

Abstract
Objective:
To study the effects of transcutaneous electrical acupoint stimulation (TEAS) on length of stay (LOS) and hospitalization costs in postoperative inpatients.
Methods:
Two researchers collectively searched PubMed, Embase, Cochrane Library, China Network Knowledge Infrastructure, and Wanfang Database. The search time was set from the beginning to 25 April 2023, to identify randomized controlled trials articles that met the criteria. Statistical analyses were performed using the Stata software (version 16.0). The risk of bias was assessed using the Cochrane risk-of-bias tool, and publication bias was evaluated using a funnel plot and Egger’s test. The quality of evidence was assessed according to the Grading of Recommendations Assessment, Development, and Evaluation approach.
Results:
Thirty-four randomized controlled trials were included. The main results showed that TEAS reduced hospitalization costs [standardized mean difference (SMD)=−1.92; 95% CI: −3.40, −0.43), LOS (SMD=−1.00; 95% CI: −1.30, −0.70) and postoperative LOS (SMD=−0.70; 95% CI: −0.91, −0.49] in postoperative patients. Subgroup analyses further revealed that TEAS was effective in reducing both the overall and postoperative LOS in patients undergoing multiple surgical procedures. It is worth noting that the observed heterogeneity in the results may be attributed to variations in surgical procedures, stimulation frequencies, and stimulation points utilized in different trials.
Conclusions:
TEAS can help postoperative patients reduce their LOS and hospitalization cost. However, considering the bias identified and heterogeneity, the results of this review should be interpreted with caution.
Keywords: hospitalization costs, length of stay, meta-analysis, perioperative management, systematic review, transcutaneous electrical acupoint stimulation
Introduction
Highlights
Transcutaneous electrical acupoint stimulation (TEAS) can reduce hospitalization costs.
TEAS can reduce postoperative length of stay.
TEAS can reduce length of stay.
Transcutaneous electrical acupoint stimulation (TEAS) is a noninvasive treatment method that involves the application of electrodes to specific acupoints on the patient’s skin1. The purpose of this technique is to deliver electrical stimulation at a predetermined intensity comparable to that of conventional electro-acupuncture1. TEAS has increasingly gained recognition in clinical settings and is now considered an essential component of perioperative management, primarily due to its lack of drug-related side effects and noninvasive characteristics2.
In recent years, there has been a surge in studies across various medical departments aimed at exploring the potential of TEAS to enhance the recovery of postoperative patients3–6. Research findings indicate that TEAS can facilitate postoperative recovery in various ways, including pain relief, regulation of gastrointestinal function, reduction of inflammation, management of stress, and prevention of postoperative cognitive dysfunction7. The length of stay (LOS) and hospitalization costs are crucial indicators for evaluating patients’ postoperative recovery3,8,9. Considering the increasing influence of LOS and hospitalization costs on the decision-making of both physicians and patients, especially in China where there is a significant conflict between rising healthcare demands and limited resources, it is essential to understand the economic value of perioperative TEAS for inpatients who have undergone surgery10. The impact of TEAS on LOS and hospitalization costs for postoperative inpatients is yet to be clearly elucidated3,11–13. To date, there has been a lack of systematic reviews or meta-analyses that specifically explore the influence of TEAS on postoperative hospitalization, with LOS and hospitalization costs as the primary outcome measures.
Thus, the objective of this review was to assess and analyze the effects of TEAS on LOS and hospitalization costs among postoperative inpatients, with the aim of offering guidance for clinical application and future research endeavors.
Materials and methods
Study design and protocol
The work has been reported in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMAP) (SDC, Table 1, Supplemental Digital Content 1, http://links.lww.com/JS9/C606, Supplemental Digital Content 2, http://links.lww.com/JS9/C607) and Assessing the methodological quality of systematic reviews (AMSTAR, Supplemental Digital Content 3, http://links.lww.com/JS9/C608) Guidelines14,15. Prior to data extraction, we registered our review in the PROSPERO database.
Search strategy
Two independent researchers conducted a thorough literature search to ensure the inclusion of as many relevant studies as possible. The following electronic databases were searched: PubMed, Embase, Cochrane Library, China Network Knowledge Infrastructure (CNKI), and Wanfang Database. The search terms included transcutaneous electrical acupoint stimulation, transcutaneous acupoint electrical stimulation, TEAS, hospital stay, length of stay, length of hospitalization, hospitalization time, hospitalization costs, and hospitalization expenses. The search covered all relevant studies from the inception of the databases to 25 April 2023. In addition, we reviewed the references of the selected studies to identify any potential additional relevant studies. For the retrieval strategy, a combination of medical subject heading (MeSH) terms and free words was used. The complete search strategy used for each database is shown in Table S2.
Inclusion criteria
Only prospective randomized controlled trials (RCTs) and peer-reviewed articles were eligible for inclusion in this meta-analysis. The participants included in the studies had to be inpatients who had recently undergone surgery without any restrictions based on age, sex, or nationality. For an RCT to be considered, it had to contain both a study group and a control group and provide quantifiable outcome indicators such as LOS, postoperative LOS, and hospitalization costs. In cases where multiple studies reported the same topic, only the most recent publication was included in the meta-analysis.
Exclusion criteria
The following types of articles were excluded from the analysis: reviews, case reports, and nonrandomized controlled trials (non-RCTs). Articles were excluded if they did not provide a description of TEAS or measurable outcome indicators. Studies that explored different forms of acupuncture, such as acupoint injection, suture embedding, transcutaneous electrical nerve stimulation, acupuncture combined with oral Chinese medicine, and other nonacupuncture-related therapies, were also excluded.
Article screening and data extraction
The identified articles were screened by two reviewers, who evaluated them based on predetermined inclusion and exclusion criteria. Full-text versions of articles that met the criteria were obtained. Data from the selected articles were extracted and entered into a predefined spreadsheet. The extracted data included information such as author, publication year, sample size, type of surgery, acupoint selection, timing of the stimulus, frequency of the stimulus, and magnitude of the stimulus current, among other relevant details. In case of any discrepancies or disagreements between the reviewers, a third reviewer was consulted to resolve them.
Quality assessment
Two reviewers independently utilized the Cochrane tool to evaluate articles for their risk of bias (RoB), and assessed the quality of the studies using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) methodology. In cases where there were discrepancies between the assessments of the two reviewers, a third reviewer was consulted to effectively address and resolve any disagreement.
Statistical analysis
A random-effects meta-analysis was used to compute the standardized mean difference (SMD) in LOS, postoperative LOS, and hospitalization cost estimates. Subgroup analysis was carried out to analyze the different effects of TEAS on the common types of surgeries, including gastrointestinal surgery, lung surgery, orthopedic surgery, urological surgery, gynecological surgery, endoscopic surgery, and surgery for the elderly.
I 2 statistics and the Cochrane Q test were used to examine the heterogeneity among the effect estimates. The heterogeneity of the pooled estimates with P<0.10 (Cochrane Q test) was deemed significant. I 2 statistics of 0–25%, 25–50%, and >50% indicated low, moderate, and high heterogeneity, respectively. Funnel plots and Egger’s test were used to evaluate potential publication bias and the Trim and Fill method was used to examine the sensitivity of the results to publication bias. Sensitivity analyses were performed to separate studies by stimulus acupoints, stimulus frequency, and quality. We further examined the influence of individual estimates on pooled RRs using leave-one-out analysis. Statistical analyses were performed using the Stata software (version 16.0).
