

Abstract
Background:
The KOJI AWARENESS (KA) test is a practical self-evaluation tool that assesses body movements and may help develop individual conditioning plans to improve movement function. However, the association between preseason KA scores and in-season injury occurrence remains unexplored.
Purpose:
To investigate whether the KA self-screening test score can predict running-related injuries in elite long-distance runners.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 47 elite college male long-distance runners (age, 18-22 years) were enrolled in this study in June 2022. The participants underwent the KA self-screening test to assess preseason upper limb, core, and lower limb function. Running-related injuries with a training time loss of >3 weeks were tracked for 6 months during the season. The participants were divided into injury and noninjury groups, and between-group comparisons and receiver operating characteristic (ROC) curve analysis were used to determine the association between the KA scores and the injury incidence. Chi-square tests and risk ratios were calculated based on the cutoff value- and injury-based grouping.
Results:
Among the runners, 10 (21.3%) sustained an injury. There were no significant differences in the demographic characteristics between the injury and noninjury groups. The injury group had significantly lower KA scores than the noninjury group (median, 44.5 [interquartile range, 43-46.8] vs median, 48 [interquartile range, 46-50], respectively; P = .009). The ROC curve analysis determined a cutoff value of 46.5 points (sensitivity, 73%; specificity, 63.6%), indicating that the KA scores exhibited a relatively high predictive value for running-related injuries (area under the ROC curve, 0.764 [95% CI, 0.600-0.930]). The risk ratio for group division based on the cutoff value was 2.590 (95% CI, 1.329-5.047).
Conclusion:
These findings demonstrated that the KA test is an effective self-screening tool for predicting the risk of running-related injuries in elite male long-distance runners.
Keywords: injury prediction, KOJI AWARENESS, risk factor, running injury, self-evaluation
Long-distance running has become increasingly popular in recent years, regardless of whether it is an elite or recreational sport.4,17,23,31 Specific injuries are more commonly associated with long-distance running because of the activity's repetitive nature and high impact on the body. 8 Common injuries in distance runners include medial tibial stress syndrome, runner's knee, plantar fasciitis, stress fractures, and iliotibial band syndrome (iliotibial band friction syndrome). 14 The incidence of injuries in long-distance runners can vary based on the characteristics of the study population, type of injury, and duration of the study. Previous studies5,14,15,29 have reported injury rates ranging between 30% and 75%. Injuries can significantly affect runners’ performance by reducing their training volume, intensity, and frequency. When runners are injured, they may need to take time off from training, modify their training program, or even stop competing. This can lead to decreased fitness, running economy, and running speed. In addition, injured runners may experience pain, fatigue, and psychological distress, further hindering their performance.13,18,29
Many studies have analyzed the relationship between running injuries and physical factors such as muscle strength, flexibility, mobility, and stability. †† Studies have found that weakness at lower strength levels, particularly in the hips, core, and lower extremities, increases the risk of running injuries.13,26,30 Poor flexibility, particularly in the lower extremities, can also increase the risk of specific injuries such as plantar fasciitis and Achilles tendinitis.6,7,13,24,26,30 Similarly, limited mobility and poor stability of the lower extremities have been linked to a higher risk of injuries such as iliotibial band syndrome and patellofemoral pain syndrome.13,26,28,30,32 Distance runners need to be aware of potential injury risks and take preventive measures, such as using proper training techniques and incorporating them into their routines to evaluate body functions such as flexibility, stability, mobility, and strength.
Our author group 20 invented the KOJI AWARENESS (KA) self-screening test with 11 components to assess mobility, stability, and strength combinations. It is a practical self-evaluation tool that evaluates each body part's function without using specific equipment, and it is comparable in accuracy to the Functional Movement Screen (FMS), which was developed to monitor movement patterns and has been widely utilized in sports rehabilitation. 22 In our 2023 study, 20 we analyzed the reliability of the KA test and found high reproducibility (intraclass correlation coefficient [1.1], 0.876 [95% CI, 0.434-0.981]). The KA test showed a significant negative correlation between the test score and musculotendinous pain grade in regularly trained individuals. 21 Therefore, it effectively assesses body movements, and the scores may help develop individual conditioning plans to improve movement function.
