

Abstract
Background
Inhaled anticholinergics as single agent bronchodilators (or in combination with beta2‐agonists) are one of the several medications available for the treatment of acute asthma in children.
Objectives
To determine the effectiveness of only inhaled anticholinergic drugs (i.e. administered alone), compared to a control in children over the age of two years with acute asthma.
Search methods
The Cochrane Register of Controlled Trials (CENTRAL), and the Cochrane Airways Group Register of trials were searched by the Cochrane Airways Group. The latest search was performed in April 2011.
Selection criteria
We included only randomised controlled trials (RCTs) in which inhaled anticholinergics were given as single therapy and compared with placebo or any other drug or drug combinations for children over the age of two years with acute asthma.
Data collection and analysis
Two authors independently selected trials, extracted data and assessed trial quality.
Main results
Six studies met the inclusion criteria but were limited by small sample sizes, various treatment regimes used and outcomes assessed. The studies were overall of unclear quality. Data could only be pooled for the outcomes of treatment failure and hospitalisation. Other data could not be combined due to divergent outcome measurements. Meta‐analysis revealed that children who received anticholinergics alone were significantly more likely to have treatment failure compared to those who received beta2‐agonists from four trials on 171 children (odds ratio (OR) 2.27; 95% CI 1.08 to 4.75). Also, treatment failure on anticholinergics alone was more likely than when anticholinergics were combined with beta2‐agonists from four trials on 173 children (OR 2.65; 95% CI 1.2 to 5.88). Data on clinical scores/symptoms that were measured on different scales were conflicting. Individual trials reported that lung function was superior in the combination group when compared with anticholinergic agents used alone. The use of anticholinergics was not found to be associated with significant side effects.
Authors' conclusions
In children over the age of two years with acute asthma exacerbations, inhaled anticholinergics as single agent bronchodilators were less efficacious than beta2‐agonists. Inhaled anticholinergics were also less efficacious than inhaled anticholinergics combined with beta2‐agonists. Inhaled anticholinergic drugs alone are not appropriate for use as a single agent in children with acute asthma exacerbations.
Keywords: Adolescent; Child; Child, Preschool; Humans; Acute Disease; Administration, Inhalation; Adrenergic beta‐2 Receptor Agonists; Adrenergic beta‐2 Receptor Agonists/administration & dosage; Albuterol; Albuterol/administration & dosage; Asthma; Asthma/drug therapy; Atropine; Atropine/administration & dosage; Bronchodilator Agents; Bronchodilator Agents/administration & dosage; Cholinergic Antagonists; Cholinergic Antagonists/administration & dosage; Drug Therapy, Combination; Drug Therapy, Combination/methods; Fenoterol; Fenoterol/administration & dosage; Ipratropium; Ipratropium/administration & dosage; Metaproterenol; Metaproterenol/administration & dosage; Randomized Controlled Trials as Topic; Scopolamine Derivatives; Scopolamine Derivatives/administration & dosage; Treatment Failure
Plain language summary
Anticholinergic therapy for acute asthma in children
Asthma is a condition that affects the airways (tubes carrying air in and out of the lungs). During an asthma exacerbation (attack), the airways narrow and drugs can be taken to dilate, or widen, the airways. Common bronchodilators (medicines used to widen the airways) are short‐acting beta2‐ agonists (e.g. salbutamol) or anticholinergics (e.g. ipratropium bromide). In this review, we examined if the use of anticholinergic inhalers during an asthma attack in children aged over two years is effective compared to either placebo or another bronchodilator. We also looked at combinations of anticholinergic plus a beta2‐agonist compared to an anticholinergic on its own.
We found six small trials of unclear quality answering these two questions. We found data from four trials on 171 children comparing anticholinergics with beta2‐agonists. Children on anticholinergics alone were significantly more likely to experience treatment failure than those on beta2‐agonists (odds ratio (OR) 2.27; 95% CI 1.08 to 4.75). We also found data from four trials on 173 children comparing children on anticholinergics alone with children on anticholinergics plus beta2‐agonists. In this case, treatment failure was more likely in children taking anticholinergics only than if they were combined with beta2‐agonists (OR 2.65; 95% CI 1.2 to 5.88). We were only able to combine data for treatment failure and hospitalisation.
In summary, we found that inhaled anticholinergics used on their own are less effective than inhaled beta2‐agonists used alone or in combination with anticholinergics. Inhaled anticholinergics seem safe, with no significant side effects apparent.
Background
Inhaled anticholinergics as single agent bronchodilators (or in combination with beta2‐agonists) are one of the several medications available for the treatment of acute asthma in children. Ipratropium bromide, an inhaled anticholinergic agent, has been used extensively in emergency departments as adjunctive therapy with beta2‐agonists for the emergency treatment of acute asthma exacerbations. The objective of this review was to determine the effectiveness of only inhaled anticholinergic drugs (i.e. administered alone), compared to a control or combination treatment in children over the age of two years with acute asthma.
Description of the condition
Asthma is an inflammatory disorder of the airways in which many cells and cellular elements play a role. In susceptible individuals, this inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness and cough. These episodes are usually associated with widespread but variable airflow obstruction that is often reversible either spontaneously or with treatment. The inflammation also causes an associated increase in the existing bronchial hyperresponsiveness to a variety of stimuli (NHLBI 2007). Airflow obstruction (excessive airway narrowing) in asthma is the result of contraction of the airway smooth muscle and swelling of the airway wall due to smooth muscle hypertrophy and hyperplasia, inflammatory cell infiltration, oedema, goblet cell and mucous gland hyperplasia, mucous hypersecretion, protein deposition including collagen and epithelial desquamation. Potential triggers for the inflammatory process in asthma include allergy, viral respiratory infections, irritants such as tobacco smoke, air pollutants and occupational dusts, gases and chemicals, certain drugs, and non‐specific stimuli such as cold air exposure and exercise (NAC 2006).
Description of the intervention
Inhaled anticholinergics are bronchodilators. Ipratropium bromide is the most studied anticholinergic bronchodilator, and now most widely used of anticholinergic agents. Ipratropium bromide has been used extensively in emergency departments as adjunctive therapy with beta2‐agonists for the emergency treatment of acute asthma exacerbations. Multiple doses of anticholinergics in combination with beta2‐adrenergic agents have shown to be beneficial in adults (Undem 2001) and of some merit in school‐aged children with severe asthma exacerbation (Plotnick 2008). Current guidelines recommend the use of a combination of inhaled beta2‐agonists and anticholinergics, particularly for patients with acute severe or life‐threatening asthma in the emergency setting. Anticholinergics tend not to be used as first‐line drugs for asthma exacerbation (Gross 1988).
Inhaled anticholinergics are the drugs of choice in bronchospasm provoked by psychogenic stimuli and beta2‐blockers (Gross 1988; Beakes 1997). Ipratropium bromide also appears to have some benefit in nocturnal asthma (Beakes 1997). However, the principal clinical use of ipratropium bromide is in the treatment of adult patients with chronic obstructive pulmonary disease (Brown 2001).
How the intervention might work
Airway calibre is controlled in health and disease by many influences. The parasympathetic nervous system is one among the many mechanisms, which regulates the airway calibre by varying the bronchomotor tone. Muscarinic receptors are widely distributed in the airways and the release of acetylcholine at these sites results in both smooth muscle contraction and release of secretions from submucosal glands. An opportunity for therapeutic intervention exists at the level of these muscarinic receptors. Anticholinergics such as atropine and its analogues are competitive inhibitors of acetylcholine and may result in bronchodilatation by reducing the tone of smooth muscles (Gross 1988).
Anticholinergic agents act at muscarinic receptors, competitively inhibiting the effects of acetylcholine. Acetylcholine acts by causing smooth muscle constriction, which provides bronchomotor tone. By antagonising the effects of acetylcholine, cholinergic bronchomotor tone is inhibited and the vagal reflexes that mediate bronchoconstriction are blocked (McDonald 2010). Cholinergic‐induced bronchoconstriction appears to involve primarily the large airways, whereas beta2‐agonist medications relax both large and small airway constriction equally (Rodrigo 2002).
Ipratropium bromide (8‐isopropyl‐noratropine‐methobromide) is a synthetic quaternary ammonium congener of atropine. Ipratropium bromide differs from atropine and other naturally occurring anticholinergic alkaloids in one major aspect ‐ it is insoluble in lipids (although freely soluble in water) and crosses biological barriers with difficulty. One could thus describe ipratropium bromide as a topical form of atropine and hence virtually free of systemic side effects. Neither atropine nor ipratropium bromide is selective for the subtypes of muscarinic receptors. It was the first anticholinergic agent to be approved for use as a bronchodilator in adults and children (for acute asthma in children), with a wide therapeutic margin of safety and has no important side effects (Gross 1988; Brown 2001). Ipratropium bromide is a less potent bronchodilator than beta2‐adrenergic agents. The onset of action of ipratropium is slower than short‐acting beta2‐adrenergic agents (30 to 90 minutes versus 5 to 15 minutes).
Why it is important to do this review
The role of anticholinergic drugs for wheezing in children under the age of two years has been reviewed (Everard 2005). The authors concluded that there is not enough support for the uncritical use of anticholinergic therapy for wheezing under the age of two years. The review by Plotnick et al focused specifically on combined treatment with anticholinergics and beta2‐agonists in asthmatic children over the age of two years and concluded that anticholinergics plus beta2‐agonists have a beneficial effect over beta2‐agonists alone in improving lung function significantly and the addition of multiple doses of anticholinergics to beta2‐agonists reduced the risk of hospital admissions in children with predominantly severe exacerbations (Plotnick 2008). Plotnick et al also found that there was no conclusive evidence for using multiple doses of anticholinergics in children with mild or moderate asthma exacerbations. There is good evidence for the safety and efficacy of frequent doses of ipratropium bromide (every 20 to 30 minutes) used in addition to beta2‐agonists for the first two hours of a severe asthma attack in children over two years (BTS 2009). The addition of ipratropium bromide to beta2‐agonists for severe acute asthma may lead to some improvement in clinical symptoms and reduce the need for more intensive treatment in children less than two years. It does not significantly reduce the length of hospital stay either in combination with beta2‐agonists or in comparison with placebo (Everard 2005; BTS 2009).
When investigating the therapeutic effect of an agent that may be used in combination with another agent, it is important to establish separately the effectiveness of both the agents over placebo. It is also essential to compare the beneficial effect of the combined agents over placebo as well as the individual agents. In this way it is possible to establish: a) if the single agents have a therapeutic effect; and b) if there is an additive or synergistic effect from combining the agents.
This review focuses on the effectiveness of anticholinergic drugs (without beta2‐agonists) in children aged over two years with acute asthma. By comparing the effect of anticholinergics as single agents with that of other single agents and with combined therapy (anticholinergics with beta2‐agonists) as reviewed previously (Plotnick 2008), we aim to establish the role of anticholinergics as a monotherapy in the treatment of children over two years of age with acute asthma.
