

Abstract
Oral cancers, specifically oral squamous cell carcinoma (OSCC), pose a significant global health challenge, with high incidence and mortality rates. Conventional treatments such as surgery, radiotherapy, and chemotherapy have limited effectiveness and can result in adverse reactions. However, as an alternative, photodynamic therapy (PDT) has emerged as a promising option for treating oral cancers. PDT involves using photosensitizing agents in conjunction with specific light to target and destroy cancer cells selectively. The photosensitizers accumulate in the cancer cells and generate reactive oxygen species (ROS) upon exposure to the activating light, leading to cellular damage and ultimately cell death. PDT offers several advantages, including its non-invasive nature, absence of known long-term side effects when administered correctly, and cost-effectiveness. It can be employed as a primary treatment for early-stage oral cancers or in combination with other therapies for more advanced cases. Nonetheless, it is important to note that PDT is most effective for superficial or localized cancers and may not be suitable for larger or deeply infiltrating tumors. Light sensitivity and temporary side effects may occur but can be managed with appropriate care. Ongoing research endeavors aim to expand the applications of PDT and develop novel photosensitizers to further enhance its efficacy in oral cancer treatment. This review aims to evaluate the effectiveness of PDT in treating oral cancers by analyzing a combination of preclinical and clinical studies.
Graphical Abstract

Keywords: Photodynamic therapy, Oral cancer, Photosensitizers, Oral squamous cell carcinoma
Introduction
The International Agency for Research on Cancer recorded 744,994 diagnoses of mouth and oral cancer in the year 2020, with a grim outcome of 364,339 lives lost. Meanwhile, the Oral Cancer Foundation provides a staggering estimate of 657,000 new cases and over 330,000 annual deaths attributed to cancers of the oral cavity and oropharynx. These figures underscore the urgent need for more effective prevention and treatment strategies in the global fight against oral cancer [1]. Oral and mouth cancers typically impact various regions, including the tongue, floor of the mouth, cheek lining, hard palate, lips, soft palate, and gums [2].
Oral cancer, particularly oral squamous cell carcinoma (OSCC), is one of the ten most common cancers worldwide, accounting for more than 90% of all malignant oral tumors. It typically develops in the paranasal sinuses, larynx, nasal and oral cavities, and pharynx. OSCC is often marked by late-stage diagnosis, unfavorable prognosis, vague symptoms, and high treatment costs [3]. HNSCC, or Head and Neck Squamous Cell Carcinoma, impacts an estimated 600,000 individuals worldwide annually. This type of cancer is responsible for taking the lives of 40–50% of those diagnosed. The origin of HNSCC can be traced back to the epithelial cells located in the larynx, hypopharynx, oral cavity, and oropharynx [4].
Although there have been considerable advances in the 5-year survival rates for head and neck cancer, particularly in advanced stages, the overall prognosis remains unsatisfactory, especially in the early stages. The global cancer-related mortality rate for head and neck cancer was 5.7% in 2009 [5]. Further, in 2012, there were 690,000 reported cases and 375,000 deaths from head and neck cancer worldwide, with developing countries accounting for 67% of new cases and 82% of related deaths [6]. The emergence of oral cancer can be attributed to various factors, such as tobacco and alcohol use, viral infections dietary, habits and nutrition, ethnicity and race, occupational hazards, oral candidiasis (thrush), syphilis, weakened immune system, and genetic predisposition [7–9].
Current treatments for oral cancer, including surgery, radiotherapy, and chemotherapy, have limited effectiveness and common adverse reactions. Prognosis is generally poor, with disfigurement from surgery and difficulties in swallowing, chewing, and talking from chemotherapy and radiotherapy. There is a growing need for safer and more effective treatment methods with fewer side effects for individuals with oral cancer [10–13].
Photodynamic therapy (PDT) has emerged as a promising alternative for treating various cancers, including oral cancers, due to its advantages over conventional therapeutic agents, despite certain limitations and adverse effects [14, 15]. PDT is a treatment that combines the use of special drugs called photosensitizing agents and light to target and destroy cancer cells. This therapy is also utilized for treating other health conditions such as psoriasis, acne, and infections. The procedure involves two main steps: The administration of the photosensitizer and the exposure of the tumor to a specific light source.
During the treatment, the photosensitizing agent is administered to the patient orally, topically, or intravenously, depending on the tumor’s location. The cancer cells absorb the drug over a specific duration. Subsequently, the tumor is exposed to a specific type of light, which activates the photosensitizer, leading to a chemical reaction that generates a unique oxygen molecule that is responsible for the destruction of the cancer cells [16, 17].
Photosensitizers play a crucial role in PDT by selectively accumulating in targeted cells and becoming activated upon exposure to specific wavelengths of light. Indeed, when the area is exposed to the appropriate activating light, the photosensitizer undergoes a chemical reaction, generating reactive oxygen species (ROS) that damage cellular components and ultimately lead to cell death. Photosensitizers used in PDT can be classified into different types based on their structures; they include dye-, chlorin-, porphyrin-, xanthene-, and monoterpene-based photosensitizers. The choice of a photosensitizer depends on factors like the medical condition, tissue penetration requirements, and the light source used for activation [18–21].
The light used in PDT can come from lasers or light-emitting diodes (LEDs), depending on the type and location of the cancer being treated. Notably, the duration of PDT treatment sessions ranges from 15 to 90 min, and the timeline for observing results depends on individual factors, the type of photosensitizer used, and the prescribed treatment plan [22–24].
As per findings, PDT is FDA-approved for the treatment of esophageal and lung cancers, as well as actinic keratosis [14, 25, 26], while ongoing research seeks to develop new PDT drugs and explore combinations with other treatments to enhance its effectiveness for a broader range of conditions. Noteworthy, PDT can be used as an effective treatment option for certain types and stages of oral cancers, including those affecting the lips, tongue, cheeks, floor of the mouth, palate, and other soft tissues. This activates the photosensitizer, leading to the generation of ROS that selectively damage and destroy cancer cells. PDT can be used as a primary treatment for early-stage oral cancers or in combination with other therapies for more advanced cases. It is particularly beneficial for treating difficult-to-access lesions or patients who are not suitable for extensive surgery [27–29].
Indeed, PDT offers several advantages compared to alternative treatments, such as the absence of known long-term side effects when administered correctly, its less invasive nature in comparison to surgery, and the possibility of repeating the procedure if needed. PDT also minimizes scarring and provides a cost-effective option for patients. However, there are limitations to consider. It is most effective for superficial or localized cancers that can be reached by light, making it unsuitable for large cancers or those deeply infiltrating the skin or organs. Additionally, individuals undergoing PDT experience light sensitivity for a specific period, requiring post-treatment precautions to be taken into account. Notably, temporary side effects such as light sensitivity, swelling, or pain may occur but can be managed with appropriate care [16, 30–32].
This review aims to elucidate the utilization of PDT in the treatment of oral cancers, evaluating its effectiveness and addressing the challenges associated with its application through an analysis of preclinical and clinical studies.
Mechanisms of PDT
PDT operates by using a combination of a photosensitizer drug, light at or near the absorbance wavelength of the drug, and oxygen to selectively destroy target cells, such as cancer cells. The photosensitizer drug is introduced into the patient’s body, where it selectively accumulates in the target cells. Once the drug accumulates in the target cells, the light is applied to activate the drug, which then reacts with oxygen to produce a form of oxygen that destroys the target cells [33, 34].
In PDT, the photosensitizer drug is introduced into the patient’s body and selectively accumulates in the target cells. Once the drug has accumulated in the target cells, it is activated by light at its specific absorbance wavelength. The absorption of light by the photosensitizer molecule causes a transition from its low-energy ground state (singlet state) to a higher-energy state (singlet-excited state). In this singlet-excited state, the photosensitizer’s electrons occupy orbitals with higher energy levels. This activated state of the photosensitizer is what allows it to react with oxygen and produce the form of oxygen that destroys the target cells [20, 35–39]. After the photosensitizer molecule is activated by light and transitions from its low-energy ground state to the higher-energy singlet-excited state, it is not stable and quickly dissipates its energy through various mechanisms. This can occur through the emission of light at a higher wavelength (lower energy), a process known as fluorescence. The absorbed energy can also be converted into heat through a process called internal conversion. Alternatively, the excited photosensitizer can undergo intersystem crossing, a process in which the spin of the electron is changed, transitioning the molecule to an excited triplet state. In this triplet state, the photosensitizer molecule exhibits three spectral lines of light absorption, instead of the single line seen in the singlet state. This triplet state is what allows the photosensitizer to react with oxygen and produce the form of oxygen that destroys the target cells [20, 35–39].
During PDT, two primary types of reactions occur: Type I and Type II [20, 35–41].
Type I reaction: The photosensitizer in the triplet state interacts with neighboring molecules, which may act as electron donors or acceptors, leading to the formation of radical anions or radical cations. These radicals can then react with molecular oxygen (O2) to produce ROS such as superoxide radical (O2-•), hydrogen peroxide (H2O2), and hydroxyl radicals (HO•). These ROS cause oxidative damage to proteins, nucleic acids, and lipids within the target cells, leading to cell death.
Type II reaction: The energy of the triplet-state photosensitizer is transferred to ground-state triplet molecular O2, resulting in the formation of highly reactive singlet oxygen (1O2). Singlet oxygen is a potent cytotoxic agent that can oxidize and damage various cellular components, leading to cell death.
Of note, a Type III mechanism has also been described in PDT, where excited photosensitizers can directly degrade nucleic acids and proteins. This oxygen-independent mechanism contributes to the cytotoxic effects of PDT.
In summary, PDT uses a photosensitizer drug that is activated by light, which then reacts with oxygen to produce various forms of ROS and other cytotoxic agents that damage and destroy the target cells [20, 35–41]. (Fig. 1)
Fig. 1.

Mechanisms of PDT. PDT encompasses two main reactions: Type I and Type II. In Type I reactions, the photosensitizer interacts with nearby molecules, forming radical anions or cations, which then react with molecular oxygen to produce ROS like superoxide anions and hydroxyl radicals. These ROS cause oxidative damage to cellular components, including lipids, proteins, and DNA, leading to cellular dysfunction and death. Type II reactions involve the transfer of energy from the excited photosensitizer to ground-state molecular oxygen, producing singlet oxygen, a highly reactive form of oxygen that directly oxidizes biological molecules, causing similar oxidative stress and damage. The combined effects of these reactions create an environment of oxidative stress, overwhelming the cell’s antioxidant defenses, disrupting cellular homeostasis, and triggering cell death pathways such as apoptosis, necrosis, and autophagy. This dual mechanism makes PDT an effective treatment for targeting and destroying cancer cells. ground-state
PDT induces cytotoxicity in target cells through various pathways. Apoptosis, a programmed cell death process, is a common mode of cell death observed in PDT. It involves cell shrinkage, DNA fragmentation, and the formation of apoptotic bodies. PDT can activate specific signaling pathways, such as the NF-κB/JNK pathway and PI3K/Akt, and involve caspase activation to induce apoptosis in cancer cells. PDT can also induce autophagy, a cellular process involving the degradation and recycling of cellular components [42–44]. Additionally, PDT can trigger the intrinsic pathway by disrupting mitochondrial function, leading to the release of cytochrome c and the activation of caspases. The extrinsic pathway can also be activated through death receptors on cancer cells, initiating a caspase cascade [45, 46]. PDT-induced oxidative stress can induce endoplasmic reticulum (ER) stress, activating the unfolded protein response (UPR) and caspase-12 [47]. The PI3K/Akt pathway, involved in cell survival, can be modulated during PDT to promote apoptosis. The interplay and activation of these pathways contribute to the apoptotic response in cancer cells during PDT [42]. (Fig. 2)
Fig. 2.
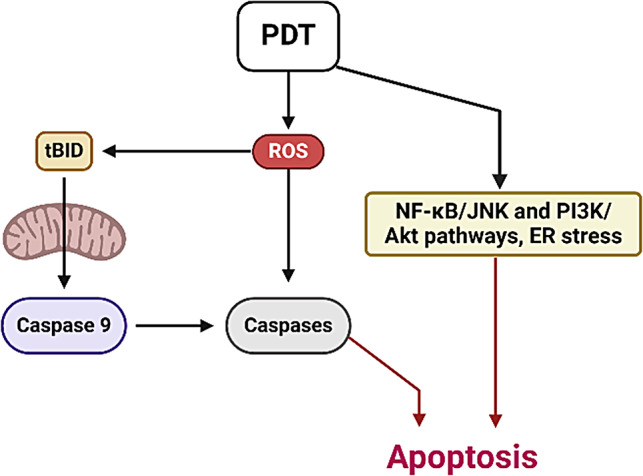
PDT induces cytotoxicity in target cancer cells through mechanisms involving apoptosis, autophagy, and the modulation of signaling pathways. Apoptosis is driven by caspase activation, mitochondrial dysfunction, and ER stress, which collectively initiate programmed cell death. Additionally, PDT can trigger autophagy, a process where cells degrade and recycle their components, which may lead to cell death if the damage is extensive. Key signaling pathways such as NF-κB/JNK and PI3K/Akt are also influenced by PDT, where their modulation can enhance the apoptotic response. This combination of mechanisms ensures that PDT effectively targets and destroys cancer cells while minimizing damage to surrounding healthy tissue
Furthermore, PDT can activate the immune system [48], contributing to its therapeutic efficacy. PDT with certain photosensitizers triggers immunogenic cell death (ICD), activating the adaptive immune response and promoting the formation of long-term immunological memory. This immune response enhances the anti-cancer effects of PDT and supports its potential as a cancer immunotherapy [49].
In addition to the photosensitizer and light, the presence of oxygen and proper dosimetry are crucial considerations in PDT. The tumoricidal effect of PDT relies on a photo-oxidative reaction, which necessitates the availability of oxygen for successful treatment. Tissue hypoxia, characterized by low oxygen levels, significantly diminishes the effectiveness of PDT [50, 51]. During in vivo exposure to light, the photosensitizer undergoes a gradual degradation process called photobleaching, caused by its reaction with singlet oxygen or free radicals. The byproducts of this interaction do not contribute further to the photodynamic activity. Photobleaching plays a vital role in minimizing or preventing damage to normal tissue by ensuring that the threshold dose required for PDT to be effective against tumors is not surpassed in healthy tissue while still being exceeded in the tumor itself [50–53].
It is of note that a thorough understanding of light dosimetry is also essential for comparing, reproducing, and predicting the outcomes of PDT, as well as identifying the factors that contribute to its success or failure. However, in clinical PDT, insufficient attention has been given to light dosimetry, with few exceptions. The measurement of light in PDT involves the power of the light source, which is expressed in watts (W), and the delivered energy, which is expressed in joules (J). The power per unit area, also known as irradiance, is expressed in watts per square meter (W/m²) or milliwatts per square centimeter (mW/cm²) when irradiating a specific surface area. The effectiveness of PDT is determined by the energy fluence (J/m²) multiplied by the absorption coefficient (m^(-1)) of the photosensitizer in tissue. Energy fluence is the product of the fluence rate (W/m²) and the irradiation time (s). In short, PDT light dosimetry involves the power of the light source, the delivered energy, the power per unit area, the energy fluence, and the absorption coefficient of the photosensitizer in tissue. These factors are critical in determining the effectiveness of PDT [51, 54, 55].
Given the unpredictable distribution of photosensitizer concentration in tissue, the calculation of the light dose absorbed by the photosensitizer in PDT is a challenging task. The incident power per unit area multiplied by the irradiation time is commonly used as the light dose in superficial PDT, but the actual energy fluence (rate) in tissue can differ due to light scattering and internal reflection at tissue boundaries. In order to better understand light dosimetry, it is necessary to measure the fluence rate, estimate the scattering properties and optical absorption of the treated tissue, and use mathematical models to predict the propagation of light in tissue. This will lead to a more accurate determination of the light dose delivered to the target tissue, which is essential for achieving the desired therapeutic effect in PDT. By utilizing these methods, the effectiveness of PDT can be improved, resulting in better treatment outcomes [56, 57].
