. For example, the Safe Streets program was adapted from the CeaseFire program and implemented in Baltimore City (Webster et al., 2013). This program explicitly targets gun violence, a major source of adversity exposure for children living in Baltimore. Results from the trial suggested significant changes in gun-related violence in the neighborhoods in which the program was implemented. The theorized mechanism through which the program impacted violence was through conflict mediation done by program outreach workers. The results of this program suggest that along with physically moving out of areas with high levels of violence, programming within neighborhoods can improve children’s experiences.
Implications for Public Mental Health and Children
The findings from this study, and others finding significant associations between adversity exposure and mental health, have crucial implications for prevention and intervention efforts targeted toward children and adolescents. Our findings support the implementation of multiple touchpoints of preventive intervention programming throughout development. Further, regardless of whether a program explicitly targets children exposed to adversity, all prevention programming should take adversity exposure into consideration. Similarly, when screening for adversity exposure, either in a clinical setting or for tailoring prevention programming, we must remember that adversity exposure happens across development and therefore must be assessed and addressed frequently. Finally, when considering the development of prevention programming targeting children exposed to adversity, there should be a focus not only on externalizing behaviors, but also on internalizing problems.
Limitations and Strengths
With unique longitudinal data spanning over 20 years, we identified prevalent changes in children’s adverse exposures across key developmental periods. The inclusion of mental health correlates from adolescence to emerging adulthood also formed a life course evaluation of exposure to outcome and is a strength of this study. A key strength and contribution of the current study is the expansion of measurement of adverse exposures by including repeated time points and leveraging longitudinally collected data. Although the field of adversity and development is moving toward utilizing prospectively collected data, a large proportion of existing work relies on adult retrospective report of their exposures in childhood and/or one time point of youth self-report (e.g., adolescence). A potentially useful framework for measuring life course changes in adverse exposures is collecting and analyzing repeated, prospective accounts of exposures. This would allow for careful examination of changes in adversity over time and can elucidate when and what types of support would benefit children and families. To fill this measurement gap, we included reports of adverse exposures in elementary, middle, and high school periods, including youth’s perceptions at the time of exposure occurrence. These repeated measures allowed us to capture unique exposures that happened within developmental periods. In addition, we examined adversity that children and youth experience occurring across multiple domains including family (e.g., death of a parent), peers (e.g., death of a close friend), and community (e.g., getting in trouble with the law, neighborhood safety). We also characterized witnessing and experiencing various forms of violence such as mugging, stabbing, and shooting, which may have salient associations with mental health, particularly exposure during adolescence. By including an expanded measurement of adversity, we captured a more well-rounded picture of the milieu of experiences informing children/youth’s adverse exposures.
Our study also has methodological strengths. First, we examined heterogeneity in adverse exposures separately in each developmental period using latent class analyses. This allowed for a better understanding of different subgroups of children that had similar patterns of adverse exposures, while also allowing for each type of adverse exposure to be acknowledged separately, unlike cumulative or sum scores. Second, a latent transition model aided in assessing how adverse exposures change over time and across domains. The person-centered approach here emphasizes the importance of considering the co-occurrence of adversity exposures and how those exposures change in individuals over time, which motivated the application of a random-intercept latent transition analysis (RI-LTA) to parse within- and between-individual variation. RI-LTA models between-subject variation through the inclusion of a random intercept; therefore, the transitions between latent classes represent within-subject variation only, offering a clearer understanding of change over time (Muthén & Asparouhov, 2022). Individuals’ ecology changes over time, therefore, it is reasonable to expect that adverse exposures and what constitutes the construct of “adversity” also change over time. Therefore, we did not impose measurement non-invariance on the construct of adversity over time. Further, by modeling within-individual change in adverse exposure, we can understand mechanisms of change at the individual level over time while accounting for heterogeneity in experiences allowing for modeling the complexity in adverse exposures by type, timing, and duration. Finally, there may be unmeasured variables that predict both adversity exposure and mental health outcomes and such confounding is minimized by employing a within-subject design.