Results
Search and study selection results
A total of 192 studies were identified using five databases. After removing replicates, 123 potentially relevant studies were identified. A total of 87 studies were excluded after reading the titles and abstracts. The full-text of the remaining 36 studies was assessed, and 2 studies were excluded according to the inclusion or exclusion criteria. Finally, 34 studies were included in the meta-analysis5,6,9,11–13,16–43. The detailed process is illustrated in Figure 1.
Figure 1.
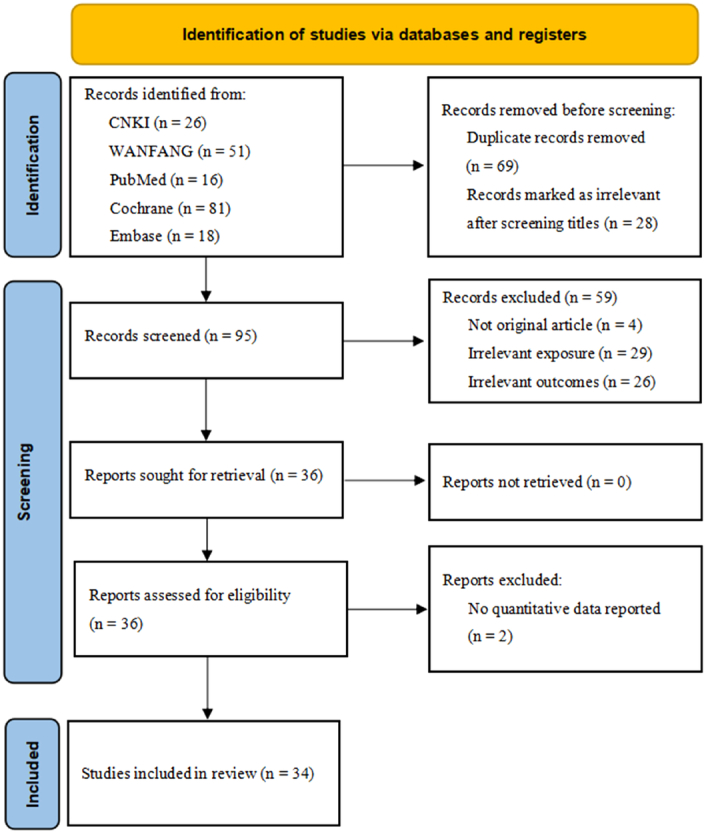
Flow chart of literature screening.
Study characteristic
The included studies were published from 2015 to 2023 and included 26 (76.5%) articles from the last 5 years. A total of 2980 patients were included in the study, including 1500 in the TEAS group and 1480 in the control group. These studies included 14 gastrointestinal surgeries, 6 gynecological surgeries, 6 lung surgeries, 3 orthopedic surgeries, 2 urological surgeries, and 1 cardiovascular surgery. In addition, two studies involved multiple surgical systems. The specific characteristics of the included studies are presented in Table 1.
Table 1.
Basic characteristics of the study articles.
| TEAS group | Control group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID | Type of surgery | Sample size | Age | Sex(Male/Female) | Sample size | Age | Sex(Male/Female) | Acupoint selections | Stimulus timing (Pr/In/Po) | Stimulus frequency | Stimulus current magnitude | GRADE |
| Chen et al., 202116 | Gastrointestinal surgery | 36 | 45.36±5.21 | 21/15 | 36 | 47.13±5.24 | 20/16 | Zusanli(ST36) + Neiguan(PC6) | Pr + In + Po | 2/100 HZ | 8–12 mA | Moderate |
| Deng et al., 201917 | Urological surgery | 30 | 40.5±6.4 | 0/30 | 30 | 39.4±7.4 | 0/30 | Zusanli (ST36) + Sanyinjiao (SP6) + Neiguan (PC6) + Hegu (LI4) | Pr + Po | 2 HZ | a | Moderate |
| Du, 201518 | Lung surgery | 46 | 56.2±12.6 | 21/25 | 44 | 55.9±13.5 | 23/21 | Neiguan (PC6) + Hegu (LI4) | Pr + In + Po | 2/100 HZ | 15–25 mA | Moderate |
| Ge et al., 202119 | Orthopedic surgery | 42 | 72.5±6.8 | 22/20 | 42 | 73.2±7.2 | 23/19 | Neimadian (Extra) + Zusanli (ST36) + Yanglingquan (GB34) + Xuehai (SP10) + Yinlingquan (SP9) | Po | 2/100 HZ | 15–25 mA | Moderate |
| Li et al., 202020 | Gynecological surgery | 60 | 53.4±11.6 | 0/60 | 60 | 52.8±13.7 | 0/60 | Hegu (LI4) + Neiguan (PC6) + Sanyinjiao (SP6) | Po | 2/100 HZ | a | Moderate |
| Lin et al., 202021 | Gynecological surgery | 30 | 38.30±7.9 | 0/30 | 30 | 35.23±7.8 | 0/30 | Neiguan (PC6) + Hegu (LI4) + Zusanli (ST36) + Sanyinjiao (SP6) | Pr + Po | 2/100 HZ | a | Moderate |
| Zhao et al., 202013 | Gastrointestinal surgery | 63 | 63.1 ± 8.1 | 48/15 | 49 | 62.3 ± 7.2 | 39/10 | Feiyu (BL13) + Hegu (LI4) + Zusanli (ST36) | Pr | 100 HZ | 20–25 mA | Moderate |
| Liu et al., 202022 | Gastrointestinal surgery | 30 | 51.2±5.0 | 18/12 | 30 | 51.0±5.2 | 20/10 | Hegu (LI4) + Laogong (PC8) + Zusanli (ST36) | Pr + In + Po | 2/100 HZ | 8-10 mA | Moderate |
| Lv et al., 202223 | Multiple operations | 52 | 37.17±10.59 | 0/52 | 51 | 34.63±9.03 | 0/51 | Neiguan (PC6) + Zusanli (ST36) | Po | 2/100 HZ | 6–9 mA | Moderate |
| Sun et al., 202024 | Gynecological surgery | 39 | 23.4±2.8 | 0/39 | 39 | 24.2±3.5 | 0/39 | Hegu (LI4) + Neiguan (PC6) | Pr + In | 2/15 HZ | 10–30 mA | Moderate |
| Tang et al., 202025 | Gastrointestinal surgery | 30 | 52.5±2.5 | 17/13 | 30 | 52.1±2.3 | 16/14 | Zusanli (ST36) + Shangjuxu (ST37) + Xiajuxu (ST39) + Neiguan (PC6) | Pr + In | 2/100 HZ | a | Moderate |
| Wang et al., 202127 | Lung surgery | 40 | 67.6±7.6 | 24/16 | 40 | 67.0±7.2 | 26/14 | Neiguan (PC6) + Hegu (LI4) | Pr + In | 2/100 HZ | 6–10 mA | Moderate |
| Wang et al., 202127 | Gynecological surgery | 40 | 67.5±7.4 | 0/40 | 40 | 67.1±7.0 | 0/40 | Neiguan (PC6) + Hegu (LI4) | Pr + In | 2/100 HZ | 6 mA | Moderate |
| Kong et al., 201928 | Lung surgery | 25 | 56±11 | Unknown | 25 | 53±10 | Unknown | Hegu (LI4) + Neiguan (PC6) + Houxi (SI3) + Zhigou (TE6) | Pr + In | 2/100 HZ | 6–12 mA | High |
| Yang et al., 201829 | Gastrointestinal surgery | 45 | 73.34±12.14 | 18/27 | 45 | 71.22±13.46 | 25/20 | Zusanli (ST36) + Shangjuxu (ST37) | Po | Unknown | Unknown | Moderate |
| Yuan et al., 201730 | Gastrointestinal surgery | 30 | 54.9±9.8 | 12/18 | 30 | 54.6±10.4 | 16/14 | Neiguan (PC6) + Hegu (LI4) + Zusanli (ST36) | Pr + In + Po | Unknown | a | High |