If the association between preseason KA scores and in-season injury occurrence is clarified, athletes at high risk of injury can be identified based on their preseason KA scores, and preventive strategies for running injuries can be implemented in advance. However, the potential association between the KA score and the risk of running injuries in elite long-distance runners remains unexplored. Therefore, our study aimed to investigate whether the total KA score can be a predictive tool for injuries in this population. We hypothesized that the KA score is a reliable predictor of running injuries in elite long-distance runners.
Methods
Participants
Our prospective cohort study included male athletes from a single university men's track and field team who participated in the Tokyo-Hakone Round-Trip College Ekiden Race in January 2023. This is an esteemed long-distance relay race, with a total length of 217.1 km, that has been held annually for >100 years. It is widely recognized as one of Japan's most prestigious and challenging athletic events, attracting top collegiate teams nationwide. The exclusion criteria were athletes with (1) a severe psychiatric, neurological, or cardiovascular disease; (2) an orthopaedic disorder; and (3) an acute infectious disease. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (October 2000) for medical research involving human participants, and the study protocol was approved by the research ethics committee of our institution.
The KA screening test was administered to the included participants in June 2022 before they participated in the preseason preparation for the Tokyo-Hakone Round-Trip College Ekiden Race. All participants were asked about their physical attributes (height, weight, sex, and age), medical history, sports history, sports level, and daily activity level in a questionnaire before taking the KA test. The athletes were instructed to stop if they experienced pain during the test. However, none withdrew from the study because of injury or discomfort throughout the entire study duration.
Descriptive data—including age, height, weight, and body mass index—were obtained through interviews. The participants were also asked whether they had sustained a running injury for >3 weeks in the past.2,16 The participants were monitored for 6 months to record any inability to participate in training due to their physical condition.
KA Screening Test
The KA screening test consists of 11 components—including neck mobility, shoulder mobility, scapular mobility, thoracic spine mobility, upper extremity stability and strength, hip mobility, hip and spine mobility, upper and lower extremity mobility and stability, midsection stability strength, lower extremity strength, and ankle mobility—to assess combinations of mobility, stability, and strength20-22 without using specific equipment. Each test component has explicit scoring criteria, with a maximum total score of 50. Higher scores indicate better physical function. The KA screening test and scoring sheet are available separately as Supplemental Material.
Injury Surveillance
After the KA assessment, injury surveillance was conducted to monitor the incidence of running-related injuries over 6 months during the competitive season. The survey recorded the specific types of injuries and the corresponding number of days lost from training and competition. The calculation of days lost encompassed the period from the first day of absence to the participant's full return to training and competition. Athletic trainers managed injured athletes. Athletes visited the hospital for diagnosis when necessary. After injury, medical treatment and rehabilitation were provided, and return to competition was determined based on medical information, physical function, and degree of performance. The team's dedicated athletic trainer meticulously tracked the presence of injury and the number of days lost. The athletic trainer fully understood the measurement protocol and conducted the injury surveillance.
Definition of Running Injury and Group Classification
Participants were classified into 2 groups based on the presence or absence of running injuries during the season. Running injuries were defined as lower limb fatigue fractures, medial tibial stress syndrome, and tendinosis disorders that specifically occurred due to running.10,14,19,30 Participants who experienced running injuries resulting in an absence from training and competition for ≥3 weeks were classified into the running injury group.2,16
Statistical Analysis
Statistical analysis was performed to assess the normality of the variable distributions using histograms and the Shapiro-Wilk normality test. Descriptive statistics are presented as mean ± standard deviation for normally distributed variables and median (interquartile range [IQR]) for nonnormally distributed variables. Group differences in participant characteristics and KA scores based on the presence or absence of running injuries were analyzed using the Mann-Whitney U test. The Fisher exact test was performed to analyze the association between the presence or absence of a history of running injury among the groups. Receiver operating characteristic (ROC) curves were generated to determine the optimal cutoff value of the KA score, maximizing sensitivity and specificity for predicting running injuries. The predictive ability of the KA score was evaluated using the area under the ROC curve (AUC), with AUC values categorized as high (0.9-1), moderate (0.7-0.9), or low (0.5-0.7) accuracy. 9 The optimal cutoff value was determined using the Youden index 1 (sensitivity+specificity) − 1. The risk ratio was calculated using the chi-square test. SPSS Statistics 27 (IBM) was used for all statistical analyses, with a significance level set at P < .05.