Limitations of our study must also be acknowledged. To begin, this study is not a good test of the cumulative impact of adversity because we did not treat each adversity exposure as a count or create a count of each adversity exposure at each developmental period. Despite the range of data collected and sufficient sample size, we dichotomized adverse exposures to account for small cell sizes, which may have limited variability. We first examined the prevalence of the categorical adverse exposure indicators as originally coded; however, we collapsed small categories with adjacent categories and into the developmental time points of interest (e.g., middle school, high school) to avoid empty cells in model estimation and streamline interpretation of model indicators and estimates. Additionally, because of model constraints and small cell sizes, we were not able to assess the role of time-varying covariates on transition probabilities. Moreover, we did not examine distal factors that predicted the propensity to be in different transition probabilities. Some of the factors that we treated as covariates (e.g., demographic characteristics) could also be modeled as distal factors. While the initial preventive interventions in 1st grade were nested within classrooms and schools, we were unable to account for clustering of participants within schools after first grade since by second grade the participating students who began the study in 9 schools and 27 classrooms were distributed across 71 schools and over 100 classrooms. In most of these schools there were only a handful of students. The number of schools and classrooms grew dramatically over the elementary, middle and high school years. Indeed, by 12th grade, the participants were distributed across 131 schools. Importantly, the school that participants attended in Baltimore City was not, in some cases, in the same neighborhood that they lived in after elementary school; as such, we do not expect that accounting for nesting of students within their 1st-grade schools would account for variability in exposures over time. Nevertheless, as a sensitivity analysis, we examined if accounting for clustering of participants within schools in first grade affected parameter estimates, particularly standard error of estimates; there were no changes in parameter estimates when accounting for clustering in first grade vs. not; therefore, we proceeded with models without clustering effects. It is important to note that we leveraged longitudinal youth self-reports in middle and high schools to capture youth’s own exposures in areas that they frequented through development (e.g., own or peer neighborhoods). This allowed us to gain a better understanding of their environments and how they changed over time, accounting for repeated measures within participants. Further, the reporter of adverse exposures changed over time; this study collected parent report in early childhood, with a focus on family-level adversity. Youth self-report of adverse exposures was collected in middle and high school periods capturing additional domains of exposure (e.g., violence exposure). In addition, the items included in the measurement of adversity changed between elementary school and middle/high school periods. Nonetheless, we saw differences in the types of adverse exposures between middle and high school periods, which used the same items. While variation in reporter and items at each time period is a limitation, our analytic method does not require that the construct of adversity is the same over time and allows us to flexibly estimate heterogeneity in adverse exposures even with the change in reporters and items. Notably, while the data used came from the longitudinal follow-up of a trial of universal interventions targeting aggressive and disruptive behavior, we did not formally test the impact of the interventions on adversity exposure. The proximal targets of the interventions were the promotion of academic achievement and the reduction of aggressive behavior in 1st grade. As such, we did not expect the interventions to affect youth’s adverse exposures, particularly across the domains examined in this study. However, downstream cross-over intervention effects on adult mental health outcomes are plausible. As such, intervention status was included in all models. Post-hoc analyses indicated no differences in the prevalences of anxiety and depressive disorders or suicide ideation or attempts by first grade intervention status. This could be partially due to the relatively low prevalence of the mental health correlates assessed in our sample. The low prevalences, in turn, may be a result of structural and societal factors in historically excluded communities (e.g., stigma associated with mental health, barriers to access mental health professionals) and/or may indicate the need for culturally sensitive measurement tools (Adams et al., 2021). Further, we were unable to establish directionality between adverse exposures and mental health in part due to the low prevalence of anxiety, depression, and suicidal behaviors in the emerging adulthood period alone, therefore we focused our investigation on mental health correlates using available data across developmental periods. Finally, the focus of this analysis was on a somewhat narrow set of mental health correlates. Future research should explore the impact of these exposure trajectories on other mental, behavioral, and physical health outcomes.