| Zhang et al., 201831 | Orthopedic surgery | 30 | 68±7 | 26/4 | 30 | 65±5 | 25/5 | Hegu (LI4) + Neiguan (PC6) | Pr + In | 2/100 HZ | a | Moderate |
| Duan et al., 202032 | Lung surgery | 30 | 66.5±4.3 | 23/7 | 30 | 67.0±3.8 | 22/8 | Neiguan (PC6) + Zhigou (TE6) + Houxi (SI3) | Pr + In | 2/100 HZ | 10–15 mA | High |
| Wang et al., 201733 | Gastrointestinal surgery | 30 | 69.1±4.5 | 17/13 | 30 | 68.5±2.1 | 18/12 | Zusanli (ST36) + Hegu (LI4) + Feiyu (BL13) | Pr + In | 2/100 HZ | 8–12 mA | Moderate |
| Wei et al., 201934 | Gastrointestinal surgery | 52 | Unknown | Unknown | 52 | Unknown | Unknown | Hegu (LI4) + Quchi (LI11) + Neiting (ST44) + Zusanli (ST36) | Po | 20 HZ | Unknown | High |
| Wu et al., 202235 | Orthopedic surgery | 44 | 56±8 | Unknown | 40 | 56±8 | Unknown | Zusanli (ST36) + Sanyinjiao (SP6) | Pr + In + Po | 2/15 HZ | Unknown | Moderate |
| Yang et al., 202036 | Cardiovascular surgery | 50 | 6.9±2.4 | 31/19 | 50 | 7.3±2.2 | 32/18 | Baihui (GV20) + Neiguan (PC6) + Hegu (LI4) + Ximen (PC4) | In | 2/100 HZ | 6 mA | Moderate |
| Wang et al., 202037 | Gastrointestinal surgery | 50 | 47±8 | 34/16 | 50 | 48±8 | 33/17 | Neiguan (PC6) + Hegu (LI4) | Pr + In | 2/100 HZ | 6–10 mA | Moderate |
| Huang et al., 201938 | Lung surgery | 20 | 47±15 | 11/9 | 20 | 45±14 | 10/10 | Feiyu (BL13) + Hegu (LI4) + Neiguan (PC6) | Pr + In | 2/100 HZ | 5–15 mA | Moderate |
| Wang et al., 202039 | Gastrointestinal surgery | 35 | 48±12 | 16/19 | 35 | 48±11 | 14/21 | Hegu (LI4) + Neiguan (PC6) | Pr + In | 2/100 HZ | a | Moderate |
| Li et al., 202340 | Multiple operations | 79 | 57±10 | 53/26 | 79 | 56±9 | 60/19 | Liangmen (ST21)+Daheng (SP15) | Po | 2–5 HZ | a | High |
| Mu et al., 201941 | Gynecological surgery | 55 | 24±3 | 0/55 | 55 | 24±3 | 0/55 | Zusanli (ST36) | Po | 30/60 HZ | 15–20 mA | Moderate |
| Fan et al., 201842 | Gastrointestinal surgery | 26 | 54±7 | 13/13 | 26 | 54±8 | 13/13 | Neiguan (PC6) + Hegu (LI4) + Zusanli (ST36) + Shangjuxu (SP6) + Xiajuxu (ST39) | Pr + In | 2/100 HZ | 3–8 mA | Moderate |
| Lu et al., 202243 | Gastrointestinal surgery | 47 | 56.2±9.0 | 26/21 | 47 | 55.6±9.9 | 23/24 | Neiguan (PC6) + Zusanli (ST36) | Pr + Po | 2/10 HZ | 4–11 mA | High |
| Tu et al., 20185 | Lung surgery | 72 | 64.34±8.25 | 42/30 | 72 | 62.88±8.37 | 39/33 | Feiyu (BL13) + Hegu (LI4) + Zusanli (ST36) | Pr + In | 2/100 HZ | 5–30 mA | High |
| Zhou et al., 20186 | Gynecological surgery | 43 | 32.2±3.5 | 0/43 | 45 | 30.6±3.9 | 0/45 | Zusanli (ST36) + Sanyinjiao (SP6) | Pr + Po | 2/10 HZ | 7–11 mA | High |
| Huang et al., 201938 | Gastrointestinal surgery | 29 | 58.59±11.27 | 12/17 | 28 | 60.57±12.1 | 17/11 | Zusanli (ST36) | Pr + In | 2/10 HZ | a | High |
| Li et al., 202111 | Gastrointestinal surgery | 140 | 60±13 | 85/55 | 140 | 62±12 | 96/44 | Hegu (LI4) + Neiguan (PC6) + Zusanli (ST36) + Shangjuxu (SP6) | Pr + In + Po | 2/100 HZ | a | High |
| Que et al., 202112 | Urological surgery | 30 | 45.4±18.7 | 18/12 | 30 | 47.1±16.3 | 19/11 | Shenyu (BL23) + Yinlingquan (SP9) + Hegu (LI4) + Neiguan (PC6) | Pr | 2/100 HZ | 5–30 mA | High |
The maximum intensity tolerated by the patient.
In, intraoperative; Po, postoperative; Pr, preoperative.
Synthesis of the results
Analysis of 19 studies with 1609 postoperative inpatients showed that the LOS was significantly lower in the TEAS group (n=813) than in the control group (n=796) (SMD=−1.00; 95% CI: −1.30, −0.70) (Fig. 2). Further subgroup analyses showed that TEAS reduced LOS for postoperative inpatients in gastrointestinal surgery, lung surgery, gynecological surgery, urological surgery, endoscopic surgery, and surgery in the elderly (Fig. 3A). Analysis of 15 studies with 1404 postoperative inpatients showed that postoperative LOS was significantly lower in the TEAS group (n=704) than in the control group (n=700) (SMD=−0.70; 95% CI: −0.91, −0.49) (Fig. 4). Further subgroup analyses showed that TEAS reduced the postoperative LOS for postoperative inpatients in gastrointestinal surgery, lung surgery, gynecological surgery, orthopedic surgery, endoscopic surgery, and surgery for the elderly (Fig. 3B). When analyzing four studies with 492 postoperative inpatients, it was found that hospitalization costs were significantly lower in the TEAS group (n=246) than in the control group (n=246) (SMD=−1.92; 95% CI: −3.40, −0.43) (Fig. 5).
