

Abstract
This preliminary study applied a computer-assisted quantitative linguistic analysis to examine the effectiveness of language-based classification models to discriminate between mothers (n = 140) with and without history of treatment for depression (51% and 49%, respectively). Mothers were recorded during a problem-solving interaction with their adolescent child. Transcripts were manually annotated and analyzed using a dictionary-based, natural-language program approach (Linguistic Inquiry and Word Count). To assess the importance of linguistic features to correctly classify history of depression, we used Support Vector Machines (SVM) with interpretable features. Using linguistic features identified in the empirical literature, an initial SVM achieved nearly 63% accuracy. A second SVM using only the top 5 highest ranked SHAP features improved accuracy to 67.15%. The findings extend the existing literature base on understanding language behavior of depressed mood states, with a focus on the linguistic style of mothers with and without a history of treatment for depression and its potential impact on child development and trans-generational transmission of depression.
Index Terms—: depression, language, dyads, mothers, LIWC, SVM
I. Introduction
Depression is one of the most common mental health problems with a lifespan risk of over 20% [1]. In the US, nearly 8% of the general adult population has experienced at least one major depressive episode, with a near 2-fold greater prevalence among adult women compared to men, and the highest prevalence among women at a child-bearing age (18–25 years) [2]
These data mean that an estimated 1 in 10 children are being cared for by a mother with depression [3]. The clinical features of major depression have the potential to adversely affect family interactional processes and relationships, and generate risk for depression in offspring [4]. Children with a depressed parent are three to four times more likely to develop depression than children of non-depressed parents [5]. Although genetic mechanisms represent one risk factor [6], [7], the exposure of children to negative parenting behaviors are an important adverse environmental factor underpinning intergenerational transmissions [8], [9]. Relative to that of mothers without depression, parenting style of mothers with depression is characterized by high levels of hostility, irritability, negative affect, intrusiveness, criticism, unpredictable behavior, withdrawal and unresponsiveness, and lower levels of maternal sensitivity, availability, and verbal and visual interaction [10]–[12]—all which have the potential to adversely impact child outcomes in cognitive, emotional, health, and social domains [3]. This effect is even more pronounced in mothers who experience adversity (e.g. poverty, separation or divorce, unemployment) and those from ethnic minority backgrounds [3]. As a consequence, children of parents affected by depression are at an increased risk of developing poorer physical health and well-being, difficult temperament, insecure attachment patterns, affective functioning difficulties and poorer internal functioning [5].
Observational research with a focus on parent-child face-to-face interaction has also found that parental expressions in interactions represent a pathway for the development of psychopathology and behavioral problems in adolescents, such as higher rates of depression, and higher rates of and more severe levels of internalizing and externalizing symptoms [13]. Despite the strengths of observational measures to explore risk trajectories for depression in young people, there is a dearth of literature that uses observational measures. This might be partly related to the expensive and time-consuming nature of observational studies compared to other methodological approaches—for example, previous empirical work on depression has emphasized experimental tasks related to the occurrence of depression using self-report measures in the clinical interview context (e.g. Hamilton Rating Scale for Depression, HRSD) [14].
This current preliminary study applied a computer-assisted quantitative linguistic analysis to the transcripts of recorded lab-based dyadic problem-solving interactions between mothers with and without a history of treatment for depression (Depressed and Non-Depressed) and their adolescent children. The Problem-Solving Interaction task (PSI) is designed to elicit negative affect [15], [16]. This study focused on mothers’ language use only, thus the utterances of the adolescent children and any dyadic features were excluded. To examine the effectiveness of a language-based classification model to discriminate between mothers in the depressed and non-depressed group, we used a machine learning approach (Support Vector Machine) and a dictionary-based natural language program approach (Linguistic Inquiry and Word Count [LIWC]) [17]. Although the applied methodology is not necessarily novel, this study is an important contribution to the clinical literature of affective disorders. We hypothesized that accurate discrimination between mothers in the depressed and non-depressed group would be possible with the combined set of the following linguistic variables: first-person singular pronouns, positive emotion words, negative emotions words (i.e. anxiety, anger, sadness), cognitive process words, and temporal words (i.e. past, present, future). Due to the interpersonal context of this study, we further hypothesized that second-person pronouns would contribute to a classification model as indicators of depression [18] and lower relationship quality (e.g. lower cohesion, higher conflict) by reflecting an interpersonal barrier rather than mother-child relational closeness [19] [20].
The main contributions of this study are three-fold:
We propose language-based classification models to discriminate between mothers in the depressed vs. non-depressed group.
We identify sets of most important linguistic features for history of treatment for depression.
To the best of our knowledge, this is the first study to analyze linguistic style in mother-child interactions of mothers with a history of treatment for depression.
II. Related Work
There is a long-standing history of assessing psychological states in individuals using automated language analysis. This work is based on the premise that language represents an observable and measurable behavior that can be studied in a systematic manner. It provides a data source to develop language-based models to make inferences and predict psychological states and behavior.