Results
A total of 47 runners were included in the analysis (Figure 1). Of these runners, 10 athletes sustained an injury within the 6-month study period, for an incidence rate of 21.3%, and were included in the injury group. The remaining 37 athletes comprised the noninjury group. No significant differences were found between participants in the injury versus the noninjury group in the descriptive data (Table 1). Details regarding the specific types and distribution of running injuries and the number of days lost because of these injuries in the injury group are shown in Table 2. None of the 10 runners in the injury group required surgical intervention.
Figure 1.
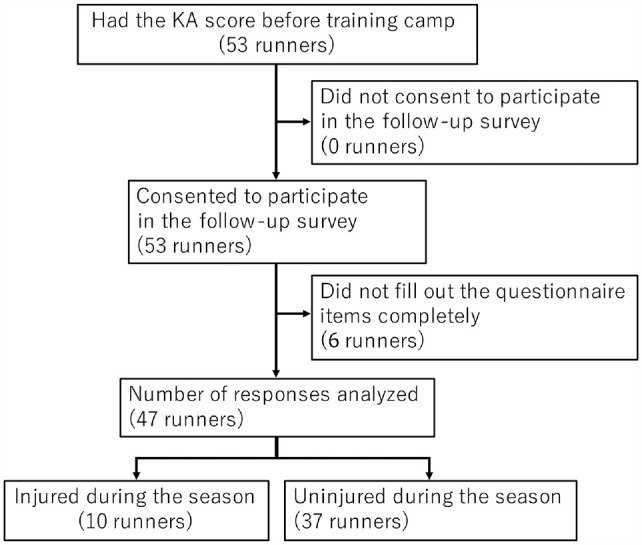
Flowchart illustrating the procedures of this study. KA, KOJI AWARENESS.
Table 1.
Characteristics of the Study Cohort Overall and in Each Group a
| Overall (N = 47) | Injury Group (n = 10) | Noninjury Group (n = 37) | P | |
|---|---|---|---|---|
| Age, y | 19.8 ± 1.2 (18.0-21) |
19.8 ± 1.6 (18-21) |
19.8 ± 1.3 (18-22) |
.870 |
| Height, cm | 172.7 ± 5.6 (161-187) |
170.3 ± 5 (163-178) |
173.2 ± 4.6 (161-187) |
.194 |
| Weight, kg | 55.8 ± 4.4 (45-65) |
54.8 ± 3.7 (48-60) |
56.0 ± 4.6 (45-65) |
.523 |
| BMI, kg/m2 | 18.7 ± 0.8 (16.8-21) |
18.9 ± 0.7 (17.7-20.1) |
18.6 ± 0.9 (16.8-21) |
.438 |
| History of running injury, n (%) | 35 (74.5) | 6 (60) | 29 (78.4) | .714 |
Data are presented as mean ± SD (range) unless otherwise indicated. BMI, body mass index.
Table 2.
Types of Running Injuries and Competition and Training Time Lost in the Injury Group (n = 10) a
| Type of Running Injury | n | Competition and Training Time Lost, Days |
|---|---|---|
| Femoral stress fracture | 3 | 79 (53-119) |
| Medial tibial stress syndrome | 3 | 45 (23-49) |
| Iliotibial band friction syndrome | 2 | 46 (36-56) |
| Achilles tendinitis | 1 | 50 |
| Plantar fasciitis | 1 | 67 |
| All | 10 | 51.5 (23-119) |
Data are presented as median (range).
In the injury group, the number of participants with reduced scores according to the KA component was as follows: neck mobility (n = 5), shoulder mobility (n = 2), scapular mobility (n = 4), thoracic spine mobility (n = 6), hip mobility (n = 1), hip and spine mobility (n = 4), upper and lower extremity mobility and stability (n = 2), lower extremity strength (n = 2), and ankle mobility (n = 2). There were no problems regarding upper extremity stability and strength or regarding midsection stability strength. The KA score was significantly lower in the injury group versus the noninjury group (median, 44.5 [IQR, 43-46.8] vs median, 48 [IQR, 46-50], respectively; P = .009) (Figure 2).