Figure 2.
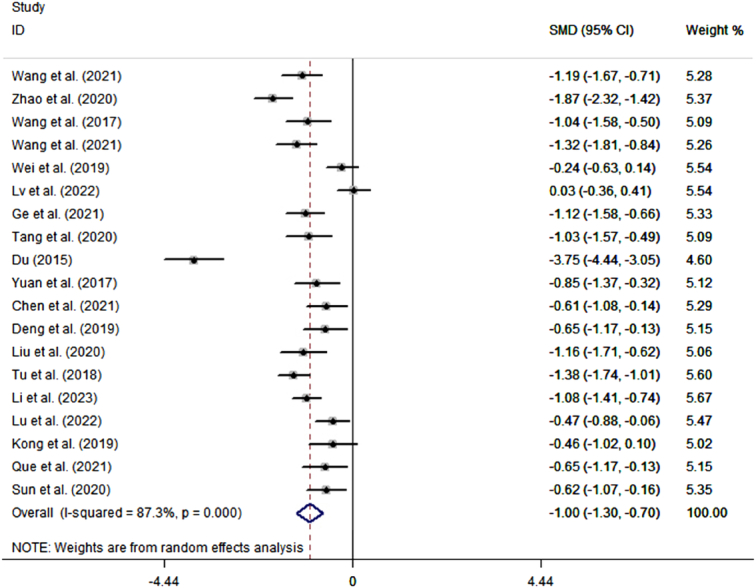
Forest plot of the length of stay.
Figure 3.

Effect of TEAS on length of stay and post-operative length of stay. Forest plot of subgroup analysis the effect of TEAS on length of stay (A) and post-operative length of stay (B).
Figure 4.
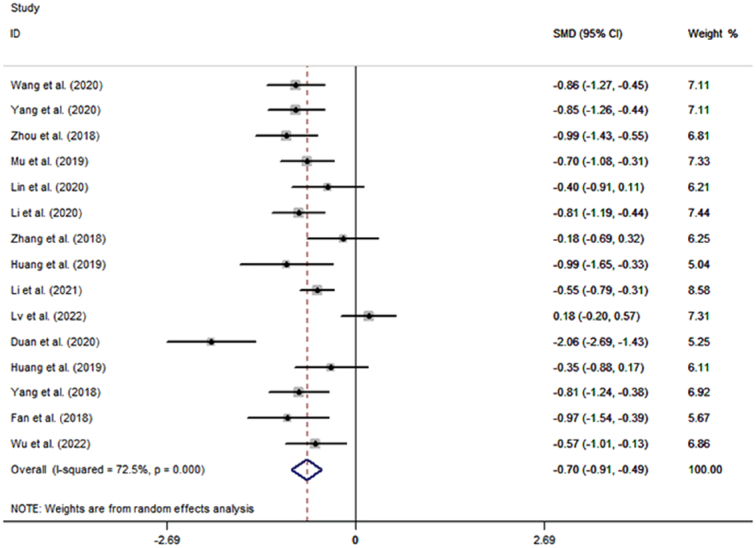
Forest plot of the postoperative length of stay.
Figure 5.
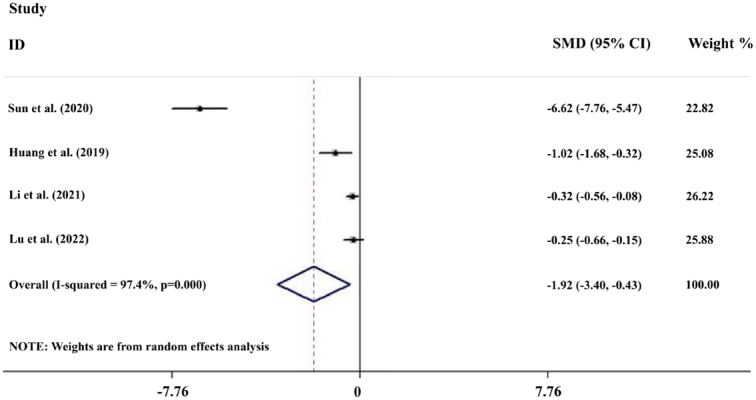
Forest plot of the hospitalization costs.
There was evidence of heterogeneity between the studies discussing the effect of TEAS on LOS (I 2=87.3%, P<0.001), postoperative LOS (I 2=72.5%, P<0.001), and hospitalization costs (I 2=97.4%, P<0.001) (Figs 2, 4, 5). To identify the source of the heterogeneity, we conducted a series of subgroup and sensitivity analyses. The leave-one-out analysis did not identify a single article as the source of heterogeneity in the estimated effects of TEAS on LOS and postoperative LOS (SDC, Fig. 1, Supplemental Digital Content 1, http://links.lww.com/JS9/C606, 2, Supplemental Digital Content 1, http://links.lww.com/JS9/C606). In the pool estimates of effect of TEAS on hospitalization costs, exclusion of the studies by Li et al. and Lu et al., respectively, rendered the results insignificant, indicating these two studies as significant sources of heterogeneity (SDC, Fig. 3, Supplemental Digital Content 1, http://links.lww.com/JS9/C606). However, meta-regression failed to identify any underlying causes of heterogeneity, considering the sample size of the studies. In the subgroup analyses of LOS, we found that heterogeneity was reduced in urological surgery and surgery in the elderly group (Fig. 3). By performing subgroup analyses of postoperative LOS, we found that heterogeneity was reduced in gastrointestinal, gynecological, and orthopedic surgeries (Fig. 3). Thus, the type of surgery was likely to be a source of heterogeneity. Moreover, a series of sensitivity analyses based on the stimulating frequency, acupoint, and quality of study showed that studies carried out TEAS with 2/100 HZ and Neiguanxue were the main sources of heterogeneity of the estimated effect of TEAS on the postoperative LOS (Tables 2 and 3). Additionally, sensitivity analyses carried out by the Trim and Fill method showed no significant differences, indicating the robustness of the results (SDC, Fig. 4, Supplemental Digital Content 1, http://links.lww.com/JS9/C606 and 5, Supplemental Digital Content 1, http://links.lww.com/JS9/C606).
Table 2.
