

Scheme of de-airing using ELIZABETH circuit.
Central Message.
De-airing via LV perfusion using the ELIZABETH circuit befroe aortic declamping is a useful and simple technique for MICS.
During cardiac surgery, removing air from the left side of the heart is essential in preventing air embolism formation in the right coronary or intracranial arteries. Air emboli in the right coronary artery can cause ventricular dysfunction or arrhythmias, whereas those in the intracranial arteries result in neurological deficits.1 We conventionally inject carbon dioxide gas, which blood and water readily absorb, into the thorax or mediastinum to prevent air embolism. Additionally, we routinely inflate the lungs to obtain blood flow from the pulmonary circulation, perform cardiac massage to evacuate air through the root cannula, and reposition the patient in the Trendelenburg position to prevent air emboli before aortic declamping. However, in minimally invasive cardiac surgery (MICS), right lung inflation is discouraged to preserve the surgical field. Moreover, direct heart massage is impossible in MICS cases. Thus, in cases of MICS, limited maneuvers can be performed to reduce air embolism formation. To avoid transient myocardial ischemia, myocardial infarction, or catastrophic neurological deficits during cardiac surgery, de-airing of the left side of the heart before aortic declamping is of paramount importance. Nonetheless, de-airing during MICS is challenging due to the limited surgical field.
To ensure safe MICS, we have been performing an original technique for more than 25 years to evacuate air from the left ventricle, using the Extending LIne for minimiZing Air embolism BETween perfusion brancH and left ventricular vent (ELIZABETH) circuit (Figure 1).2 Consequently, in this report, we have presented and described the de-airing technique using this simple and useful ELIZABETH circuit, demonstrating how we maintained safety during MICS.
Figure 1.

Extending LIne for minimizing Air emboli BETween perfusion brancH and left ventricular vent circuit. A, The circuit connector between the left ventricular vent tube and suction line is shown. B, Postprocedure, before aortic declamping, extension line between the connector and perfusion branch of the cardiopulmonary bypass is depicted.
Technique
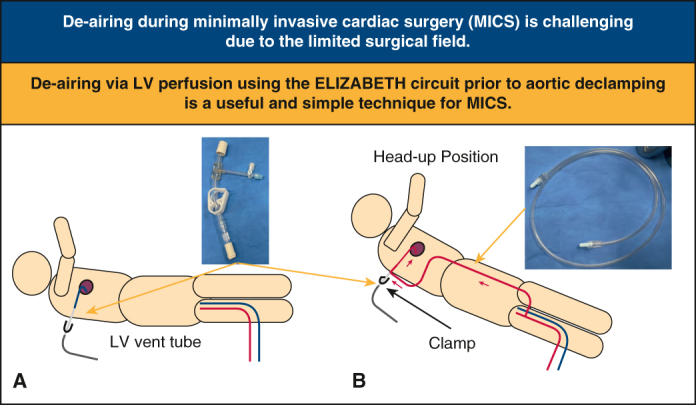
For each patient undergoing MICS, we placed a circuit connector (Figure 1, A), 6 mm in diameter, between the left ventricular vent and suction line before performing the main procedure (Figure 2, A). We introduced carbon dioxide gas into the surgical field. After the procedure, before aortic declamping, an extension line (inside diameter, 3.5 mm; length, 1 m) (Figure 1, B) was attached between the connector and perfusion branch of the cardiopulmonary bypass (CPB). Thereafter, we opened the connector, clamped the CPB side of the suction line, perfused blood from the perfusion line of the CPB through the ELIZABETH circuit into the left ventricle, and evacuated the air through the root cannula in the head-up position (Figure 2, B). If blood was evacuated from the root cannula, we judged adequate de-airing from the left ventricle. Thereafter, we closed the ELIZABETH circuit and injected “hot shot” cardioplegia through the root cannula (Video 1). After repositioning the patient in the Trendelenburg position, the aorta was de-clamped. Thereafter, the patient was weaned off the CPB.
Figure 2.

Setting before de-airing and de-airing using the Extending LIne for minimizing Air emboli BETween perfusion brancH (ELIZABETH) and left ventricular vent circuit. A, Setting before de-airing is shown. B, De-airing using the ELIZABETH circuit is shown.
We have performed this de-airing technique in 141 cases (12 and 129 cases of right minithoracotomy and ministernotomy aortic valve replacements, respectively) for more than 25 years.
Written informed consent was obtained from all patients whose intraoperative videos were used for this report and the publication of their de-identified data. The Institutional Review Board of Kansai Electric Power Hospital approved this report on December 27, 2023 (approval No.: 23-133).
Discussion
In this report, we have presented and described in detail the de-airing technique involving the use of the simple ELIZABETH circuit.
The advantage of de-airing using the ELIZABETH circuit is due to its simplicity because air can easily be evacuated from the left side of the heart. Therefore, this circuit can be used in various procedures, including minithoracotomy and ministernotomy AVRs as well as minithoracotomy mitral valve repairs. Furthermore, active de-airing, which is generally performed passively, is possible with this technique. No contraindications or disadvantages of the technique are known; nevertheless, the only inconvenience is the need to prepare the ELIZABETH circuit preoperatively.
Conclusions
De-airing using the ELIZABETH circuit before aortic declamping is a useful and simple technique for MICS.
Conflict of Interest Statement
The authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Acknowledgments
The authors thank Editage (www.editage.com) for English language editing.
Footnotes
IRB number and date of approval: 23-133; December 27, 2023.
Informed consent statement: Written informed consent was obtained from the patient whose video was used for this report.
Supplementary Data
This video depicts how the Extending LIne for minimizing Air emboli BETween perfusion brancH and left ventricular vent circuit has been used during minimally invasive cardiac surgery. Video available at: https://www.jtcvs.org/article/S2666-2507(24)00251-7/fulltext.
{kind=link}
References
- 1.Orihashi K., Ueda T. “De-airing” in open heart surgery: report from the CVSAP nation-wide survey and literature review. Gen Thorac Cardiovasc Surg. 2019;67(10):823–834. doi: 10.1007/s11748-019-01168-6. [DOI] [PubMed] [Google Scholar]
- 2.Suenaga E., Suda H., Katayama Y., et al. Comparison of limited and full sternotomy in aortic valve replacement. Jpn J Thorac Cardiovasc Surg. 2004;52(6):286–291. doi: 10.1007/s11748-004-0044-9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
This video depicts how the Extending LIne for minimizing Air emboli BETween perfusion brancH and left ventricular vent circuit has been used during minimally invasive cardiac surgery. Video available at: https://www.jtcvs.org/article/S2666-2507(24)00251-7/fulltext.