Figure 2.
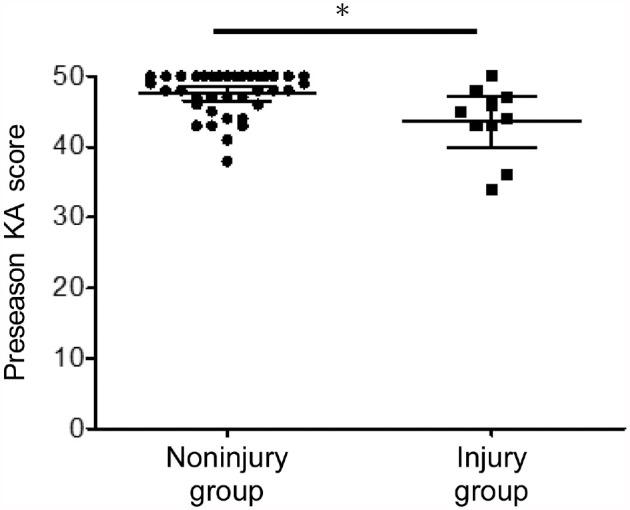
Preseason KA scores in the injury and noninjury groups. The middle line indicates the median and the top and bottom lines indicate the interquartile range. *Statistically significant difference between groups (P < .05). KA, KOJI AWARENESS.
ROC curve analysis yielded an AUC of 0.764, indicating moderate accuracy in predicting running injuries (Figure 3 and Table 3). The sensitivity and specificity of the KA score for predicting running injuries were 73% and 63.6%, respectively (Table 3). The cutoff value for the KA score to predict running injuries was 46.5 (Table 3). The chi-square test revealed a risk ratio of 2.590 (95% CI, 1.329-5.047) for participants with a KA score below the cutoff value, indicating a higher risk of running injuries (Table 3). Of the players with a KA score of ≥46.5 (n = 30), 3 players (10%) were injured, whereas of the players with a score of <46.5 (n = 17), 7 players (41.2%) were injured.
Figure 3.
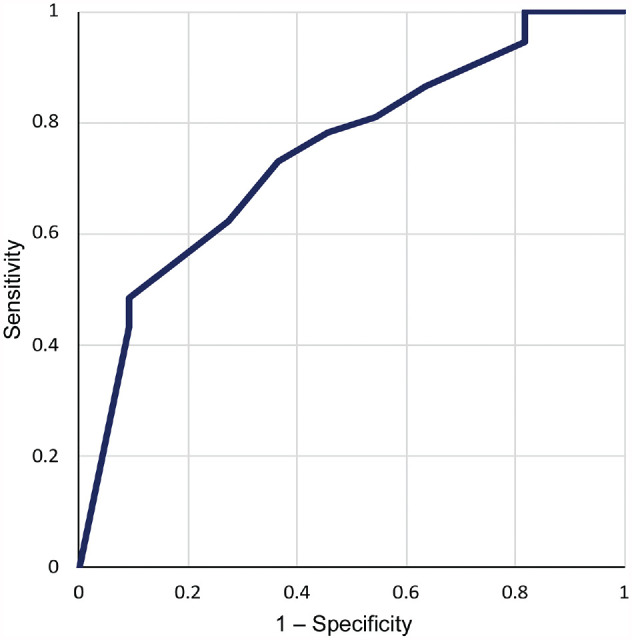
The receiver operator characteristic curve was used to evaluate the ability of the KOJI AWARENESS score to predict running injuries.
Table 3.
Ability of the KOJI AWARENESS Score to Predict Running Injury in Elite Long-Distance Runners a
| Parameter | Value |
|---|---|
| Cutoff score | 46.5 |
| AUC (95% CI) | 0.764 (0.600-0.930) |
| Sensitivity, % | 73 |
| Specificity, % | 63.6 |
| Risk ratio for KA score ≤46 (95% CI) | 2.590 (1.329-5.047) |
AUC, area under the receiver operating characteristic curve; KA, KOJI AWARENESS.