Significantly, when it comes to PDT, tumors that exhibit superficial growth and have a higher accumulation of photosensitizers can be effectively targeted. However, as the depth within the tissue increases, the energy fluence rate experiences an exponential decline. Consequently, achieving a tumoricidal effect at the deepest regions of thicker tumors necessitates a higher surface light dose. This, in turn, can potentially result in necrosis of the surrounding normal tissue located closer to the surface [58, 59]. As a result, the limitations of selective PDT extend beyond the photosensitizer distribution in tumor and normal tissue. The depth to which light can effectively penetrate also plays a crucial role. Ongoing research strives to identify new photosensitizers that exhibit selective retention or activation when exposed to longer wavelength light. This exploration holds promise for enabling deeper tissue penetration during PDT, opening up new avenues for treatment.
On the whole, PDT is a medical treatment that selectively destroys cancer cells using a photosensitizer drug, light, and oxygen. The photosensitizer can generate ROS, oxidative damage, and cell death. PDT also activates the immune system, promoting long-term immunity and anti-cancer effects. Factors like oxygen availability, dosimetry, and photobleaching influence its effectiveness. Ongoing research should focus on discovering photosensitizers with greater tissue penetration depth.
Photosensitizers
PDT utilizes photosensitizers to target and destroy cancerous or abnormal cells through light activation. Commonly used photosensitizers in PDT include Photofrin (Porfimer Sodium), which is effective against esophageal, lung, and bladder cancer [60, 61]. Levulan (Aminolevulinic Acid or ALA) is a synthetic compound that converts to the photosensitizer protoporphyrin IX (PpIX) and is used in dermatology for treating skin lesions and certain skin cancers [61–63]. Foscan (Temoporfin) is derived from chlorophyll and is primarily employed in head and neck cancer treatment [64, 65]. Metvix (Methyl Aminolevulinate or MAL) treats actinic keratosis and superficial basal cell carcinoma [66, 67], while Hexvix (Hexaminolevulinate or HAL) aids in diagnosing and treating bladder cancer [68]. The choice of photosensitizer depends on factors such as cell type, location, tissue penetration, and treatment goals, highlighting the importance of selecting the appropriate photosensitizer for optimal PDT outcomes.
Photosensitizers Used in Common
The five photosensitizers have been shown to offer distinct applications in PDT. In the ensuing subheadings, the efficacy and role of such photosensitizers in oral cancers will be elucidated.
5-Aminolevulinic Acid (ALA)
5-aminolevulinic acid (ALA) is a vital component in the heme biosynthetic pathway, acting as a precursor for the photosensitizer known as protoporphyrin IX (PpIX). When exogenous ALA is introduced into the system, it hampers the initial stage of porphyrin synthesis, resulting in the buildup of PpIX within the tissue [69, 70].
PDT using ALA has been extensively studied in clinical trials for the treatment of oral leukoplakia, a condition that has the potential to develop into malignant cancer [71]. Oral leukoplakia serves as a convenient model for studying cancer prevention strategies [72]. In a pioneering study conducted by Kübler et al., a 20% ALA cream was topically applied to leukoplakia lesions in 12 patients for a duration of 2 h. Subsequently, the cream was removed, and the lesions were subjected to monochromatic red light at 630 nm wavelength using an argon-dye laser. The light exposure lasted for 1 h, with a radiant exposure of 100 J/cm². Following a therapeutic period of 3 months, it was observed that five patients achieved complete remission, four showed a partial response, and three did not exhibit a favorable response to the treatment [73].
Sieron et al. conducted an additional study exploring the use of PDT for the treatment of oral leukoplakia, a pre-malignant condition. The study involved 12 patients with lesions in various intraoral sites. A 10% ALA emulsion was topically applied to the lesions, followed by exposure to light emitted by an argon-pumped dye laser with a wavelength of 635 nm. Each treatment session delivered a total dose of 100 J/cm². The results were promising, with 10 out of the 12 treated patients achieving a complete response, indicating the disappearance or significant improvement of the lesions. During a 6-month follow-up period, only one instance of recurrence was observed. Based on these findings, the study concluded that PDT could be a viable alternative to traditional therapies for managing pre-malignant lesions in the oral cavity, demonstrating its potential effectiveness in this specific context [74].
Another study was conducted by Chen et al. to evaluate the efficacy of ALA-PDT in various diseases and treatment regimens. Thirty-two patients participated in the study, with 8 of them having oral verrucous hyperplasia and 24 having oral leukoplakia. The results showed that the oral verrucous hyperplasia lesions responded better to the PDT compared to the oral leukoplakia lesions. In the case of oral leukoplakia lesions, the protocol had to be applied twice a week to observe even a partial response, while the oral verrucous hyperplasia lesions showed a complete response in less than six treatments, with a weekly application [75].
In the study conducted by Siddiqui et al., the researchers explored the effects of photoactivated ALA in the treatment of oral cancer. The patients involved in the study were administered ALA at a dosage of 60 mg/kg, which was divided into three doses. This administration aimed to promote the accumulation of a photosensitive product called PpIX within the tumor cells. Approximately 0.5 to 1 h after ALA administration, the tumor area was exposed to LED light with a wavelength of 635 nm. The light exposure delivered a dose of 100 J/cm² to the tumor site. Remarkably, the study reported that a complete response, indicating the complete disappearance or significant reduction of the tumor, was achieved in 76% of the patients. These findings suggest that the use of photoactivated ALA and LED light therapy may hold promise as an effective treatment approach for oral cancer [76].
Yao et al. conducted a study to examine the combination of an ablative fractional laser with ALA-PDT in the treatment of oral leukoplakia lesions in 48 patients. In the study, an ablative fractional laser was applied to the lesions, followed by the application of a 20% ALA gel for 3 h. The lesions were then illuminated with red light at a wavelength of 630 nm using a Yage LED-IB device at a dose of 180 J/cm². After one month, 30 patients showed complete recovery, and 12 patients showed partial recovery. The recurrence rate was 37.5%, and the malignant transformation rate was 8.3% after 3 years of follow-up. The results of Yao et al.’s study suggest that the combination of an ablative fractional laser and ALA-PDT may improve the clinical success of treating oral leukoplakia lesions. However, the recurrence rate and malignant transformation rate after 3 years of follow-up indicate that further studies are needed to evaluate the long-term effectiveness of this treatment approach [77].
The mentioned studies highlight the potential of ALA-mediated PDT for oral leukoplakia, but response rates varied due to differences in treatment protocols and disease characteristics, and also further research is needed to refine the treatment and enhance long-term outcomes.
Methylene Blue
Oral lichen planus is a long-term inflammatory disorder that affects the oral mucous membrane, leading to the appearance of white or red patches, sores, and discomfort in the mouth. In some cases, it can progress to squamous cell carcinoma, a type of oral cancer. The standard treatment for oral lichen planus involves the use of topical corticosteroids, which can have local side effects when used over a long period of time [78, 79].
Methylene blue is a photosensitizer, a compound that can be activated by specific wavelengths of light to produce ROS. These ROSs can cause damage to targeted cells, such as abnormal or cancerous cells while sparing healthy tissue. Methylene blue has been used in the treatment of various skin conditions and cancers [80–83].
A study was carried out by Aghahosseini et al. to assess the effectiveness and safety of methylene blue-mediated PDT for oral lichen planus. The study consisted of 13 patients with a total of 26 oral lichen planus lesions. The treatment process entailed rinsing the mouth with a 5% methylene blue solution, followed by the application of laser light to the lesions for 2 min using a diode laser with a wavelength of 632 nm and a dose of 120 J/cm². The specific wavelength of the laser light was chosen to correspond to the absorption peak of methylene blue, ensuring its efficient activation. Following a 12-week follow-up period, 16 out of 26 lesions showed a significant reduction in size, with an average reduction of approximately 44%. The study also found that the treatment was safe, with no serious side effects reported [84].
Another study was conducted with 20 patients suffering from oral lichen planus, who were administered methylene blue-mediated PDT. The treatment involved gargling with a methylene blue solution and then illuminating the lesions with laser light. After four weeks, 17 out of 20 patients showed a positive response, with a noticeable reduction in the size of their lesions. However, the three patients who did not respond to the treatment had longer-standing lesions, indicating that the duration of the lesion may impact the treatment outcome [85].
Bakhtiari et al. conducted a randomized clinical trial to compare the clinical effects of PDT and dexamethasone mouthwash in the treatment of oral lichen planus, a challenging autoimmune disorder. The trial included 30 patients, 15 of whom received PDT with methylene blue and a Fotosan device, and the other 15 who used dexamethasone mouthwash. Researchers assessed various parameters related to the efficacy and severity of the condition at different time points after treatment initiation. The results showed no significant differences between the two treatment modalities regarding treatment efficacy, symptom scores, sign scores, and clinical severity. Both groups experienced statistically significant decreases in symptoms. Therefore, the study concluded that PDT is as effective as dexamethasone mouthwash in treating oral lichen planus, providing a safe treatment option without identified side effects for oral lichen planus lesions [86].
Mostafa et al. aimed to compare the clinical effectiveness of PDT mediated by methylene blue (MB-PDT) with conventional topical corticosteroid (TC) treatment for erosive oral lichen planus (EOLP). EOLP is a challenging condition to manage, and although corticosteroids are commonly used, their prolonged use can lead to complications. Twenty patients with EOLP were randomly divided into two groups: Group A received TC treatment with kenakort A-orabase, while Group B underwent MB-PDT using a diode laser at 660 nm. The researchers evaluated the signs and symptoms of EOLP and found that both treatment groups showed significant improvements over the follow-up period. However, the MB-PDT group exhibited a more notable reduction in pain and lesion scores compared to the corticosteroid group. Consequently, the study concluded that MB-PDT is a superior treatment option for EOLP, offering better pain relief and lesion regression when compared to conventional TC treatment [87].
According to such clinical research, PDT using methylene blue shows great potential as a viable alternative for treating oral lichen planus. This approach offers several advantages, including minimized side effects and enhanced pain alleviation. However, additional studies are required to fine-tune treatment protocols and conduct comparative analyses to determine their efficacy in relation to other treatments.
Porphyrin Photosensitizers
Photofrin, an initial iteration sensitizer employed in PDT to address HNSCC, gathers within tumor cells and generates ROS when subjected to specific light wavelengths. Despite drawbacks such as sensitivity to light and restricted tissue penetration, Photofrin has played a pivotal role in propelling PDT as an effective cancer treatment [88, 89].
Dr. Biel conducted a significant study focusing on the treatment of head and neck squamous cell carcinoma, specifically laryngeal tumors, using Photofrin as the photosensitizer in PDT. The study involved a large group of patients and yielded remarkable results. In this study, Dr. Biel initially targeted “true” cancer of the larynx, which refers to confirmed cases of laryngeal cancer. The patients included in the study had previously undergone other therapies, such as radiation, which had not been successful in achieving a complete response. Despite this, Photofrin PDT led to a complete response in approximately 90% of the patients. This highlights the effectiveness of Photofrin as a photosensitizer in treating laryngeal tumors, even in cases where other treatments had failed [90–93].
Dr. Biel reported the treatment of 110 patients with recurrent or primary laryngeal tumors using Photofrin-mediated PDT. The protocol consisted of an intravenous injection of Photofrin at a dose of 2 mg/kg, followed by a 48-hour waiting period before the light-based therapy. The therapy was delivered using an Nd: Yag pumped-dye laser with a wavelength of 630 nm and a fused silica optical fiber with a microlens to reach the larynx. The light dose rate was 80 J/cm² and the power density was 150 mW/cm² in the larynx area. The 5-year cure rate was an impressive 90%, indicating the high efficacy of Photofrin PDT in treating laryngeal tumors. Recurrences, if any, were successfully managed with additional PDT sessions, surgery, or radiation. These results suggest that Photofrin PDT is a highly effective option for treating laryngeal tumors [93].
Based on the positive outcomes observed in these studies, Dr. Biel suggested that PDT using Photofrin should be considered as a treatment option for primary and recurrent squamous cell carcinoma of the larynx. Specifically, it could be beneficial in cases classified as Tis (in situ carcinoma in the superficial lining of the oral cavity), T1 (tumor ≤ 2 cm across), and T2 (tumor > 2 cm and < 4 cm across) stages. This recommendation is based on the significant response rates and the potential to achieve long-term cure, as well as the ability to manage any recurrences effectively with additional sessions of photodynamic therapy, surgery, or radiation [93]. These findings emphasize the potential of Photofrin-mediated PDT as a valuable therapeutic approach for HNSCC, particularly in the treatment of laryngeal tumors. However, it is important to note that further research is necessary to optimize treatment protocols, assess long-term outcomes, and investigate potential side effects to ensure the safe and effective use of Photofrin PDT in clinical practice.
A study was conducted to evaluate the use of Photofrin-mediated PDT in treating squamous cell carcinoma and epithelial dysplasia with hyperkeratosis in the oral cavity. The study consisted of 18 patients with squamous cell carcinoma and 7 patients with epithelial dysplasia. The treatment protocol involved the intravenous administration of Photofrin at a dose of 2 mg/kg, 48 h before laser irradiation. The lesions in the oral cavity were then exposed to light using an excimer dye laser with a wavelength of 630 nm, with an output of 4 mJ/pulse/cm² and a repetition rate of 40 Hz. To deliver the light to the tumor sites, a 400 μm flat-tipped quartz fiber was employed.
The results of the study were highly promising, with a cure rate of 96% among the patients. This suggests that Photofrin-mediated PDT is effective in treating both oral squamous cell carcinoma and epithelial dysplasia with hyperkeratosis. However, it is important to note that this study included a specific group of patients with these conditions, and the sample size was relatively small. Therefore, further research is required to validate these findings and assess the broader efficacy of Photofrin-mediated PDT in treating oral cavity lesions [94].
In summary, clinical investigations indicate that methylene blue-mediated PDT holds promise as a compelling alternative treatment for oral lichen planus. This therapeutic approach brings about advantages such as diminished side effects and enhanced pain relief. Nevertheless, additional research is required to refine treatment protocols and evaluate their efficacy through comparative analysis with other treatments.
Foscan (Temoporfin; mTHPC)
Foscan, also known as Temoporfin or mTHPC, is a photosensitizing agent used in photodynamic therapy for the treatment of advanced head and neck cancer, where it is activated by light to destroy tumor cells.
The use of PDT with the photosensitizer Foscan, also known as Temoporfin or mTHPC, has shown positive results in the treatment of various oral conditions, particularly early oral squamous cell carcinoma. In a study with 114 patients, Foscan was given intravenously at a dose of 0.15 mg/kg and the lesions in the floor of the mouth, lip, and anterior tongue were exposed to laser light at a wavelength of 652 nm. The study found a response rate of 93% for T1 lesions and 58% for T2 lesions. Additionally, patients maintained good functional status after therapy, and there was no need for airway management. These results suggest that Foscan-mediated PDT can be an effective treatment option for early oral squamous cell carcinoma, providing good functional outcomes and minimal impact on the patient’s quality of life [95].
In cases where a disease is incurable or has recurred, PDT utilizing Foscan has been investigated as a potential salvage treatment option. For instance, D’Cruz et al. conducted a study involving 128 patients, some of whom had multiple lesions. The patients received intravenous administration of a photosensitizing agent called mTHPC (Foscan), followed by illumination of the tumor surface using a nonthermal diode laser with a microlens fiber. The results showed that approximately 16% of patients achieved a complete response to the treatment. These findings suggest that salvage PDT could be beneficial for patients who have previously undergone extensive surgery and radiation. It offers a potential alternative for those with limited treatment options, providing a chance for disease control or improvement in cases where curative treatment is not feasible [96].
Notably, Foscan has shown promise in treating lip cancer [97] and advanced head and neck cancer by targeting difficult-to-access tumors, preserving healthy tissue, and generating reactive oxygen species to induce cell death. Compared to traditional approaches like surgery and radiation, Foscan-mediated PDT offers advantages such as improved functional outcomes, particularly for recurrent or persistent tumors that have not responded well to previous treatments, while minimizing the impact on patient’s physical appearance and functional abilities, ultimately enhancing their quality of life during and after treatment. However, treatment decisions should consider individual factors such as tumor characteristics, patient preferences, and overall health [95, 98].