A growing number of studies have explored the relationship between negative schemas underlying depressive symptomatology and language behavior using computerized approaches to language analysis. Consistent with negative schemas underlying depressive symptoms and their impact on views of the self (i.e. feeling worthless or inadequate), the world (i.e. feeling nothing is worthwhile) and the future (i.e. nothing will ever change) [21], computer-assisted studies using language analysis have identified depression-specific word use in various contexts, including social media [22]–[29], literature [30], psychotherapy dialogues [31]–[34], and experimental writing and speech tasks [35], [36]. Based on the cognitive schemas underlying depression and existing empirical studies the following linguistic features have been associated with depressive symptoms: a greater use of self-references reflecting self-focused attention; negative emotion associated with negative thoughts about the past, present and future; and cognitive process words related to rumination, and a lower use of positive emotion words.
Linguistic studies of behavior using computerized approaches to language analysis with a focus on depression in mothers and their offspring are relatively rare. The majority of studies explored language behavior associated with positive affect. For example, Goodlett et al [37] examined maternal positivity emotion word use as an indicator of maternal positivity and potential buffer between maternal depressive symptoms and child internalizing problems in a vulnerable sample (i.e. low-income, ethnic minority families raising young children in an impoverished urban context). Based on positive emotion word use during an attachment script assessment, the results identified that mothers’ use of positive emotions words partially attenuated the link between maternal depressive symptoms and at-risk young children’s internalizing problems. This finding has implications about the association between maternal depression and child internalizing problems. With a focus on late childhood depressive symptoms, Moran et al [38] explored the links between mothers’ positive affect socialization and children’s affect regulation and depressive symptoms. They showed that mothers’ questioning responses to children’s positive affect during the discussant task related to children’s depressive symptoms, indicating that mothers’ questioning may be maladaptive.
III. Methodology
A. Data and Sample Characteristics
The data were collected as part of a larger study of parenting behavior in mothers of young adolescents [15] that included 180 mothers with a history of treatment of depression (Depressed) and without a history of treatment of depression (Not Depressed). Of these, 140 women aged 22.35 to 54.97 (mean age=40.25 years) and their adolescent children aged 10.3 to 15.9 (mean age=12.86 years) took part in a lab-based dyadic interaction task which is the focus of this study. The group of women did not differ significantly in age or diversity (i.e. race, ethnicity). Demographics of mothers are presented in Table I.
TABLE I:
Maternal demographic characteristics by group
| Depressed | Non-Depressed | |||||
|---|---|---|---|---|---|---|
| Variable | N | Mean | % | N | Mean | % |
| Age | 72 | 40.31 | 68 | 40.19 | ||
| Race | ||||||
| American Indian/ Alaska Native | 1 | 1.4 | 3 | 4.4 | ||
| Asian | 1 | 1.4 | 0 | 0 | ||
| Native Hawaiian/Pacific islander | 0 | 0 | 2 | 2.9 | ||
| White or Caucasian | 63 | 87.5 | 57 | 83.8 | ||
| Multiple Races | 7 | 9.7 | 4 | 5.9 | ||
| No response/ unknown | 0 | 0 | 2 | 2.9 | ||
| Ethnicity | ||||||
| Latino or Hispanic descent | 4 | 5.6 | 7 | 10.3 | ||
| Not Latino or Hispanic descent | 68 | 94.4 | 61 | 89.7 | ||
Seventy two mothers (51.4%) had a history of treatment for depression. They were aged 28.43 to 54.97 years (mean age 40.31). Sixty eight mothers (48.6%) were without a history of treatment for depression. They were aged 22.35 to 54.48 years (mean age=40.19). Screening of depressive symptoms was conducted using the Patient Health Questionnaire-8 (PHQ-8) [39]. Mothers in the depressed group were selected for current elevated depressive symptoms (PHQ-8 >/= 10) and a history of depression. Mothers in the non-depressed group demonstrated no more than mild current depressive symptomatology (PHQ-8 < 8), no history of treatment for depression, and no recent (i.e. past month) treatment for any mental health disorder. The women were of low income; meeting eligibility criteria for Medicaid. Exclusion criteria for mothers and adolescents included no current diagnosis of psychosis or other illness or cognitive impairment that would interfere with participation (e.g. substance use that would render abstinence for the assessment difficult to tolerate). In specific, for the purpose of this study we refer to mothers with a history of treatment for depression as ‘mother with a history of depression’, and mothers without a history of treatment for depression as ‘mothers without a history of depression’.
B. Recruitment
The majority of participants were recruited through the organization that administers the Oregon Health Plan (Medicaid) in the county where data were collected, and the remainder of participants were recruited through online advertisements. Mothers and adolescents were compensated for their participation.