Objectives
To determine the effectiveness of inhaled anticholinergic drugs (used alone) compared to a control or combination treatment in children over the age of two years with acute asthma.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) in which only inhaled anticholinergics were given compared with placebo, or any other drug, or drug combinations for children over the age of two years with acute asthma.
Types of participants
We included trials of children aged two to eighteen years with acute asthma in all settings (emergency room, observation unit, in‐patient, out‐patient, general practice and home). Asthma must have been physician diagnosed or must have satisfied the criteria established internationally (such as BTS 2009 guidelines).
We excluded studies involving children under the age of two years since difficulties arise in establishing the diagnosis of asthma unequivocally. Also they have been reviewed previously (Everard 2005).
Types of interventions
Inhaled anticholinergic drugs delivered by any means; nebulised or by metered dose inhalers with or without spacer devices, and with or without facemask. We included all doses and dosing regimens.
We included the following comparisons.
Anticholinergics versus placebo.
Anticholinergics versus beta2‐agonists.
Anticholinergics versus anticholinergics plus beta2‐agonists.
Anticholinergics versus any other drugs or drug combinations.
Types of outcome measures
Outcome measures in the studies are summarised in Table 1.
1. Outcomes reported.
| Outcome | Calvo | Cook | Guill | Watson | Van Bever |
| Treatment failure | Yes: three criteria (TAL score < 2; PEF < 15% baseline measurement; intolerance to treatment) | Yes: one criterion (IV therapy) | Yes: three criteria for treatment failure (return visit to ED within 12 to 24 hours; IV treatment; admission to hospital) | Yes: one criterion (admission to hospital) | No |
| Admission | Yes (No patients required admission) | No | Yes | Yes | No |
| PEF | Yes (response to treatment determined by change in PEF) | No | Yes | No | No |
| FEV1 | No | No | No | Yes | Yes |
| FEF25‐75 | No | No | No | Yes | No |
| Residual bronchodilation (FEV1 and FEF25‐75) | No | No | No | Yes | No |
| Clinical scores | Yes (TAL score) | Yes (in‐house 4‐point scale. Wheeze, air entry on auscultation, respiratory distress measured) | Yes (Pulmonary Index ‐ respiratory rate, wheezing score, I/E ratio, accessory muscle use) | Yes (Pulmonary Index ‐ respiratory rate, wheezing score, I/E ratio, accessory muscle use) | No |
| Need for additional medication | Yes (need for bronchodilator/steroid and repeat nebulisation) | Yes (repeat nebulisation and need for IV therapy) | Yes (repeat nebulisation and need for IV therapy) | No | No |
| Withdrawals | No patients withdrew | 3 patients had treatment failure and dropped out | 10 episodes of wheezing had treatment failure | No patients withdrew; 2 children required hospital admission at the end of the study because of treatment failure | Not reported |
| Pulse oximetry | No | No | No | Yes | No |
| Side effects | Yes (no patient suffered SEs) | Yes (no patient suffered SEs) | Yes (no patient suffered SEs) | Yes (no patient suffered SEs) | Yes (no patient suffered SEs) |
ED: emergency department; FEF25‐75: forced expiratory flow at the 25 to the 75% point of forced vital capacity; FEV1: forced expiratory volume in the first second; I/E ratio: inspiration/expiration ratio; IV: intravenous; PEF: peak expiratory flow; SE: side effects; TAL: a clinical scoring system based on several markers such as respiratory rate, wheezing and cyanosis (the scale runs from 0 to 12, where 12 indicates a very severe illness).
Primary outcomes
Treatment failure
Admission to hospital
Secondary outcomes
Changes in symptoms or symptom scores
Requirement for additional medication
Changes in pulmonary function tests (peak expiratory flow (PEF) and forced expiratory volume in one second (FEV1))
Effects on oxygenation
Duration of hospital stay
Adverse effects
Withdrawals
Search methods for identification of studies
The methods used to identify the studies are summarised below.
Electronic searches
We identified trials from the Cochrane Airways Group Specialised Register of trials (CAGR), which is derived from systematic searches of bibliographic databases including the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, CINAHL, AMED, and PsycINFO, and handsearching of respiratory journals and meeting abstracts (please see Appendix 1 for further details). We searched all records in the CAGR coded as 'asthma' using the following terms:
("cholinergic antagonists" or "anticholinergic" or "anti‐cholinergic" or "cholinergic" or "muscarinic" or "antimuscarinic" or "ipratropium" or "tiotropium" or "atropine" or "atrovent" or "oxitropium" or "Sch1000" or "duovent", all as (textword) or (MeSH )) AND ("asthma" or "wheez" or "respiratory sounds" or "bronchial spasm", "bronchospas" or "bronch" or "spasm" or "bronchoconstrict" or "bronchoconstriction" or "bronch" or "constrict", all as (textword) or (MeSH )) AND ("adolescent" or "child" or "paediat" or "pediat" or "infan" or "toddler" or "bab" or "young" or "preschool" or "pre school" or "pre‐school" or "newborn" or "new born" or "new‐born" or "neo‐nat" or "neonat", all as (textword) or (MeSH )).
We also conducted an additional search of CENTRAL (see Appendix 2). We searched all databases from their inception to April 2011 and we imposed no restriction on the language of publication.
Searching other resources
We checked reference lists of all primary studies and review articles for additional references.
Data collection and analysis
From the title, abstract, or descriptors, two review authors (LT and AC) independently reviewed literature searches to identify potentially relevant trials for full review. We conducted searches of bibliographies and texts to identify additional studies.
Selection of studies
From the full text, using specific criteria, two reviewers (LT and AC) independently selected trials for inclusion. We resolved disagreement by consensus.
Data extraction and management
LT and AC extracted data for the trials for the outcomes above. We combined all trials using Review Manager 5 (RevMan 2011).
Assessment of risk of bias in included studies
Two review authors (LT and AC) performed methodological quality assessment, using the 'risk of bias' tool described in the Cochrane Handbook of Systematic Reviews of Interventions (Higgins 2011), focusing on:
random sequence generation;
allocation concealment; and
blinding
We graded each domain as either 'high', 'low' or 'unclear' risk of bias.
Measures of treatment effect
We obtained all outcomes directly from the publications of the included studies.
Continuous Outcomes
For continuous outcomes measured on the same metrics, we calculated individual and pooled statistics as weighted mean differences (WMDs) with 95% confidence intervals (CIs). For continuous outcomes measured on different metrics, we combined data with a standardised mean difference (SMD).
Dichotomous Outcomes
For dichotomous variables, we calculated individual and pooled statistics as odds ratios (ORs) with 95% CIs.
Unit of analysis issues
None relevant.
Dealing with missing data
The review authors did not contact any study authors as it was not felt necessary and the studies were also not recent.
Assessment of heterogeneity
We initially pooled all data with a fixed‐effect model. We measured heterogeneity using the I2 statistic (a measure of the degree of inconsistency between pooled studies). We used a random‐effects model to determine the impact of the variation in the results on the overall effect estimate.
Assessment of reporting biases
We planned to investigate publication bias by visually inspecting a funnel plot if ten or more trials had been included in a single meta‐analysis.
Data synthesis
We grouped outcomes relating to studies according to:
anticholinergic agents versus beta2‐ agonists; and
anticholinergic agents versus combination of anticholinergic agents plus beta2‐ agonists.
We pooled outcomes that were reported in the studies when possible, in accordance with primary and secondary outcomes.
Subgroup analysis and investigation of heterogeneity
We examined the influence of trial characteristics on the observed treatment effect. Assuming sufficient numbers of trials and the availability of necessary data, we described clinical heterogeneity with respect to treatment setting and asthma severity.
Age: two to five years versus five to eighteen years.
Co‐interventions: with corticosteroids versus none.
Different delivery methods of anticholinergics: metered dose inhaler (MDI) versus nebuliser.
Duration of anticholinergics administration: less than seven days versus more than seven days duration.
Asthma severity: mild and moderate versus severe asthma.
Sensitivity analysis
Sensitivity analyses provide an approach for testing how robust the results of a review are relative to key decisions and assumptions that have been made in the process of conducting the review. We planned to investigate the overall study quality of the pooled result using the Cochrane approach.
Results
Description of studies
Results of the search are summarised below.
Results of the search
Of the 349 abstracts that we identified, we retrieved 81 papers for full assessment by the reviewers (LT and AC). After excluding articles that focused on adult patients or articles that did not use inhaled anticholinergics as single agents for comparison (see Characteristics of excluded studies for reasons for exclusion), seven studies (one paper was an abstract from a conference proceeding of a paper (Van Bever 1994)) from six trials met the inclusion criteria for the review (Cook 1985; Guill 1987; Watson 1988; Van Bever 1994; Calvo 1998; Ni 2003). See 'Characteristics of included studies' for full details on each study.
Included studies
Study design
All studies were randomised and double‐blind except Ni 2003. All studies were of a parallel group design.
Participants
The included studies involved children between the ages of two and eighteen years who were treated for acute asthma. These studies recruited patients mainly from the emergency room (Cook 1985; Guill 1987). Van Bever 1994 and Watson 1988 did not refer to the study setting. Cook 1985 and Watson 1988 included patients with moderately severe asthma. Guill 1987 included patients of any severity of acute asthma and used episodes of wheezing for randomisation rather than individual patients. Calvo 1998 recruited participants who did not require hospitalisation and whose peak expiratory flow (PEF) was less than 80%. Symptom scores indicated that participants were suffering from moderately severe acute asthma (Calvo 1998).
Interventions
Route/Delivery
Three studies used nebulisers to deliver therapy (Cook 1985; Guill 1987; Watson 1988). These studies utilised a Hudson nebuliser with face mask but different models and techniques for driving therapy. Cook 1985 used an oxygen (8 litres/min) driven nebuliser unit and Watson 1988 used an air (7 litres/min) driven nebuliser. Guill 1987 did not describe the driving gas for the nebuliser. Ni 2003 used an oxygen driven nebuliser but no further details were available (translated paper). Calvo 1998 and Van Bever 1994 used a holding chamber and MDI.
Type of drug/dosage
Differing drugs, doses and dosing regimens were used in the six studies.
Calvo 1998: Three groups (ipratropium versus salbutamol versus ipratropium + salbutamol). Salbutamol 100 mcg (two inhalations; total 200 mcg per dose) four times in the first hour and three times in the subsequent hour at regular intervals, versus ipratropium bromide 20 mcg (two inhalations; total 40 mcg per dose) at the same time‐points versus combination salbutamol and ipratropium (equivalent doses to the parallel component therapies) at the same time‐points. Also, Calvo 1998 allowed for the addition of inhaled salbutamol or oral steroids where participants were deemed poor responders to therapy.
Cook 1985: Three groups (ipratropium versus fenoterol versus ipratropium + fenoterol). 0.025% (250 mcg/mL) solution of ipratropium bromide versus 0.5% (5000 mcg/mL) fenoterol solution versus combination 0.025% (250 mcg/mL) ipratropium bromide and 0.5% (5000 mcg/mL) fenoterol. The doses of both fenoterol and ipratropium bromide solution were adjusted according to the age of the children.