In a study involving 170 patients diagnosed with early-stage oral cavity and oropharynx squamous cell cancers, Foscan-based PDT was employed as a treatment approach. The patients received intravenous administration of Foscan at a dose of 0.15 mg/kg. Subsequently, they were exposed to a diode laser emitting light at a wavelength of 652 nm, with a dose of 20 J/cm². The study reported an overall response rate of 91%, indicating that the majority of patients demonstrated a positive response to the Foscan-mediated PDT treatment. Furthermore, a complete response rate of 71% was observed, indicating that a significant proportion of patients achieved complete eradication of their tumors. These findings highlight the potential efficacy of Foscan-mediated PDT in the management of early-stage oral cavity and oropharynx squamous cell cancers. The high overall response rate suggests that this treatment approach has the ability to effectively target and destroy cancer cells in these specific types of tumors. The substantial complete response rate further underscores the potential of Foscan-based PDT as a curative treatment option for early-stage oral cancers. It is important to note that the results of this study specifically apply to early-stage oral cavity and oropharynx squamous cell cancers, and the efficacy of Foscan-mediated PDT may vary in other types or stages of cancer. Therefore, treatment decisions should be made in consultation with healthcare professionals, considering individual patient characteristics and preferences [99].
A trial was conducted with 25 patients diagnosed with T1-T2 N0 tumors in the oral cavity and/or oropharynx, who were treated with PDT using mTHPC (Foscan) as the photosensitizer. The results of the study showed complete remission for all patients, indicating that Foscan-based PDT could be an effective treatment option for early-stage tumors that have not spread to the local lymph nodes. This demonstrates the potential of mTHPC-mediated PDT in providing a successful treatment outcome for patients with these types of tumors [100]. Additionally, the use of Foscan-mediated PDT employing mTHPC as a photosensitizer has been applied to patients with stage IV advanced and/or recurrent tongue base carcinoma. The treatment has been successful in reducing tumor-associated symptoms, as well as improving breathing, swallowing, and speech (voice) problems. This demonstrates the potential of Foscan-mediated PDT as an effective treatment option for late-stage and recurrent tongue-based carcinoma, providing both tumor reduction and improved quality of life for patients [101].
Taken together, Foscan-mediated photodynamic therapy has shown promising results in the treatment of early oral squamous cell carcinoma, lip cancer, and advanced head and neck cancer. The treatment has demonstrated high response rates, favorable functional outcomes, and potential as a salvage therapy for patients with incurable or recurrent disease. However, further research and larger clinical trials are necessary to validate these findings and optimize treatment protocols for a wider range of patients.
Chlorin e6 and HPPH
Chlorin e6 and HPPH (Hexylaminolevulinate-mediated PDT) are two photosensitizing agents utilized in PDT for the treatment of various medical conditions, including oral cancers [102, 103].
Chlorin e6 is a synthetic chlorin-based photosensitizer that selectively accumulates in tumor tissues and generates ROS upon light activation, leading to tumor cell death. It has been investigated for its potential in PDT for lung, breast, and bladder cancer [103, 104]. HPPH, on the other hand, is a second-generation photosensitizer derived from porphyrin. It is primarily used for the diagnosis and treatment of early-stage or pre-cancerous lesions such as actinic keratosis and bladder cancer. HPPH is either topically applied or administered intravesically, and upon light activation, it induces cell destruction. Notably, the selection of Chlorin e6 or HPPH as a photosensitizer depends on factors like the specific medical condition, disease stage, and the properties of the sensitizing agent, allowing for tailored treatment approaches in PDT [103, 105, 106].
In a study conducted by Sobaniec et al., the potential of PDT as a treatment for oral leukoplakia was investigated. Oral leukoplakia is a precancerous condition characterized by white patches or plaques on the oral mucosa. The study involved 23 patients diagnosed with oral leukoplakia. The patients received treatment with chlorin e6, specifically using a product called Photolon®, which contained 20% chlorin e6 and 10% dimethylsulfoxide as a photosensitizer. PDT treatment sessions were scheduled biweekly, meaning patients underwent the therapy every two weeks. The results of the study demonstrated that PDT using chlorin e6 led to a significant reduction in the size of the oral leukoplakia lesions. On average, the size of the lesions decreased by approximately 55% following the treatment. This reduction in lesion size indicates a positive response to the PDT treatment, suggesting its potential efficacy in managing oral leukoplakia [107].
However, it is important to note that the study focused specifically on the use of chlorin e6 in PDT for oral leukoplakia and that the results were obtained from a relatively small sample size. Notably, the study provides valuable insights into the potential use of PDT as a therapeutic approach for this precancerous oral condition [107].
In another clinical trial involving patients with oral dysplasia, carcinoma in situ (an early stage of cancer), or early-stage HNSCC, HPPH was utilized. The patients received systemic administration of HPPH at a dose of 4 mg/m², 22–26 h before the light was delivered. Following the administration of HPPH, the tumor site was illuminated with light at various doses ranging from 50 to 140 J/cm². The results of the trial, assessed on day 28 following treatment, revealed promising outcomes. Among the patients, 58% achieved a complete response, indicating the complete eradication of the targeted lesions. Additionally, 11% of patients demonstrated a partial response, indicating a significant reduction in tumor size or extent. Another 11% of patients had stable disease, meaning there was no significant change in the tumor’s status. These findings suggest that the use of HPPH in PDT holds potential as an effective treatment option for patients with oral dysplasia, carcinoma in situ, or early-stage HNCSS. The high complete response rate indicates the ability of HPPH-mediated PDT to achieve complete eradication of the targeted lesions. The partial response and stable disease rates further demonstrate the therapeutic efficacy, as they indicate favorable disease control and stability [108].
These findings indicate that PDT using chlorin e6 and HPPH as photosensitizers has shown promise in the treatment of oral leukoplakia, oral dysplasia, carcinoma in situ, and early-stage HNSCC. The treatments resulted in a reduction in lesion size and a significant proportion of patients achieving complete or partial responses. However, further research and clinical trials are needed to validate these results and optimize treatment protocols for these specific conditions.
Photosensitizers in in vitro Studies
The studies described different photosensitizers and their effectiveness in PDT for oral cancer treatment. The researchers evaluated various compounds, including sulfanyl porphyrazines, tribenzoporphyrazines, and other photosensitizers like zinc phthalocyanine and aluminum phthalocyanine chloride [108–112]. In these studies, researchers focused on developing and evaluating different types of photosensitizers, which are compounds that can induce cell death when activated by light, for their cytotoxic effects on oral cancer cells. They conducted experiments using various compounds and tested their effectiveness in killing oral cancer cells when exposed to light.
The initial experiments involved sulfanyl porphyrazines labeled as 4-fluorobutyl (1a) and 2-(2-ethoxyethoxy) ethyl (1b). These compounds were tested on two different types of oral cancer cell lines derived from the tongue (HSC-3) and buccal mucosa (H413). The researchers found that at concentrations up to 50 µM, compounds 1a and 1b did not exhibit toxicity in the absence of light. However, at the highest concentration, both compounds showed aggregation. When exposed to light within the range of 600 to 850 nm, porphyrazine 1b did not induce any light-induced toxicity in either cell line. In contrast, 1a reduced the viability of H413 cells by about 30–35% at both concentrations. Importantly, the observed phototoxicity varied between the two cell lines [113].
Further investigations involved other porphyrazines and tribenzoporphyrazine, which had annulated diazepine rings. These compounds were tested on the same oral cancer cell lines, HSC-3 and H413. Dark toxicity experiments showed minimal toxicity, except for tribenzoporphyrazine on H413 cells at higher concentrations. However, under LED light irradiation at 690 nm, tribenzoporphyrazine demonstrated significant photocytotoxicity, especially against HSC-3 cells [114].
The researchers discussed several potential administration routes for liposomal photosensitizers. They suggested direct injection into tumors or transmucosal administration by stable adhesion to the mucosa using cationic liposomes. Another possibility was embedding liposomes in oral films to facilitate transmucosal transport [115–119]. A study also investigated the phototoxic effects of other sulfanyl porphyrazines labeled as 4a and 4b (with 4-bromobenzyl and 4-biphenylylmethyl substituents) in free-form and liposomal formulations. Liposomes composed of DOTAP: POPC showed high photocytotoxicity against HSC-3 cells when incorporating 4a, while cationic DOTAP: POPC liposomes demonstrated light-induced toxicity against HSC-3 cells when incorporating 4b. These results highlighted the potential of liposomal formulations as drug delivery systems for sulfanyl porphyrazines, with the effectiveness depending on the specific photosensitizer structure [120].
In addition to porphyrazines, researchers also evaluated magnesium(II) and zinc(II) porphyrazines with different substituents. These porphyrazines were tested on squamous cell carcinoma cell lines derived from the tongue (SCC-25 and CAL-27). The photosensitizers were tested in their free forms as well as in liposomal formulations. The study found that the magnesium(II) porphyrazine with morpholinoethyl groups exhibited high photocytotoxicity on both cell lines, while the zinc analog was less effective, only affecting the SCC-25 cells. This indicates that the magnesium(II) porphyrazine with morpholinoethyl groups has a greater potential as a photosensitizer in photodynamic therapy for treating cancer, as it was effective against both cell lines. Liposomal formulations generally enhanced the cytotoxic effect of the photosensitizers [121].
The researchers also investigated sulfanyl tribenzoporphyrazines with dendrimeric moieties. These compounds were tested on CAL-27 and HSC-3 cells. The tribenzoporphyrazine with branched G1-dendrimeric substituents showed moderate activity against CAL-27 cells and higher activity against HSC-3 cells. The photocytotoxicity decreased when the dendrimeric substituent generation was reduced. However, the lowest nanomolar IC50 values were observed for a phthalocyanine derivative with hydroxymethyl groups, which exhibited potent photodynamic activity [122].
Porphyrinoid compounds, including phthalocyanines, were studied for their phototoxic effects on oral cancer cells. Zinc phthalocyanine and aluminum phthalocyanine chloride were tested on HSC-3 and HeLa cells. Both phthalocyanines showed a phototoxic effect, but the effectiveness varied depending on the cell type. These results suggest that certain porphyrinoid compounds, such as phthalocyanines, have the potential as photosensitizers for photodynamic therapy in treating oral cancer, and further research is needed to optimize their use and determine their effectiveness in clinical settings [123]. The study found that zinc phthalocyanine had a more potent phototoxic effect on HSC-3 cells, while aluminum phthalocyanine chloride was more sensitive to HeLa cells, suggesting the effectiveness of phthalocyanines in photodynamic therapy [124]. The studies also evaluated other porphyrinoid photosensitizers, such as a water-soluble N-confused porphyrin [125] and glycerol-substituted phthalocyanines [126], on various cancer cell lines, including OSCC. Table 1 summarizes some important in vitro studies evaluating PDT in oral cancer cells.
Table 1.
A summary of in vitro studies evaluating PDT in oral cancer cells
| Cell Types | PDT Type | Photosensitizers | Outcome | Ref |
|---|---|---|---|---|
| SGT cells | Illumination 4 h after PS administration | ALA, ALA-hx | 613–645 nm red LED (5 J/cm2) | [127] |
| Cal-27 hOSCC cell line | Photodestruction assessed using MTT assay | Gold nanorods, rose bengal | 532 nm green LED (170 mw/cm2) for 90 s | [128] |
| FaDu, FaDuPTX hPSCC cell line | Preincubation with Pa followed by assessment | Pa | 613–645 nm LED (1.2 J/cm2); Inhibited tumor growth via HOXC6/MDR-1 pathway suppression | [129] |
| S462, A375, A549, C26, CL1-0, CL1-5, NSC, NIH3T3 | ALA treatment followed by light irradiation | ALA | 635 nm diode laser (30 mw/cm2); Selective growth suppression in tumor cells | [130] |
| SCC-25, 562 HNSCC cell lines | Exposure to MB before illumination | MB | 660 nm diode laser for 8 min; Significant growth inhibition in both cell lines | [131] |
| SCC25 | Evaluation of ALA concentrations and PpIX production | ALA | 635 nm laser (87 mw/cm2, 10.4 J/cm2); Induced cytotoxicity and apoptosis via ROS generation | [132] |
| Human OSCC cell lines | Measurement of intracellular ROS levels | PaH | 405 nm semiconductor laser; Significant phototoxic effect by inhibiting cell proliferation | [133] |
| CAL-27, HOEC | Synthesis of PEGlated prodrug of doxorubicin for NP-encapsulated HP | HP | 633-nm laser for 10 min (100 mw/cm2); Strong PDT efficiency with suitable cellular uptake | [134] |
| DOK, CAL-27 | Incubation with ALA followed by various measurements | ALA | 635 nm laser (87 mw/cm2, 10.4 J/cm2); Selective inhibition of proliferation and induction of apoptosis | [135] |
| SCC25 | Evaluation of ALA’s individual and synergistic effects | ALA | 635 nm laser (87 mw/cm2, 10.4 J/cm2); Remarkable synergistic apoptosis induction effect | [136] |
| CAL27, FaDu | Study of cell death using Calcein-AM/PI Double Staining Kit | ICG, EVO | 808 nm laser (100 mW/cm2) for 5 min; Efficient tumor suppression and apoptosis induction | [137] |
| SCC 25, SCC 9, HOK | bioavailability of PEGylated GQDs was evaluated in hOSCC and normal cells | GQDs | Laser for 10 min. GQD-PEG dominantly contributed to PDT efficacy in triggering antitumor immune responses | [138] |
Light Sources
All light sources follow a similar principle, where the input energy is transformed into light. Light is generated through spontaneous emission, where excited atoms emit photons in a random manner in an incoherent light source, like a lightbulb. As a result, this process produces radiation that spreads in all directions, encompassing a broad range of wavelengths. The emitted photons do not have any correlation with each other, meaning they are not synchronized or coordinated [51, 139].
As mentioned earlier, PDT utilizes a combination of a photosensitizing agent and light to selectively destroy abnormal cells, such as cancer cells. PDT relies on different light sources, each with its characteristics and advantages, to deliver the necessary light energy for the treatment.
Lasers, a commonly used light source in PDT, emit coherent and monochromatic light. This coherence allows lasers to produce a focused and concentrated beam of light, which is crucial for targeting specific areas during treatment. They can deliver high optical power and can be precisely tuned to match the absorption wavelength of the photosensitizer used in PDT. Notably, lasers are often connected to optical fibers for light delivery and beam-expanding lenses can be used to cover larger areas of tissue evenly [140–143].
Dye lasers, another light source used in PDT, use organic dye molecules as the lasing medium. They emit light within a specific range of wavelengths that corresponds to the absorption wavelength of certain photosensitizers. Dye lasers provide flexibility in selecting the appropriate wavelength for different photosensitizers. However, they tend to be less portable and more complex, requiring specialized equipment such as a high-voltage power supply, high current, and water cooling [51, 144].
Diode lasers, which utilize semiconductor materials, offer advantages over dye lasers in terms of cost, size, portability, stability, and weight. They are compact, lightweight, and highly stable, and can provide high power by combining multiple laser diodes. However, diode lasers emit a larger and more widely spread beam compared to dye lasers, and each diode laser has a fixed wavelength, requiring different laser units for each photosensitizer [51].
Light-emitting diodes (LEDs) are semiconductor devices that produce incoherent light. They have a broader spread of light and a wider spectral width compared to lasers. LEDs are generally less powerful but offer affordability and portability. They are suitable for superficial tumor treatments and can be used in endoscopic and interstitial applications. LEDs are particularly useful in areas with limited access to advanced medical care due to their low cost and ease of use [51, 145–148].
Lamps, which were commonly used in the early stages of PDT, emit a broad spectrum of light. Different types of lamps, such as fluorescent, incandescent, metal halide, xenon arc, and sodium arc lamps, were employed. Lamps require optical filters to select the appropriate wavelengths for photoactivation. They are generally used for superficial tumors, but dosimetry becomes more complex with broadband light sources [51, 141, 149].
In conclusion, the choice of light source in PDT depends on various factors, including the type and location of the target tissue, the specific photosensitizer used, and the desired treatment depth. Lasers offer coherence and precision, dye lasers provide flexibility, diode lasers offer compactness and stability, LEDs are affordable and portable, and lamps emit a broad spectrum. Selecting the appropriate light source is crucial in PDT to ensure optimal therapeutic outcomes.