Conclusion
To date, research on adverse exposures and life course health has focused on lifetime experiences of adversity and, as such, has often treated adversity as a static measure. Our findings suggest that adverse exposures are dynamic over time and adapting measurement to assess exposures within and between different developmental periods is key to capturing variation over time. Similarly, we saw differential pathways between exposure to adversity and mental health, suggesting variability in the role of adversity on mental health and well-being. Perhaps analytic models that allow for variation in mental health status over time in tandem with changes in adverse exposures will be better suited to modeling the heterogeneity and complexity of such relationships. Taken together, researchers, clinicians and practitioners may be in a better position to address the impact of, and changes in, adversity exposure using repeated assessments of adversity focused on narrower snapshots of development. In conclusion, it is evident that prevention and intervention efforts must be developed to address adversity exposure and its role in health and well-being, moving beyond individually-focused interventions to multi-level programming that spans development.
PUBLIC HEALTH SIGNIFICANCE.
Children are exposed to changing forms of adversity across development with differential impacts on mental health. Focusing on repeated, adaptive, coordinated, and multi-level preventive mental health efforts will be crucial to support the well-being of children and adolescents through the life course.
References
- Adams LB, Baxter SLK, Lightfoot AF, Gottfredson N, Golin C, Jackson LC, Tabron J, Corbie-Smith G, & Powell W (2021). Refining Black men’s depression measurement using participatory approaches: a concept mapping study. BMC Public Health, 21(1), 1194. 10.1186/s12889-021-11137-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andersen SH, Steinberg L, & Belsky J (2021). Beyond early years versus adolescence: The interactive effect of adversity in both periods on life-course development. Developmental Psychology, 57(11), 1958–1967. 10.1037/dev0001247 [DOI] [PubMed] [Google Scholar]
- Berman IS, McLaughlin KA, Tottenham N, Godfrey K, Seeman T, Loucks E, Suomi S, Danese A, & Sheridan MA (2022). Measuring early life adversity: A dimensional approach. Dev Psychopathol, 34(2), 499–511. 10.1017/s0954579421001826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bethell CD, Carle A, Hudziak J, Gombojav N, Powers K, Wade R, & Braveman P (2017). Methods to Assess Adverse Childhood Experiences of Children and Families: Toward Approaches to Promote Child Well-being in Policy and Practice. Acad Pediatr, 17(7s), S51–s69. 10.1016/j.acap.2017.04.161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bungay H, & Vella-Burrows T (2013). The effects of participating in creative activities on the health and well-being of children and young people: a rapid review of the literature. Perspect Public Health, 133(1), 44–52. 10.1177/1757913912466946 [DOI] [PubMed] [Google Scholar]
- Coddington RD (1972). The significance of life events as etiologic factors in the diseases of children. II. A study of a normal population. J Psychosom Res, 16(3), 205–213. 10.1016/0022-3999(72)90045-1 [DOI] [PubMed] [Google Scholar]
- Compas BE, Davis GE, & Forsythe CJ (1985). Characteristics of life events during adolescence. American Journal of Community Psychology, 13(6), 677–691. 10.1007/BF00929795 [DOI] [PubMed] [Google Scholar]
- Cooley-Quille MR, Turner SM, & Beidel DC (1995). Emotional impact of children's exposure to community violence: a preliminary study. J Am Acad Child Adolesc Psychiatry, 34(10), 1362–1368. 10.1097/00004583-199510000-00022 [DOI] [PubMed] [Google Scholar]
- Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, Pachter LM, & Fein JA (2015). Adverse Childhood Experiences: Expanding the Concept of Adversity. Am J Prev Med, 49(3), 354–361. 10.1016/j.amepre.2015.02.001 [DOI] [PubMed] [Google Scholar]
- Das JK, Salam RA, Lassi ZS, Khan MN, Mahmood W, Patel V, & Bhutta ZA (2016). Interventions for Adolescent Mental Health: An Overview of Systematic Reviews. J Adolesc Health, 59(4s), S49–s60. 10.1016/j.jadohealth.2016.06.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeLuca S, & Jang-Trettien C (2020). “Not Just a Lateral Move”: Residential Decisions and the Reproduction of Urban Inequality. City & Community, 19(3), 451–488. https://doi.org/ 10.1111/cico.12515 [DOI] [Google Scholar]
- Dunn EC, Soare TW, Raffeld MR, Busso DS, Crawford KM, Davis KA, Fisher VA, Slopen N, Smith A, Tiemeier H, & Susser ES (2018). What life course theoretical models best explain the relationship between exposure to childhood adversity and psychopathology symptoms: recency, accumulation, or sensitive periods? Psychol Med, 48(15), 2562–2572. 10.1017/s0033291718000181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn EC, Soare TW, Zhu Y, Simpkin AJ, Suderman MJ, Klengel T, Smith A, Ressler KJ, & Relton CL (2019). Sensitive Periods for the Effect of Childhood Adversity on DNA Methylation: Results From a Prospective, Longitudinal Study. Biol Psychiatry, 85(10), 838–849. 10.1016/j.biopsych.2018.12.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott DS, Huizinga D, & Ageton SS (1985). Explaining delinquency and drug use (Vol. 27). Sage Publications; Beverly Hills, CA. [Google Scholar]
- Elmore AL, & Crouch E (2020). The Association of Adverse Childhood Experiences With Anxiety and Depression for Children and Youth, 8 to 17 Years of Age. Acad Pediatr, 20(5), 600–608. 10.1016/j.acap.2020.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK, & Bandalos DL (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling, 8, 430–457. 10.1207/S15328007SEM0803_5 [DOI] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Koss MP, & Marks JS (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. 10.1016/S0749-3797(98)00017-8 [DOI] [PubMed] [Google Scholar]
- Foell A, Pitzer KA, Nebbitt V, Lombe M, Yu M, Villodas ML, & Newransky C (2021). Exposure to community violence and depressive symptoms: Examining community, family, and peer effects among public housing youth. Health Place, 69, 102579. 10.1016/j.healthplace.2021.102579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gollub EL, Green J, Richardson L, Kaplan I, & Shervington D (2019). Indirect violence exposure and mental health symptoms among an urban public-school population: Prevalence and correlates. PLOS ONE, 14(11), e0224499. 10.1371/journal.pone.0224499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gondek D, Patalay P, & Lacey RE (2021). Adverse childhood experiences and multiple mental health outcomes through adulthood: A prospective birth cohort study. SSM - Mental Health, 1, 100013. https://doi.org/ 10.1016/j.ssmmh.2021.100013 [DOI] [Google Scholar]
- Graham JW (2009). Missing data analysis: making it work in the real world. Annu Rev Psychol, 60, 549–576. 10.1146/annurev.psych.58.110405.085530 [DOI] [PubMed] [Google Scholar]
- Hajat A, Nurius P, & Song C (2020). Differing trajectories of adversity over the life course: Implications for adult health and well-being. Child Abuse & Neglect, 102, 104392. https://doi.org/ 10.1016/j.chiabu.2020.104392 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ialongo NS, Werthamer L, Kellam SG, Brown CH, Wang S, & Lin Y (1999). Proximal Impact of Two First-Grade Preventive Interventions on the Early Risk Behaviors for Later Substance Abuse, Depression, and Antisocial Behavior. American Journal of Community Psychology, 27(5), 599–641. https://doi.org/ 10.1023/A:1022137920532 [DOI] [PubMed] [Google Scholar]