Sensitivity analysis of the length of stay.
| n | RR | Lci | Uci | I2 | P | Eagger’s test | |
|---|---|---|---|---|---|---|---|
| Stimulation frequency | |||||||
| 100 Hz | 18 | −0.953 | −1.249 | −0.657 | 86.30% | <0.001 | 0.107 |
| 20 Hz | 18 | −1.480 | −1.352 | −0.744 | 86.80% | <0.001 | 0.208 |
| 2 Hz | 18 | −1.024 | −1.336 | −0.711 | 87.90% | <0.001 | 0.114 |
| 2/100 Hz | 8 | −0.803 | −1.158 | −0.449 | 80.70% | <0.001 | 0.936 |
| 2/15 Hz | 18 | −1.026 | −1.340 | −0.712 | 87.80% | <0.001 | 0.136 |
| 2/100 Hz | 17 | −1.058 | −1.386 | −0.730 | 88.20% | <0.001 | 0.145 |
| Unknown | 18 | −1.013 | −1.327 | −0.699 | 88.20% | <0.001 | 0.126 |
| Acupoint | |||||||
| Zusanli | 7 | −1.268 | −1.888 | −0.648 | 91.40% | <0.001 | 0.318 |
| Hegu | 6 | −0.705 | −1.089 | −0.322 | 79.50% | <0.001 | 0.877 |
| Neiguan | 7 | −1.123 | −1.500 | −0.746 | 81.60% | <0.001 | 0.739 |
| Feiyu | 16 | −0.921 | −1.246 | −0.596 | 87.00% | <0.001 | 0.036 |
| Sanyinjiao | 17 | −1.058 | −1.386 | −0.731 | 88.20% | <0.001 | 0.145 |
| Grade | |||||||
| Moderate | 7 | −0.746 | −1.075 | −0.418 | 75.60% | <0.001 | 0.366 |
| High | 12 | −1.172 | −1.624 | −0.719 | 90.20% | <0.001 | 0.009 |
Table 3.
Sensitivity analysis of the postoperative length of stay.
| n | RR | Lci | Uci | I 2 | P | Eagger’s test | |
|---|---|---|---|---|---|---|---|
| Stimulation frequency | |||||||
| 2/100 Hz | 6 | −0.642 | −0.793 | −0.491 | 0.00% | 0.430 | 0.589 |
| 2/15 HZ | 14 | −0.711 | −0.941 | −0.481 | 74.40% | <0.001 | 0.255 |
| 2/10 HZ | 12 | −0.724 | −0.997 | −0.451 | 76.40% | <0.001 | 0.174 |
| Acupoint | |||||||
| Zusanli | 6 | −0.928 | −1.328 | −0.528 | 76.20% | <0.001 | 0.421 |
| Hegu | 7 | −0.730 | −1.177 | −0.284 | 85.50% | <0.001 | 0.103 |
| Neiguan | 5 | −0.730 | −0.899 | −0.508 | 0.00% | 0.415 | 0.418 |
| Sanyinjiao | 11 | −0.706 | −0.991 | −0.422 | 78.60% | <0.001 | 0.264 |
| Shangjuxu | 12 | −0.693 | −0.970 | −0.415 | 77.40% | <0.001 | 0.290 |
| Grade | |||||||
| Moderate | 4 | −0.950 | −1.543 | −0.356 | 86.80% | <0.001 | 0.358 |
| High | 11 | −0.620 | −0.843 | −0.396 | 63.20% | <0.001 | 0.650 |
Risk of bias and study quality assessment
We assessed the RoB of the included studies and rated their study quality using the GRADE approach. The details of the RoB assessment and individual study assessment are shown in Figure 6. As for study quality assessment, 11 (32.4%) studies were rated as high and 23 (67.6%) were rated as moderate (Table 1). The Funnel plot and Egger’s test suggested that there was no evidence of publication bias in studies discussing the effects of TEAS on LOS, postoperative LOS, and hospital costs (SDC, Figs 6–8, Supplemental Digital Content 1, http://links.lww.com/JS9/C606, Supplemental Digital Content 4, http://links.lww.com/JS9/C609).
Figure 6.

Cochrane risk of bias assessment. Note: A. the risk of bias of each research. B. The risk of bias of all studies. ‘+’ represents low risk; ‘?’ represents unclear risk; ‘-’ represents high risk.
Discussion
TEAS combines the traditional Chinese acupuncture theory with modern electrical stimulation technology and is widely utilized in clinics because of its simplicity, stability, and safety44. However, previous research has predominantly focused on the clinical effectiveness of TEAS overlooking the significance of hospitalization costs and LOS as crucial factors for both patients and healthcare professionals2,10,45. LOS plays a significant role in determining healthcare expenses, and implementing efficient and secure discharge strategies can contribute to reducing financial burden46. Moreover, hospitalization costs directly impact inpatients, physician decision-making processes, and the overall economic strain on the nation46. Thus, reducing LOS and minimizing hospitalization costs are essential for establishing an effective and economically efficient healthcare system47.
Accumulate evidence has emerged over the past 10 years that TEAS plays many beneficial roles in perioperative patients. Firstly, TEAS can improve the gastrointestinal function of postoperative patients, including accelerating the time to the first postoperative gas and bowel movement, the time to the recovery of bowel sounds, the time to the recovery of a normal diet, and reducing the incidence of postoperative nausea and vomiting and paralytic bowel obstruction48–50. Mechanistically, acupoint stimulation by TEAS can influence the brain-gut axis, which is a bridge connecting the central nervous system and the gastrointestinal tract. This influence includes the change of brain-gut peptide secretion and the stimulation of the vague nerve and posterior horn of the spinal cord, leading to constructive effects on gastrointestinal sensation, peristalsis and microbiota11,51,52. Secondly, TEAS has been reported to reduce the incidence of psychiatric system-related symptoms or disorders, such as anxiety, insomnia, postoperative delirium, postoperative cognitive dysfunction, etc. in postoperative patients4,53–57. These roles are closely related to the modulation of endogenous substances by TEAS in perioperative patients. For example, TEAS improves sleep quality by modulating levels of serotonin (5-HT), norepinephrine, cortisol, melatonin, etc.57. In addition, TEAS decrease IL-6 and high-sensitivity C-reactive protein levels and increases serum Calcitonin Gene-Related Peptide levels to reduce the cumulative duration of cognitive decline in postoperative patients58. Thirdly, TEAS also modulates neurological-related functions, leading to pain relief, less anesthetic drug use, and sedation59,60. This may be related to the fact that TEAS induces the release of endogenous opioid peptides (e.g. enkephalins, endorphins, and dynorphins) at the central level to produce analgesia60. β-endorphin is the main analgesic substance released by the pituitary gland and plays an important role in self analgesia61. Perioperative use of TEAS has been reported to increase serum β-endorphin concentrations in patients62,63. Collectively, usage of TEAS could modulate various endogenous substances and regulate nerve system, thus reducing LOS and hospitalization costs in perioperative patients by diverse biological mechanisms. In reviewing the literature, we found that TEAS also plays beneficial roles in the population from countries such as Poland, America, and Turkey, when they are in the perioperative period64–70. These studies demonstrated that TEAS relieves pain levels, reduces the use of paroxysmal medications, maintains blood pressure, and reduces the incidence of nausea, indicating that people from other nations besides the Chinese people will also benefit from TEAS in perioperative period 64–70. They were not included in our review because they did not evaluate two important indicators of interest, LOS, and cost of hospitalization. However, due to its diverse beneficial effects in the perioperative period in these population, it is reasonable to speculate that TEAS might reduce LOS and hospitalization costs in these patients. Furthermore, as a highest level of evidence, our systematic review and meta-analysis will serve as an important reminder for more attention to the role of TEAS on LOS and the hospitalization costs, to the future studies related to TEAS in the perioperative period worldwide.