Effects of PDT on Different Types of Oral Cancers in Clinical Studies
PDT has shown promise as a treatment for various oral cancers with the ability to selectively target and destroy tumor cells while preserving normal tissue. Table 2 summarizes some important clinical trials of PDT impacts on oral cancers.
Table 2.
An overview of key clinical trials assessing the effects of PDT on oral cancers
| Type of study | Included Patients | PDT Type | Outcomes | Ref |
|---|---|---|---|---|
| Clinical trial phase I | Oral dysplasia/CIS/early-stage HNSCC | HPPH-PDT | HPPH-PDT proved to be a safe treatment option for the three types of cancer studied, especially for early-stage oral cancer | [108] |
| Retrospective study | No oral squamous cell carcinoma and oral mucosal dysplasia | Photofrin®-PDT | The treatment led to full recovery without any lasting functional or aesthetic issues. | [94] |
| Retrospective study | One patient with recurrent BOT-SCC with a history of radiotherapy and one with a history of concomitant chemoradiotherapy | Temoporfin-PDT | Outstanding oncological and functional outcomes, with no recurrence observed over one to two years of follow-up | [150] |
| Phase 1 clinical trial | High-grade dysplasia/CIS or micro-invasive SCC | ALA-PDT | The combined PDT reduced light restriction periods but led to some adverse effects, such as an initial high rate of marginal recurrence, grade 3 mucositis, odynophagia, voice changes, photosensitivity, and grade 5 sepsis. | [151] |
| Retrospective study | Superficial oral SCC or CIS | Photofrin®-PDT | The combined PDT yielded satisfactory results in managing superficial oral cancer, yet it led to adverse effects, such as recurrence (particularly in red patches), photosensitivity, sequestrum formation, maxillary sinus perforation, pain, and swelling. | [152] |
| Retrospective cohort analysis | Oral cavity cancer | Meta-tetrahydroxy phenyl chlorin (mTHPC)- PDT | Outstanding disease-free survival outcomes were achieved with post-surgery PDT at a minimum 6-week interval. | [153] |
| Prospective cohort clinical study | T1/T2 N0 oral SCC | mTHPC-PDT | A comparable modality with reduced morbidity in managing low-risk tumors | [154] |
| Retrospective clinical study | Cancerous lesions of the gingiva and oral mucosa | Topical ALA-PDT synchronized with ICT | Explored as a safe and beneficial addition to ICT for patients with localized OSCC | [155] |
| Clinical case report | An extensive tumor on the mouth floor | PDT with Redaporfin | Observation of complete destruction of all visible tumors | [156] |
| Prospective cohort clinical study | Stage IV tongue base carcinoma | Ultrasound-guided interstitial PDT + Foscan | Successful treatment of advanced/recurrent tongue base carcinoma | [157] |
| Clinical trial | High-risk dysplasia, CIS, and T1 SCC of the larynx | HPPH-mediated PDT | Beneficial for early-stage laryngeal cancer | [158] |
| Clinical study | Oral SCC without metastasis | talaporfin sodium-mediated PDT (t-PDT) | t-PDT is potentially beneficial for oral SCC treatment, as Talaporfin sodium is rapidly eliminated from the body | [159] |
| Retrospective clinical study | Early-stage neoplasms of the oral cavity and oropharynx (Tis-T2) | mTHPC-PDT | PDT yielded more favorable outcomes, with overall and complete response rates of 90.7% and 70.8%, respectively | [99] |
| A cohort study | Early-stage oral cavity malignancies | mTHPC + PDT | PDT could be beneficial as an alternative to surgery | [160] |
| Retrospective clinical study | Early stage OSCC | mTHPC + PDT | Comparable outcomes to surgery for T1 tumors, but not for T2 tumors | [161] |
| Retrospective cohort analysis | Oral/oropharyngeal SCC | mTHPC + PDT | Offering the potential for achieving an acceptable toxicity profile and stable outcomes | [162] |
| Clinical study | Recurrent tongue cancer | mTHPC + iPDT | Being beneficial in inoperable tumors as an alternative to palliative care | [163] |
| Clinical study | Recurrent paranasal sinus tumors | mTHPC + PDT | Being safe when surgery only partially removes these tumors | [164] |
| Clinical study | Persistent/recurrent NPC | NP-PDT | Being effective in treating these kinds of cancers when they are unsuitable for conventional treatments. An effective strategy involves combining NP-PDT and ENT-MNS. | [165] |
| Clinical study | Laryngeal malignancies | HpD/temoporfin + PDT | PDT presents a viable and safe alternative with a success rate akin to conventional methods. There is a potential for preserving organs and functions with this therapy. | [166] |
| Cohort case series | Recurrent advanced nasopharynx carcinoma | mTHPC + PDT | Successful management of nasopharyngeal cancer was achieved using this therapy as a palliative measure. | [167] |
| Clinical trial | Persistent/recurrent NPC | temoporfin + PDT | Residual or recurrent nasopharyngeal cancer can be treated with this therapy. | [168] |
| Phase II clinical study | Local recurrent or residual NPC | Foscan® | NPC failures with a depth of less than 10 mm can be treated effectively with PDT | [169] |
| Retrospective clinical study | Tis-T2N0M0 oral/oropharynx SqCCA | Photofrin®-PDT | Being curative in primary/failed cases of early malignancies of the oral cavity/ oropharynx | [170] |
| Retrospective clinical study | Residual/recurrent HNSCC | Porfimer sodium-PDT | Being effective therapy to treat HNSCC leads to an increase in the quality of life. | [171] |
| Clinical trial phase I | HNSCC | HPPH-PDT | In adjuvant application of surgery, HPPH-PDT appears to be safe | [172] |
| Retrospective clinical study | Recurrent/secondary Oropharyngeal/oral carcinoma | Temoporfin-PDT | Being safe as it has low toxicity | [173] |
Oral Squamous Cell Carcinoma (OSCC)
OSCC is a malignant tumor originating from the squamous epithelium of the oral cavity. Histopathological examination of OSCC involves analyzing tissue sections from biopsied or surgically resected specimens. Key features evaluated include histological grade, tumor invasion depth and patterns, keratinization, nuclear features, and the tumor microenvironment. Well-differentiated OSCC closely resembles normal squamous epithelium, while poorly differentiated OSCC shows little resemblance. The presence of an inflammatory infiltrate, tumor-associated stroma, and desmoplastic reaction may also be noted. Immunohistochemistry can provide additional information about differentiation, proliferation, and viral etiology. Histopathology plays a crucial role in determining the tumor stage, prognosis, and treatment planning for OSCC [174–176] (Fig. 3).
Fig. 3.

Histopathological examination of OSCC involves analyzing tissue sections from biopsied or surgically resected specimens. One of the key features evaluated is the differentiation of the tumor. Well-differentiated OSCC closely resembles normal squamous epithelium, exhibiting organized tissue architecture and possible keratinization. Moderately differentiated OSCC shows some loss of differentiation compared to normal cells, with variable sizes and shapes. Poorly differentiated OSCC bears little resemblance to normal squamous cells, lacking organized architecture and often appearing as sheets or cords of cells. Poorly differentiated OSCC tends to grow rapidly and has a higher likelihood of metastasis, resulting in a poorer prognosis compared to well-differentiated and moderately differentiated OSCC. Histopathological examination also considers other features such as tumor invasion patterns, nuclear characteristics, and the presence of an inflammatory infiltrate or desmoplastic reaction. Immunohistochemistry can provide additional information about differentiation, proliferation, and viral etiology, such as HPV infection. Overall, histopathology plays a critical role in diagnosing OSCC, determining its aggressiveness, and guiding treatment decisions
A study evaluated the effectiveness of Photofrin-mediated PDT for early carcinoma and dysplasia in the oral cavity. Over a period of four years, 25 patients with OSCC and mucosal dysplasia received PDT treatment at Nagasaki University Hospital. The results showed a high success rate, with a complete response achieved in 96% of the patients, and a partial response in one patient. Recurrence was observed in three patients, but salvage surgery or a second PDT was performed. The disease-specific survival rate was calculated at 96%. Treatment-related edema and pain were experienced by all patients, requiring pain management for several weeks. However, complete healing occurred within 4–6 weeks, and no long-term functional or esthetic issues were reported. This study highlights the promising outcomes of Photofrin-mediated PDT for early oral malignancies and dysplasia, supporting its potential as a minimally invasive treatment option in these cases [177]. [176]
Another study aimed to assess the efficacy of PDT in treating superficial OSCC and examine the long-term clinical outcomes. A total of 34 patients with superficial oral cancers received PDT with Photofrin as the photosensitizer. Photofrin was administered intravenously (2 mg/kg) 48 h before light irradiation. Photoradiation was performed using a 630-nm excimer dye laser at doses of 100–150 J/cm². After six months, complete responses were observed in 88.2% of patients, but during long-term follow-up, 26.5% experienced local relapses. The 5-year overall survival, disease-specific survival, and disease-free survival rates for superficial oral carcinomas treated with Photofrin-mediated PDT were 76.5%, 84.6%, and 63.3%, respectively. Lesions with red patches had a significantly higher recurrence rate compared to white patches, highlighting the need for accurate lesion evaluation and appropriate photoradiation to improve outcomes. Adverse events, such as sunburn and sequestrum formation of alveolar bone, were reported, but no abnormal laboratory values or systemic complications were observed. In conclusion, PDT using Photofrin demonstrated effectiveness in treating superficial oral carcinomas, yielding excellent healing outcomes with minimal side effects [152].
Some studies indicate that for oral cavity tumors with low risk, PDT using a specific photosensitizer called mTHPC can be a viable alternative to traditional treatment methods such as chemotherapy, radiotherapy, and surgery. PDT is considered less invasive and has fewer associated side effects compared to these conventional therapies. Even if multiple rounds of PDT treatment are required, it remains a less burdensome option for patients. Additionally, the study highlights the potential of a specific type of PDT called ALAPDT, which involves the use of a topical application of aminolevulinic acid. ALAPDT shows promise as a safe therapy for patients with locally advanced OSCC. It is suggested that ALAPDT could be a valuable complement to platinum-based induction chemotherapy (ICT) in the treatment of these patients, potentially enhancing the overall treatment outcomes [154, 155].
In a study of eight patients with non-metastatic oral SCC, talaporfin sodium-mediated photodynamic therapy (t-PDT) was assessed. Biopsies conducted 4–6 weeks after t-PDT revealed that six out of eight cases achieved a complete response (CR) and two cases showed a partial response (PR). Although one of the CR cases experienced recurrence after 9 months and required tumor resection, there was no recurrence observed after surgery. Unfortunately, the two cases with PR succumbed to cancer despite additional PDT treatment. The study concluded that t-PDT is an effective treatment strategy for oral SCC, and talaporfin sodium offers the advantage of efficient elimination from the body compared to porfimer sodium [159].
According to Schweitzer et al.’s investigation, PDT is an attractive additional treatment option for the primary management of superficial oral and oropharyngeal carcinomas that have a low risk of nodal metastases. The study suggests that PDT can be used as a local clinical oncologic treatment in cases of Tis-T2N0M0 SCC of the oral cavity and oropharynx. This implies that PDT can be a beneficial approach for early-stage cancers that have not spread to the lymph nodes. The findings of the investigation highlight the potential of PDT as a valuable therapeutic option for select patients with superficial oral and oropharyngeal carcinomas, providing an alternative to conventional treatment methods [170].
Furthermore, Karakullukcu et al. have highlighted the potential benefits of PDT as a treatment option for early-stage oral cavity cancer compared to surgery. Specifically, PDT is well-suited for cancers that are smaller than 5 mm in diameter and without lymph node metastases. Additionally, patients with an increased risk of developing multiple oral malignancies, such as those with extensive leukoplakia or erythroplakia, can greatly benefit from PDT’s tissue-sparing properties. By minimizing invasive procedures and preserving oral function, PDT offers a promising alternative for treating early-stage oral cancer [178].
Visscher et al. conducted a study comparing the effectiveness of PDT using mTHPC and transoral surgery in treating primary T1 oral cavity tumors, finding them to be equally effective. However, for T2 tumors, PDT yielded inferior outcomes compared to surgery. The study also found that both PDT and surgery had similar overall survival rates for T1 and T2 tumors following treatment. These results suggest that while PDT and surgery can be comparable options for T1 tumors, surgery may be more suitable for T2 tumors. Additionally, the study highlights the need for further research to optimize PDT protocols for the treatment of T2 tumors [179]. Further research is needed to compare the morbidity associated with PDT and standard treatments, as well as to conduct prospective and comparative studies that assess the efficacy of PDT. This will provide a more comprehensive understanding of PDT’s effectiveness and help determine its role in the management of oral cavity cancer.
Taken together, PDT has shown high success rates and promising outcomes in treating early oral carcinoma, dysplasia, and superficial oral cancers, with minimal side effects and potential as a minimally invasive alternative to conventional treatments.
Recurrent SCC of the Base of the Tongue
A study focused on exploring the use of postoperative temoporfin-mediated PDT as an adjuvant treatment for patients with recurrent SCC at the base of the tongue who had involved resection margins following transoral robot-assisted salvage surgery (TORS) after primary (chemo)radiotherapy. Two patients in this situation underwent TORS but were found to have involved resection margins based on postoperative pathology reports. To address the risk of further recurrence, temoporfin-mediated PDT was employed as a novel adjuvant approach to target and treat any remaining microscopic disease at the resection margins. The results showed encouraging outcomes, with both patients achieving good oncological and functional results. They remained disease-free at 42 and 24 months of follow-up and were able to speak, breathe, and eat normally. This suggests that postoperative temoporfin-mediated PDT could be effective in achieving successful oncological outcomes and functional recovery for selected patients who undergo salvage surgery with involved resection margins at the base of the tongue [180].
In a prospective study, US-iPDT (ultrasound-guided interstitial photodynamic therapy) was evaluated as a treatment for stage IV tongue base carcinoma. Twenty-one patients with advanced and/or recurrent tongue base cancer received US-iPDT using mTHPC as the photosensitizing agent. The treatment resulted in significant improvements in breathing, swallowing, and speech for the majority of patients. Clinical assessment showed positive responses in over half of the patients, while radiological assessment revealed stable or minimally responsive pathology in most cases. Although some patients passed away during the follow-up period, US-iPDT demonstrated promising results as a palliative treatment option for advanced and/or recurrent tongue base carcinoma [157]. To further expand, PDT, specifically iPDT, has emerged as a viable treatment option for nonmetastatic recurrent base of tongue tumors in patients who are ineligible for surgery or radiation therapy. The use of iPDT has been shown to offer long-term disease control and provide a curative alternative to palliative care. By effectively treating the tumors, iPDT can significantly improve the quality of life for these patients, providing them with a more promising prognosis [181].
The bottom line is that both the use of postoperative temoporfin-mediated PDT and US-iPDT show promise as treatment options for patients with recurrent SCC at the base of the tongue. Postoperative temoporfin-mediated PDT as an adjuvant treatment after salvage surgery with involved resection margins has demonstrated positive oncological outcomes and functional recovery. US-iPDT has shown significant improvements in symptoms and disease control for patients with advanced and/or recurrent tongue base carcinoma, serving as a potential palliative treatment option. These findings suggest that PDT techniques offer valuable therapeutic approaches for tongue base carcinoma patients, either as adjuvant or palliative interventions.
Head and Neck SCC/Malignant Tumors of Paranasal Sinuses
As to findings, PDT has been shown to have the clinical benefit in a surgery-adjuvant treatment for HNSCCs and related conditions.
One study focused on the surgery-PDT time intervals and their impact on patient outcomes. The study involved patients who underwent surgery for HNSCC and received PDT using a photosensitizer called mTHPC. The timing of light delivery during PDT was dependent on the size and location of the tumor. According to this study, there is evidence to suggest that patients who undergo PDT with shorter intervals between surgery and PDT experience fewer adverse events. This finding indicates that PDT could serve as a potential alternative approach to complement surgery in the treatment of malignancies with tumor resection margins. This is particularly valuable in cases where treatment options are limited [182].