C. Assessment Procedure
Family-interaction assessment: Mother-adolescent dyads completed a 15-minute lab-based Problem-Solving Interaction task (PSI) designed to elicit negative affect was video recorded for subsequent coding. For the PSI task, mother-adolescent dyads were asked to discuss and try to resolve an issue of conflict from the Issues Checklist [40]. Topics chosen for discussion were those with the highest mean frequency by intensity ratings across mother and adolescent reports. The PSI task has been shown to elicit negative affect [41]. The artificial lab-based context of the behavioral PSI task ensures standardized conditions and control to eliminate confounding extraneous variables.
D. Measures
1). Diagnostic Measure:
Mothers completed the Structured Clinical Interview, non-patient version (SCID-NP) [42] to characterize the sample and ensure that participants in the non-depressed group, did not meet criteria for current depressive disorder.
2). Self-Report Questionnaires:
Mothers completed the Patient Health Questionnaire-9 (PHQ-9) [43] which is a self-administered questionnaire to assess the presence and severity of depression. 30 out of 72 mothers reported their PHQ-9 scores within in one week of the task. The distribution of PHQ-9 in the depressed of group can be found in Table II. Because depression symptoms are a state rather than trait-dependent, we do not report severity for mothers who reported their PHQ-9 beyond one week about the PSI task.
TABLE II:
Distribution of current depression in the depressed group (N=72)
| Depression severity | PHQ-9 range | # mothers |
|---|---|---|
| None | 1 – 4 | 3 |
| Mild | 5 – 9 | 7 |
| Moderate | 10 – 14 | 12 |
| Moderate-severe | 15 – 19 | 5 |
| Severe | 20 – 17 | 3 |
| Not reported within 1 week | 42 |
3). Linguistic Measure:
To calculate the linguistic measures, the audio recordings collected during the PSI task were manually segmented and transcribed. We defined utterances as continuous spoken activity with less than 300ms of silence. Each utterance was characterized with a start and stop time. Filler words such as ”mhm”, ”uhh”, ”err” were also segmented and transcribed. The utterances were transcribed by native English speakers. Segmentations and transcriptions were reviewed to ensure accuracy. During the transcription process, the speaker of each utterance was identified along with the spoken content. In case of overlapping speech, both speakers were identified and content was transcribed. Subsequently, the English version of the LIWC [17] was administered to all transcripts. However this study focused on mothers’ language use only, thus the utterances of the adolescent children and any dyadic features were not included for further analysis. The LIWC is a dictionary-based natural language program that measures the frequency of words that have been pre-categorized into semantic and syntactic categories. The LIWC uses a word count method to measure the frequency of words categorized to psychological meaning categories with the aim to predict behavioral outcomes. The LIWC output refers to the percentages of each variable of total words within a text. The LIWC comprizes approximately 4,500 words and word stems that are categorized to 80 semantic categories and sub-categories. The semantic categories are organized with three overarching categories, including ‘Linguistic Processes’ (e.g. personal pronouns, articles, verbs), ‘Psychological Processes’ (e.g. social processes, affective processes, cognitive processes), and ‘Personal Concerns’ (e.g. work, leisure, death). The LIWC is hierarchically organized and, for example, all sadness words belong to the sub-category ‘negative emotions’ which forms part of ‘affect words’ category. Table III provides a list of example words that characterize the linguistic features, including main categories and sub-categories, relevant to this study. A series of non-parametric independent samples tests were computed to identify the linguistic variables that differ significantly between mothers in the depressed and non-depressed group at a liberal cut-off of p<.05 (Table III). The amount of text normalization performed was minimal. We removed words that were not discernible to the annotators and corrected any misspelling manually. Since the LIWC contains features related to punctuation, we preserved the punctuation. We did not perform stemming or lemmatization of words to preserve tense and parts-of-speech.
TABLE III:
Linguistics frequencies and their comparison between depressed and non-depressed groups of LIWC features. ns indicates p>.05
| Depressed Mothers | Non-Depressed Mothers | ||||
|---|---|---|---|---|---|
| Variable | Mean | SD | Mean | SD | p-value |
| Word count | 853.38 | 283.37 | 964.04 | 379.73 | ns |
| Personal pronouns | |||||
| First-person singular pronouns (e.g. I, me, mine) | 4.59 | 1.99 | 3.92 | 1.52 | .047 |
| Second-person pronouns (e.g. you, your, thou) | 7.72 | 1.86 | 7 | 2.24 | .044 |
| Affect | 5.48 | 1.39 | 5.42 | 1.92 | ns |
| Positive emotion (e.g. love, nice, sweet) | 3.81 | 1.17 | 4.1 | 1.67 | ns |
| Negative emotion (e.g. hurt, ugly, nasty) | 1.6 | 0.9 | 1.29 | 0.86 | .011 |
| Anger (e.g. hate, kill, annoyed) | 0.63 | 0.66 | 0.42 | 0.54 | .026 |
| Sadness (e.g. crying, grief, sad) | 0.25 | 0.27 | 0.21 | 0.18 | ns |
| Anxiety (e.g. worried, fearful) | 0.18 | 0.21 | 0.18 | 0.24 | ns |
| Cognitive process (e.g. cause, know ought) | 15.3 | 2.5 | 14.98 | 2.18 | ns |
| Time | |||||
| Focus past (e.g. ago, did, talk) | 2.26 | 1.09 | 2.7 | 1.37 | ns |
| Focus present (e.g. today, is, now) | 18.27 | 2.36 | 17.06 | 2.14 | .002 |
| Focus future (e.g. may, will, soon) | 1.83 | 0.72 | 2.05 | 0.79 | ns |
4). Support Vector Machine:
Support Vector Machines (SVM) are supervised non-probabilistic machine learning methods, that separate data points using hyperplanes. We used SVM for classification of dichotomous outcomes-i.e. mothers’ with and without a history of depression. Hassan et. al [44] examined the state-of-art supervised machine learning methods performance on LIWC features and found that SVM outperform other methods. Motivated by this finding, we also use SVM in our experiments. To evaluate the SVM learning model, the following classifier evaluation metrics were used: accuracy, precision, recall, positive agreement (PA), negative agreement (NA), and Cohen’s Kappa (κ).