Although there was heterogeneity in our results, we conducted subgroup and sensitivity analyses to identify the potential sources of heterogeneity. These included the type of surgery and frequency of stimulation versus stimulation points. We observed that most of the TEAS stimulation intensities used clinically were at the maximum intensity tolerated by patients. However, there were variations in the stimulation frequency and choice of acupuncture points among studies with the same type of surgery. Previous studies have explored different stimulation frequencies in the perioperative period; however, our research has revealed that this approach is inadequate. Therefore, it is essential to identify the specific frequencies and acupuncture points that have the greatest impact on TEAS. Notably, the pooled estimates revealed a pronounced effect of TEAS on hospitalization costs in patients undergoing cesarean section, while TEAS induced decrease in LOS and postoperative LOS were rather prominent in elderly patients and those underwent lung surgery. Furthermore, both studies identified as primary sources of heterogeneity through leave-one-out analysis focused on patients undergoing gastrointestinal surgery. These findings implies that the effect of TEAS may be more prominent in patients undergoing surgeries with greater trauma or those with a poorer baseline condition, although further validation is warranted. Furthermore, we found only one study that included both LOS and postoperative LOS23. The inclusion of both metrics not only increases the credibility of the evidence but also allows for a more comprehensive analysis. The current literature has significant limitations in this area, and we strongly encourage future researchers to conduct studies that encompass both LOS and postoperative LOS metrics.
This study has certain limitations. First, the majority of the included trials did not adequately describe allocation concealment, blinding of participants and personnel, or blinding of outcome data. This lack of information raises concerns about the reliability of the results. In addition, some results were drawn from a limited number of studies, leading to a low level of evidence. This restricts the generalizability of the findings and highlights the need for further research. Furthermore, it is worth noting that most of the included studies had intermediate research quality, which may have influenced the reliability of the results. These limitations should be considered when interpreting the findings of this study. Further well-designed trials with a focus on addressing these limitations are necessary to provide more robust and reliable evidence.
Conclusion
This systematic review and meta-analysis suggests that the use of TEAS during the perioperative period may reduce hospitalization costs, LOS, and postoperative LOS. However, caution is needed when interpreting the results of this review because of the identified bias and the diversity of the findings. Despite the use of TEAS in various surgeries during the perioperative period, current research remains inadequate in comparison to the wide range of surgical conditions. Subsequently, further high-quality studies pertaining to TEAS are required.
Ethical approval
No patients were involved in this study.
Consent
No patients were involved in this study.
Source of funding
None.
Author contribution
Y.L.: concept development, article writing, and data analysis; J.F. and X.Z.: data collection and data analysis; W.X.: concept presentation and article revision; Z.S. and J.C.: data collection; P.W.: concept presentation and article revision.
Conflicts of interest disclosure
The authors declare that they have no financial conflict of interest with regard to the content of this report.
Research registration unique identifying number (UIN)
As required, we registered our systematic review and meta-analysis in the PROSPERO database (registration number: CRD42023416677).
Guarantor
Peiqin Wang.
Data availability statement
The data are publicly available.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Supplementary Material
Acknowledgements
Assistance with the study: none.
Presentation: none.
Footnotes
Yilong Liu, Jiefu Fan, Xiaoqing Zhang, and Wenping Xu contributed equally to this work.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Supplemental Digital Content is available for this article. Direct URL citations are provided in the HTML and PDF versions of this article on the journal's website, www.lww.com/international-journal-of-surgery.
Published online 22 May 2024
Contributor Information
Yilong Liu, Email: 2481498850@qq.com.
Jiefu Fan, Email: fanjf6382018037@163.com.
Xiaoqing Zhang, Email: xiaoanbao@vip.qq.com.
Wenping Xu, Email: xwp198527@sina.com.
Zhiwen Shi, Email: ssszwww@163.com.
Jiarong Cai, Email: 253933281@qq.com.
Peiqin Wang, Email: fjqpq1987@163.com.
References
- 1. Pan YY, Shao YF, Chi ZH, et al. Transcutaneous electrical acupoint stimulation accelerates the recovery of patients undergoing laparoscopic myomectomy: a randomized controlled trial. J Pain Res 2023;16:809–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Li SY, Jiang HL, Liu W, et al. Transcutaneous electrical acupoint stimulation for the prevention of perioperative neurocognitive disorders in geriatric patients: a systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore) 2022;101:e32329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zhang YF, Gong LR, Zhang Y, et al. Effect of transcutaneous acupoint electrical stimulation on urinary retention and urinary ATP in elderly patients after laparoscopic cholecystectomy: a prospective, randomized, controlled clinical trial. Clin Interv Aging 2022;17:1751–1760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Fan QQ, Lei C, Wang YH, et al. Transcutaneous electrical acupoint stimulation combined with auricular acupressure reduces postoperative delirium among elderly patients following major abdominal surgery: a randomized clinical trial. Front Med (Lausanne) 2022;9:855296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tu Q, Yang Z, Gan JH, et al. Transcutaneous electrical acupoint stimulation improves immunological function during the perioperative period in patients with non-small cell lung cancer undergoing video-assisted thoracic surgical lobectomy. Technol Cancer Res Treat 2018;17:1533033818806477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zhou DD, Hu B, He S, et al. Transcutaneous electrical acupoint stimulation accelerates the recovery of gastrointestinal function after cesarean section: a randomized controlled trial. Evid Based Complement Alternat Med 2018;2018:7341920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Zhang TT, Ou L, Chen ZH, et al. Transcutaneous electrical acupoint stimulation for the prevention of postoperative cognitive dysfunction: a systematic review and meta-analysis. Front Med (Lausanne) 2021;8:756366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. De Roo AC, Vu JV, Regenbogen SE. Statewide utilization of multimodal analgesia and length of stay after colectomy. J Surg Res 2020;247:264–270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Huang W, Long WF, Xiao JB, et al. Effect of electrically stimulating acupoint, Zusanli (ST 36), on patient’s recovery after laparoscopic colorectal cancer resection: a randomized controlled trial. J Tradit Chin Med 2019;39:433–439. [PubMed] [Google Scholar]