Ahn et al., in 2016, conducted a phase 1 clinical trial to assess the use of PDT with ALA for early superficial lesions in the head and neck. The trial involved 35 subjects with high-grade premalignant and early squamous cell carcinoma. After oral administration of ALA, subjects received escalating intraoperative light doses. The treatment was generally well-tolerated, with manageable toxicities such as mucositis, odynophagia, voice alteration, and photosensitivity reactions. However, there was one death that might have been related to the treatment, as well as one case of sepsis. Over a median follow-up period of 42 months, 34% of patients experienced local recurrence, while 34% developed recurrence adjacent to the treated area. The study suggests that ALA-PDT is tolerable, and longer follow-up is needed to determine the impact of light dose on local recurrence. The findings also indicate the potential need for larger treatment fields to address high marginal recurrence rates [151].
Another PDT procedure utilized a photosensitizer called 3-(1’-hexyloxyethyl) pyropheophorbide-a (HPPH) for the treatment of early-stage HNSCC, advanced dysplasia, and/or carcinoma in situ (CIS). The trial demonstrated that HPPH-PDT is a safe therapy for the mentioned diseases, particularly for HNSCC. This suggests that PDT using HPPH can be a viable treatment option for patients with early-stage HNSCC or precancerous lesions [183].
In a case report study, researchers investigated the combination of Redaporfin PDT with ICIs as a treatment approach for challenging or resistant cases of HNSCC. By combining the tumor-targeting effects of Redaporfin PDT with the immune-activating properties of ICIs, the researchers aimed to maximize tumor destruction. The study demonstrated promising results, showing improved outcomes and prolonged survival times in HNSCC patients who had previously shown resistance to other treatments. This combination therapy approach holds potential as a novel treatment option for patients with difficult-to-treat or resistant HNSCC cases. However, further research and larger-scale studies are needed to validate these findings and fully explore the effectiveness and broader applicability of this therapeutic strategy [156].
Furthermore, Hosokawa et al. have shown that PDT can be a valuable treatment option for patients with residual and recurrent HNSCC to enhance their quality of life. The study emphasized the potential of PDT in managing symptoms and improving the overall well-being of patients with recurrent HNSCC, offering a promising alternative to traditional treatment options. By alleviating symptoms and reducing the negative impact of the disease, PDT can significantly improve the patient’s experience and contribute to a better prognosis [171].
The study conducted by Rigual et al. focused on investigating the adjuvant use of a photosensitizer called HPPH-PDT in combination with surgery for patients with HNSCC. The findings of the study indicated that this combined approach was safe for use. Similarly, the study by Caesar et al. supported the use of PDT as an adjunct to surgery in cases of recurrent tumors in the paranasal sinuses and the anterior skull base, where complete tumor removal is not feasible [172].
An important aspect highlighted in the study by Caesar et al. was the absence of serious complications such as cerebrospinal fluid leak, meningitis, major bleeding, or vision loss when PDT was employed alongside surgery. This suggests that PDT can be considered as a viable additional treatment option for patients in these specific cases where complete tumor resection is not possible. However, it is important to note that adverse events were reported in the studies. For example, transient diplopia (double vision) occurred in four patients due to edema of the medial rectus muscle, and one patient experienced severe necrosis leading to an oro-nasal fistula. Nevertheless, despite these adverse events, the treatment resulted in a complete response in five patients, indicating a positive therapeutic outcome [184].
To summarize, the clinical studies discussed highlight the potential of PDT as a surgery-adjuvant treatment for HNSCC and related conditions. They provide insights into the safety and efficacy of different photosensitizers in PDT for treating various stages of HNSCC and related pathologies. Additionally, the combination of PDT with other therapeutic modalities, such as immune checkpoint inhibitors, shows promise in improving treatment outcomes and extending survival in patients with challenging or resistant HNSCC cases.
Laryngeal/Oropharynx Neoplasms
PDT has shown clinical advantages and safety in the treatment of various types of head and neck cancers, as indicated by several studies. One study conducted by Shafirstein et al. focused on the use of PDT with the photosensitizer HPPH for early laryngeal cancer. The researchers concluded that HPPH-PDT could be safely used, provided that the light dose did not exceed 100 and patients were closely monitored for laryngeal edema immediately after treatment. They found that early-stage T1 SCC lesions responded better to HPPH-PDT compared to dysplasia/CIS lesions [158].
In another study, PDT was used successfully to treat laryngeal carcinoma. Out of ten patients, nine achieved successful outcomes. PDT alone was used in seven patients, while temoporfin, another photosensitizer, was used to treat four sarcomas. The study reported no harmful adverse effects, and post-treatment, five patients experienced improvement in their voices, with none experiencing vocal deterioration [166].
In their research, Karakullukcu et al. discovered that temoporfin-mediated PDT is a highly favorable treatment option for tongue tumors, soft palate, alveolar process, and retromolar trigone. This approach offers several benefits, including reduced morbidity and a satisfactory rate of complete response. Furthermore, temoporfin-PDT proves to be particularly effective for challenging lesions, such as recurring primary neoplasms in areas that have undergone previous surgery or radiation therapy, while maintaining minimal morbidity [99].
Similarly, the study conducted by Lambert et al. demonstrated the effectiveness of temoporfin-mediated PDT for the treatment of oral and/or oropharyngeal HNSCC. The results indicated that in 76.9% of cases, complete tumor response was achieved, and recurrence-free rates were reported. Notably, the outcomes were more favorable for oropharyngeal squamous cell carcinoma compared to oral cavity squamous cell carcinoma alone. The study also found that adverse events were manageable, and a significant number of patients maintained swallowing and upper airway functionality [162].
PDT has shown promise in the treatment of nasopharyngeal carcinoma (NPC). For instance, Succo et al. investigated its use for recurrent/persistent NPC and found that precision nasopharyngeal PDT may benefit patients who do not respond to other conventional therapies [165]. Similarly, another study focusing on recurrent advanced NPC demonstrated significant symptom reduction and tumor volume reduction with PDT [167].
In addition, in their respective studies, both Stoker et al. and Nyst et al. shed light on the potential benefits of PDT in the treatment of head and neck malignancies, including NPC. Stoker et al. demonstrated that PDT has comparable efficacy to surgery and reirradiation, suggesting it as a viable treatment option when surgical intervention or reirradiation is not feasible or preferred [169]. Likewise, Nyst et al. emphasized the advantages of PDT for NPC, such as its short treatment duration and the ability to be performed in an outpatient clinic under local anesthesia [168]. These findings collectively support the consideration of PDT as a convenient and well-tolerated alternative or adjunctive therapy for selected patients with head and neck malignancies, including NPC, in cases where other treatment options may be limited or less desirable.
In summary, these studies collectively provide evidence of the clinical advantages, safety, and efficacy of PDT in the treatment of various head and neck cancers. PDT has shown positive outcomes, minimal adverse effects, preservation of organ function, and improved quality of life for patients. However, it is important to consider individual patient factors and further research to determine the optimal use of PDT in clinical practice.
Theranostics and Photodynamic Therapy
The theranostic approach in PDT combines several modalities in a single system, allowing for precise drug delivery, therapy monitoring, improved tumor penetration, and controlled drug release. In the field of oral cancer research, liposomes are among the theranostic agents being explored. These liposomes serve as platforms for both MRI contrast agents and photosensitizers, enhancing relaxivity and photodynamic efficacy compared to liposomes with only the contrast agent. The theranostic strategy of merging diagnostic and therapeutic agents in a single system may lead to more targeted and precise treatment of oral cancer, improving patient outcomes [185].
To enhance the performance of PDT, targeted platforms have been developed. Wang et al. investigated iron-oxide nanoparticles targeted to head and neck cancer, which accumulated in tumors and reduced the size of squamous cell carcinoma xenografts [186]. Stimuli-responsive drug delivery systems have been employed in oral cancer research, taking advantage of the unique tumor microenvironment properties. One such example is the use of light-responsive drug delivery systems, which combine photodynamic and photothermal therapies, demonstrating synergistic therapeutic effects in treating HNSCC. The dual-therapy approach can enhance treatment efficacy, reduce drug resistance, and minimize side effects, offering a promising strategy for HNSCC management. Thus, these drug delivery systems, by leveraging the responsiveness to specific stimuli, can provide targeted and personalized treatment for oral cancer patients [187, 188].
In addition to combining different modalities, researchers have explored multimodal treatment approaches [189]. For instance, nanoplatforms combining photodynamic therapy and photothermal therapy have been developed using agents such as Rose Bengal and gold nanorods. These platforms demonstrated enhanced anti-cancer efficacy against oral cancer. Hybrid nanoparticles incorporating photothermal and photodynamic therapy agents have also been used to produce hyperthermia and ROS, effectively killing OSCC [128, 190].
Gene therapy has been combined with photodynamic therapy in a theranostic system to treat HNSCC. This dual-therapy approach targets the Wnt/β-catenin signaling pathway, which is involved in tumor progression, to enhance the efficacy of PDT. Nanoparticles delivering Wnt-1 siRNA and photodynamic therapy have shown significant inhibition of OSCC growth and increased cancer cell killing. This innovative strategy has the potential to improve treatment outcomes, decrease drug resistance, and minimize side effects for HNSCC patients. To clarify, through targeted delivery of Wnt-1 siRNA, the nanoparticles effectively suppress the expression of the Wnt-1 gene, which is involved in the Wnt/β-catenin signaling pathway. By attenuating the aberrant activation of this pathway, cancer cell proliferation and survival are reduced. When combined with PDT, which utilizes a photosensitizing agent and light activation to generate ROS and induce tumor damage, the efficacy of cancer cell killing is further enhanced. The synergistic effect of Wnt-1 suppression and PDT has demonstrated significant inhibition of OSCC growth and increased cancer cell death in preclinical studies. However, additional research is needed to validate these findings and explore the clinical potential of this combination therapy [191].
These studies highlight the potential of theranostic approaches in oral cancer treatment, offering enhanced drug delivery, therapy monitoring, and improved therapeutic outcomes. Thus, researchers, by combining different modalities and targeting strategies, aim to optimize the efficacy and safety of photodynamic therapy for the management of head and neck cancers.
Concluding Remarks and Prospective
PDT is a non-invasive treatment for subcutaneous tumors, focusing on oral, head, and neck cancers. Researchers aim to improve PDT by developing new photosensitizers that are more soluble, less toxic, and better at targeting cancer cells. One promising method is conjugating sugars to photosensitizers to enhance targeting of sugar receptors on tumor cells, exploiting tumors’ increased glucose consumption.
Two-photon PDT uses longer wavelengths of light for deeper tissue penetration, potentially treating deep-seated tumors. Advances in endoscopic devices, photosensitizers, and tumor vaccines are enhancing PDT’s effectiveness, including targeting cancer stem cells with antibody-conjugated photosensitizers. Topical ALA-PDT, using ALA as a photosensitizer, is a minimally invasive approach for oral cancer with minimal side effects and is suitable for outpatient settings. Researchers are also exploring upconversion nanoparticles to enable deeper tissue penetration and strategies to counter tumor hypoxia, such as introducing exogenous oxygen or inhibiting hypoxia-inducible factor 1, to improve PDT efficacy. Efforts are underway to discover better photosensitizers with improved properties. Currently, to the best of our knowledge, Photofrin and Chlorin e6 are the FDA-approved photosensitizer for clinical use in PDT. However, researchers are searching for photosensitizing agents with greater tissue penetration, narrower excitation wavelength bands, high excitation efficiency, selectivity for malignant tissue, good fluorescent properties, and rapid clearance from the body. Second-generation photosensitizers, such as Phthalocyanins, Bacteriochlorophyl, and Bacteriochlorin a, are currently being investigated. PDT can also be used as an adjunct to surgery, particularly in cases where tumor margins are unclear or radical resection is challenging. Intra-operative PDT has shown promise in preventing local recurrence in certain types of cancer. Additionally, researchers are exploring the concept of in situ photosensitizer synthesis, where a precursor is administered and preferentially accumulated or converted into an active photosensitizer by the targeted tissue.
Future studies in PDT, to the best of our knowledge, should focus on several key areas to enhance its efficacy and broaden its clinical applications. First, there is a critical need for the development of advanced photosensitizers that improve targeting specificity to cancer cells while reducing toxicity and enhancing solubility. This includes exploring novel strategies like conjugating sugars or other targeting molecules to photosensitizers to exploit tumor-specific characteristics such as increased glucose metabolism and surface receptors. Additionally, optimizing two-photon PDT for deeper tissue penetration and combining it with other therapies could improve treatment outcomes, particularly for deep-seated tumors. Overcoming tumor hypoxia remains a significant challenge, prompting research into innovative methods to enhance oxygen delivery within tumors or modulate the hypoxic tumor microenvironment to make PDT more effective. Moreover, advancing clinical applications with portable devices for outpatient use, refining endoscopic PDT techniques, and exploring PDT’s synergistic effects with immunotherapies or tumor vaccines are crucial avenues for future investigation. Ultimately, integrating these advancements could pave the way for personalized PDT approaches tailored to individual patient profiles, thereby improving overall treatment efficacy and patient outcomes across various cancer types.
In conclusion, PDT holds promise as a non-invasive treatment modality for subcutaneous tumors, particularly in the field of oral, head, and neck cancers. Ongoing research efforts focus on improving photosensitizers, enhancing tumor targeting, addressing tumor hypoxia, and optimizing treatment parameters. Advancing our understanding of PDT will ultimately lead to improved efficacy, expanded applications, and a better understanding of its clinical value.
Acknowledgements
Not applicable.
Abbreviations
- OSCC
Oral squamous cell carcinoma
- HNSCC
Head and Neck Squamous Cell Carcinoma
- PDT
Photodynamic therapy
- ALA
Aminolevulinic Acid
- PpIX
Protoporphyrin IX
Author Contributions
The core of the study came from MNA and ShG. All authors wrote the manuscript. MNA and ShG supervised the manuscript.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability
No datasets were generated or analysed during the current study.
Declarations
Ethics Approval and Consent to Participate
This research was a review, and no participants took part, so there was no need for it.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Shayan Golestani, Email: Shayan.golestani@gmail.com.
Mohsen Nabi Afjadi, Email: mohsennabi66@gmail.com, Email: mohsen.nabiafjadi@modares.ac.ir.