Discussion
In this study, we found that the running injury incidence rate during the season was 21.3%, and the running-injury group exhibited significantly lower KA scores than the noninjury group. Furthermore, the preseason KA scores predicted the incidence of running injuries during the season with a sensitivity of 73% and a specificity of 63.6%. Additionally, the cutoff value for the KA score to predict running injuries was determined to be 46.5, with a risk ratio of 2.590. These findings support our study hypothesis and provide new insights into the possible utilization of the preseason KA score for predicting the incidence of running injuries during the season.
The incidence of running injuries reported in the present study (21.3%) was lower than that of running injuries during the season reported in a previous study by Baltich et al 3 (40%). The difference in incidence rates may be attributed to differences in the competition level of the study cohort and the definition of running injury. We included elite collegiate runners and defined running injuries as lower limb injuries—including tendon and stress fractures—resulting in an inability to train or compete for >3 weeks. In contrast, Baltich et al included novice runners and defined running injuries as impairments restricting running for ≥1 week. The median number of days missed because of running injuries during the season, which was 50 days in this study, highlights the need for prolonged treatment and emphasizes the importance of preventing running injuries in long-distance male runners.
The running-injury group in this study showed significantly lower KA scores compared with the noninjury group. Factors contributing to the incidence of running injuries included reduced ankle mobility, decreased core stability, and lower extremity muscle weakness, which have been reported in previous studies.6,7,11,24,25,28,32 It has also been reported that decreased upper extremity function can contribute to running injuries because arm swinging is associated with propulsion during running. 27 These findings suggest that an overall functional decline may be associated with the incidence of running injuries.
A report by Hreljac 13 showed that deep-squat and active straight-leg-raise scores on the FMS effectively predict the risk of running injury, while the FMS composite score did not predict this risk in male athletes. In contrast, the KA test can predict this risk with a total score. The differences in the evaluation items between the FMS and KA likely influence the results. Overall, this study revealed novel findings that the total KA score, which assesses overall body function, can predict the incidence of running injuries.
This study showed that athletes with a preseason KA score <46.5 have a higher risk of experiencing running injuries during the season. This association between low KA scores, musculoskeletal issues, and pain severity highlights the relevance of the KA test as a valuable tool for self-assessment without needing specialized devices. 21 Furthermore, the confirmed validity of the KA score, as evidenced by its correlation with the evaluations conducted by specialized staff, emphasizes its reliability.20,22
Clinical Implications
The findings underscore the importance of incorporating the KA test into preseason evaluations to identify athletes at risk of running injuries. By identifying high-risk athletes based on their KA scores, proactive interventions can be implemented to improve musculoskeletal function and prevent injury. Moreover, the ability of the KA score to improve with corrective exercises further supports its potential as a modifiable intervention variable. 20 In our previous study, 20 we instructed athletes to perform corrective exercises on the areas with decreased scores in the KA test and analyzed changes in pain and KA scores. The results showed that corrective exercises increased the KA score and reduced pain. The incidence of running injuries may be effectively reduced by assessing the risk of running injuries based on the KA preseason score and implementing targeted preventive measures, such as corrective exercises, for those at high risk.
Limitations
Our study had several limitations. First, the sample size was small (n = 47 participants). This study included runners from a single university; thus, caution must be exercised in generalizing the results. Additional studies with more participants are required to draw a robust conclusion. Second, the study focused only on male athletes from a top-level university team in Japan, which limits the generalizability of the findings to female athletes, different age groups, and athletes of different competitive levels and disciplines. Third, results may differ depending on the definition of injury. The definition of injury used in this study was a lower extremity running injury that resulted in a longer than 3-week break from running. Previous reports defined injury as lasting ≥1 week; thus, results depend on the definition. 3 However, since lower extremity running injury lasting for >3 weeks significantly reduces physical function and performance, the results of this study are important because they suggest that the KA score predicts running injury that forces long-term withdrawal from running. Therefore, future studies should aim to increase the sample size and expand the range of sports disciplines and competitions. Furthermore, the relationship between the KA scores and specific injury types was investigated to enhance injury prevention strategies. Nonetheless, this study provides important findings using a prospective cohort analysis targeting elite male runners and demonstrating that the KA test can predict the risk of running injuries.