- Johnson SB, Riley AW, Granger DA, & Riis J (2013). The science of early life toxic stress for pediatric practice and advocacy. Pediatrics, 131(2), 319–327. 10.1542/peds.2012-0469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Juwariah T, Suhariadi F, Soedirham O, Priyanto A, Setiyorini E, Siskaningrum A, Adhianata H, & Fernandes ADC (2022). Childhood adversities and mental health problems: A systematic review. J Public Health Res, 11(3), 22799036221106613. 10.1177/22799036221106613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laurens KR, Tzoumakis S, Dean K, Brinkman SA, Bore M, Lenroot RK, Smith M, Holbrook A, Robinson KM, Stevens R, Harris F, Carr VJ, & Green MJ (2017). The 2015 Middle Childhood Survey (MCS) of mental health and well-being at age 11 years in an Australian population cohort. BMJ Open, 7(6), e016244. 10.1136/bmjopen-2017-016244 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCubbin HI, Patterson JM, Bauman E, & Harris L (1985). A-FILE: Adolescent--Family Inventory of Life Events and Changes. Family inventories: inventories used in a national survey of families across the family life cycle/[David H. Olson…[et al.]]. [Google Scholar]
- McLaughlin KA, Weissman D, & Bitrán D (2019). Childhood Adversity and Neural Development: A Systematic Review. Annual Review of Developmental Psychology, 1(1), 277–312. 10.1146/annurev-devpsych-121318-084950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mercy JA, & Saul J (2009). Creating a Healthier Future Through Early Interventions for Children. JAMA, 301(21), 2262–2264. 10.1001/jama.2009.803 [DOI] [PubMed] [Google Scholar]
- Merrick MT, Ford DC, Ports KA, & Guinn AS (2018). Prevalence of Adverse Childhood Experiences From the 2011-2014 Behavioral Risk Factor Surveillance System in 23 States. JAMA Pediatr, 172(11), 1038–1044. 10.1001/jamapediatrics.2018.2537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merrick MT, Ports KA, Ford DC, Afifi TO, Gershoff ET, & Grogan-Kaylor A (2017). Unpacking the impact of adverse childhood experiences on adult mental health. Child Abuse Negl, 69, 10–19. 10.1016/j.chiabu.2017.03.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moos RH, Cronkite R, Billings A, & Finney J (1984). Health and daily living form. Mind Garden. [Google Scholar]
- Muthén B, & Asparouhov T (2022). Latent transition analysis with random intercepts (RI-LTA). Psychol Methods, 27(1), 1–16. 10.1037/met0000370 [DOI] [PubMed] [Google Scholar]
- Naicker SN, Norris SA, & Richter LM (2021). Secondary analysis of retrospective and prospective reports of adverse childhood experiences and mental health in young adulthood: Filtered through recent stressors. eClinicalMedicine, 40. 10.1016/j.eclinm.2021.101094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson CA, Bhutta ZA, Burke Harris N, Danese A, & Samara M (2020). Adversity in childhood is linked to mental and physical health throughout life. BMJ, 371, m3048. 10.1136/bmj.m3048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nylund KL, Asparouhov T, & Muthén BO (2007). Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569. 10.1080/10705510701575396 [DOI] [Google Scholar]
- Nylund-Gibson K, Garber AC, Carter DB, Chan M, Arch DAN, Simon O, Whaling K, Tartt E, & Lawrie SI (2023). Ten frequently asked questions about latent transition analysis. Psychol Methods, 28(2), 284–300. 10.1037/met0000486 [DOI] [PubMed] [Google Scholar]
- Nylund-Gibson K, Grimm RP, & Masyn KE (2019). Prediction from Latent Classes: A Demonstration of Different Approaches to Include Distal Outcomes in Mixture Models. Structural Equation Modeling: A Multidisciplinary Journal, 26(6), 967–985. 10.1080/10705511.2019.1590146 [DOI] [Google Scholar]