References
- 1.Mouth. and Oral Cancer Statistics [ https://www.wcrf.org/cancer-trends/mouth-and-oral-cancer-statistics/
- 2.Watters C, Brar S, Pepper T. Oral mucosa cancer. 2020. [PubMed]
- 3.Tan Y, Wang Z, Xu M, Li B, Huang Z, Qin S, et al. Oral squamous cell carcinomas: state of the field and emerging directions. Int J Oral Sci. 2023;15(1):44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gupta B, Johnson NW, Kumar N. Global Epidemiology of Head and Neck cancers: a Continuing Challenge. Oncology. 2016;91(1):13–23. [DOI] [PubMed] [Google Scholar]
- 5.Rigual NR, Thankappan K, Cooper M, Sullivan MA, Dougherty T, Popat SR, et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg. 2009;135(8):784–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mirzaei M, Hosseini SA, Ghoncheh M, Soheilipour F, Soltani S, Soheilipour F, Salehiniya H. Epidemiology and Trend of Head and Neck Cancers in Iran. Glob J Health Sci. 2015;8(1):189–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Irani S. New insights into oral Cancer-risk factors and Prevention: a review of literature. Int J Prev Med. 2020;11:202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aghiorghiesei O, Zanoaga O, Nutu A, Braicu C, Campian RS, Lucaciu O, Berindan Neagoe I. The world of oral Cancer and its risk factors viewed from the aspect of MicroRNA expression patterns. Genes (Basel). 2022;13(4). [DOI] [PMC free article] [PubMed]
- 9.Kumar M, Nanavati R, Modi TG, Dobariya C. Oral cancer: etiology and risk factors: a review. J Cancer Res Ther. 2016;12(2). [DOI] [PubMed]
- 10.Tolentino Ede S, Centurion BS, Ferreira LH, Souza AP, Damante JH, Rubira-Bullen IR. Oral adverse effects of head and neck radiotherapy: literature review and suggestion of a clinical oral care guideline for irradiated patients. J Appl Oral Sci. 2011;19(5):448–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Huang SH, O’Sullivan B. Oral cancer: current role of radiotherapy and chemotherapy. Med Oral Patol Oral Cir Bucal. 2013;18(2):e233–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Raber-Durlacher JE, Brennan MT, Verdonck-de Leeuw IM, Gibson RJ, Eilers JG, Waltimo T, et al. Swallowing dysfunction in cancer patients. Support Care Cancer. 2012;20(3):433–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sroussi HY, Epstein JB, Bensadoun RJ, Saunders DP, Lalla RV, Migliorati CA, et al. Common oral complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med. 2017;6(12):2918–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kim TE, Chang JE. Recent studies in photodynamic therapy for Cancer Treatment: from Basic Research to clinical trials. Pharmaceutics. 2023;15(9). [DOI] [PMC free article] [PubMed]
- 15.Gunaydin G, Gedik ME, Ayan S. Photodynamic therapy for the treatment and diagnosis of Cancer–A review of the current clinical status. Front Chem. 2021;9. [DOI] [PMC free article] [PubMed]
- 16.Alvarez N, Sevilla A. Current advances in photodynamic therapy (PDT) and the future potential of PDT-Combinatorial Cancer therapies. Int J Mol Sci [Internet]. 2024; 25(2). [DOI] [PMC free article] [PubMed]
- 17.Jiang W, Liang M, Lei Q, Li G, Wu S. The current status of photodynamic therapy in Cancer Treatment. Cancers (Basel). 2023;15(3). [DOI] [PMC free article] [PubMed]
- 18.Przygoda M, Bartusik-Aebisher D, Dynarowicz K, Cieślar G, Kawczyk-Krupka A, Aebisher D. Cellular mechanisms of Singlet Oxygen in Photodynamic Therapy. Int J Mol Sci. 2023;24(23). [DOI] [PMC free article] [PubMed]
- 19.Wachowska M, Muchowicz A, Firczuk M, Gabrysiak M, Winiarska M, Bobrowicz M, et al. Aminolevulinic Acid (ALA) as a Prodrug in Photodynamic Therapy of Cancer. Molecules. 2011;16:4140–64. [Google Scholar]
- 20.Abrahamse H, Hamblin MR. New photosensitizers for photodynamic therapy. Biochem J. 2016;473(4):347–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wang N, Zhao Z, Xiao X, Mo L, Yao W, Yang H, et al. ROS-responsive self-activatable photosensitizing agent for photodynamic-immunotherapy of cancer. Acta Biomater. 2023;164:511–21. [DOI] [PubMed] [Google Scholar]
- 22.Mang TS. Lasers and light sources for PDT: past, present and future. Photodiagn Photodyn Ther. 2004;1(1):43–8. [DOI] [PubMed] [Google Scholar]
- 23.Gunaydin G, Gedik M, Ayan S. Photodynamic therapy for the treatment and diagnosis of Cancer–A review of the current clinical status. Front Chem. 2021;9:686303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Neupane J, Ghimire S, Shakya S, Chaudhary L, Shrivastava VP. Effect of light emitting diodes in the photodynamic therapy of rheumatoid arthritis. Photodiagn Photodyn Ther. 2010;7(1):44–9. [DOI] [PubMed] [Google Scholar]
- 25.Shafirstein G. Current status of PDT in the United States. Photodiagn Photodyn Ther. 2023;41:103439. [Google Scholar]
- 26.Morton CA. Photodynamic therapy for nonmelanoma skin Cancer—and more? Arch Dermatol. 2004;140(1):116–20. [DOI] [PubMed] [Google Scholar]
- 27.Kim SJ, Kim HS, Seo YR. Understanding of ROS-Inducing Strategy in Anticancer Therapy. Oxid Med Cell Longev. 2019;2019:5381692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tada DB, Baptista MS. Photosensitizing nanoparticles and the modulation of ROS generation. Front Chem. 2015;3:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.El-Missiry MA, Abou-Seif M. Photosensitization induced reactive oxygen species and oxidative damage in human erythrocytes. Cancer Lett. 2000;158(2):155–63. [DOI] [PubMed] [Google Scholar]
- 30.Calixto G, Bernegossi J, de Freitas L, Fontana C, Chorilli M. Nanotechnology-based drug Delivery systems for photodynamic therapy of Cancer: a review. Molecules. 2016;21:342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sun B, Bte Rahmat JN, Zhang Y. Advanced techniques for performing photodynamic therapy in deep-seated tissues. Biomaterials. 2022;291:121875. [DOI] [PubMed] [Google Scholar]
- 32.Correia JH, Rodrigues JA, Pimenta S, Dong T, Yang Z. Photodynamic therapy review: principles, photosensitizers, applications, and future directions. Pharmaceutics. 2021;13(9). [DOI] [PMC free article] [PubMed]
- 33.Kwiatkowski S, Knap B, Przystupski D, Saczko J, Kędzierska E, Knap-Czop K, et al. Photodynamic therapy – mechanisms, photosensitizers and combinations. Biomed Pharmacother. 2018;106:1098–107. [DOI] [PubMed] [Google Scholar]
- 34.Allison RR, Moghissi K. Photodynamic therapy (PDT): PDT mechanisms. Clin Endosc. 2013;46(1):24–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Robertson CA, Evans DH, Abrahamse H. Photodynamic therapy (PDT): a short review on cellular mechanisms and cancer research applications for PDT. J Photochem Photobiol B. 2009;96(1):1–8. [DOI] [PubMed] [Google Scholar]
- 36.Castano A, Demidova T, Hamblin M. Mechanisms in photodynamic therapy: part two - Cellular signaling, cell metabolism and modes of cell death. Photodiagnosis Photodyn Ther. 2005;2:1–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Przygoda M, Bartusik-Aebisher D, Dynarowicz K, Cieślar G, Kawczyk-Krupka A, Aebisher D. Cellular mechanisms of Singlet Oxygen in Photodynamic Therapy. Int J Mol Sci [Internet]. 2023; 24(23). [DOI] [PMC free article] [PubMed]
- 38.Sharma D, Singh S, Kumar P, Jain G, Aggarwal G, Almalki W, Kesharwani P. Mechanisms of photodynamic therapy. 2023. pp. 41–54.
- 39.Pallavi P, Girigoswami A, Girigoswami K, Hansda S, Ghosh R. Photodynamic therapy in Cancer. In: Chakraborti S, editor. Handbook of oxidative stress in Cancer: therapeutic aspects. Singapore: Springer Nature Singapore; 2022. pp. 1285–308. [Google Scholar]
- 40.Yao Q, Fan J, Long S, Zhao X, Li H, Du J et al. The concept and examples of type-III photosensitizers for cancer photodynamic therapy. Chem. 2021;8.
- 41.Rak J, Kabesova M, Benes J, Pouckova P, Vetvicka D. Advances in Liposome-Encapsulated Phthalocyanines for photodynamic therapy. Life [Internet]. 2023; 13(2). [DOI] [PMC free article] [PubMed]
- 42.Mroz P, Yaroslavsky A, Kharkwal GB, Hamblin MR. Cell death pathways in photodynamic therapy of cancer. Cancers (Basel). 2011;3(2):2516–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Broekgaarden M, Weijer R, van Gulik TM, Hamblin MR, Heger M. Tumor cell survival pathways activated by photodynamic therapy: a molecular basis for pharmacological inhibition strategies. Cancer Metastasis Rev. 2015;34(4):643–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Martins WK, Belotto R, Silva MN, Grasso D, Suriani MD, Lavor TS, et al. Autophagy regulation and photodynamic therapy: insights to improve outcomes of Cancer Treatment. Front Oncol. 2020;10:610472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kessel D, Luo Y. Photodynamic therapy: a mitochondrial inducer of apoptosis. Cell Death Differ. 1999;6(1):28–35. [DOI] [PubMed] [Google Scholar]
- 46.Granville DJ, Carthy CM, Jiang H, Shore GC, McManus BM, Hunt DWC. Rapid cytochrome c release, activation of caspases 3, 6, 7 and 8 followed by Bap31 cleavage in HeLa cells treated with photodynamic therapy. FEBS Lett. 1998;437(1):5–10. [DOI] [PubMed] [Google Scholar]
- 47.Yoon HE, Ahn MY, Kim YC, Yoon JH. Involvement of endoplasmic reticulum stress and cell death by synthesized Pa-PDT in oral squamous cell carcinoma cells. J Dent Sci. 2022;17(4):1722–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dudzik T, Domański I, Makuch S. The impact of photodynamic therapy on immune system in cancer - an update. Front Immunol. 2024;15:1335920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Tan L, Shen X, He Z, Lu Y. The role of photodynamic therapy in triggering cell death and facilitating Antitumor Immunology. Front Oncol. 2022;12. [DOI] [PMC free article] [PubMed]
- 50.Kareliotis G, Liossi S, Makropoulou M. Assessment of singlet oxygen dosimetry concepts in photodynamic therapy through computational modeling. Photodiagn Photodyn Ther. 2018;21:224–33. [DOI] [PubMed] [Google Scholar]
- 51.Kim MM, Darafsheh A. Light sources and Dosimetry techniques for photodynamic therapy. Photochem Photobiol. 2020;96(2):280–94. [DOI] [PubMed] [Google Scholar]
- 52.Van der Veen N, De Bruijn HS, Star WM. Photobleaching during and re-appearance after photodynamic therapy of topical ALA-induced fluorescence in UVB-treated mouse skin. Int J Cancer. 1997;72(1):110–8. [DOI] [PubMed] [Google Scholar]
- 53.Foster TH, Gao L. Dosimetry in Photodynamic Therapy: Oxygen and the critical importance of Capillary density. Radiat Res. 1992;130(3):379–83. [DOI] [PubMed] [Google Scholar]
- 54.Grossweiner LI. PDT light dosimetry revisited. J Photochem Photobiol B. 1997;38(2):258–68. [DOI] [PubMed] [Google Scholar]
- 55.Sterenborg H, Veen R, Aans J-B, Amelink A, Robinson D. Light Dosimetry for Photodynamic Therapy: Basic concepts. 2013. pp. 281 – 91.
- 56.Krishnamurthy S, Powers SK, Witmer P, Brown T. Optimal light dose for interstitial photodynamic therapy in treatment for malignant brain tumors. Lasers Surg Med. 2000;27(3):224–34. [DOI] [PubMed] [Google Scholar]
- 57.Schaberle FA. Assessment of the actual light dose in photodynamic therapy. Photodiagnosis Photodyn Ther. 2018;23:75–7. [DOI] [PubMed] [Google Scholar]
- 58.Al-Hinai AS, Al-Abri MS. Half-fluence photodynamic therapy to treat chronic central serous chorioretinopathy: a case series. Oman J Ophthalmol. 2011;4(2):63–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Grossman CE, Carter SL, Czupryna J, Wang L, Putt ME, Busch TM. Fluence Rate differences in Photodynamic Therapy Efficacy and Activation of Epidermal Growth Factor Receptor after treatment of the Tumor-involved murine thoracic cavity. Int J Mol Sci 2016;17(1). [DOI] [PMC free article] [PubMed]
- 60.Lui H. Photodynamic therapy in dermatology with porfimer sodium and benzoporphyrin derivative: an update. Semin Oncol. 1994;21(6 Suppl 15):11–4. [PubMed] [Google Scholar]
- 61.Tsukagoshi S. [Porfimer sodium (Photofrin-II)]. Gan Kagaku Ryoho. 1995;22(9):1271–8. [PubMed] [Google Scholar]
- 62.Lang K, Schulte K, Ruzicka T, Fritsch C. Aminolevulinic acid (Levulan) in photodynamic therapy of actinic keratoses. Skin Ther Lett. 2001;6:1–2. [PubMed] [Google Scholar]
- 63.Champeau M, Vignoud S, Mortier L, Mordon S. Photodynamic therapy for skin cancer: how to enhance drug penetration? J Photochem Photobiol B. 2019;197:111544. [DOI] [PubMed] [Google Scholar]
- 64.Tan IB, Dolivet G, Ceruse P, Vander Poorten V, Roest G, Rauschning W. Temoporfin-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: a multicenter study. Head Neck. 2010;32(12):1597–604. [DOI] [PubMed] [Google Scholar]
- 65.Senge MO, Brandt JC. Temoporfin (Foscan®, 5,10,15,20-Tetra(m-hydroxyphenyl)chlorin)—A second-generation Photosensitizer†‡. Photochem Photobiol. 2011;87(6):1240–96. [DOI] [PubMed] [Google Scholar]
- 66.Morton CA. Methyl aminolevulinate (Metvix) photodynamic therapy - practical pearls. J Dermatolog Treat. 2003;14(Suppl 3):23–6. [DOI] [PubMed]
- 67.Foley P. Clinical efficacy of methyl aminolevulinate (Metvix) photodynamic therapy. J Dermatolog Treat. 2003;14(Suppl 3):15–22. [DOI] [PubMed] [Google Scholar]
- 68.Di Stasi SM, De Carlo F, Pagliarulo V, Masedu F, Verri C, Celestino F, Riedl C. Hexaminolevulinate hydrochloride in the detection of nonmuscle invasive cancer of the bladder. Ther Adv Urol. 2015;7(6):339–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Traylor JI, Pernik MN, Sternisha AC, McBrayer SK, Abdullah KG. Molecular and metabolic mechanisms underlying selective 5-Aminolevulinic Acid-Induced fluorescence in Gliomas. Cancers (Basel). 2021;13(3). [DOI] [PMC free article] [PubMed]
- 70.Howley R, Chandratre S, Chen B. 5-Aminolevulinic acid as a Theranostic Agent for Tumor fluorescence imaging and photodynamic therapy. Bioeng (Basel). 2023;10(4). [DOI] [PMC free article] [PubMed]
- 71.Zhang R, Gao T, Wang D. Photodynamic therapy (PDT) for oral leukoplakia: a systematic review and meta-analysis of single-arm studies examining efficacy and subgroup analyses. BMC Oral Health. 2023;23(1):568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Hu Y, Wang Y, Li Y, Zeng X, Li J, Zhou Y, Chen Q. Retinoid treatment for oral leukoplakia: current evidence and Future Development. J Clin Pharm Ther. 2024;2024:6616979. [Google Scholar]
- 73.Kübler A, Haase T, Rheinwald M, Barth T, Mühling J. Treatment of oral leukoplakia by topical application of 5-aminolevulinic acid. Int J Oral Maxillofac Surg. 1998;27(6):466–9. [DOI] [PubMed] [Google Scholar]
- 74.Sieroń A, Adamek M, Kawczyk-Krupka A, Mazur S, Ilewicz L. Photodynamic therapy (PDT) using topically applied δ‐aminolevulinic acid (ALA) for the treatment of oral leukoplakia. J oral Pathol Med. 2003;32(6):330–6. [DOI] [PubMed] [Google Scholar]