For our experiments, we performed LOO testing with nested grid search to identify the best parameters. The search was done using 5 fold cross validation. LOO gives as an unbiased estimate of the error rates [45] over a k-fold and hence our results are based on the LOO testing. For the first experiment, we used LIWC features that have been identified in previous empirical research on language use in depression: first-person singular pronouns, second-person pronouns, positive emotion words, anger words, sadness words, anxiety words, cognitive process words, focus past words, focus present words, and focus future words; we refer to it as Model 1.
Next, we used SHapley Additive exPlanation (SHAP) [46] approach to understand what features would be significant for SVM prediction. As SHAP values are averaged they have multiple advantages such as they are regularized, consistent and are not prone to multicollinearity distortions. Next, to see the prominent features and how they affect the SVM predictions, we plotted the SHAP values [47]. Finally, for the second experiment we trained a SVM using only those features that were identified to be most impactful, by SHAP values, to see if there is change in the predictive power of the SVM; referred to as Model 2.
IV. Results
A. Clinical outcome measures
At assessment, mothers in the depressed group (N 72) had a PHQ-9 mean of 12.15 (SD=5.89, range=2–27) and mothers in the non-depressed group (N 68) had a PHQ-9 of 2.42 (SD=2.55, range=0–12).
B. Predicting Mothers’ Depression vs. Non-Depression
The descriptive statistics of the LIWC features in mothers with and without a history of depression can be seen in Table III.
Model 1, the SVM classifier gave 62.85% accuracy, 0.63 precision, 0.67 recall, 0.65 PA score, 0.61 NA, and 0.26 κ. From the confusion matrix (Figure 1a), it can be seen that 48 cases were correctly classified as depressed and 40 cases as non-depressed. We performed the Chi Square Contingency test, and obtained p<.01, indicating the model was not a random guess.
Fig. 1:

Confusion Matrix for SVM Classifier
Figure 2a plots SHAP values in decreasing order of feature importance. The top feature is most important and the bottom feature is the least important. Each point on the SHAP plot is a prediction from the LOO validation, and the color represents the value of the feature; red color indicates a higher value of the linguistic feature whereas blue color indicates a lower linguistic feature value. The position of the dot indicates the effect of the linguistic feature; when the SHAP value is negative it indicates that the linguistic feature is contributing towards the non-depressed and when the linguistic feature is positive it is indicative that the linguistic feature is contributing towards the depressed category. Based on this and the plot, we can see that focus present, focus future, focus past, first-person singular pronouns, second-person pronouns and anger words are the most important linguistic features. Focus present, first-person singular pronouns, second-person pronouns, anger words and sadness words have a positive impact on SVM prediction; that is the higher the value, the prediction is more likely to be that the mother is in the depressed group. In contrast, focus future words, focus past words, cognitive process words and anxiety words have a negative impact on the prediction; the higher the value, the more likely the model is to predict that the mother is not in the depressed group.