Guill 1987: Three groups (atropine versus metaproterenol versus atropine + metaproterenol). Atropine sulfate (0.05 to 0.1 mg/kg i.e. 500 to 1000 mcg/kg) versus 5% (50,000 mcg/mL) metaproterenol versus combination (5% metaproterenol and atropine sulfate). The dose of metaproterenol was adjusted to age and the dose of atropine sulfate was adjusted to weight.
Ni 2003: Three groups (ipratropium versus salbutamol versus ipratropium + salbutamol). 0.5% (5000 mcg/mL) salbutamol (0.25 to 1 mL i.e. 1250 to 5000 mcg) versus 0.025% (250 mcg/mL) ipratropium bromide (0.25 to 1 mL i.e. 62.5 to 250 mcg) versus combination (salbutamol (0.25 to 1 mL i.e. 1250 to 5000 mcg) and ipratropium bromide (0.25 to 1 mL i.e. 62.5 to 250 mcg)). The dose of both salbutamol and ipratropium bromide solution were adjusted according to the age of the children.
Van Bever 1994: Two groups (oxitropium versus fenoterol). Oxitropium bromide 200 mcg versus fenoterol 200 mcg. Subsequently all patient received 400 mcg fenoterol in an open label study.
Watson 1988: Three groups (ipratropium versus fenoterol versus ipratropium + fenoterol). Ipratropium bromide 250 mcg versus fenoterol 625 mcg versus combination (ipratropium bromide 250 mcg plus fenoterol 625 mcg).
Measurements of outcomes
Outcomes measured differed between the studies. For an overview of the outcomes measured in the studies, please see Table 1.
Definition of treatment failure varied between the studies. Guill 1987 considered three criteria for treatment failure (return visit to the emergency department within 12 to 24 hours; intravenous (IV) treatment; or admission to hospital). Watson 1988 considered admission to hospital as treatment failure and Cook 1985 set IV therapy as indication of treatment failure. Calvo 1998 did not report any pre‐defined treatment failure criteria, although this study reported that treatment was stopped if the TAL score was less than 2, if there was a poor response to the therapy and/or PEF was less than 15% at first measurement or if there was intolerance to the treatment (TAL score is a clinical scoring system based on several markers such as respiratory rate, wheezing and cyanosis; the scale runs from 0 to 12, where 12 indicates a very severe illness; Tal 1983). Poor response to therapy was defined in terms of change in PEF + 4% or less.
Four of the included studies used symptom scores: Calvo 1998 measured symptoms on the TAL scale; Watson 1988 and Guill 1987 used pulmonary index which used a scale of 0 to 12; and Cook 1985 used a clinical score on an in‐house four‐point scale.
Cook 1985 and Guill 1987 measured repeat nebulisations as one of their outcome measures. Watson 1988 did not measure additional medication. Calvo 1998 measured need for additional bronchodilation and steroid therapy.
Guill 1987 used improvement in PEF as one of their objective measures, while Watson 1988 elaborately measured spirometric functions (forced expiratory volume in 1 second (FEV1), forced expiratory flow at the 25 to the 75% point of forced vital capacity (FEF25‐75) and forced vital capacity (FVC)), at various time intervals to monitor the change. In addition to the improvement in the oxygen saturations, Watson 1988 also determined whether bronchodilation was still possible after study medication had been given, by administering open label salbutamol and measuring spirometry.
Excluded studies
We excluded studies that focused on adult patients or that did not use inhaled anticholinergics as single agents for comparison (see Characteristics of excluded studies for reasons for exclusion).
Risk of bias in included studies
Our judgement on the risk of bias for included studies is summarised in Figure 1.
1.
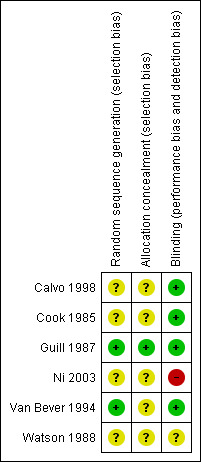
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Allocation
We judged two studies to be at low risk of bias for random sequence generation (Guill 1987; Van Bever 1994). The randomisation method was less well described in four studies and we therefore judged them to be at unclear risk of bias (Cook 1985; Watson 1988; Calvo 1998; Ni 2003).
Blinding
We judged four studies to be at low risk of bias for blinding (Cook 1985; Guill 1987; Van Bever 1994; Calvo 1998), while we were unclear about the risk of bias in Watson 1988 and we judged Ni 2003 to be at high risk of bias.
Calvo 1998: Blinding and randomisation were referred to, but were not described. Participants were excluded from study entry if they required hospitalisation. No participants failed treatment and all were accounted for. The addition of salbutamol and/or oral steroids may have influenced the response to therapy across the three groups.
Cook 1985: This study is described as a double‐blind trial although the method of double‐blinding is not explicit. Three patients (one from each group) required IV therapy and did not complete the trial. Children of various age groups received different volumes of the medicines in their respective groups, however, there is no explanation of how this was done with the blinding intact.
Guill 1987: This study is described as a double‐blind trial. Randomisation was done for each episode of wheezing, rather than for individual patients. Although the method of double‐blinding is explicit, it is difficult to explain how blinding was preserved when subjects entered into the trial more than once and yet did not receive the same treatment more than once. Ten episodes of wheezing were classified as treatment failure, six of these were in the group which received atropine sulfate only.
Ni 2003: This study is an unblinded trial. No patients withdrew or dropped out. This paper was published in Chinese and translated.
Van Bever 1994: This study is described as a double‐blind trial. Medications were administered from blinded metered dose inhalers. Withdrawals were not reported.
Watson 1988: This study is described as a double‐blind trial although the method of randomisation is not mentioned. No patients withdrew from the study because of the need for an additional bronchodilator. Two children were admitted to hospital at the end of the study because of failure to achieve a clinically significant improvement. These patients were in the group which received ipratropium bromide only.
Incomplete outcome data
Guill 1987 reported ten episodes of wheezing that were classified as treatment failure (two in the group which received metaproterenol only, six in the group which received atropine sulfate only and two in the group which received combination treatment). One study (Cook 1985) reported that three patients (one from each group) required IV therapy and did not complete the trial and hence we excluded the results of these patients from the analysis. Withdrawals were not reported in Van Bever 1994's study. No detailed description was available for outcome measures in one study which was published in Chinese and translated; but no patients withdrew or dropped out (Ni 2003).
Selective reporting
Outcomes measured differed between the studies. Outcome measures in each individual study were reported.
One study (Ni 2003) reported outcome measures as "no symptoms" or "improved symptoms" (shortness of breath, wheeze and hypoxia); no detailed description was available for outcome measures. Ni 2003 reported complete improvement in symptoms in 40 children and partial improvement in symptoms in 22 children in the group treated with salbutamol in combination with ipratropium bromide. However, only 55 children were allocated to this group. This paper was published in Chinese and translated.
Other potential sources of bias
One study (Watson 1988) was supported by a grant from a pharmaceutical company. Two studies (Guill 1987; Van Bever 1994) received pharmaceutical company support for the medications.
Effects of interventions
Only data for anticholinergics versus beta2‐agonists and anticholinergics versus anticholinergics plus beta2‐agonists were available. We entered relevant data into forest plots but were only able to pool data for the outcomes of treatment failure and hospitalisation. We could not pool other data due to divergent outcome measurements, and different types of anticholinergic agents and bronchodilators used in the studies. Results are presented according to comparison and then by outcome, with the primary outcome listed first.
Anticholinergic agents versus beta2‐agonists
We were able to include all six studies (Cook 1985; Guill 1987; Watson 1988; Van Bever 1994; Calvo 1998; Ni 2003) in this intervention. However insufficient data (translated paper) was available from Ni 2003 and hence we did not include data from this paper below.
Primary outcome: treatment failure (analysis 1.1)
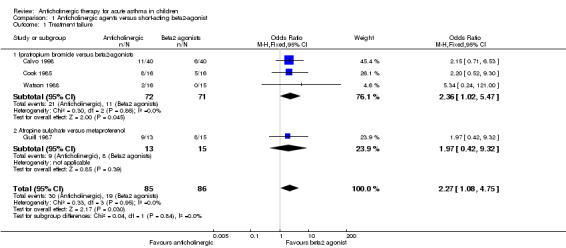
There is variability in the definition of 'treatment failure', although all required additional treatment. One study reported admission data discreetly from treatment failure data (Watson 1988). The other four studies reported data on treatment failure according to their own pre‐defined criteria (see Table 1). In one study (Calvo 1998), we considered treatment failure as those children who were poor responders to bronchodilator therapy (PEF + 4% or less). In another study (Cook 1985), we considered treatment failure as those children who required intravenous therapy as well as those who required repeat nebulizations of medications. In the study of Guill 1987 and colleagues, treatment failure was considered as those children who required repeat nebulizations of medications, those who either worsened after nebulized treatment and required alternative therapy (injectable epinephrine) or improved initially after one or two nebulized treatments but deteriorated within one hour and required hospitalisation. We could pool data from three studies that used similar medications (ipratropium versus beta2‐agonist) (Cook 1985; Watson 1988; Calvo 1998). Pooled analysis revealed a (just) significant difference between the two groups with those who received ipratropium bromide more likely to have treatment failure compared to those on beta2‐agonist (OR 2.36; 95% CI 1.02 to 5.47; Analysis 1.1). The addition of Guill 1987's study (to the forest plot) that used atropine sulphate compared to metaproterenol (9/13 versus 8/15, respectively) further strengthened the efficacy of beta2‐agonists compared to anticholinergic agents (OR 2.27; 95% CI 1.08 to 4.75) as depicted in Figure 2.
1.1. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 1 Treatment failure.
2.
Forest plot of comparison: 1 Anticholinergic agents versus short‐acting beta2‐agonists, outcome: 1.1 Treatment failure.
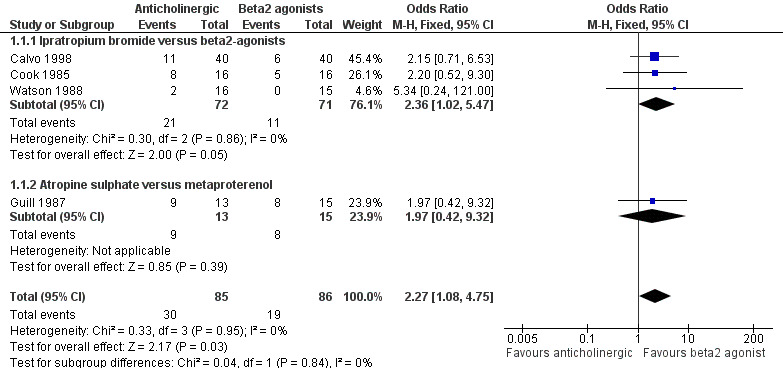
Primary outcome: hospital admissions (analysis 1.2)
Three studies (Guill 1987; Watson 1988; Calvo 1998) reported on this outcome but only two studies had children who required hospitalisation (Guill 1987; Watson 1988). No admissions occurred in the Calvo 1998 study. Pooled data from the two studies (Calvo 1998; Watson 1988) that used similar medications (ipratropium versus beta2‐agonist) showed no significant difference between groups (OR 5.34; 95% CI 0.24 to 121.0). The addition of Guill 1987's study (to the forest plot) that used atropine sulphate versus metaproterenol, revealed a significant difference between the two groups, with those who received anticholinergic agents more likely to result in a hospital admission compared to those on beta2‐agonists (OR 5.50; 95% CI 1.11 to 27.16; Analysis 1.2).