- 75.Chen HM, Yu CH, Tu PC, Yeh CY, Tsai T, Chiang CP. Successful treatment of oral verrucous hyperplasia and oral leukoplakia with topical 5-aminolevulinic acid‐mediated photodynamic therapy. Lasers Surg Medicine: Official J Am Soc Laser Med Surg. 2005;37(2):114–22. [DOI] [PubMed] [Google Scholar]
- 76.Siddiqui SA, Siddiqui S, Hussain MB, Khan S, Liu H, Akhtar K, et al. Clinical evaluation of a mobile, low-cost system for fluorescence guided photodynamic therapy of early oral cancer in India. Photodiagn Photodyn Ther. 2022;38:102843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Yao YL, Wang YF, Li CX, Wu L, Tang GY. Management of oral leukoplakia by ablative fractional laser-assisted photodynamic therapy: a 3‐year retrospective study of 48 patients. Lasers Surg Med. 2022;54(5):682–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Boorghani M, Gholizadeh N, Taghavi Zenouz A, Vatankhah M, Mehdipour M. Oral lichen planus: clinical features, etiology, treatment and management; a review of literature. J Dent Res Dent Clin Dent Prospects. 2010;4(1):3–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Elenbaas A, Enciso R, Al-Eryani K. Oral Lichen Planus: a review of clinical features, etiologies, and treatments. Dentistry Rev. 2022;2(1):100007. [Google Scholar]
- 80.Silman I, Roth E, Paz A, Triquigneaux MM, Ehrenshaft M, Xu Y, et al. The specific interaction of the photosensitizer methylene blue with acetylcholinesterase provides a model system for studying the molecular consequences of photodynamic therapy. Chem Biol Interact. 2013;203(1):63–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.da Veiga Moreira J, Nleme N, Schwartz L, Leclerc-Desaulniers K, Carmona E, Mes-Masson A-M, Jolicoeur M. Methylene Blue metabolic therapy restrains. In Vivo Ovarian Tumor Growth Cancers [Internet]. 2024; 16(2). [DOI] [PMC free article] [PubMed]
- 82.Taldaev A, Terekhov R, Nikitin I, Melnik E, Kuzina V, Klochko M et al. Methylene blue in anticancer photodynamic therapy: systematic review of preclinical studies. Front Pharmacol. 2023;14. [DOI] [PMC free article] [PubMed]
- 83.Tardivo JP, Del Giglio A, De Oliveira CS, Gabrielli DS, Junqueira HC, Tada DB, et al. Methylene blue in photodynamic therapy: from basic mechanisms to clinical applications. Photodiagn Photodyn Ther. 2005;2(3):175–91. [DOI] [PubMed] [Google Scholar]
- 84.Aghahosseini F, Arbabi-Kalati F, Fashtami LA, Djavid GE, Fateh M, Beitollahi JM. Methylene blue‐mediated photodynamic therapy: a possible alternative treatment for oral lichen planus. Lasers Surg Medicine: Official J Am Soc Laser Med Surg. 2006;38(1):33–8. [DOI] [PubMed] [Google Scholar]
- 85.Sadaksharam J, Nayaki KT, Panneer Selvam N. Treatment of oral lichen planus with methylene blue mediated photodynamic therapy–a clinical study. PhotoDermatol PhotoImmunol PhotoMed. 2012;28(2):97–101. [DOI] [PubMed] [Google Scholar]
- 86.Bakhtiari S, Azari-Marhabi S, Mojahedi SM, Namdari M, Rankohi ZE, Jafari S. Comparing clinical effects of photodynamic therapy as a novel method with topical corticosteroid for treatment of oral Lichen Planus. Photodiagn Photodyn Ther. 2017;20:159–64. [DOI] [PubMed] [Google Scholar]
- 87.Mostafa D, Moussa E, Alnouaem M. Evaluation of photodynamic therapy in treatment of oral erosive lichen planus in comparison with topically applied corticosteroids. Photodiagn Photodyn Ther. 2017;19:56–66. [DOI] [PubMed] [Google Scholar]
- 88.Sun H, Yang W, Ong Y, Busch TM, Zhu TC. Fractionated photofrin-mediated photodynamic therapy significantly improves long-term survival. Cancers (Basel). 2023;15(23). [DOI] [PMC free article] [PubMed]
- 89.Mehraban N, Freeman H. Developments in PDT sensitizers for increased selectivity and Singlet Oxygen production. Materials. 2015;8:4421–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Biel MA. Photodynamic therapy in head and neck cancer. Curr Oncol Rep. 2002;4(1):87–96. [DOI] [PubMed] [Google Scholar]
- 91.Biel MA. Photodynamic therapy and the treatment of head and neck cancers. J Clin Laser Med Surg. 1996;14(5):239–44. [DOI] [PubMed] [Google Scholar]
- 92.Biel MA. Photodynamic therapy as an adjuvant intraoperative treatment of recurrent head and neck carcinomas. Archives Otolaryngology–Head Neck Surg. 1996;122(11):1261–5. [DOI] [PubMed] [Google Scholar]
- 93.Biel M. Advances in photodynamic therapy for the treatment of head and neck cancers. Lasers Surg Medicine: Official J Am Soc Laser Med Surg. 2006;38(5):349–55. [DOI] [PubMed] [Google Scholar]
- 94.Ikeda H, Tobita T, Ohba S, Uehara M, Asahina I. Treatment outcome of photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagn Photodyn Ther. 2013;10(3):229–35. [DOI] [PubMed] [Google Scholar]
- 95.Hopper C, Kübler A, Lewis H, Tan IB, Putnam G, Group FS. mTHPC-mediated photodynamic therapy for early oral squamous cell carcinoma. Int J Cancer. 2004;111(1):138–46. [DOI] [PubMed] [Google Scholar]
- 96.D’Cruz AK, Robinson MH, Biel MA. mTHPC-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: a multicenter study of 128 patients. Head Neck: J Sci Specialties Head Neck. 2004;26(3):232–40. [DOI] [PubMed] [Google Scholar]
- 97.Kübler A, De Carpentier J, Hopper C, Leonard A, Putnam G. Treatment of squamous cell carcinoma of the lip using foscan-mediated photodynamic therapy. Int J Oral Maxillofac Surg. 2001;30(6):504–9. [DOI] [PubMed] [Google Scholar]
- 98.Kubler A. Cost-effectivity analysis of photodynamic therapy with foscan (R)(Foscan (R)-PDT) compared with a palliative chemotherapy in patients with advanced head and neck tumors in Germany. Laryngorhinootologie. 2005;84:725–32. [DOI] [PubMed] [Google Scholar]
- 99.Karakullukcu B, van Oudenaarde K, Copper MP, Klop W, van Veen R, Wildeman M, Bing Tan I. Photodynamic therapy of early stage oral cavity and oropharynx neoplasms: an outcome analysis of 170 patients. Eur Arch Otorhinolaryngol. 2011;268:281–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Copper MP, Tan IB, Oppelaar H, Ruevekamp MC, Stewart FA. Meta-tetra (hydroxyphenyl) chlorin photodynamic therapy in early-stage squamous cell carcinoma of the head and neck. Archives Otolaryngology–Head Neck Surg. 2003;129(7):709–11. [DOI] [PubMed] [Google Scholar]
- 101.Jerjes W, Upile T, Radhi H, Hopper C. Photodynamic therapy and end-stage tongue base cancer. Head Neck Oncol. 2011;3:1–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Ma QL, Shen MO, Han N, Xu HZ, Peng XC, Li QR, et al. Chlorin e6 mediated photodynamic therapy triggers resistance through ATM-related DNA damage response in lung cancer cells. Photodiagnosis Photodyn Ther. 2022;37:102645. [DOI] [PubMed] [Google Scholar]
- 103.Hak A, Ali MS, Sankaranarayanan SA, Shinde VR, Rengan AK. Chlorin e6: a Promising Photosensitizer in Photo-Based Cancer Nanomedicine. ACS Appl Bio Mater. 2023;6(2):349–64. [DOI] [PubMed] [Google Scholar]
- 104.Shrestha R, Mallik SK, Lim J, Gurung P, Magar TBT, Kim YW. Efficient synthesis of Chlorin e6 and its potential photodynamic immunotherapy in mouse melanoma by the Abscopal Effect. Int J Mol Sci. 2023;24(4). [DOI] [PMC free article] [PubMed]
- 105.Kou J, Dou D, Yang L. Porphyrin photosensitizers in photodynamic therapy and its applications. Oncotarget. 2017;8(46):81591–603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Sine J, Urban C, Thayer D, Charron H, Valim N, Tata DB, et al. Photo activation of HPPH encapsulated in Pocket liposomes triggers multiple drug release and tumor cell killing in mouse breast cancer xenografts. Int J Nanomed. 2015;10:125–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Sobaniec S, Bernaczyk P, Pietruski J, Cholewa M, Skurska A, Dolińska E, et al. Clinical assessment of the efficacy of photodynamic therapy in the treatment of oral lichen planus. Lasers Med Sci. 2013;28:311–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Rigual N, Shafirstein G, Cooper MT, Baumann H, Bellnier DA, Sunar U, et al. Photodynamic therapy with 3-(1′-hexyloxyethyl) pyropheophorbide a for cancer of the oral cavity. Clin Cancer Res. 2013;19(23):6605–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Koczorowski T, Szczolko W, Teubert A, Goslinski T. Sulfanyl Porphyrazines with Morpholinylethyl Periphery-Synthesis, Electrochemistry, and Photocatalytic studies after Deposition on Titanium(IV) oxide P25 nanoparticles. Molecules. 2021;26(8). [DOI] [PMC free article] [PubMed]
- 110.Mlynarczyk DT, Dlugaszewska J, Falkowski M, Popenda L, Kryjewski M, Szczolko W, et al. Tribenzoporphyrazines with dendrimeric peripheral substituents and their promising photocytotoxic activity against Staphylococcus aureus. J Photochem Photobiol B. 2020;204:111803. [DOI] [PubMed] [Google Scholar]
- 111.Wang X, Hu J, Wang P, Zhang S, Liu Y, Xiong W, Liu Q. Analysis of the in vivo and in vitro effects of photodynamic therapy on breast cancer by using a sensitizer, sinoporphyrin sodium. Theranostics. 2015;5(7):772–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Kim J, Kim J, Yoon H, Chae YJ, Rhew K, Chang JE. The in vitro and in vivo Anticancer Effect of Photomed for photodynamic therapy: comparison with photofrin and Radachlorin. Curr Issues Mol Biol. 2023;45(3):2474–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Piskorz J, Skupin P, Lijewski S, Korpusinski M, Sciepura M, Konopka K, et al. Synthesis, physical–chemical properties and in vitro photodynamic activity against oral cancer cells of novel porphyrazines possessing fluoroalkylthio and dietherthio substituents. J Fluorine Chem. 2012;135:265–71. [Google Scholar]
- 114.Piskorz J, Konopka K, Düzgüneş N, Gdaniec Z, Mielcarek J, Goslinski T. Diazepinoporphyrazines containing peripheral styryl substituents and their promising nanomolar photodynamic activity against oral cancer cells in liposomal formulations. ChemMedChem. 2014;9(8):1775–82. [DOI] [PubMed] [Google Scholar]
- 115.Neves S, Faneca H, Bertin S, Konopka K, Düzgüneş N, Pierrefite-Carle V, et al. Transferrin lipoplex-mediated suicide gene therapy of oral squamous cell carcinoma in an immunocompetent murine model and mechanisms involved in the antitumoral response. Cancer Gene Ther. 2009;16(1):91–101. [DOI] [PubMed] [Google Scholar]
- 116.Liu J, Tian L, Zhang R, Dong Z, Wang H, Liu Z. Collagenase-encapsulated pH-responsive nanoscale coordination polymers for tumor microenvironment modulation and enhanced photodynamic nanomedicine. ACS Appl Mater Interfaces. 2018;10(50):43493–502. [DOI] [PubMed] [Google Scholar]
- 117.Kohli AG, Kivimäe S, Tiffany MR, Szoka FC. Improving the distribution of Doxil® in the tumor matrix by depletion of tumor hyaluronan. J Controlled Release. 2014;191:105–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Pandey M, Choudhury H, Ying JNS, Ling JFS, Ting J, Ting JSS, et al. Mucoadhesive nanocarriers as a promising strategy to enhance intracellular delivery against oral cavity carcinoma. Pharmaceutics. 2022;14(4):795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Alaei S, Omidian H. Mucoadhesion and mechanical assessment of oral films. Eur J Pharm Sci. 2021;159:105727. [DOI] [PubMed] [Google Scholar]
- 120.Piskorz J, Lijewski S, Gierszewski M, Gorniak K, Sobotta L, Wicher B, et al. Sulfanyl porphyrazines: molecular barrel-like self-assembly in crystals, optical properties and in vitro photodynamic activity towards cancer cells. Dyes Pigm. 2017;136:898–908. [Google Scholar]
- 121.Skupin-Mrugalska P, Koczorowski T, Szczolko W, Dlugaszewska J, Teubert A, Piotrowska-Kempisty H, et al. Cationic porphyrazines with morpholinoethyl substituents–Syntheses, optical properties, and photocytotoxicities. Dyes Pigm. 2022;197:109937. [Google Scholar]
- 122.Mlynarczyk DT, Lijewski S, Falkowski M, Piskorz J, Szczolko W, Sobotta L, et al. Dendrimeric sulfanyl porphyrazines: synthesis, physico-chemical characterization, and biological activity for potential applications in photodynamic therapy. ChemPlusChem. 2016;81(5):460–70. [DOI] [PubMed] [Google Scholar]
- 123.Young J, Yee M, Kim H, Cheung J, Chino T, Düzgüneş N, Konopka K. Phototoxicity of liposomal Zn-and Al-phthalocyanine against cervical and oral squamous cell carcinoma cells in vitro. Med Sci Monit Basic Res. 2016;22:156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Young J, Yee M, Kim H, Cheung J, Chino T, Düzgüneş N, Konopka K. Phototoxicity of liposomal Zn- and Al-phthalocyanine against cervical and oral squamous cell carcinoma cells in Vitro. Med Sci Monit Basic Res. 2016;22:156–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Thomas AP, Saneesh Babu PS, Asha Nair S, Ramakrishnan S, Ramaiah D, Chandrashekar TK, et al. Meso-tetrakis(p-sulfonatophenyl)N-confused porphyrin tetrasodium salt: a potential sensitizer for photodynamic therapy. J Med Chem. 2012;55(11):5110–20. [DOI] [PubMed] [Google Scholar]
- 126.Chin Y, Lim SH, Zorlu Y, Ahsen V, Kiew LV, Chung LY, et al. Improved photodynamic efficacy of zn (II) phthalocyanines via glycerol substitution. PLoS ONE. 2014;9(5):e97894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Park J-H, Moon Y-H, Kim D-J, Kim S-A, Lee J-B, Ahn S-G, Yoon J-H. Photodynamic therapy with hexenyl ester of 5-aminolevulinic acid induces necrotic cell death in salivary gland adenocarcinoma cells. Oncol Rep. 2010;24(1):177–81. [PubMed] [Google Scholar]
- 128.Wang B, Wang J-H, Liu Q, Huang H, Chen M, Li K, et al. Rose-bengal-conjugated gold nanorods for in vivo photodynamic and photothermal oral cancer therapies. Biomaterials. 2014;35(6):1954–66. [DOI] [PubMed] [Google Scholar]
- 129.Kim S-A, Lee MR, Yoon J-H, Ahn S-G. HOXC6 regulates the antitumor effects of pheophorbide a-based photodynamic therapy in multidrug-resistant oral cancer cells. Int J Oncol. 2016;49(6):2421–30. [DOI] [PubMed] [Google Scholar]
- 130.Lee M-J, Hung S-H, Huang M-C, Tsai T, Chen C-T. Doxycycline potentiates antitumor effect of 5-aminolevulinic acid-mediated photodynamic therapy in malignant peripheral nerve sheath tumor cells. PLoS ONE. 2017;12(5):e0178493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Kofler B, Romani A, Pritz C, Steinbichler TB, Schartinger VH, Riechelmann H, Dudas J. Photodynamic effect of methylene blue and low level laser radiation in head and neck squamous cell carcinoma cell lines. Int J Mol Sci. 2018;19(4):1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Zhu M, Shi S, Wan G, Wang Y, Wang Y, Zhang L, Zhao Y. In vitro and in vivo effects of 5-aminolevulinic acid-mediated photodynamic therapy against oral squamous cell carcinoma. Zhonghua Kou Qiang Yi Xue Za Zhi = Zhonghua Kouqiang Yixue Zazhi = Chinese. J Stomatology. 2019;54(3):176–82. [DOI] [PubMed] [Google Scholar]
- 133.Qi F, Sun Y, Lv M, Qin F, Cao W, Bi L. Effects of palmatine hydrochloride mediated photodynamic therapy on oral squamous cell carcinoma. Photochem Photobiol Sci. 2019;18:1596–605. [DOI] [PubMed] [Google Scholar]