Fig. 2:
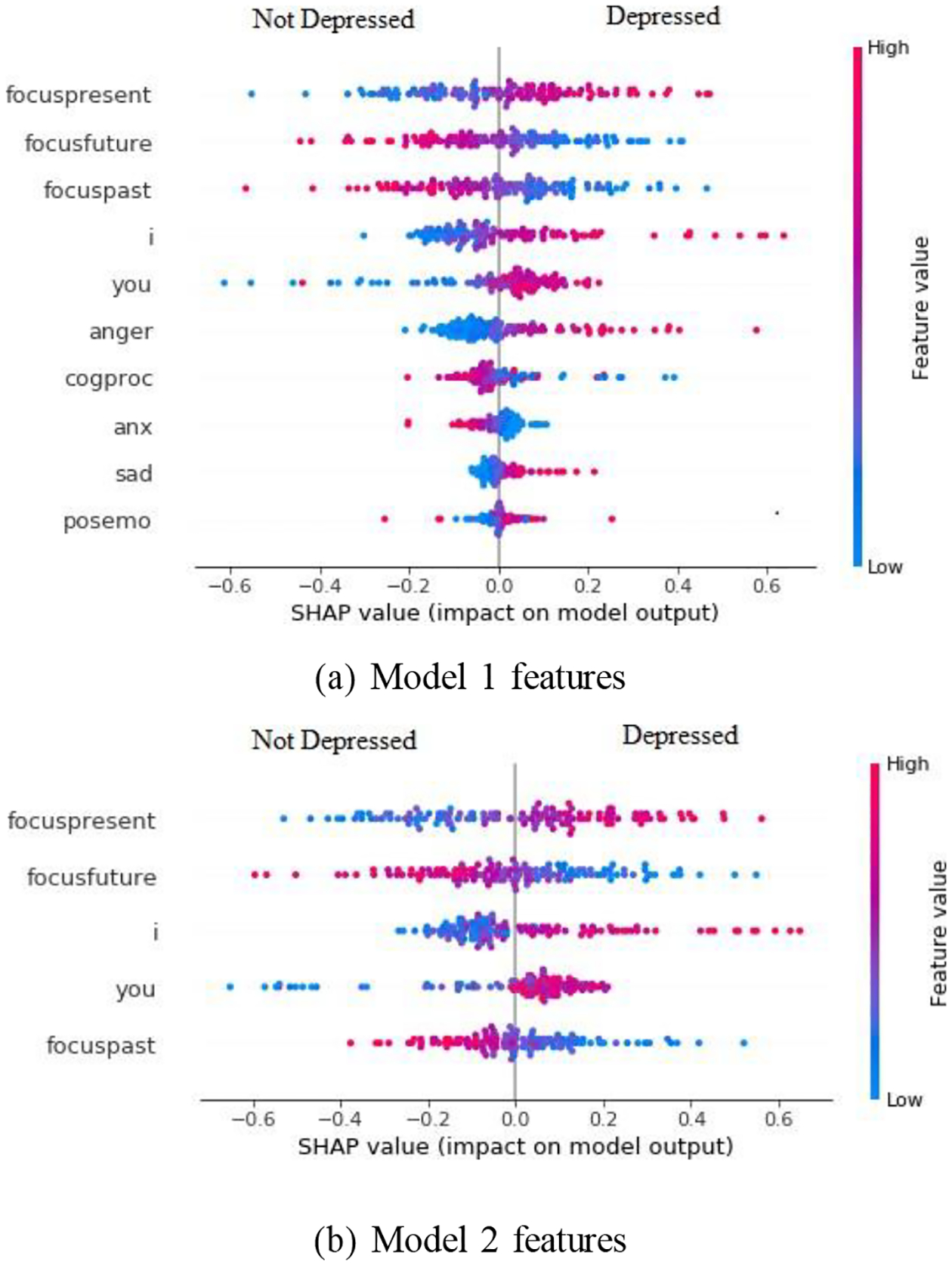
SHAP Values Plot
Based on Figure 2a, we selected the top 5 most SHAP impactful features; that is, focus present words, focus future words, focus past words, first-person singular pronouns, and second-person pronouns, and trained the second SVM model (Model 2). From Table IV, we can see that selecting just the top 5 linguistic features boosted SVMs predictive power across all the metrics. Accuracy increased from 62.85% to 67.15%, PA increased from 0.65 to 0.68, NA from 0.61 to 0.66, Precision from 0.63 to 0.68, Recall from 0.67 to 0.68 and κ from 0.26 to 0.34. Model 2 obtained p<.01, indicating the model was not a random guess. From Figure 1b, we can see that the SVM model can more accurately detect mothers in the non-depressed group. From the Figure 2, we can see that the impact of the linguistic features are consistent in both models, and the correlations of the linguistic features also remain consistent between both models. That is, increased values of focus present word, first-person singular pronouns, and second-person pronouns increased the chance of a prediction of mothers with a history of treatment for depression, whereas increased values of focus future words and focus past words decreased the chance of predicting mothers with a history of depression. Using McNemar’s test [48], we obtained p<.01, this shows that the two models were statistically different.
TABLE IV:
Performance of the models
| Model 1 | Model 2 | |
|---|---|---|
| Number of Features | 10 | 5 |
| Accuracy | 0.63 | 0.67 |
| NA | 0.61 | 0.66 |
| PA | 0.65 | 0.68 |
| Precision | 0.63 | 0.68 |
| Recall | 0.67 | 0.68 |
| Cohen’s Kappa | 0.26 | 0.34 |
| Chi Sq (p-value) | <.01* | <.01* |
V. Discussion
The application of computer-assisted approaches to language analysis to examine, predict and classify depressive symptoms has assumed increased interest in various disciplines, including computing science and clinical psychology. In contrast to previous computer-assisted linguistic research that focused on language in individuals with depression across different contexts [22]– [35], or studies that examined depression in mothers and their offspring with an emphasis on language reflecting positive affect [37], [38], this study is novel as it is the first to examine the effectiveness of an automatic algorithm based on Support Vector Machines (SVM) to discriminate between mothers with and without a history of depression (Depressed and Non-Depressed).