1.2. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 2 Admission to hospital.
Secondary outcome: symptom scores
Guill 1987 and Watson 1988 reported pulmonary index scores (composite scores of several outcome measures). Guill 1987 did not report a significant difference between treatment groups at first nebulisation. Watson 1988 reported that clinical scores improved significantly in all treatment groups at all times (no P values were reported). Calvo 1998 reported data on TAL score from eight measurements over two hours. We only extracted data for the first 30 minutes due to concerns arising over the addition of a known bronchodilator if there was a lack of improvement after 30 minutes. For results taken up to 30 minutes for the three treatment groups, please see Table 2. Significant differences were observed at 15 and 30 minutes for salbutamol versus ipratropium bromide (at 30 minutes: 3.3 (standard deviation (SD) 1.1) versus 4.2 (SD 0.9); P < 0.01). Cook 1985 measured symptoms on an in‐house symptom score (see Table 1). No significant difference was reported between the treatment groups across the two hours of treatment on clinical rating.
2. TAL scores measured in Calvo 1998.
| Treatment group | 0 minutes | 15 minutes | 30 minutes |
| Ipratropium (IP) | 5.6 (SD 0.7) | 5.4 (SD 0.7) | 4.2 (SD 0.9) |
| Salbutamol (SAL) | 5.6 (SD 0.7) | 4.5 (SD 1.0) | 3.3 (SD 1.1) |
| Combination (IP + SAL) | 6.0 (SD 0.8) | 4.3 (SD 1.2) | 2.8 (SD 1.0) |
| P value IP versus SAL | > 0.05 | < 0.01 | < 0.01 |
| P value IP versus IP + SAL | > 0.05 | < 0.01 | < 0.01 |
Secondary outcome: requirement for additional medication
Calvo 1998, Cook 1985 and Guill 1987 measured the requirement for additional treatment in different ways (see Table 1).
Calvo 1998 reported no significant difference in the requirement for additional study medication between children on ipratropium and those on salbutamol (5.3 (SD 1.1) versus 4.7 (SD 1.2); P > 0.05) respectively. Furthermore, there was no significant difference in the requirement for corticosteroids at 60 minutes between children on ipratropium and those on salbutamol (0.3 (SD 0.4) versus 0.2 (SD 0.4) respectively; P > 0.05). There was a significant difference in terms of need for additional bronchodilators in the ipratropium group compared with salbutamol (1.7 (SD 2.1) versus 1.0 (SD 1.8); P < 0.05).
Cook 1985 reported the number of repeat nebulisations required. No statistically significant differences were observed between treatment groups.
Guill 1987 reported the number of treatments required. More participants in the metaproterenol group (7/15) could be discharged after fewer treatments than those in the atropine group (4/13). No P value was reported for the metaproterenol group versus the atropine group.
Secondary outcome: lung function
Data are presented by outcome (PEF and FEV1) and then by study. We have extracted and presented data for outcome assessment at 30 and 120 minutes where possible. We consider these time‐points to be the most clinically relevant in an asthma attack. P values are presented from the published papers; some of these considered data at all time‐points.
PEF (percentage predicted)
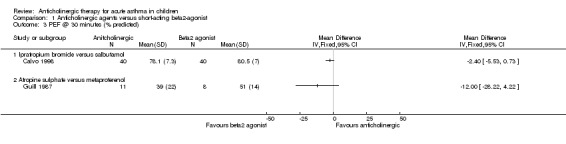
Calvo 1998 reported no significant difference between salbutamol (80.5 (SD 7)) and ipratropium (78.1 (SD 7.3)); P > 0.05 at 30 minutes (Analysis 1.3). We did not extract subsequent data due to the potential for confounding by the introduction of concomitant therapy in all groups.
1.3. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 3 PEF @ 30 minutes (% predicted).
Guill 1987 reported lung function at 20 to 30 minutes after treatments were administered. We extracted data for lung function taken after the first administration which corresponds approximately to 30 minute data. We did not observe any significant differences between the groups at 30 (Analysis 1.3) minutes. We did not include data extracted for subsequent lung function measurement in the review as they represented assessment 20 to 30 minutes after a second treatment, and 40 to 60 minutes after the first treatment.
FEV1
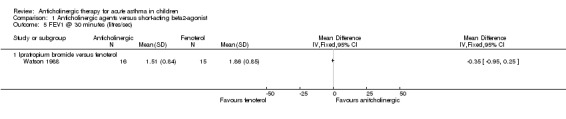
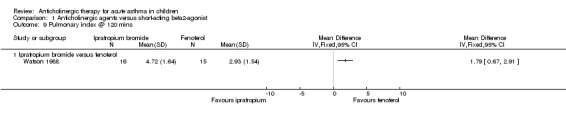
Watson 1988 reported non‐significant differences when data were analysed as absolute change in FEV1 and percentage change from baseline. When Watson 1988 and colleagues analysed data as change in percentage predicted, fenoterol was significantly better than ipratropium alone (P = 0.02, at each time‐point).
Absolute scores at 30 minutes were: ipratropium group 1.51 (SD 0.84) and fenoterol group 1.86 (SD 0.85) (Analysis 1.5).
1.5. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 5 FEV1 @ 30 minutes (litres/sec).
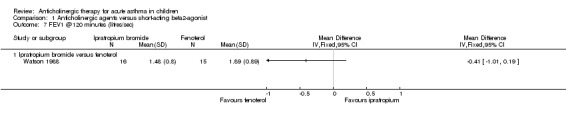
Absolute scores at 120 minutes were: ipratropium group 1.48 (SD 0.8) and fenoterol group 1.89 (SD 0.89) (Analysis 1.7).
1.7. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 7 FEV1 @120 minutes (litres/sec).
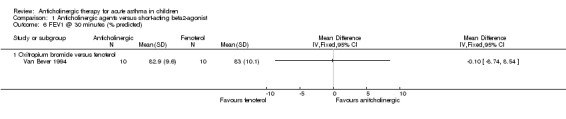
Van Bever 1994 reported lung function at 20 minutes after treatments were administered. A significant improvement in FEV1 in both groups (i.e. children on oxitropium bromide and those on fenoterol) compared to baseline (82.9 SD (9.6); P 0.003). A significant improvement in FEV1 was observed after administration of 200 mcg oxitropium bromide or fenoterol and subsequent administration of 400 mcg of fenoterol (87.2 (SD 11.0); P 0.03).
FEF25‐75
One study (Watson 1988) reported results for FEF25‐75 for the comparison of ipratropium with fenoterol. There was a significant difference between fenoterol and ipratropium in FEF25‐75 whether considered as absolute change or as change in percentage predicted (P < 0.05, no time‐point specified).
Absolute scores at 30 minutes were: ipratropium group 0.92 (SEM 0.15) and fenoterol group 1.40 (SEM 0.22).
Absolute scores at 120 minutes were: ipratropium group 0.94 (SEM 0.13) and fenoterol group 1.56 (SEM 0.25).
Secondary outcome: pulse oximetry
Watson 1988 reported that there was no significant difference between the two groups for pulse oximetry. However, there was a significant improvement in oxygen saturation in the fenoterol group at 30 minutes which continued throughout the study (no P value reported). The improvement in oxygen saturation for ipratropium alone was not statistically significant at 30 minutes, but was so at 60 minutes and thereafter (no P values reported).
Secondary outcome: withdrawals
No withdrawals occurred in three studies (Watson 1988; Calvo 1998; Ni 2003). Three children dropped out from one study (Cook 1985; one from each group). Guill 1987 reported the number of treatment failures. Because the primary outcome was the number of additional treatments required before clinical improvement was observed, participants only contributed data for subsequent clinical assessment if they had not improved subsequent to the previous treatment; withdrawals were not therefore measured. Van Bever 1994 did not report on withdrawals.
Secondary outcome: side effects
All studies reported no significant differences in side effects between the participants.
Anticholinergic agents versus combination of anticholinergic agents + beta2‐agonists
Primary outcome: treatment failure (analysis 2.1)
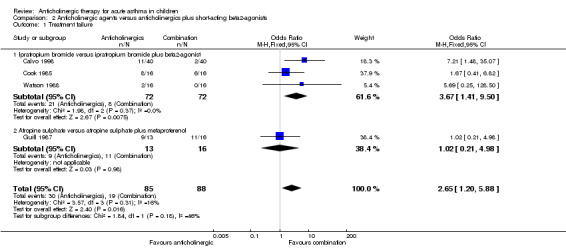
Four studies reported data on treatment failure according to their own pre‐defined criteria (see Table 1). In one study (Calvo 1998), we considered treatment failure as those children who were poor responders to bronchodilator therapy (PEF + 4% or less). In another study (Cook 1985), we considered treatment failure as those children who required intravenous therapy as well as those who required repeat nebulizations of medications. In one study (Guill 1987), we considered treatment failure as those children who required repeat nebulizations of medications, those who either worsened after nebulized treatment and required alternative therapy (injectable epinephrine) or improved initially after one or two nebulized treatments but deteriorated within one hour and required hospitalization.We were able to pool data from three studies that used similar medications (ipratropium versus beta2‐agonist plus ipratropium) (Cook 1985; Watson 1988; Calvo 1998). A significant difference between anticholinergic and combination therapy was observed (OR 3.67; 95% CI 1.41 to 9.50; Analysis 2.1) i.e. those who received ipratropium alone were more likely to have treatment failure compared to those on combination therapy.
2.1. Analysis.
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 1 Treatment failure.
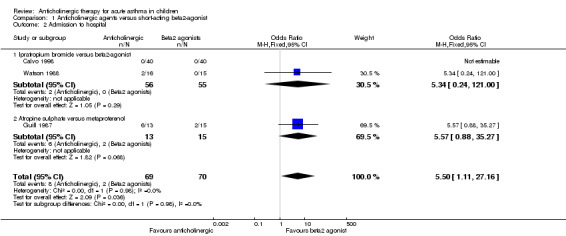
Guill 1987 reported that 2 out of 16 participants failed treatment in the combination (atropine and metaproterenol) group (P < 0.02) versus atropine sulfate alone. Combining these studies (anticholinergics alone versus anticholinergic agents + beta2‐agonists), those who received anticholinergics alone were significantly more likely to experience treatment failure compared to those who received anticholinergic + beta2‐agonists, Figure 3 (OR 2.65; 95% CI 1.20 to 5.88).
3.