- 134.Shi S, Zhang L, Zhu M, Wan G, Li C, Zhang J, et al. Reactive oxygen species-responsive nanoparticles based on PEGlated Prodrug for targeted treatment of oral Tongue squamous cell carcinoma by combining photodynamic therapy and chemotherapy. ACS Appl Mater Interfaces. 2018;10(35):29260–72. [DOI] [PubMed] [Google Scholar]
- 135.Wang X, Jin J, Li W, Wang Q, Han Y, Liu H. Differential in vitro sensitivity of oral precancerous and squamous cell carcinoma cell lines to 5-aminolevulinic acid-mediated photodynamic therapy. Photodiagnosis Photodyn Ther. 2020;29:101554. [DOI] [PubMed] [Google Scholar]
- 136.Ma Y, Qu S, Xu L, Lu H, Li B. An in vitro study of the effect of 5-ALA-mediated photodynamic therapy on oral squamous cell carcinoma. BMC Oral Health. 2020;20(1):258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Wei Z, Zou H, Liu G, Song C, Tang C, Chen S, et al. Peroxidase-mimicking evodiamine/indocyanine green nanoliposomes for multimodal imaging-guided theranostics for oral squamous cell carcinoma. Bioact Mater. 2021;6(7):2144–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Zhang X, Li H, Yi C, Chen G, Li Y, Zhou Y, et al. Host Immune Response triggered by Graphene Quantum-dot-mediated photodynamic therapy for oral squamous cell carcinoma. Int J Nanomed. 2020;15:9627–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Algorri JF, López-Higuera JM, Rodríguez-Cobo L, Cobo A. Advanced Light Source Technologies for photodynamic therapy of skin Cancer lesions. Pharm [Internet]. 2023; 15(8). [DOI] [PMC free article] [PubMed]
- 140.Algorri JF, Ochoa M, Roldán-Varona P, Rodríguez-Cobo L, López-Higuera JM. Light technology for efficient and effective photodynamic therapy: a critical review. Cancers (Basel). 2021;13(14). [DOI] [PMC free article] [PubMed]
- 141.Brancaleon L, Moseley H. Laser and non-laser light sources for photodynamic therapy. Lasers Med Sci. 2002;17:173–86. [DOI] [PubMed] [Google Scholar]
- 142.Piksa M, Lian C, Samuel IC, Pawlik KJ, Samuel ID, Matczyszyn K. The role of the light source in antimicrobial photodynamic therapy. Chem Soc Rev. 2023;52(5):1697–722. [DOI] [PubMed] [Google Scholar]
- 143.Zou J, Li W, Meng N, Jiang J, Wu C, Lei TC, et al. Evaluation of lensed fibers used in photodynamic therapy (PDT). Photodiagn Photodyn Ther. 2020;31:101924. [DOI] [PubMed] [Google Scholar]
- 144.Wilson BC. Photodynamic therapy: light delivery and dosage for second-generation photosensitizers. Ciba Found Symp. 1989;146:60–73. discussion – 7. [DOI] [PubMed]
- 145.Huang A, Nguyen JK, Jagdeo J. Light-emitting diode-based photodynamic therapy for photoaging, scars, and Dyspigmentation: a systematic review. Dermatol Surg. 2020;46(11):1388–94. [DOI] [PubMed] [Google Scholar]
- 146.Sorbellini E, Rucco M, Rinaldi F. Photodynamic and photobiological effects of light-emitting diode (LED) therapy in dermatological disease: an update. Lasers Med Sci. 2018;33(7):1431–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Shi X, Yin H, Dong X, Li H, Li Y. Photodynamic therapy with light-emitting diode arrays producing different light fields induces apoptosis and necrosis in gastrointestinal cancer. Front Oncol. 2022;12. [DOI] [PMC free article] [PubMed]
- 148.Barolet D. Light-Emitting Diodes (LEDs) in Dermatology. Seminars in cutaneous medicine and surgery. 2009;27:227 – 38. [DOI] [PubMed]
- 149.Huang Z. A review of progress in clinical photodynamic therapy. Technol Cancer Res Treat. 2005;4(3):283–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Vander Poorten V, Meulemans J, Nuyts S, Clement P, Hermans R, Hauben E, Delaere P. Postoperative photodynamic therapy as a new adjuvant treatment after robot-assisted salvage surgery of recurrent squamous cell carcinoma of the base of tongue. World J Surg Oncol. 2015;13:1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Ahn PH, Quon H, O’Malley BW, Weinstein G, Chalian A, Malloy K, et al. Toxicities and early outcomes in a phase 1 trial of photodynamic therapy for premalignant and early stage head and neck tumors. Oral Oncol. 2016;55:37–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Toratani S, Tani R, Kanda T, Koizumi K, Yoshioka Y, Okamoto T. Photodynamic therapy using photofrin and excimer dye laser treatment for superficial oral squamous cell carcinomas with long-term follow up. Photodiagn Photodyn Ther. 2016;14:104–10. [DOI] [PubMed] [Google Scholar]
- 153.van Doeveren TE, Karakullukçu MB, van Veen RL, Lopez-Yurda M, Schreuder WH, Tan IB. Adjuvant photodynamic therapy in head and neck cancer after tumor‐positive resection margins. Laryngoscope. 2018;128(3):657–63. [DOI] [PubMed] [Google Scholar]
- 154.Jerjes W, Upile T, Hamdoon Z, Alexander Mosse C, Morcos M, Hopper C. Photodynamic therapy outcome for T1/T2 N0 oral squamous cell carcinoma. Lasers Surg Med. 2011;43(6):463–9. [DOI] [PubMed] [Google Scholar]
- 155.Wang X, Li N, Meng J, Wen N. The use of topical ALA-photodynamic therapy combined with induction chemotherapy for locally advanced oral squamous cell carcinoma. Am J Otolaryngol. 2021;42(6):103112. [DOI] [PubMed] [Google Scholar]
- 156.Santos LL, Oliveira J, Monteiro E, Santos J, Sarmento C. Treatment of head and neck cancer with photodynamic therapy with redaporfin: a clinical case report. Case Rep Oncol. 2018;11(3):769–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Jerjes W, Upile T, Hamdoon Z, Abbas S, Akram S, Mosse CA, et al. Photodynamic therapy: the minimally invasive surgical intervention for advanced and/or recurrent tongue base carcinoma. Lasers Surg Med. 2011;43(4):283–92. [DOI] [PubMed] [Google Scholar]
- 158.Shafirstein G, Rigual NR, Arshad H, Cooper MT, Bellnier DA, Wilding G, et al. Photodynamic therapy with 3-(1′‐hexyloxyethyl) pyropheophorbide‐a for early‐stage cancer of the larynx: phase ib study. Head Neck. 2016;38(S1):E377–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Ikeda H, Ohba S, Egashira K, Asahina I. The effect of photodynamic therapy with talaporfin sodium, a second-generation photosensitizer, on oral squamous cell carcinoma: a series of eight cases. Photodiagn Photodyn Ther. 2018;21:176–80. [DOI] [PubMed] [Google Scholar]
- 160.Karakullukcu B, Stoker SD, Wildeman AP, Copper MP, Wildeman MA, Tan IB. A matched cohort comparison of mTHPC-mediated photodynamic therapy and trans-oral surgery of early stage oral cavity squamous cell cancer. Eur Arch Otorhinolaryngol. 2013;270:1093–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.de Visscher SA, Melchers LJ, Dijkstra PU, Karakullukcu B, Tan IB, Hopper C, et al. mTHPC-mediated photodynamic therapy of early stage oral squamous cell carcinoma: a comparison to surgical treatment. Ann Surg Oncol. 2013;20:3076–82. [DOI] [PubMed] [Google Scholar]
- 162.Lambert A, Nees L, Nuyts S, Clement P, Meulemans J, Delaere P, Vander Poorten V. Photodynamic therapy as an alternative therapeutic tool in functionally inoperable oral and oropharyngeal carcinoma: a single tertiary center retrospective cohort analysis. Front Oncol. 2021;11:626394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Karakullukcu B, Nyst HJ, van Veen RL, Hoebers FJ, Hamming–Vrieze O, Witjes MJ, et al. mTHPC mediated interstitial photodynamic therapy of recurrent nonmetastatic base of tongue cancers: development of a new method. Head Neck. 2012;34(11):1597–606. [DOI] [PubMed] [Google Scholar]
- 164.Caesar L, van Doeveren T, Tan I, Dilci A, van Veen R, Karakullukcu B. The use of photodynamic therapy as adjuvant therapy to surgery in recurrent malignant tumors of the paranasal sinuses. Photodiagn Photodyn Ther. 2015;12(3):414–21. [DOI] [PubMed] [Google Scholar]
- 165.Succo G, Rosso S, Fadda G, Fantini M, Crosetti E. Salvage photodynamic therapy for recurrent nasopharyngeal carcinoma. Photodiagn Photodyn Ther. 2014;11(2):63–70. [DOI] [PubMed] [Google Scholar]
- 166.von Beckerath MP, Reizenstein JA, Berner AL, Nordqvist KW, Landström FJ, Löfgren AL, Möller CG. Outcome of primary treatment of early laryngeal malignancies using photodynamic therapy. Acta Otolaryngol. 2014;134(8):852–8. [DOI] [PubMed] [Google Scholar]
- 167.Abbas S, Jerjes W, Upile T, Vaz F, Hopper C. The palliative role of PDT in recurrent advanced nasopharyngeal carcinoma: Case series. Photodiagn Photodyn Ther. 2012;9(2):142–7. [DOI] [PubMed] [Google Scholar]
- 168.Nyst HJ, Wildeman MA, Indrasari SR, Karakullukcu B, van Veen RLP, Adham M, et al. Temoporfin mediated photodynamic therapy in patients with local persistent and recurrent nasopharyngeal carcinoma after curative radiotherapy: a feasibility study. Photodiagn Photodyn Ther. 2012;9(3):274–81. [DOI] [PubMed] [Google Scholar]
- 169.Stoker SD, Indrasari SR, Herdini C, Hariwiyanto B, Karakullukcu B, Dhamiyati W, et al. Photodynamic therapy as salvage therapy for patients with nasopharyngeal carcinoma experiencing local failures following definitive radiotherapy. Photodiagn Photodyn Ther. 2015;12(3):519–25. [DOI] [PubMed] [Google Scholar]
- 170.Schweitzer VG, Somers ML. PHOTOFRIN-mediated photodynamic therapy for treatment of early stage (Tis-T2N0M0) SqCCa of oral cavity and oropharynx. Lasers Surg Med. 2010;42(1):1–8. [DOI] [PubMed] [Google Scholar]
- 171.Hosokawa S, Takebayashi S, Takahashi G, Okamura J, Mineta H. Photodynamic therapy in patients with head and neck squamous cell carcinoma. Lasers Surg Med. 2018;50(5):420–6. [DOI] [PubMed] [Google Scholar]
- 172.Rigual NR, Shafirstein G, Frustino J, Seshadri M, Cooper M, Wilding G, et al. Adjuvant intraoperative photodynamic therapy in head and neck cancer. JAMA Otolaryngol Head Neck Surg. 2013;139(7):706–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 173.Durbec M, Cosmidis A, Fuchsmann C, Ramade A, Céruse P. Efficacy and safety of photodynamic therapy with temoporfin in curative treatment of recurrent carcinoma of the oral cavity and oropharynx. Eur Arch Otorhinolaryngol. 2013;270(4):1433–9. [DOI] [PubMed] [Google Scholar]
- 174.Rivera C, Venegas B. Histological and molecular aspects of oral squamous cell carcinoma (review). Oncol Lett. 2014;8(1):7–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175.Panigrahi S, Nanda BS, Bhuyan R, Kumar K, Ghosh S, Swarnkar T. Classifying histopathological images of oral squamous cell carcinoma using deep transfer learning. Heliyon. 2023;9(3):e13444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176.Pathak J, Swain N, Patel S, Poonja L. Histopathological variants of oral squamous cell carcinoma-institutional case reports. J Oral Maxillofac Pathol. 2014;18(1):143–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Ikeda H, Tobita T, Ohba S, Uehara M, Asahina I. Treatment outcome of photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagnosis Photodyn Ther. 2013;10(3):229–35. [DOI] [PubMed] [Google Scholar]
- 178.Karakullukcu B, Stoker SD, Wildeman AP, Copper MP, Wildeman MA, Tan IB. A matched cohort comparison of mTHPC-mediated photodynamic therapy and trans-oral surgery of early stage oral cavity squamous cell cancer. Eur Arch Otorhinolaryngol. 2013;270(3):1093–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.de Visscher SA, Melchers LJ, Dijkstra PU, Karakullukcu B, Tan IB, Hopper C, et al. mTHPC-mediated photodynamic therapy of early stage oral squamous cell carcinoma: a comparison to surgical treatment. Ann Surg Oncol. 2013;20(9):3076–82. [DOI] [PubMed] [Google Scholar]
- 180.Vander Poorten V, Meulemans J, Nuyts S, Clement P, Hermans R, Hauben E, Delaere P. Postoperative photodynamic therapy as a new adjuvant treatment after robot-assisted salvage surgery of recurrent squamous cell carcinoma of the base of tongue. World J Surg Oncol. 2015;13:214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 181.Karakullukcu B, Nyst HJ, van Veen RL, Hoebers FJP, Hamming–Vrieze O, Witjes MJH, et al. mTHPC mediated interstitial photodynamic therapy of recurrent nonmetastatic base of tongue cancers: development of a new method. Head Neck. 2012;34(11):1597–606. [DOI] [PubMed] [Google Scholar]
- 182.van Doeveren TEM, Karakullukçu MB, van Veen RLP, Lopez-Yurda M, Schreuder WH, Tan IB. Adjuvant photodynamic therapy in head and neck cancer after tumor-positive resection margins. Laryngoscope. 2018;128(3):657–63. [DOI] [PubMed] [Google Scholar]
- 183.Rigual N, Shafirstein G, Cooper MT, Baumann H, Bellnier DA, Sunar U, et al. Photodynamic therapy with 3-(1’-hexyloxyethyl) pyropheophorbide a for cancer of the oral cavity. Clin Cancer Res. 2013;19(23):6605–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Caesar L, van Doeveren TEM, Tan IB, Dilci A, van Veen RLP, Karakullukcu B. The use of photodynamic therapy as adjuvant therapy to surgery in recurrent malignant tumors of the paranasal sinuses. Photodiagn Photodyn Ther. 2015;12(3):414–21. [DOI] [PubMed] [Google Scholar]
- 185.Skupin-Mrugalska P, Zalewski T, Elvang PA, Nowaczyk G, Czajkowski M, Piotrowska-Kempisty H. Insight into theranostic nanovesicles prepared by thin lipid hydration and microfluidic method. Colloids Surf B. 2021;205:111871. [DOI] [PubMed] [Google Scholar]
- 186.Wang D, Fei B, Halig LV, Qin X, Hu Z, Xu H, et al. Targeted iron-oxide nanoparticle for photodynamic therapy and imaging of head and neck cancer. ACS Nano. 2014;8(7):6620–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Liang J, Yang B, Zhou X, Han Q, Zou J, Cheng L. Stimuli-responsive drug delivery systems for head and neck cancer therapy. Drug Delivery. 2021;28(1):272–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.Song C, Ran J, Wei Z, Wang Y, Chen S, Lin L, et al. Organic near-infrared-II nanophotosensitizer for safe cancer phototheranostics and improving immune microenvironment against metastatic tumor. ACS Appl Mater Interfaces. 2021;13(3):3547–58. [DOI] [PubMed] [Google Scholar]
- 189.Wang Y, Xie D, Pan J, Xia C, Fan L, Pu Y, et al. A near infrared light-triggered human serum albumin drug delivery system with coordination bonding of indocyanine green and cisplatin for targeting photochemistry therapy against oral squamous cell cancer. Biomaterials Sci. 2019;7(12):5270–82. [DOI] [PubMed] [Google Scholar]
- 190.Ren S, Cheng X, Chen M, Liu C, Zhao P, Huang W, et al. Hypotoxic and rapidly metabolic PEG-PCL-C3-ICG nanoparticles for fluorescence-guided photothermal/photodynamic therapy against OSCC. ACS Appl Mater Interfaces. 2017;9(37):31509–18. [DOI] [PubMed] [Google Scholar]
- 191.Ma C, Shi L, Huang Y, Shen L, Peng H, Zhu X, Zhou G. Nanoparticle delivery of Wnt-1 siRNA enhances photodynamic therapy by inhibiting epithelial-mesenchymal transition for oral cancer. Biomater Sci. 2017;5(3):494–501. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No datasets were generated or analysed during the current study.