The results supported the hypothesis that the LIWC features were critical in achieving a sufficient level of accurate discrimination between mothers with and without a history of depression, with a classification performance of approximately 63%. According to our findings, the LIWC features that predicted mothers with a history of depression related to a high frequency of words with a focus on the present, pre-occupation with themselves and their adolescent conversational partner, and feelings of anger, whereas LIWC features that predicted mothers without a history of depression related to a high frequency of words that focus on the past and future. However, cognitive process words, positive emotion words, anxiety and sadness words did not contribute sufficiently to the model.
Consistent with previous empirical research [49], the language of mothers with a history of depression was characterized by a high frequency of self-referential terminology as a marker of self-focused rumination and distress. Unsurprisingly previous studies identified that individuals with depression are also more likely to use negative emotion words [28], [50], and in our sample, anger words were a high-importance linguistic feature associated in mothers with a history of depression, but not sadness words as mentioned in previous research [33]. Anger typically relates to the occurrence of irritability and hostility, which has been associated with depression [25], and in this study it might be also related with an increased negative affective arousal elicited by the problem-solving task.
Interesting is the use of temporal words. In mothers with a history of depression, present focus was identified as a high-importance linguistic feature which might be related to increased reflection and rumination as part of resolving discrepancy experienced as part of problem-solving task. In contrast, mothers without a history of depression might have presented higher cognitive flexibility, reflected in a greater focus on past experiences as a reference for solving the problem-solving task and to guide related actions in the future [51].
Also consistent with our hypothesis, second-person pronouns ”you” were a high-importance linguistic feature in accurately classifying mothers with a history of depression, possibly indicating a lower-quality mother-child relationship characterized by negative relationship processes, such as higher conflict and lower interpersonal cohesion [19], compared to children of mothers without a history of depression.
VI. Conclusions
This study examined the possibility and effectiveness of using a language-based classifier to discriminate between mothers with and without a history of treatment for depression. We assessed the importance of the included linguistic features that would be significant for SVM prediction, and through this identified a set of high and low-importance linguistic features. These findings extend the existing literature-base with a focus on language style by a) exploring the application of a linguistic classifier, b) analyzing language obtained in the context of lab-based parent-child dyadic interactions, and c) including mothers with and without a history of treatment for depression. These findings extend the existing literature-base on the relationship between language and mood states with a focus on the linguistic style of mothers with and without a history of treatment for depression, and its potential impact on child development and transgenerational transmission of depression.
Acknowledgments
Research reported in this publication was supported in part by the US National Institutes of Health under Award Number MH096951. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Ethical Impact Statement
The study has obtained ethical approval from the Institutional Review Board (IRB) at Oregon Research Institute, and secondary-data analysis of the study was ethically approved by the University of Pittsburgh and University of Edinburgh. Prior to participation, all participants (i.e. mothers and adolescents) provided informed consent and assent, respectively. All participants were informed about their ethical right to decline and withdraw from the study, potential risks, protections to minimize risks, and limits of confidentiality. Risk of potential discomfort associated with the data collection procedure were mitigated following ethical guidelines, including explaining procedures to the participants, and during the debrief, following the lab-based data collection, the researchers asked participants about their well-being and offered information of local support services.
Contributor Information
Laura A. Cariola, Clinical and Health Psychology, University of Edinburgh, Edinburgh, UK
Saurabh Hinduja, Department of Psychology, University of Pittsburgh, Pittsburgh, USA.
Maneesh Bilalpur, Intelligent Systems Program, University of Pittsburgh, Pittsburgh, USA.
Lisa B. Sheeber, Oregon Research Institute, Eugene, USA
Nicholas Allen, Department of Psychology, University of Oregon, Eugene, USA.
Louis-Philippe Morency, Language Technologies Institute, Carnegie Mellon University, Pittsburgh, USA.
Jeffrey F. Cohn, Department of Psychology, University of Pittsburgh, Pittsburgh, USA, Deliberate.AI, NY, USA
References
- [1].Hasin DS, Sarvet AL, Meyers JL, Saha TD, Ruan WJ, Stohl M, and Grant BF, “Epidemiology of adult dsm-5 major depressive disorder and its specifiers in the united states,” JAMA psychiatry, vol. 75, no. 4, pp. 336–346, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].“National institute of mental health https://www.nimh.nih.gov/health/statistics/major-depression.”
