

Abstract
The authors report on the case of a 30-year-old male who sustained a wrist injury following a motorcycle accident. Emergency department evaluation revealed a left open distal radius fracture with distal radioulnar joint dislocation. The patient underwent surgical fixation to restore full mobility of his wrist.
Keywords: radioulnar dislocation, Frykman fracture, distal radius fracture
Introduction
Wrist fracture dislocations are severe injuries involving both a fracture of the wrist bones and a dislocation of the joint. They are frequently caused by high-energy trauma, such as falls, sports injuries, and motor vehicle accidents (MVA). These cases are clinically significant due to the complex anatomy of the wrist, with many small bones and intricate ligament structures that contribute to its wide range of motion and functionality. Depending on severity, wrist fracture displacement can be treated with immobilization and splinting or orthopedic surgery. Wrist fracture displacement is generally more common in men than women when comparing both age groups below sixty. However, wrist fracture displacements are more common in women when observing both sexes above the age of 60 years.1 Common risks associated with these statistics are that many older women experience minor household trauma, whereas men of younger age experience wrist trauma while engaging in sports. Low bone density is a significant risk factor for wrist fracture displacements and has been shown to cause more wrist fractures within both genders. People who frequently engage in higher-level sports are at a higher risk of suffering wrist trauma, which can be a precursor for wrist fracture displacement. Older individuals or those who have low calcium intake and lack vital nutrients possess brittle bones, which are more susceptible to fracturing.2 Those who have osteoporosis also have higher chances of experiencing wrist fracture displacement.3 Clinical presentation of wrist fracture displacements often includes a visible fork-like structure in the hand due to the bone being disconnected from the corresponding bone and pointing in the incorrect direction, in addition to other visible deformities.4 Patients suffering from a wrist fracture displacement may often suffer from a significant loss of strength in the wrist and hand, pain, stiffness, carpal instability, and post-traumatic arthritis.5
Case Presentation
A 30-year-old male with no significant past medical or surgical history arrived at the emergency department after a MVA. He was riding his motorcycle when a van pulled out in front of him, and he hit the back of the van. He was wearing a helmet, and emergency medical services reported that the helmet had been cracked at the scene. The patient remained conscious and remembered the events surrounding the accident. At the time of arrival, his airway was intact, accompanied by bilateral breath sounds, and intact pulses. The patient had a GCS score of 15 and equal and reactive pupils. The patient suffered no head trauma, but there was an obvious deformity of the left wrist, abrasions to the left shoulder, left thigh, and knee, a small skin tear on the left foot, right wrist pain, and pain in the left big toe. He complained of pain in his right wrist, for which a hematoma block was performed in the emergency department.
The patient’s physical exam showed a pulse oximetry of 100%, blood pressure of 122/70 mmHg, mean arterial pressure of 87 mmHg, temperature of 36.1 C, pulse of 87 beats per minute, and respiratory rate of 17 breaths per minute. The patient’s laboratory analyses were unremarkable.
Plain radiographs revealed a severely comminuted and displaced distal left radial diaphyseal fracture and a dislocated distal left radioulnar joint fracture with adjacent subcutaneous soft tissue emphysema [Figure 1].
Figure 1.

There were no fractures or dislocations involving the remainder of the left ulna and radius. A hematoma block was performed in the ED and the wrist was splinted to provide some immobilization [Figure 2]. The patient also received prophylactic intravenous cefazolin, and tetanus immunoglobulin.
Figure 2.