Conclusion
The KA preseason score was able to predict running-related injuries during the season. Specifically, athletes with KA scores ≤46.5 had a higher risk of experiencing running-related injuries. Incorporating KA assessments into training programs may help identify high-risk athletes so that preventive measures can be implemented.
Supplemental Material
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241260517 for Predictive Value of the KOJI AWARENESS Self-Evaluation System for Running Injuries in Elite Male Long-Distance Runners: A Prospective Cohort Study by Koji Murofushi, Sho Mitomo, Kenji Hirohata, Hidetaka Furuya, Hiroki Katagiri, Koji Kaneoka, Susumu Hara and Kazuyoshi Yagishita in Orthopaedic Journal of Sports Medicine
Acknowledgments
The authors express their sincere appreciation to the participants of this study for their time and commitment. Their involvement was invaluable in making this research possible. They also thank the coaching staff and medical personnel of Aoyama Gakuin University as well as the men's track and field team for its cooperation and assistance throughout the data-collection process.
Footnotes
Final revision submitted December 7, 2023; accepted January 10, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tokyo Medical and Dental University (ref No. M2021-350-01).
Supplemental material: Supplemental Material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671241260517#supplementary-materials
References
- 1. Akobeng AK. Understanding diagnostic tests 3: receiver operating characteristic curves. Acta Paediatr. 2007;96(5):644-647. [DOI] [PubMed] [Google Scholar]
- 2. Akoto R, Lambert C, Balke M, Bouillon B, Frosch KH, Höher J. Epidemiology of injuries in judo: a cross-sectional survey of severe injuries based on time loss and reduction in sporting level. Br J Sports Med. 2018;52(17):1109-1115. [DOI] [PubMed] [Google Scholar]
- 3. Baltich J, Emery CA, Whittaker JL, Nigg BM. Running injuries in novice runners enrolled in different training interventions: a pilot randomized controlled trial. Scand J Med Sci Sports. 2017;27(11):1372-1383. [DOI] [PubMed] [Google Scholar]
- 4. Bonet JB, Javierre C, Guimarães JT, et al. Benefits on hematological and biochemical parameters of a high-intensity interval training program for a half-marathon in recreational middle-aged women runners. Int J Environ Res Public Health. 2022;19(1):498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Buist I, Bredeweg SW, Lemmink KA, van Mechelen W, Diercks RL. Predictors of running-related injuries in novice runners enrolled in a systematic training program: a prospective cohort study. Am J Sports Med. 2010;38(2):273-280. [DOI] [PubMed] [Google Scholar]
- 6. Clement DB, Taunton JE, Smart GW. Achilles tendinitis and peritendinitis: etiology and treatment. Am J Sports Med. 1984;12(3):179-184. [DOI] [PubMed] [Google Scholar]
- 7. Dierks TA, Manal KT, Hamill J, Davis IS. Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. J Orthop Sports Phys Ther. 2008;38(8):448-456. [DOI] [PubMed] [Google Scholar]
- 8. Ferber R, Hreljac A, Kendall KD. Suspected mechanisms in the cause of overuse running injuries: a clinical review. Sports Health. 2009;1(3):242-246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Fischer JE, Bachmann LM, Jaeschke R. A readers’ guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med. 2003;29(7):1043-1051. [DOI] [PubMed] [Google Scholar]
- 10. Francis P, Whatman C, Sheerin K, et al. The proportion of lower limb running injuries by gender, anatomical location and specific pathology: a systematic review. J Sports Sci Med. 2019;18(1):21-31. [PMC free article] [PubMed] [Google Scholar]
- 11. Geraci MC, Brown W. Evidence-based treatment of hip and pelvic injuries in runners. Phys Med Rehabil Clin N Am. 2005;16(3):711-747. [DOI] [PubMed] [Google Scholar]
- 12. Hotta T, Nishiguchi S, Fukutani N, et al. Functional movement screen for predicting running injuries in 18- to 24-year-old competitive male runners. J Strength Cond Res. 2015;29(10):2808-2815. [DOI] [PubMed] [Google Scholar]
- 13. Hreljac A. Impact and overuse injuries in runners. Med Sci Sports Exerc. 2004;36(5):845-849. [DOI] [PubMed] [Google Scholar]