- [3].Ertel KA, Rich-Edwards JW, and Koenen KC, “Maternal depression in the united states: Nationally representative rates and risks,” Journal of women’s health, vol. 20, no. 11, pp. 1609–1617, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, and Heyward D, “Maternal depression and child psychopathology: A meta-analytic review,” Clinical child and family psychology review, vol. 14, no. 1, pp. 1–27, 2011. [DOI] [PubMed] [Google Scholar]
- [5].Loechner J, Sfärlea A, Starman K, Oort F, Thomsen LA, Schulte-Körne G, and Platt B, “Risk of depression in the offspring of parents with depression: The role of emotion regulation, cognitive style, parenting and life events,” Child Psychiatry & Human Development, vol. 51, no. 2, pp. 294–309, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Goldberg D, “The aetiology of depression,” Psychological medicine, vol. 36, no. 10, pp. 1341–1347, 2006. [DOI] [PubMed] [Google Scholar]
- [7].Levinson DF, “The genetics of depression: a review,” Biological psychiatry, vol. 60, no. 2, pp. 84–92, 2006. [DOI] [PubMed] [Google Scholar]
- [8].Weissman MM, Berry OO, Warner V, Gameroff MJ, Skipper J, Talati, Pilowsky DJ, and Wickramaratne P, “A 30-year study of 3 generations at high risk and low risk for depression,” JAMA psychiatry, vol. 73, no. 9, pp. 970–977, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Wolford SN, Cooper AN, and McWey LM, “Maternal depression, maltreatment history, and child outcomes: The role of harsh parenting.” American journal of orthopsychiatry, vol. 89, no. 2, p. 181, 2019. [DOI] [PubMed] [Google Scholar]
- [10].Campbell SB, Brownell CA, Hungerford A, Spieker SJ, Mohan R, and Blessing JS, “The course of maternal depressive symptoms and maternal sensitivity as predictors of attachment security at 36 months,” Development and psychopathology, vol. 16, no. 2, pp. 231–252, 2004. [DOI] [PubMed] [Google Scholar]
- [11].Leinonen JA, Solantaus TS, and Punamäki R-L, “Parental mental health and children’s adjustment: The quality of marital interaction and parenting as mediating factors,” Journal of child psychology and psychiatry, vol. 44, no. 2, pp. 227–241, 2003. [DOI] [PubMed] [Google Scholar]
- [12].Norcross PL, Leerkes EM, and Zhou N, “Examining pathways linking maternal depressive symptoms in infancy to children’s behavior problems: The role of maternal unresponsiveness and negative behaviors,” Infant Behavior and Development, vol. 49, pp. 238–247, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Jaser SS, Fear JM, Reeslund KL, Champion JE, Reising MM, and Compas BE, “Maternal sadness and adolescents’ responses to stress in offspring of mothers with and without a history of depression,” Journal of Clinical Child & Adolescent Psychology, vol. 37, no. 4, pp. 736–746, 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Cohn JF, Cummins N, Epps J, Goecke R, Joshi J, and Scherer S, “Multimodal assessment of depression from behavioral signals,” The Handbook of Multimodal-Multisensor Interfaces: Signal Processing, Architectures, and Detection of Emotion and Cognition-Volume 2, pp. 375–417, 2018. [Google Scholar]
- [15].Nelson BW, Sheeber L, Pfeifer JH, and Allen NB, “Affective and autonomic reactivity during parent–child interactions in depressed and non-depressed mothers and their adolescent offspring,” Research on Child and Adolescent Psychopathology, vol. 49, no. 11, pp. 1513–1526, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Schwartz OS, Byrne ML, Simmons JG, Whittle S, Dudgeon P, Yap MB, Sheeber LB, and Allen NB, “Parenting during early adolescence and adolescent-onset major depression: A 6-year prospective longitudinal study,” Clinical Psychological Science, vol. 2, no. 3, pp. 272–286, 2014. [Google Scholar]
- [17].Pennebaker JW, Boyd RL, Jordan K, and Blackburn K, “The development and psychometric properties of liwc2015,” Tech. Rep, 2015. [Google Scholar]
- [18].Robbins ML, Mehl MR, Smith HL, and Weihs KL, “Linguistic indicators of patient, couple, and family adjustment following breast cancer,” Psycho-Oncology, vol. 22, no. 7, pp. 1501–1508, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Georgiou PG, Black MP, and Narayanan SS, “Behavioral signal processing for understanding (distressed) dyadic interactions: some recent developments,” in Proceedings of the 2011 joint ACM workshop on Human gesture and behavior understanding, 2011, pp. 7–12. [Google Scholar]
- [20].Simmons RA, Gordon PC, and Chambless DL, “Pronouns in marital interaction: What do “you” and “i” say about marital health?” Psychological science, vol. 16, no. 12, pp. 932–936, 2005. [DOI] [PubMed] [Google Scholar]
- [21].Beck A, Depression: Clinical, experimental and theoretical aspects, 1969.