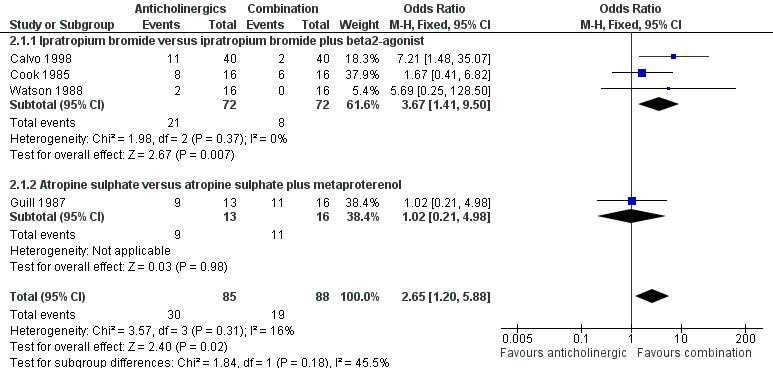
Forest plot of comparison: 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, outcome: 2.1 Treatment failure.
Primary outcome: admission to hospital (analysis 2.2)
Three studies (Guill 1987; Watson 1988; Calvo 1998) reported on this outcome but only two studies had children who required hospitalisation (Guill 1987; Watson 1988). Pooled data from the two studies that used similar medications (ipratropium versus beta2‐agonist plus ipratropium) showed no significant difference between groups (OR 5.69; 95% CI 0.25 to 128.5; Analysis 2.2). The addition to the forest plot of Guill 1987's study that used atropine sulfate versus atropine sulfate and metaproterenol, revealed a significant difference between the two groups with those who received anticholinergic agents more likely to result in a hospital admission compared to those on combination therapy (OR 5.90; 95% CI 1.20 to 29.05).
2.2. Analysis.
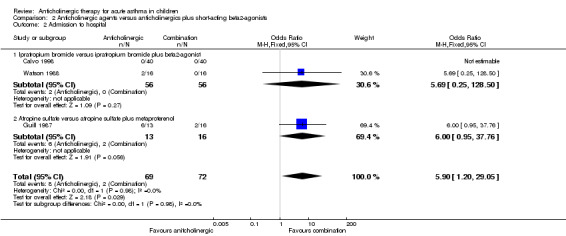
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 2 Admission to hospital.
Secondary outcome: symptom scores
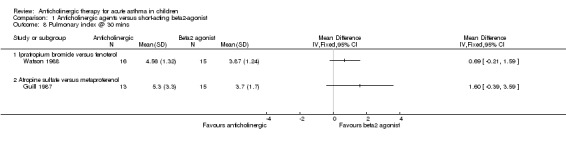
Guill 1987 and Watson 1988 reported pulmonary index scores. Guill 1987 did not report a significant difference between treatment groups at first nebulisation. Watson 1988 reported that clinical scores improved significantly in all treatment groups at all times (no P values were reported). Calvo 1998 reported data on TAL score from eight measurements over two hours. We extracted data only for the first 30 minutes due to concerns arising over the addition of a known bronchodilator if there was a lack of improvement after 30 minutes. For results taken up to 30 minutes for the three treatment groups, please see Table 2. Significant differences were observed at 15 and 30 minutes for combination therapy versus ipratropium (at 30 minutes 2.8 (SD 1.0) versus 4.2 (SD 0.9); P < 0.01). Cook 1985 measured symptoms on an in‐house symptom score (see Table 1). No difference was reported between the treatment groups across the two hours of treatment on clinical rating.
Secondary outcome: requirement for additional medication
Calvo 1998, Cook 1985 and Guill 1987 measured the requirement for additional treatment in different ways (see Table 1). Calvo 1998 reported a significant difference between combination therapy and ipratropium in terms of study medication requirement (3.7 (SD 1.1) versus 5.3 (SD 1.1) respectively; P < 0.01) and bronchodilator requirement (0.5 (SD 1.3) versus 1.7 (SD 2.1) respectively; P < 0.01). There was a non‐significant difference between combination and ipratropium in terms of corticosteroid requirement (0.1 (SD 0.3) versus 0.3 (SD 0.4) respectively; P >0.05). Cook 1985 reported the number of repeat nebulisations required. No statistically significant differences were observed between treatment groups. Guill 1987 reported the number of treatments required. More participants in the metaproterenol and combination groups could be discharged after fewer treatments than those in the atropine group (atropine group 4/13; combination group 5/16). No P values were reported for the combination group versus atropine group.
Secondary outcome: lung function
Data are presented by outcome (PEF and FEV1) and then by study. We have extracted and presented data for outcome assessment at 30 and 120 minutes where possible. We consider these time‐points to be the most clinically relevant in an asthma attack. P values are presented from the published papers; some of these considered data at all time‐points.
PEF (percentage predicted)
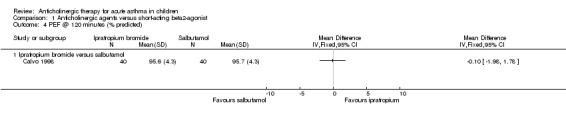
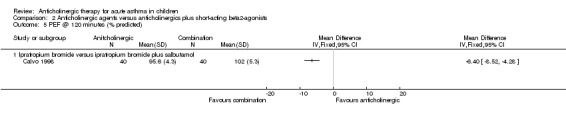
Two studies (Guill 1987; Calvo 1998) reported PEF percentage predicted. Calvo 1998 reported a significant difference between the combination (85.1 (SD 6.7)) and ipratropium groups (78.1 (SD 7.3)); P < 0.01 at 30 minutes (Analysis 2.4). We did not extract subsequent data due to the potential for confounding by the introduction of concomitant therapy in all groups. Guill 1987 reported lung function at 20 to 30 minutes after treatments were administered. We extracted data for lung function taken after the first administration which corresponds approximately to 30 minute data. No significant differences were observed between the groups. We did not include data extracted for subsequent lung function measurement in the review as they represented assessment 20 to 30 minutes after a second treatment, and 40 to 60 minutes after the first treatment.
2.4. Analysis.
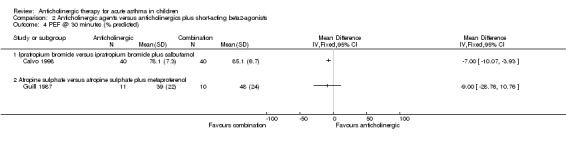
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 4 PEF @ 30 minutes (% predicted).
FEV1
Watson 1988 reported a significant difference between combination and ipratropium alone in terms of absolute change, (P = 0.005, all time‐points), change in percentage predicted (P = 0.0002, all time‐points; Analysis 2.6) and percentage change from baseline (P = 0.002, all time‐points). All data were presented graphically. Absolute scores at 30 minutes were: combination group 1.94 (SD 0.93) and ipratropium group 1.51 (SD 0.84) (Analysis 2.6). Absolute scores at 120 minutes were: combination group 2.11 (SD 1.05) and ipratropium group 1.48 (SD 0.8) (Analysis 2.7).
2.6. Analysis.
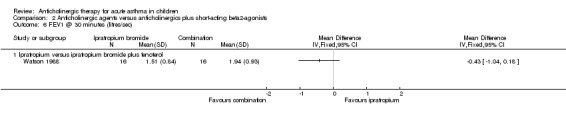
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 6 FEV1 @ 30 minutes (litres/sec).
2.7. Analysis.
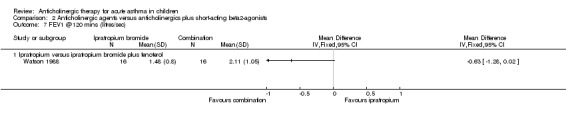
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 7 FEV1 @120 mins (litres/sec).
FEF25‐75
One study (Watson 1988) reported this. A significant difference in FEF25‐75 was reported between the combination and ipratropium group (P < 0.005, no time‐point specified). Absolute scores at 30 minutes were: combination group 1.57 (SEM: 0.25) and ipratropium group: 0.92 (SEM 0.15). Absolute scores at 120 minutes were: combination group 1.82 (SEM: 0.3) and ipratropium group: 0.94 (SEM 0.13).
Secondary outcome: pulse oximetry
Watson 1988 reported that there were no significant differences between the three groups. However, there was a significant improvement in oxygen saturation in the combination and fenoterol groups at 30 minutes which continued throughout the study (no P values reported).
Secondary outcome: withdrawals
No withdrawals occurred in three studies (Watson 1988; Calvo 1998; Ni 2003). Three children dropped out from one study (Cook 1985; one from each group). Guill 1987 reported the number of treatment failures. Because the primary outcome was the number of additional treatments required before clinical improvement was observed, participants only contributed data for subsequent clinical assessment if they had not improved subsequent to the previous treatment; withdrawals were not therefore measured. Van Bever 1994 also did not report on withdrawals.
Secondary outcome: side effects
All studies reported no significant differences in side effects between the participants.
Discussion
In this review, we evaluated the trials that studied the efficacy of ipratropium bromide given alone or in combination with beta2‐agonists (compared to a control of beta2‐agonists) for acute asthma in children aged over two years. Despite an extensive and thorough literature search in which we found hundreds of papers examining anticholinergic drugs, only seven studies (one paper was an abstract from a conference proceedings of a paper (Van Bever 1994)) from six trials met the inclusion criteria for the review.
Summary of main results
We found that inhaled anticholinergic agents as single agent bronchodilators were less efficacious (i.e. led to more treatment failure) than beta2‐agonists in children over the age of two years with acute asthma exacerbations. Anticholinergics were also less efficacious (i.e. led to more treatment failure) than anticholinergics combined with beta2‐agonists. In this review, data on clinical scores/symptoms that were measured on different scales were variable but all generally showed that ipratropium bromide used alone was less efficacious compared to beta2‐agonists or combined with beta2‐agonists. Also, individual trials reported that lung function was superior in the combination group when compared to anticholinergic agents.
In our review, there was no significant increase in the occurrence of tachycardia, tremor, mydriasis or dryness of oral mucous membranes observed among participants treated with anticholinergic agents. Ipratropium bromide has no or very little systemic toxicity. Another significant advantage to ipratropium bromide in the critically ill asthma patient is the lack of increase in heart rate, which does occur with beta2‐agonist use (Cugell 1986). The only remarkable reported side effect in the literature is the inhibition of salivary secretions at high doses. When nebulised, ipratropium is very unlikely to affect urinary flow or intraocular tension, and possible effects on the eye (i.e. glaucoma) can be prevented by using a mouthpiece during nebulisation. Although data is not available in children, the speed of onset of effect is reported in adults with airway disease to be 3 to 30 minutes with up to 50% of the response occurring in three minutes and 80% in 30 minutes, with a peak bronchodilator effect observed within one to two hours, and duration of action of up to approximately six hours (Gross 1988).
Overall completeness and applicability of evidence
Our thorough systematic search for published and unpublished trials resulted in identification of important trials. We could only extract data from six trials. Despite the small number of studies, we conclude from the studies that inhaled anticholinergic drugs as single agent bronchodilators were less efficacious than beta2‐agonists and anticholinergics combined with beta2‐agonists.