The patient was admitted to the surgical floor with orthopedic consultation. The surgical procedure consisted of open reduction and internal fixation (ORIF) of the left distal radius fracture, irrigation and debridement of open left distal radius fracture, and open reduction of the left distal radioulnar joint with percutaneous fixation twice two 1.6 mm K-wires. A 3.5-millimeter distal radius plate was also placed for stabilization. The left distal radioulnar joint was also repaired.
Discussion
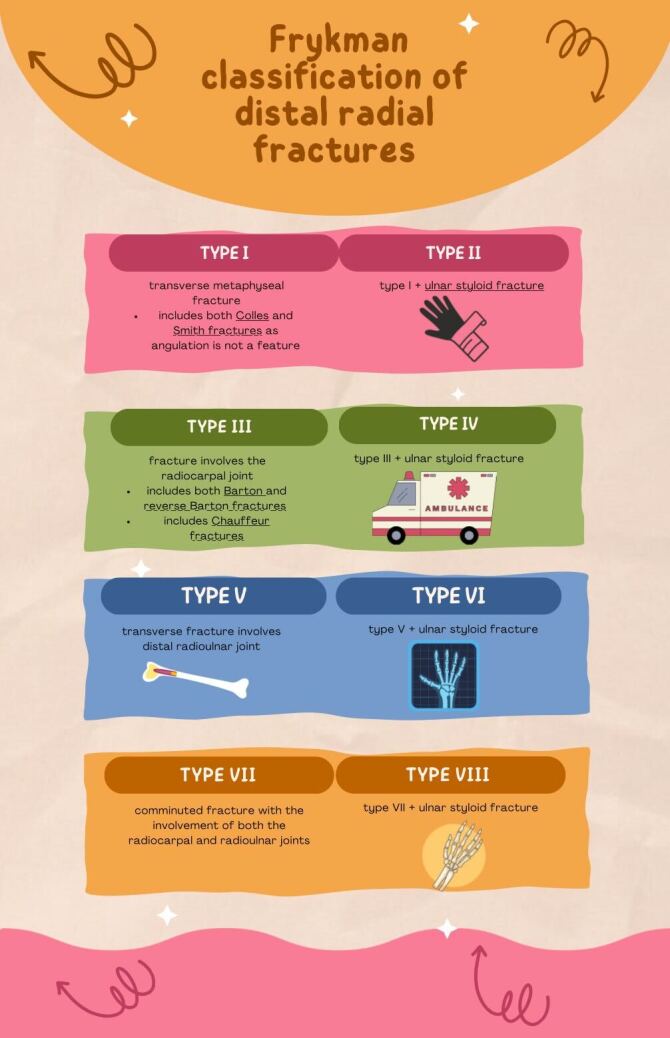
This patient sutained an open distal radius fracture with distal radioulnar joint dislocation after MVA, underwent surgical fixation after consulting over various treatment options. Distal radius fractures have varying degrees of complexity and can be classified using the Frykman system6 [Figure 3].
Figure 3.
Although trauma is a main cause of distal radial fractures, falls specifically are responsible for many of the wrist fractures admitted to the Emergency Department. This is due to human instinct to attempt to break a fall by extending the hand, causing the wrist to sustain most of the impact of the fall.6,7 Other cases of wrist fractures may take a conservative approach in terms of treatment if there is doubt that the patient can tolerate local anesthesia or if there are other risk factors for the patient’s health. Conservative treatments include immobilizing the fracture with various possibilities of splints.8
It is important to consider the long-term consequences of leaving displaced wrist fractures untreated, which consist of chronic pain, reduced wrist function, stiffness, and arthritis. Conservative options are typically not as optimal as those of surgery.9
Conclusion
A 30-year-old male, who was hit by a van, was admitted to the Emergency Department with full consciousness and orientation. He cracked his helmet in the accident but was shown to have no neurological deficits during his examination in the ED. He sustained a left open distal radius fracture with distal radioulnar joint dislocation and underwent ORIF to realign and reconnect the left distal radius with the corresponding bones in the wrist. This was followed by the repair of the left distal radioulnar joint. The patient made a good recovery.
References
- Prevalence, Characteristics, and Associated Risk Factors of Wrist Fractures in Americans Above 50: The Cross-Sectional NHANES Study. Ye J., Li Q., Nie J. Apr 25;2022 Front Endocrinol (Lausanne) 13:800129. doi: 10.3389/fendo.2022.800129. doi: 10.3389/fendo.2022.800129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Risk factors of refracture after a fragility fracture in elderly. Sriruanthong K., Philawuth N., Saloa S., Daraphongsataporn N., Sucharitpongpan W. Jul 25;2022 Arch Osteoporos. 17(1):98. doi: 10.1007/s11657-022-01143-4. doi: 10.1007/s11657-022-01143-4. [DOI] [PubMed] [Google Scholar]
- A comprehensive overview on osteoporosis and its risk factors. Pouresmaeili F., Kamalidehghan B., Kamarehei M., Goh Y.M. Nov 6;2018 Ther Clin Risk Manag. 14:2029–2049. doi: 10.2147/TCRM.S138000. doi: 10.2147/TCRM.S138000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clin Calcium. Yajima H. 200818(11):1627–1633. [PubMed] [Google Scholar]
- Peri-lunate dislocation and fracture-dislocation of the wrist: Retrospective evaluation of 65 cases. Israel D., Delclaux S., André A.., et al. 2016Orthop Traumatol Surg Res. 102(3):351–355. doi: 10.1016/j.otsr.2016.01.004. doi: 10.1016/j.otsr.2016.01.004. [DOI] [PubMed] [Google Scholar]
- Frykman VIII Fracture Secondary to Falling Onto an Outstretched Hand (FOOSH) Dande V., D'Souza D., Mangal R., Daniel A.R., Ganti L. Dec 16;2023 Cureus. 15(12):e50641. doi: 10.7759/cureus.50641. doi: 10.7759/cureus.50641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Displaced Paediatric Distal Radius Fractures with Volar Skin Tenting Following Manipulation and Reduction: A Report of Two Cases and Literature Review. Chou Andrew, Chew Darryl, Chia Dawn, Mahadev Arjandas, Wong Kenneth. Sep;2022 Journal of Orthopaedic Experience & Innovation. :8. doi: 10.60118/001c.35699. [DOI]
- The past, present and future of the conservative treatment of distal radius fractures. de Bruijn M. A. N., van Ginkel L. A., Boersma E. Z., van Silfhout L., Tromp T. N., van de Krol E., van der Heijden B. E. P. A., Hermans E., Stirler V. M. A., Edwards M. J. R. 2023Injury. 54 Suppl 5:110930. doi: 10.1016/j.injury.2023.110930. doi: 10.1016/j.injury.2023.110930. [DOI] [PubMed] [Google Scholar]
- Long-term outcome of nonsurgically treated distal radius fractures. Földhazy Z., Törnkvist H., Elmstedt E., Andersson G., Hagsten B., Ahrengart L. 2007The Journal of hand surgery. 32(9):1374–1384. doi: 10.1016/j.jhsa.2007.08.019. doi: 10.1016/j.jhsa.2007.08.019. [DOI] [PubMed] [Google Scholar]