- O'Connor M, Slopen N, Becares L, Burgner D, Williams DR, & Priest N (2020). Inequalities in the Distribution of Childhood Adversity From Birth to 11 Years. Acad Pediatr, 20(5), 609–618. 10.1016/j.acap.2019.12.004 [DOI] [PubMed] [Google Scholar]
- Pereira M, Johnsen I, Hauken MA, Kristensen P, & Dyregrov A (2017). Early Interventions Following the Death of a Parent: Protocol of a Mixed Methods Systematic Review. JMIR Res Protoc, 6(6), e127. 10.2196/resprot.7931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollmann A, Fritz J, Barker E, & Fuhrmann D (2022). Networks of Adversity in Childhood and Adolescence and Their Relationship to Adult Mental Health. Research on Child and Adolescent Psychopathology. 10.1007/s10802-022-00976-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reuben A, Moffitt TE, Caspi A, Belsky DW, Harrington H, Schroeder F, Hogan S, Ramrakha S, Poulton R, & Danese A (2016). Lest we forget: comparing retrospective and prospective assessments of adverse childhood experiences in the prediction of adult health. J Child Psychol Psychiatry, 57(10), 1103–1112. 10.1111/jcpp.12621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sacks V, & Murphey DA (2018). The prevalence of adverse childhood experiences, nationally, by state, and by race or ethnicity. [Google Scholar]
- Schroeder A, Slopen N, & Mittal M (2020). Accumulation, Timing, and Duration of Early Childhood Adversity and Behavior Problems at Age 9. J Clin Child Adolesc Psychol, 49(1), 36–49. 10.1080/15374416.2018.1496440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaffer D, Fisher P, Lucas CP, Dulcan MK, & Schwab-Stone ME (2000). NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. J Am Acad Child Adolesc Psychiatry, 39(1), 28–38. 10.1097/00004583-200001000-00014 [DOI] [PubMed] [Google Scholar]
- Shonkoff JP, Garner AS, CHILD, T. C. O. P. A. O., FAMILY HEALTH, C. O. E. C., ADOPTION, DEPENDENT CARE, DEVELOPMENTAL, S. O., PEDIATRICS, B., Siegel BS, Dobbins MI, Earls MF, Garner AS, McGuinn L, Pascoe J, & Wood DL (2012). The Lifelong Effects of Early Childhood Adversity and Toxic Stress. Pediatrics, 129(1), e232–e246. 10.1542/peds.2011-2663 [DOI] [PubMed] [Google Scholar]
- Smith KE, & Pollak SD (2021). Rethinking Concepts and Categories for Understanding the Neurodevelopmental Effects of Childhood Adversity. Perspect Psychol Sci, 16(1), 67–93. 10.1177/1745691620920725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steptoe A, Marteau T, Fonagy P, & Abel K (2019). ACEs: Evidence, Gaps, Evaluation and Future Priorities. Social Policy and Society, 18(3), 415–424. 10.1017/S1474746419000149 [DOI] [Google Scholar]
- Thompson MP, Kingree JB, & Lamis D (2019). Associations of adverse childhood experiences and suicidal behaviors in adulthood in a U.S. nationally representative sample. Child Care Health Dev, 45(1), 121–128. 10.1111/cch.12617 [DOI] [PubMed] [Google Scholar]
- Umberson D, Olson JS, Crosnoe R, Liu H, Pudrovska T, & Donnelly R (2017). Death of family members as an overlooked source of racial disadvantage in the United States. Proceedings of the National Academy of Sciences, 114(5), 915–920. https://doi.org/doi: 10.1073/pnas.1605599114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webster DW, Whitehill JM, Vernick JS, & Curriero FC (2013). Effects of Baltimore's Safe Streets Program on gun violence: a replication of Chicago's CeaseFire Program. J Urban Health, 90(1), 27–40. 10.1007/s11524-012-9731-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wymbs NF, Orr C, Albaugh MD, Althoff RR, O'Loughlin K, Holbrook H, Garavan H, Montalvo-Ortiz JL, Mostofsky S, Hudziak J, & Kaufman J (2020). Social supports moderate the effects of child adversity on neural correlates of threat processing. Child Abuse Negl, 102, 104413. 10.1016/j.chiabu.2020.104413 [DOI] [PMC free article] [PubMed] [Google Scholar]