Quality of the evidence
This systematic review was limited by the quality of existing data. In addition, there was clinical heterogeneity amongst the trials and we could not pool some data due to divergent outcome measurements and different types of anticholinergic agents and bronchodilators used in the studies. The number (i.e. six trials) and size of studies pooled were small. There were limited data on hospital admissions.
Potential biases in the review process
The studies were generally small with potential risk of bias as shown in Figure 1.
Agreements and disagreements with other studies or reviews
Inhaled anticholinergics in combination with beta2‐agonists is now the standard recommended treatment for children with acute moderate to severe asthma exacerbations.
Authors' conclusions
Implications for practice.
In children over the age of two years with acute asthma exacerbations, inhaled anticholinergic drugs as single agent bronchodilators were less efficacious than beta2‐agonists. Inhaled anticholinergics on their own were also less efficacious than anticholinergics combined with beta2‐agonists. Thus in children over the age of two years with acute asthma exacerbations, inhaled anticholinergics alone are not appropriate as a single agent. None of the major asthma guidelines currently recommend inhaled anticholinergics as a single agent and our review supports this. The use of anticholinergics was not found to be associated with significant side effects such as tachycardia, tremor, mydriasis or dryness of oral mucous membranes.
Implications for research.
Inhaled anticholinergics combined with beta2‐agonists is now the standard recommended treatment in guidelines for children with acute moderate to severe asthma exacerbations. Thus, in light of our conclusion above, we do not recommend any further trials comparing inhaled anticholinergics as a single agent in children with acute asthma exacerbations.
Notes
None relevant.
Acknowledgements
We thank Elizabeth Stovold and Susan Hansen from the Cochrane Airways Group for performing the searches and obtaining the relevant articles. We also thank Toby Lasserson for the support in the protocol development and review of the manuscript. We also thank the Australian Cochrane Airways Group for providing Dr Teoh a scholarship.
Appendices
Appendix 1. Sources and search methods for the Cochrane Airways Group Specialised Register (CAGR)
Electronic searches: core databases
| Database | Frequency of search |
| MEDLINE (Ovid) | Weekly |
| EMBASE (Ovid) | Weekly |
| CENTRAL (The Cochrane Library) | Quarterly |
| PsycINFO (Ovid) | Monthly |
| CINAHL (EBSCO) | Monthly |
| AMED (EBSCO) | Monthly |
Handsearches: core respiratory conference abstracts
| Conference | Years searched |
| American Academy of Allergy, Asthma and Immunology (AAAAI) | 2001 onwards |
| American Thoracic Society (ATS) | 2001 onwards |
| Asia Pacific Society of Respirology (APSR) | 2004 onwards |
| British Thoracic Society Winter Meeting (BTS) | 2000 onwards |
| Chest Meeting | 2003 onwards |
| European Respiratory Society (ERS) | 1992, 1994, 2000 onwards |
| International Primary Care Respiratory Group Congress (IPCRG) | 2002 onwards |
| Thoracic Society of Australia and New Zealand (TSANZ) | 1999 onwards |
MEDLINE search strategy used to identify trials for the CAGR
Asthma search
1. exp Asthma/
2. asthma$.mp.
3. (antiasthma$ or anti‐asthma$).mp.
4. Respiratory Sounds/
5. wheez$.mp.
6. Bronchial Spasm/
7. bronchospas$.mp.
8. (bronch$ adj3 spasm$).mp.
9. bronchoconstrict$.mp.
10. exp Bronchoconstriction/
11. (bronch$ adj3 constrict$).mp.
12. Bronchial Hyperreactivity/
13. Respiratory Hypersensitivity/
14. ((bronchial$ or respiratory or airway$ or lung$) adj3 (hypersensitiv$ or hyperreactiv$ or allerg$ or insufficiency)).mp.
15. ((dust or mite$) adj3 (allerg$ or hypersensitiv$)).mp.
16. or/1‐15
Filter to identify RCTs
1. exp "clinical trial [publication type]"/
2. (randomised or randomised).ab,ti.
3. placebo.ab,ti.
4. dt.fs.
5. randomly.ab,ti.
6. trial.ab,ti.
7. groups.ab,ti.
8. or/1‐7
9. Animals/
10. Humans/
11. 9 not (9 and 10)
12. 8 not 11
The MEDLINE strategy and RCT filter are adapted to identify trials in other electronic databases
Appendix 2. CENTRAL search strategy
#1 MeSH descriptor Asthma explode all trees
#2 (asthma*)
#3 (wheez*)
#4 MeSH descriptor Respiratory Sounds, this term only
#5 MeSH descriptor Bronchial Spasm, this term only
#6 (bronchospas*)
#7 (bronch* near/3 spasm*)
#8 (bronchoconstrict*)
#9 MeSH descriptor Bronchoconstriction, this term only
#10 (bronch* near/3 constrict*)
#11 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10)
#12 MeSH descriptor Cholinergic Antagonists explode all trees
#13 anticholinergic* or anti‐cholinergic* or cholinergic* or muscarinic* or antimuscarinic or ipratropium or tiotropium or atropine or atrovent or oxitropium or Sch1000 or duovent
#14 (#12 OR #13)
#15 (#11 AND #14)
#16 MeSH descriptor Child explode all trees
#17 MeSH descriptor Infant explode all trees
#18 MeSH descriptor Adolescent explode all trees
#19 MeSH descriptor Pediatrics explode all trees
#20 child* or paediat* or pediat* or infan* or toddler* or bab* or young* or preschool* or "pre school*" or pre‐school* or newborn* or "newborn*" or new‐born* or neo‐nat* or neonat*
#21 (#16 OR #17 OR #18 OR #19 OR #20)
#22 (#15 AND #21)
Data and analyses
Comparison 1. Anticholinergic agents versus short‐acting beta2‐agonist.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment failure | 4 | 171 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.27 [1.08, 4.75] |
| 1.1 Ipratropium bromide versus beta2‐agonists | 3 | 143 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.36 [1.02, 5.47] |
| 1.2 Atropine sulphate versus metaproterenol | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.97 [0.42, 9.32] |
| 2 Admission to hospital | 3 | 139 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.50 [1.11, 27.16] |
| 2.1 Ipratropium bromide versus beta2‐agonist | 2 | 111 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.34 [0.24, 121.00] |
| 2.2 Atropine sulphate versus metaproterenol | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.57 [0.88, 35.27] |
| 3 PEF @ 30 minutes (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 Ipratropium bromide versus salbutamol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Atropine sulphate versus metaproterenol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 PEF @ 120 minutes (% predicted) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 Ipratropium bromide versus salbutamol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 FEV1 @ 30 minutes (litres/sec) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 Ipratropium bromide versus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 FEV1 @ 30 minutes (% predicted) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 Oxitropium bromide versus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 FEV1 @120 minutes (litres/sec) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1 Ipratropium bromide versus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Pulmonary index @ 30 mins | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.1 Ipratropium bromide versus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Atropine sulfate versus metaproterenol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 Pulmonary index @ 120 mins | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9.1 Ipratropium bromide versus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
1.4. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 4 PEF @ 120 minutes (% predicted).
1.6. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 6 FEV1 @ 30 minutes (% predicted).
1.8. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 8 Pulmonary index @ 30 mins.
1.9. Analysis.
Comparison 1 Anticholinergic agents versus short‐acting beta2‐agonist, Outcome 9 Pulmonary index @ 120 mins.
Comparison 2. Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment failure | 4 | 173 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.65 [1.20, 5.88] |
| 1.1 Ipratropium bromide versus ipratropium bromide plus beta2‐agonist | 3 | 144 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.67 [1.41, 9.50] |
| 1.2 Atropine sulphate versus atropine sulphate plus metaproterenol | 1 | 29 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.21, 4.98] |
| 2 Admission to hospital | 3 | 141 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.90 [1.20, 29.05] |
| 2.1 Ipratropium bromide versus ipratropium bromide plus beta2‐agonist | 2 | 112 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.69 [0.25, 128.50] |
| 2.2 Atropine sulfate versus atropine sulfate plus metaproterenol | 1 | 29 | Odds Ratio (M‐H, Fixed, 95% CI) | 6.0 [0.95, 37.76] |
| 3 Participants requiring no repeat nebulisation | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 Moderate‐severe acute asthma | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 PEF @ 30 minutes (% predicted) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 Ipratropium bromide versus ipratropium bromide plus salbutamol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Atropine sulphate versus atropine sulphate plus metaproterenol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 PEF @ 120 minutes (% predicted) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 Ipratropium bromide versus ipratropium bromide plus salbutamol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 FEV1 @ 30 minutes (litres/sec) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 Ipratropium versus ipratropium bromide plus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 FEV1 @120 mins (litres/sec) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1 Ipratropium versus ipratropium bromide plus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Pulmonary index @ 30 mins | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8.1 Ipratropium bromide versus ipratropium bromide plus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 Atropine sulfate versus atropine sulfate plus metaproterenol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 Pulmonary index @ 120 mins | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9.1 Ipratropium bromide versus ipratropium bromide plus fenoterol | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
2.3. Analysis.
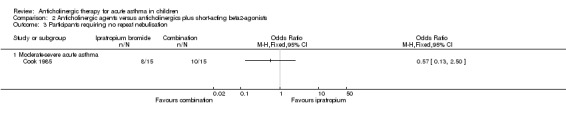
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 3 Participants requiring no repeat nebulisation.
2.5. Analysis.
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 5 PEF @ 120 minutes (% predicted).
2.8. Analysis.
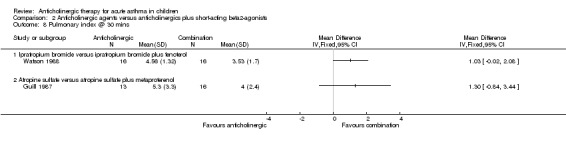
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 8 Pulmonary index @ 30 mins.