- 10. Zhu X, Zhang P, Lou C, et al. Perioperative inhaled corticosteroids treatment is associated with decreased length-of-stay and direct medical costs in high-respiratory-risk surgeries. J Med Econ 2020;23:280–286. [DOI] [PubMed] [Google Scholar]
- 11. Li WJ, Gao C, An LX, et al. Perioperative transcutaneous electrical acupoint stimulation for improving postoperative gastrointestinal function: a randomized controlled trial. J Integr Med 2021;19:211–218. [DOI] [PubMed] [Google Scholar]
- 12. Que B, Tu Q, Shi JL, et al. Effects of transcutaneous electrical acupoint stimulation on systemic inflammatory response syndrome of patients after percutaneous nephrolithotomy: a randomized controlled trial. Evid Based Complement Alternat Med 2021;2021:5909956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Zhao FC, Wang ZY, Ye CY, et al. Effect of transcutaneous electrical acupoint stimulation on one-lung ventilation-induced lung injury in patients undergoing esophageal cancer operation. Evid Based Complement Alternat Med 2020;2020:9018701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg 2021;88:105906. [DOI] [PubMed] [Google Scholar]
- 15. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017;358:j4008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Chen J, Fang YL, Lan YY. Effect of transcutaneous acupoint electrical stimulation on postoperative intestinal function in patients with colorectal cancer (Chinese). Chinese Foreign Med Res 2021;19:22–24. [Google Scholar]
- 17. Deng QZ, Li XH. Effects of transcutaneous electrical acupoint stimulation on postoperative recovery after laparoscopic nephrectomy (Chinese). J Clin Surg 2019;27:477–479. [Google Scholar]
- 18. Du HR. Study on effect transcutaneous electrical acupoint stimulation on immune function in perioperative patients with lung cancer (Chinese). Modern J Integrat Traditional Chinese Western Med 2015;24:4010–4013. [Google Scholar]
- 19. Ge M, Qu XJ, Li Y. Clinical efficacy of adductor canal blockade combined with transcutaneous electrical acupoint stimulation for total knee arthroplasty (Chinese). China J Orthop Traumatol 2021;34:750–754. [DOI] [PubMed] [Google Scholar]
- 20. Li F, Gu SH, Gan JH, et al. Effects of TEAS on pain, gastrointestinal function and plasma inflammatory factors after radical hysterectomy of cervical cancer under laparoscope (Chinese). Western J Tradition Chinese Med 2020;33:118–122. [Google Scholar]
- 21. Lin X, Zhang LL, Cui XG, et al. Application of transcutaneous electrical acupoint stimulation in gynecological enhanced recovery after surgery (Chinese). J Harbin Med Univ 2020;54:431–435. [Google Scholar]
- 22. Liu ZY, Song ZP, Tang F, et al. Effects of percutaneous electrical stimulation on immune function in patients undergoing laparoscopic radical gastrectomy (Chinese). Jiangxi Med J 2020;55:508–925. [Google Scholar]
- 23. Lv ZF, Wang Y, Zhu JP, et al. Effects of transcutaneous electrical acupoint stimulation treating nausea and vomiting after laparoscopic gastrointestinal surgery (Chinese). Tradition Chinese Med Res 2022;35:24–28. [Google Scholar]
- 24. Sun W, Zhou Q, Zhang XZ, et al. Effects of transcutaneous electrical acupoint stimulation on the recovery of body function of cesarean women (Chinese). J Clin Anesthesiol 2020;36:271–274. [Google Scholar]
- 25. Tang F, Song ZP, Liu ZY, et al. Effect of transcutaneous electrical acupoint stimulation on patients undergoing laparoscopic radical gastrectomy for gastric cancer (Chinese). Med Innov China 2020;17:50–54. [Google Scholar]
- 26. Wang PH, Meng XH. Transcutaneous electrical acupoint stimulation relieving postoperative fatigue syndrome in elderly patients undergoing radical resection of lung cancer by inhibiting inflammatory respond (Chinese). Int Med Health Guid News 2021;27:1428–1432. [Google Scholar]
- 27. Wang QN, Zhang JQ, Cui MZ, et al. Effect of acupuncture-drug balanced anesthesia on early cognitive function and short-term clinical prognosis after gynecological tumor surgery of elderly patients (Chinese). Int Med Health Guid News 2021;27:2655–2660. [Google Scholar]
- 28. Kong JQ, Feng D, Chen YL, et al. Effects of transcutaneous electrical acupoint stimulation on inflammation in patients undergoing video-assisted thoracoscopic lobectomy (Chinese). J Tongji Univ (Medical Science) 2019;40:321–325. [Google Scholar]
- 29. Yang Q, Yu BY, Ma CL. Clinical study of transcutaneous acupoint electrical stimulation in the treatment of gastrointestinal dysfunction in the elderly after gastrointestinal surgery (Chinese). China Modern Doctor 2018;56:14–18. [Google Scholar]
- 30. Yuan L, Guo J, Tang W, et al. Effect of transcutaneous electrical acupoint stimulation on gastrointestinal function in perioperative period of laparoscopic intestinal surgery (Chinese). J Clin Anesthesiol 2017;33:567–569. [Google Scholar]
- 31. Zhang LH, Zhao XY, Wang Z, et al. Effect of transcutaneous electrical acupoint stimulation-aided anesthesia on postoperative outcome in the elderly patients undergoing total knee arthroplasty (Chinese). J Shanxi Med Univ 2018;49:1243–1246. [Google Scholar]
- 32. Duan ZX, Wu XH, Wang JH, et al. Effects of transcutaneous electrical acupoint stimulation-assisted anesthesia on pain and rapid recovery in elderly patients undergoing thoracoscopic surgery (Chinese). Chinese J Geriatr 2020;39:323–327. [Google Scholar]
- 33. Wang MY, Yang CW, Han MM, et al. Effect of transcutaneous electric acupoint stimulation on prognosis in patients at high risk of postop-erative pulmonary complications (Chinese). Chinese J Anesthesil 2017;37:1287–1290. [Google Scholar]
- 34. Wei QL, Pang YH, Zuo HQ, et al. Eff1ect of transcutaneous electrical acupoint stimulation combined with chewing gum on postoperative gastrointestinal function after colorectal cancer resection (Chinese). Chinese J Modern Nurs 2019;25:2746–2749. [Google Scholar]
- 35. Wu XY, Jiang MT, Huang JL, et al. Effect of perioperative transcutaneous electrical acupoint stimulation on postoperative cellular immune function in patients undergoing posterior spinal internal fixation (Chinese). Chinese J Anesthesiol 2022;42:1030–1034. [Google Scholar]
- 36. Yang YL, Zhu GS, Rong XF, et al. Improvement in outcomes by acupuncture-drug balanced anesthesia following radical correction of tetralogy of Fallot under cardiopulmonary bypass in pediatric patients (Chinese). Chinese J Anesthesiol 2020;40:462–465. [Google Scholar]
- 37. Wang QY, Li J, Qian XL. Effect of transcutaneous electrical acupoint stimulation on sleep quality after radical operation for esophageal cancer (Chinese). Chinese J Anesthesiol 2020;40:404–407. [Google Scholar]
- 38. Huang L, Zhang FX, Xu C, et al. Efficacy of TEAS for general anesthesia preserving spontaneous breathing in patients undergoing thoracoscopic surgery (Chinese). Chinese J Anesthesiol 2019;39:961–965. [Google Scholar]
- 39. Wang XJ, Li JL, Wei DD, et al. Effects of acupoint compatibility factors on efficacy of acupuncture-drug balanced anesthesia in patients undergoing laparoscopic cholecystectomy (Chinese). Chinese J Anesthesiol 2020;40:707–710. [Google Scholar]
- 40. Li H, Wen Q, Hu HQ, et al. Transcutaneous electrical acupoint stimulation combined with electroacupuncture for rapid recovery after abdominal surgery: a randomized controlled trial (Chinese). Chinese Acupunct Moxibust 2023;43:135–140. [DOI] [PubMed] [Google Scholar]