- 14. Kakouris N, Yener N, Fong DTP. A systematic review of running-related musculoskeletal injuries in runners. J Sport Health Sci. 2021;10(5):513-522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kluitenberg B, van Middelkoop M, Diercks R, van der Worp H. What are the differences in injury proportions between different populations of runners? A systematic review and meta-analysis. Sports Med. 2015;45(8):1143-1161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Lambert C, Reinert N, Stahl L, et al. Epidemiology of injuries in track and field athletes: a cross-sectional study of specific injuries based on time loss and reduction in sporting level. Phys Sportsmed. 2022;50(1):20-29. [DOI] [PubMed] [Google Scholar]
- 17. Leyk D, Erley O, Gorges W, et al. Performance, training and lifestyle parameters of marathon runners aged 20-80 years: results of the PACE-study. Int J Sports Med. 2009;30(5):360-365. [DOI] [PubMed] [Google Scholar]
- 18. Lopes AD, Hespanhol Júnior LC, Yeung SS, Costa LO. What are the main running-related musculoskeletal injuries? A systematic review. Sports Med. 2012;42(10):891-905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Mucha MD, Caldwell W, Schlueter EL, Walters C, Hassen A. Hip abductor strength and lower extremity running related injury in distance runners: a systematic review. J Sci Med Sport. 2017;20(4):349-355. [DOI] [PubMed] [Google Scholar]
- 20. Murofushi K, Yamaguchi D, Kaneoka K, et al. The effectiveness of corrective exercises on the KOJI AWARENESS score and activity-related pain intensity. J Med Invest. 2023;70(1.2):208-212. [DOI] [PubMed] [Google Scholar]
- 21. Murofushi K, Yamaguchi D, Katagiri H, et al. The relationship between movement self-screening scores and pain intensity during daily training. J Med Invest. 2022;69(3.4):204-216. [DOI] [PubMed] [Google Scholar]
- 22. Murofushi K, Yamaguchi D, Katagiri H, et al. Validity of the KOJI AWARENESS self-screening test for body movement and comparison with functional movement screening. PLoS One. 2022;17(12):e0277167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Nikolaidis PT, Knechtle B. Participation and performance characteristics in half-marathon run: a brief narrative review. J Muscle Res Cell Motil. 2023;44(2):115-122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am. 2003;85(5):872-877. [DOI] [PubMed] [Google Scholar]
- 25. Saeterbakken AH, Andersen V, Behm DG, et al. The role of trunk training for physical fitness and sport-specific performance. Protocol for a meta-analysis. Front Sports Act Living. 2021;3:625098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Saragiotto BT, Yamato TP, Hespanhol Junior LC, Rainbow MJ, Davis IS, Lopes AD. What are the main risk factors for running-related injuries? Sports Med. 2014;44(8):1153-1163. [DOI] [PubMed] [Google Scholar]
- 27. Simoni L, Pancani S, Vannetti F, Macchi C, Pasquini G. Relationship between lower limb kinematics and upper trunk acceleration in recreational runners. J Healthc Eng. 2020;2020:8973010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: a theoretical model. J Orthop Sports Phys Ther. 1987;9(4):160-165. [DOI] [PubMed] [Google Scholar]
- 29. van der Worp MP, ten Haaf DS, van Cingel R, de Wijer A, Nijhuis-van der Sanden MW, Staal JB. Injuries in runners; a systematic review on risk factors and sex differences. PLoS One. 2015;10(2):e0114937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW. Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med. 2007;41(8):469-480; discussion 480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. van Poppel D, van der Worp M, Slabbekoorn A, et al. Risk factors for overuse injuries in short- and long-distance running: a systematic review. J Sport Health Sci. 2021;10:14-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Winkelmann ZK, Anderson D, Games KE, Eberman LE. Risk factors for medial tibial stress syndrome in active individuals: an evidence-based review. J Athl Train. 2016;51(12):1049-1052. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241260517 for Predictive Value of the KOJI AWARENESS Self-Evaluation System for Running Injuries in Elite Male Long-Distance Runners: A Prospective Cohort Study by Koji Murofushi, Sho Mitomo, Kenji Hirohata, Hidetaka Furuya, Hiroki Katagiri, Koji Kaneoka, Susumu Hara and Kazuyoshi Yagishita in Orthopaedic Journal of Sports Medicine