2.9. Analysis.
Comparison 2 Anticholinergic agents versus anticholinergics plus short‐acting beta2‐agonists, Outcome 9 Pulmonary index @ 120 mins.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Calvo 1998.
| Methods | Randomised, double‐blind parallel group trial. Method of randomisation not reported Outpatient Setting |
|
| Participants | N = 120 (Group 1: 40; Group 2: 40; Group 3: 40). 73 M/47 F. Mean age 7.3 years (age range: 5 to 14 years). No withdrawals occurred and all participants were accounted for
|
|
| Interventions | All treatments were administered by aerochamber
2 inhalations 4 times in first hour, 2 inhalations 3 times in second hour |
|
| Outcomes | PEF; TAL score; need for additional treatment (salbutamol and oral steroids) | |
| Notes | Trial protocol allowed for addition of salbutamol (100 mcg per inhalation, 2 inhalations after each control) to trial medicines if participants showed no response (clinical or PEF) at 30 minutes or corticosteroid therapy at 60 minutes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
Cook 1985.
| Methods | Randomised double‐blind parallel group trial. Method of randomisation not reported Emergency Department setting No intention to treat population |
|
| Participants | N = 48 (Group 1: 16; Group 2: 16; Group 3: 16). 26 M/22 F. Mean age 6.6 years (age range 18 months to 12 years). 3 withdrawals due to requirement of IV therapy (1 from each group)
|
|
| Interventions | All treatments were administered via a Hudson nebuliser driven by oxygen (flow rate 8 L/min)
Duration 2 hours. Repeat nebulisations at 2‐hourly intervals until stable enough to return to inhaled or oral medication |
|
| Outcomes | Repeat nebulisation; pulse rate; respiratory rate; clinical rating of wheeze; air entry; respiratory distress; overall index of response to treatment | |
| Notes | Plotnick and Ducharme contacted trialists and established that allocation concealment was adequate. Different volumes of trial medication were given according to age of the participants in each treatment group. The trial was described as 'double‐blind' and it was not reported how the blinding of the trialists to the treatment was maintained |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Low risk | All doses administered blind |
Guill 1987.
| Methods | Randomised double‐blind parallel group trial. Method of randomisation: computer‐generated random numbers table Emergency department or outpatient setting |
|
| Participants | N = 35 with 44 episodes of acute asthma (Group 1: 15; Group 2: 13; Group 3: 16) 26 M/18 F; age range: 13 months to 13 years |
|
| Interventions | All treatments were administered via a Hudson 1700 updraft nebuliser and paediatric face mask attached with standard oxygen tubing to a Pulmo‐Aid compressor
Three doses of nebulised medicines were administered 20 to 30 minutes apart |
|
| Outcomes |
|
|
| Notes | Computer generated random numbers were used for each episode rather than for individual patients | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated random numbers |
| Allocation concealment (selection bias) | Low risk | Randomly assigned in a double‐blind manner |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded |
Ni 2003.
| Methods | Randomised unblinded parallel group trial. Method of randomisation not reported Inpatient setting |
|
| Participants | N = 141 (Group 1: 55; Group 2: 48; Group 3: 38) No withdrawals occurred and all participants were accounted for 75 M/66 F Age range: 1 to 12 years
|
|
| Interventions | All treatments were administered via a nebuliser
Nebulised medications were administered 2 to 4 times a day |
|
| Outcomes | No symptoms or improved symptoms (shortness of breath, wheeze and hypoxia) | |
| Notes | Translated paper | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details |
| Allocation concealment (selection bias) | Unclear risk | No details |
| Blinding (performance bias and detection bias) All outcomes | High risk | Not double‐blinded |
Van Bever 1994.
| Methods | Randomised double‐blind parallel group trial. Method of randomisation: computerised random function choosing 10 numbers from 1 to 20, subsequently open study design Setting not reported |
|
| Participants | All treatments were administered via blinded metered dose inhalers with aeroscopic N = 20; 15 M/5 F Mean age: 12.7 years (age range: 4.9 to 15.1 years)
|
|
| Interventions |
Subsequently all patient received 400 mcg fenoterol in an open label study |
|
| Outcomes | Lung function: FEV1; VC; MEF50; MEF25; medication side effects | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computerised random numbers |
| Allocation concealment (selection bias) | Unclear risk | No details |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Blinded metered dose inhalers |
Watson 1988.
| Methods | Randomised double‐blind parallel group trial. Method of randomisation not reported Setting not reported |
|
| Participants | N = 47 (Group 1: 16; Group 2: 15; Group 3: 16) Age range: 6 to 17 years
|
|
| Interventions |
All treatments were administered via a Hudson nebuliser driven by 7 L/min of room air. Two doses of inhalations were given 60 minutes apart |
|
| Outcomes | Clinical scores at 30, 60, 90 and 120 min
Oxygen saturation at 30, 60, 90 and 120 min
Spirometry at 30, 60, 90 and 120 min and after nebulised salbutamol Medication side effects |
|
| Notes | No mention of the method of randomisation At end of study, albuterol 0.5% (5000 mcg/mL) (i.e. 0.02 mL/kg (100 mcg/kg)), max 1 mL (5000 mcg), diluted to 2 mL with normal saline) was administered in an open fashion to assess for possible additional bronchodilatation |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
F: female; FEV1: forced expiratory volume in the first second; IV: intravenous; M: male; mcg: micrograms; MEF50: maximal expiratory flow at 50% of vital flow capacity; MEF25: maximal expiratory flow at 25% of vital flow capacity; MDI: metered dose inhaler; PEF: peak expiratory flow; TAL: a clinical scoring system based on several markers such as respiratory rate, wheezing and cyanosis (the scale runs from 0 to 12, where 12 indicates a very severe illness); VC: vital capacity.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Beck 1985 | RCT: Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| BenitoFernandez 2000 | RCT: Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Bratteby 1986 | Non‐RCT and chronic asthma. Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Browne 2002 | Control group did not fulfil criteria. RCT: Beta2‐agonist compared with combination anticholinergic and beta‐agonist therapy |
| Craven 2001 | Control group did not fulfil criteria. RCT: Beta2‐agonist compared with combination anticholinergic and beta‐agonist therapy |
| De Stefano 1990 | Chronic asthma. Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Ducharme 1998 | Control group did not fulfil criteria. RCT: Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Ferres 1988 | Children were aged less than 1 year |
| Goggin 2001 | Control group did not fulfil criteria. RCT: Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Hayday 2002 | Control group did not fulfil criteria. RCT: Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Iramain 2011 | Control group did not fulfil criteria. RCT:‐ Beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Lew 1990 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta‐agonist therapy |
| Lin 1978 | RCT: Combination therapy in non‐acute asthma |
| Mallol 1987 | RCT: Infants with acute wheezing |
| Mirsadraee 2009 | RCT: Adult study |
| Monge 2000 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Pulejo 1986 | Control group did not fulfil criteria. Double‐blind study: Combination anticholinergic and beta2‐agonist (duovent) therapy compared with placebo |
| Qureshi 1997 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Qureshi 1998 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Rayner 1987 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Reisman 1988 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Schuh 1995 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Storms 1986 | RCT: Chronic asthma |
| Storr 1986 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Timsit 2002 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
| Ulrik 1992 | Chronic asthma |
| Ward 1981 | Non‐RCT: mainly adult study |
| Ward 1985 | RCT: mainly adult study |
| Yeung 1980 | Exercise induced asthma |
| Youngchaiyud 1989 | RCT: adult study |
| Zimmerman 1984 | RCT: Chronic asthma |
| Zorc 1999 | Control group did not fulfil criteria. RCT: beta2‐agonist compared with combination anticholinergic and beta2‐agonist therapy |
RCT: randomised controlled trial
Differences between protocol and review
We subgrouped the data by anticholinergic type. We added withdrawals and requirement for additional medication as secondary outcomes and pooled the data. We removed parent and patient perceptions and physician assessment as outcomes as they are not clearly defined outcomes.
Contributions of authors
The original protocol was written by Satish Bangalore, Anna Bara and Nicola McDonald. The protocol was revised prior to commencing the review by Laurel Teoh (LT) and Anne Chang (AC).
LT and AC wrote the review and independently selected, reviewed, and extracted the data from the papers. All authors reviewed the submitted review.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Australian Cochrane Airway Scholarship, Australia.
Support to LT
-
National Health and Medical Research Council (NHMRC), Australia.
Fellowship for AC (grant number 545216)
Declarations of interest
None known.
New
References
References to studies included in this review
Calvo 1998 {published data only}
- Calvo GM, Calvo AM, Marin HF, Moya GJ. Is it useful to add an anticholinergic treatment to ß2‐adrenergic medication in acute asthma attack?. Journal of Investigational Allergology and Clinical Immunology 1998;8(1):30‐4. [PubMed] [Google Scholar]
Cook 1985 {published data only}
- Cook JJ, Ferguson DM, Dawson KP. Ipratropium and fenoterol in the treatment of acute asthma. Pharmatherapeutica 1985;4(6):383‐6. [PubMed] [Google Scholar]
Guill 1987 {published data only}
- Guill MF, Maloney MJ, DuRant RH. Comparison of inhaled metaproterenol, inhaled atropine sulfate, and their combination in treatment of children with acute asthma. Annals of Allergy 1987;59:367‐71. [PubMed] [Google Scholar]
Ni 2003 {published data only}
- Ni SF, Yao WJ. Combined application of salbutamol and ipratropium bromide in the treatment of bronchial asthma in children. Herald of Medicine 2003;22(2):96‐7. [Google Scholar]
Van Bever 1994 {published data only}
- Bever HP, Desager KN, Pauwels JH, Vermeire PA. Comparison of the bronchodilating effect of oxitropium bromide and fenoterol in asthmatic children. European Journal of Pediatrics 1994;153:604‐6. [DOI] [PubMed] [Google Scholar]
Watson 1988 {published data only}
- Wade TA, Watson MD, Becker AB, Simons FER. Comparison of ipratropium solution, fenoterol solution, and their combination administered by nebulizer and face mask to children with acute asthma. Journal of Allergy and Clinical Immunology 1988;82:1012‐8. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Beck 1985 {published data only}
- Beck R, Robertson C, Galdes‐Sebaldt M, Levison H. Combined salbutamol and ipratropium bromide by inhalation in the treatment of severe acute asthma. Journal of Pediatrics 1985;107(4):605‐8. [DOI] [PubMed] [Google Scholar]
BenitoFernandez 2000 {published data only}
- Benito Fernandez J, Mintegui Raso S, Sanchez Echaniz J, Vazquez Ronco MA, Pijoan Zubizarreta JI. Efficacy of early administration of nebulised ipratropium bromide in children with acute asthma attack [Eficacia de la administracion precoz de bromuro de ipratropio nebulizado en ninos con crisis asmatica]. Anales Espanoles De Pediatria Sept 2000;53(3):217‐22. [PubMed] [Google Scholar]
Bratteby 1986 {published data only}
- Bratteby LE, Foucard T, Lӧnnerholm G. Combined treatment with ipratropium bromide and beta‐2‐adrenoceptor agonists in childhood asthma. European Journal of Respiratory Disease 1986;68(4):239‐47. [PubMed] [Google Scholar]
Browne 2002 {published data only}
- Browne GJ, Trieu L, Asperen P. Randomized, double‐blind, placebo‐controlled trial of intravenous salbutamol and nebulized ipratropium bromide in early management of severe acute asthma in children presenting to an emergency department. Critical Care Medicine 2002;30(2):448‐53. [DOI] [PubMed] [Google Scholar]
Craven 2001 {published data only}
- Craven D, Kercsmar CM, Meyers TR, O'Riordan MA, Golonka G, Moore S. Ipratropium bromide plus nebulized albuterol for the treatment of hospitalized children with acute asthma. Journal of Pediatrics 2001;138(1):51‐8. [DOI] [PubMed] [Google Scholar]
De Stefano 1990 {published data only}
- DeStefano G, Bonetti S, Bonizzatto C, Valletta EA, Piacentini GL, Boner AL. Additive effect of albuterol and ipratropium bromide in the treatment of bronchospasm in children. Annals of Allergy 1990;65(4):260‐2. [PubMed] [Google Scholar]
Ducharme 1998 {published data only}
- Ducharme FM, Davis GM. Randomized controlled trial of ipratropium bromide and frequent low doses of Salbutamol in the management of mild and moderate acute pediatric asthma. Journal of Pediatrics 1998;133(4):479‐85. [DOI] [PubMed] [Google Scholar]
Ferres 1988 {published data only}
- Ferres J, Guinovart G, Carreras G, Julia A, Mangues MA, Farre R. Inhaled salbutamol versus combined fenoterol and ipratropium bromide treatment in childhood acute asthma. 7th Congress of the European Society of Pneumology; 1988 September 5‐9; Budapest. 1988; Vol. 1 Suppl:2336s.