- 41. Mu L, Gao H, Zhao ML, et al. Effect of transcutaneous electrical acupoint stimulation on recovery of gastrointestinal function after cesarean section (Chinese). Chinese Acupunct Moxibustion 2019;39:259–262. [DOI] [PubMed] [Google Scholar]
- 42. Fan XM, Zhang FX, Huang L, et al. Effects of TEAS combined with general anesthesia versus epidural block combined with general anesthesia on recovery of patients undergoing laparoscopic radical resection of colorectal cancer (Chinese). Chinese J Anesthesil 2018;38:1053–1057. [Google Scholar]
- 43. Lu ZH, Luo AL, Min S, et al. Acupoint stimulation for enhanced recovery after colon surgery: a prospective multicenter randomized controlled trial. J Multidiscip Healthc 2022;15:2871–2879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Guo F, Yan YT, Sun L, et al. Transcutaneous electrical acupoint stimulation for preventing postoperative delirium: a meta-analysis. Neuropsychiatr Dis Treat 2023;19:907–920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Zhang S, Guo WP, Jiao YL, et al. Systematic review and meta-analysis of the effect of transcutaneous electrical acupoint stimulation on gastrointestinal function after laparoscopic surgery. Ann Palliat Med 2021;10:11840–11848. [DOI] [PubMed] [Google Scholar]
- 46. Ou WJ, Zhang Q, He JL, et al. Hospitalization costs of injury in elderly population in China: a quantile regression analysis. BMC Geriatr 2023;23:143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Lundgren ME, Detwiler AN, Lamping JW, et al. Effect of instrumented spine surgery on length of stay. J Am Acad Orthop Surg Glob Res Rev 2023;7:e22.00231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Izzo AA, Hoon-Kim S, Radhakrishnan R, et al. A critical approach to evaluating clinical efficacy, adverse events and drug interactions of herbal remedies. Phytother Res 2016;30:691–700. [DOI] [PubMed] [Google Scholar]
- 49. Wang J, Lu FF, Ge MM, et al. Transcutaneous electrical acupoint stimulation improves postoperative sleep quality in patients undergoing laparoscopic gastrointestinal tumor surgery: a prospective, randomized controlled trial. Pain Ther 2023;12:707–722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Su X, Wang DX. Improve postoperative sleep: what can we do? Curr Opin Anaesthesiol 2018;31:83–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Kjølhede P, Langström P, Nilsson P, et al. The impact of quality of sleep on recovery from fast-track abdominal hysterectomy. J Clin Sleep Med 2012;8:395–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Song BJ, Chang YY, Li Y, et al. Effects of transcutaneous electrical acupoint stimulation on the postoperative sleep quality and pain of patients after video-assisted thoracoscopic surgery: a prospective, randomized controlled trial. Nat Sci Sleep 2020;12:809–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Tanaka M, Török N, Tóth F, et al. Co-players in chronic pain: neuroinflammation and the tryptophan-kynurenine metabolic pathway. Biomedicines 2021;9:897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Wang D, Shi HS, Yang ZG, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation for postoperative pain: a meta-analysis of randomized controlled trials. Pain Res Manag 2022;2022:7570533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Li T, Li J, Yuan LY, et al. Effect of regional vs general anesthesia on incidence of postoperative delirium in older patients undergoing hip fracture surgery: the RAGA randomized trial. JAMA 2022;327:50–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Oh ST, Park JY. Postoperative delirium. Korean J Anesthesiol 2019;72:4–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Ding LL, Ning JQ, Guo YH, et al. The preventive effect of transcutaneous electrical acupoint stimulation on postoperative delirium in elderly patients with time factors: a randomized trial. J Integr Complement Med 2022;28:689–696. [DOI] [PubMed] [Google Scholar]
- 58. Gao F, Zhang Q, Li Y, et al. Transcutaneous electrical acupoint stimulation for prevention of postoperative delirium in geriatric patients with silent lacunar infarction: a preliminary study. Clin Interv Aging 2018;13:2127–2134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Gao W, Li WP, Yan YQ, et al. Transcutaneous electrical acupoint stimulation applied in lower limbs decreases the incidence of paralytic ileus after colorectal surgery: a multicenter randomized controlled trial. Surgery 2021;170:1618–1626. [DOI] [PubMed] [Google Scholar]
- 60. Xiong QJ, Min S, Wei K, et al. Transcutaneous electrical acupoint stimulation combined with dexamethasone and tropisetron prevents postoperative nausea and vomiting in female patients undergoing laparoscopic sleeve gastrectomy: a prospective, randomized controlled trial. Obes Surg 2021;31:1912–1920. [DOI] [PubMed] [Google Scholar]
- 61. Yeh ML, Chung YC, Hsu LC, et al. Effect of transcutaneous acupoint electrical stimulation on post-hemorrhoidectomy-associated pain, anxiety, and heart rate variability: a randomized-controlled study. Clin Nurs Res 2018;27:450–466. [DOI] [PubMed] [Google Scholar]
- 62. Zhou X, Cao SG, Tan XJ, et al. Effects of transcutaneous electrical acupoint stimulation (TEAS) on postoperative recovery in patients with gastric cancer: a randomized controlled trial. Cancer Manag Res 2021;13:1449–1458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Qi WH, Miao WJ, Ji YZ, et al. The analgesic effect of transcutaneous electrical acupoint stimulation on labor: a randomized control study. Int J Gen Med 2021;14:559–569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Lu L, Zhang Y, Tang X, et al. Evidence on acupuncture therapies is underused in clinical practice and health policy. BMJ 2022;376:e067475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Szmit M, Agrawal S, Goździk W, et al. Transcutaneous electrical acupoint stimulation reduces postoperative analgesic requirement in patients undergoing inguinal hernia repair: a randomized, placebo-controlled study. J Clin Med 2021;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. AminiSaman J, Mohammadi S, Karimpour H, et al. Transcutaneous electrical nerve stimulation at the acupuncture points to relieve pain of patients under mechanical ventilation: a randomized controlled study. J Acupunct Meridian Stud 2018;11:290–295. [DOI] [PubMed] [Google Scholar]
- 67. Yildiz M, Kozanhan B. Transcutaneous electric acupoint stimulation reduces rocuronium injection-related pain: a prospective randomized controlled study. Eur Rev Med Pharmacol Sci 2022;26:6215–6220. [DOI] [PubMed] [Google Scholar]
- 68. Arai YC, Kato N, Matsura M, et al. Transcutaneous electrical nerve stimulation at the PC-5 and PC-6 acupoints reduced the severity of hypotension after spinal anaesthesia in patients undergoing caesarean section. Br J Anaesth 2008;100:78–81. [DOI] [PubMed] [Google Scholar]
- 69. Zárate E, Mingus M, White PF, et al. The use of transcutaneous acupoint electrical stimulation for preventing nausea and vomiting after laparoscopic surgery. Anesth Analg 2001;92:629–635. [DOI] [PubMed] [Google Scholar]
- 70. Greif R, Laciny S, Mokhtarani M, et al. Transcutaneous electrical stimulation of an auricular acupuncture point decreases anesthetic requirement. Anesthesiology 2002;96:306–312. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data are publicly available.