Goggin 2001 {published data only}
- Goggin N, Macarthur C, Parkin PC. Randomized trial of the addition of ipratropium bromide to albuterol and corticosteroid therapy in children hospitalized because of an acute asthma exacerbation. Archives of Pediatrics and Adolescent Medicine 2001;155(12):1329‐34. [DOI] [PubMed] [Google Scholar]
Hayday 2002 {published data only}
- Hayday K, Stevermer JJ. In children hospitalized for asthma exacerbation, does adding ipratropium bromide to albuterol and corticosteroids improve outcome?. Journal of Family Pracitice 2002;51(3):280. [PubMed] [Google Scholar]
Iramain 2011 {published data only}
- Iramain R, Lopez‐Herce J, Coronel J, Spitters C, Guggiari J, Bogado N. Inhaled salbutamol plus ipratropium in moderate and severe asthma crises in children. Journal of Asthma 2011;48(3):298‐303. [DOI] [PubMed] [Google Scholar]
Lew 1990 {published data only}
- Lew DB, Herrod HG, Crawford LV. Combination of atropine and isoetharine aerosol therapy in pediatric acute asthma. Annals of Allergy 1990;64(2):195‐200. [PubMed] [Google Scholar]
Lin 1978 {published data only}
- Lin MT, Lee‐Hong E, Collins‐Williams C. A clinical trial of the bronchodilator effect of SCH 1000 aerosol in asthmatic children. Annals of Allergy May 1978;40:326‐32. [PubMed] [Google Scholar]
Mallol 1987 {published data only}
- Mallol J, Barrueto L, Girardi G, Toro O. Bronchodilator effect of fenoterol and ipratropium bromide in infants with acute wheezing: use of MDI with a spacer device. Pediatric Pulmonology 1987;3(5):352‐6. [DOI] [PubMed] [Google Scholar]
Mirsadraee 2009 {published data only}
- Mirsadraee M, Kabolie M, Boskabady MH. Best drugs for avoiding paradoxical bronchospasm during spirometry. Tanaffos 2009;8(3):58‐64. [Google Scholar]
Monge 2000 {published data only}
- Sienra Monge JJ, Bermejo Guevara MA, Rio Navarro BE, Rosas Vargas MA, Reyes Ruiz NI. Degree and duration of Bronchodilatation with a beta 2‐agonist administered alone versus a beta 2‐ agonist administered with ipratropium bromide in children with acute asthma [Grado y duracion de la bronchodilatatacion mediante la administracion de un agonista beta 2 solo vs un agonista beta 2 mas bromuro de ipratropio en ninos con asma aguda.]. Revista Alergia Mexico 2000;47(1):26‐9. [PubMed] [Google Scholar]
Pulejo 1986 {published data only}
- Pulejo R, Romano L, Noto M. Double‐blind study with duovent and placebo in 20 asthmatic children. Respiration 1986;50(2):236‐9. [DOI] [PubMed] [Google Scholar]
Qureshi 1997 {published data only}
- Qureshi F, Zaritsky A, Lakkis H. Efficacy of nebulized ipratropium in severely asthmatic children. Annals of Emergency Medicine 1997;29(2):205‐11. [DOI] [PubMed] [Google Scholar]
Qureshi 1998 {published data only}
- Quereshi F, Pestian J, Davis P, Zaritsky A. Effect of nebulized ipratropium on the hospitalization rates of children with asthma. New England Journal of Medicine 1998;339:1030‐5. [DOI] [PubMed] [Google Scholar]
Rayner 1987 {published data only}
- Rayner RJ, Cartlidge PH, Upton CJ. Salbutamol and ipratropium in acute asthma. Archives of Disease in Childhood 1987;62(8):840‐1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reisman 1988 {published data only}
- Reisman J, Galdes‐Sebalt M, Kazim F, Canny G, Levison H. Frequent administration by inhalation of salbutamol and ipratropium bromide in the initial management of severe acute asthma in children. Journal of Allergy and Clinical Immunology 1988;81(1):16‐20. [DOI] [PubMed] [Google Scholar]
Schuh 1995 {published data only}
- Schuh S, Johnson DW, Callahan S, Canny G, Levison‐H. Efficacy of frequent nebulized ipratropium bromide added to frequent high‐dose albuterol therapy in severe childhood asthma. Journal of Pediatrics 1995;126(4):639‐45. [DOI] [PubMed] [Google Scholar]
Storms 1986 {published data only}
- Storms WW, Bodman SF, Nathan RA, Busse WW, Bush RK, Falliers CJ, et al. Use of ipratropium bromide in asthma. Results of a multi‐clinic study. American Journal of Medicine 1986;81(5A):61‐6. [DOI] [PubMed] [Google Scholar]
Storr 1986 {published data only}
- Storr J, Lenney W. Nebulised ipratropium and salbutamol in asthma. Archives of Disease in Childhood 1986;61(6):602‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Timsit 2002 {published data only}
- Timsit S, Sannier N, Bocquet N, Cojocaru B, Wille C, Boursiquot C, et al. Benefit of ipratropium bromide for the treatment of childhood asthma in the emergency department [Apport du bromure d'ipratropium dans la prise en charge des crises d'asthme aux urgences]. Archives de Pediatrie 2002;9(2):117‐24. [DOI] [PubMed] [Google Scholar]
Ulrik 1992 {published data only}
- Ulrik CS, Backer V, Bach‐Mortensen N. Bronchodilating effect of ipratropium bromide inhalation powder and aerosol in children and adolescents with stable bronchial asthma. Allergy 1992;47(2):133‐7. [DOI] [PubMed] [Google Scholar]
Ward 1981 {published data only}
- Ward MJ, Fentem PH, Smith WH, Davies D. Ipratropium bromide in acute asthma. British Medical Journal (Clinical Research Ed) 1981;282(6262):598‐600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ward 1985 {published data only}
- Ward MJ, MacFarlane JT, Davies D. A place for ipratropium bromide in the treatment of severe acute asthma. British Journal of Diseases of the Chest 1985;79(4):374‐8. [DOI] [PubMed] [Google Scholar]
Yeung 1980 {published data only}
- Yeung R, Nolan GM, Levison H. Comparison of the effect of inhaled SCH 1000 and fenoterol on excercise‐induced bronchospasm in children. Pediatrics 1980;66(1):109‐14. [PubMed] [Google Scholar]
Youngchaiyud 1989 {published data only}
- Youngchaiyud P, Charoenratanakul S, Suthamsmai T, Sriwatanakul K. Comparison of fenoterol, ipratropium bromide and their combination in asthma. Siriraj Hospital Gazette 1989;41(4):197‐201. [Google Scholar]
Zimmerman 1984 {published data only}
- Zimmerman T, Drexel W. Bronchial asthma in childhood. Therapy with fenoterol and ipratropium bromide powder [Asthma bronchiale im Kindersalter‐ Therapie mit Fenoterol und Ipratropiumbromid‐Pulver]. Monatsschr‐Kinderheilkd 1984;132(12):915‐7. [PubMed] [Google Scholar]
Zorc 1999 {published data only}
- Zorc JJ, Pusic MX, Ogborn CJ, Lebet R, Duggan AK. Ipratropium bromide added to asthma treatment in pediatric emergency department. Pediatrics 1999;103(4 Pt 1):748‐52. [DOI] [PubMed] [Google Scholar]
Additional references
Beakes 1997
- Beakes DE. The use of anticholinergics in Asthma. Journal of Asthma 1997;34(5):357‐68. [DOI] [PubMed] [Google Scholar]
Brown 2001
- Brown JH, Taylor P. Muscarinic receptor agonists and antagonists. In: Hardman JG, Limbird LE editor(s). Goodman and Gilman's: The Pharmacological Basis of Therapeutics. 10th Edition. McGraw‐Hill, 2001:155‐73. [Google Scholar]
BTS 2009
- British Thoracic Society. British Thoracic Society guideline on the management of asthma. Thorax 2009;June:1‐125. [Google Scholar]
Cugell 1986
- Cugell DW. Clinical pharmacology and toxicology of ipratropium bromide. American Journal of Medicine 1986;81:18‐22. [DOI] [PubMed] [Google Scholar]
Everard 2005
- Everard ML, Bara A, Kurian M, Elliott TM, Ducharme F, Mayowe V. Anticholinergic drugs for wheeze in children under the age of two years. Cochrane Database of Systematic Reviews 2005, Issue 3. [DOI: 10.1002/14651858.CD001279.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gross 1988
- Gross NJ. The use of anticholinergic agents in the treatment of airways disease. Clinics in Chest Medicine 1988;9(4):591‐8. [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
McDonald 2010
- McDonald N, Bara A, McKean MC. Anticholinergic therapy for chronic asthma in children over two years of age. Cochrane Database of Systematic Reviews 2010, Issue 3. [DOI: 10.1002/14651858.CD003535] [DOI] [PMC free article] [PubMed] [Google Scholar]
NAC 2006
- National Asthma Council Australia. Asthma Management Handbook. National Asthma Council Australia, 2006. [Google Scholar]
NHLBI 2007
- National Heart, Lung, and Blood Institute. Guidelines for the Diagnosis and Management of Asthma. Maryland: National Heart, Lung, and Blood Institute, 2007. [Google Scholar]
Plotnick 2008
- Plotnick LH, Ducharme FM. Combined inhaled anticholinergics and beta2‐agonists for initial treatment of acute asthma in children. Cochrane Database of Systematic Reviews 2008, Issue 3. [DOI: 10.1002/14651858.CD000060] [DOI] [PubMed] [Google Scholar]
RevMan 2011 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Rodrigo 2002
- Rodrigo GJ, Rodrigo C. The role of anticholinergics in acute asthma treatment. An evidence‐based evaluation. Chest 2002;121:1977‐87. [DOI] [PubMed] [Google Scholar]
Tal 1983
- Tal A, Bavilski C, Yohai D, Bearman JE, Gorodischer R, Moses SW. Dexamethasone and salbutamol in the treatment of acute wheezing in infants. Pediatrics 1983;71(1):13‐8. [PubMed] [Google Scholar]
Undem 2001
- Undem BJ, Lichtenstein LM. Drugs used in the treatment of asthma. In: Hardman JG, Limbird LE editor(s). Goodman and Gilman's: The Pharmacological Basis of Therapeutics. 10th Edition. McGraw‐Hill, 2001:733‐54. [Google Scholar]