- [22].De Choudhury M, Gamon M, Counts S, and Horvitz E, “Predicting depression via social media,” in Seventh international AAAI conference on weblogs and social media, 2013. [Google Scholar]
- [23].Islam M, Kabir MA, Ahmed A, Kamal ARM, Wang H, Ulhaq A et al. , “Depression detection from social network data using machine learning techniques,” Health information science and systems, vol. 6, no. 1, pp. 1–12, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Tadesse MM, Lin H, Xu B, and Yang L, “Detection of depression-related posts in reddit social media forum,” IEEE Access, vol. 7, pp. 44 883–44 893, 2019. [Google Scholar]
- [25].Al-Mosaiwi M and Johnstone T, “In an absolute state: Elevated use of absolutist words is a marker specific to anxiety, depression, and suicidal ideation,” Clinical Psychological Science, vol. 6, no. 4, pp. 529–542, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Eichstaedt JC, Smith RJ, Merchant RM, Ungar LH, Crutchley P, Preoţiuc-Pietro D, Asch DA, and Schwartz HA, “Facebook language predicts depression in medical records,” Proceedings of the National Academy of Sciences, vol. 115, no. 44, pp. 11 203–11 208, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].O’Dea B, Larsen ME, Batterham PJ, Calear AL, and Christensen H, “A linguistic analysis of suicide-related twitter posts.” Crisis: The Journal of Crisis Intervention and Suicide Prevention, vol. 38, no. 5, p. 319, 2017. [DOI] [PubMed] [Google Scholar]
- [28].Park M, McDonald D, and Cha M, “Perception differences between the depressed and non-depressed users in twitter,” in Proceedings of the International AAAI Conference on Web and Social Media, vol. 7, no. 1, 2013, pp. 476–485. [Google Scholar]
- [29].Ramirez-Esparza N, Chung C, Kacewic E, and Pennebaker J, “The psychology of word use in depression forums in english and in spanish: Testing two text analytic approaches,” in Proceedings of the international AAAI conference on web and social media, vol. 2, no. 1, 2008, pp. 102–108. [Google Scholar]
- [30].Stirman SW and Pennebaker JW, “Word use in the poetry of suicidal and nonsuicidal poets,” Psychosomatic medicine, vol. 63, no. 4, pp. 517–522, 2001. [DOI] [PubMed] [Google Scholar]
- [31].Dirkse D, Hadjistavropoulos HD, Hesser H, and Barak A, “Linguistic analysis of communication in therapist-assisted internet-delivered cognitive behavior therapy for generalized anxiety disorder,” Cognitive behaviour therapy, vol. 44, no. 1, pp. 21–32, 2015. [DOI] [PubMed] [Google Scholar]
- [32].Jones LS, Anderson E, Loades M, Barnes R, and Crawley E, “Can linguistic analysis be used to identify whether adolescents with a chronic illness are depressed?” Clinical psychology & psychotherapy, vol. 27, no. 2, pp. 179–192, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Sonnenschein R, Hofmann SG, Ziegelmayer T, and Lutz W, “Linguistic analysis of patients with mood and anxiety disorders during cognitive behavioral therapy,” Cognitive behaviour therapy, vol. 47, no. 4, pp. 315–327, 2018. [DOI] [PubMed] [Google Scholar]
- [34].Zimmermann J, Brockmeyer T, Hunn M, Schauenburg H, and Wolf M, “First-person pronoun use in spoken language as a predictor of future depressive symptoms: Preliminary evidence from a clinical sample of depressed patients,” Clinical psychology & psychotherapy, vol. 24, no. 2, pp. 384–391, 2017. [DOI] [PubMed] [Google Scholar]
- [35].Tackman M, Sbarra DA, Carey AL, Donnellan MB, Horn AB, Holtzman NS, Edwards TS, Pennebaker JW, and Mehl MR, “Depression, negative emotionality, and self-referential language: A multi-lab, multi-measure, and multi-language-task research synthesis.” Journal of personality and social psychology, vol. 116, no. 5, p. 817, 2019. [DOI] [PubMed] [Google Scholar]
- [36].Rodriguez J, Holleran SE, and Mehl MR, “Reading between the lines: The lay assessment of subclinical depression from written self-descriptions,” Journal of personality, vol. 78, no. 2, pp. 575–598, 2010. [DOI] [PubMed] [Google Scholar]
- [37].Goodlett D, Trentacosta CJ, McLear C, Crespo L, Wheeler R, Williams A, Chaudhry K, and Smith-Darden J, “Maternal depressive symptoms and at-risk young children’s internalizing problems: The moderating role of mothers’ positivity,” Merrill-Palmer quarterly (Wayne State University. Press), vol. 63, no. 1, p. 77, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Moran KM, Root AE, Vizy BK, Wilson TK, and Gentzler AL, “Maternal socialization of children’s positive affect regulation: Associations with children’s savoring, dampening, and depressive symptoms,” Social Development, vol. 28, no. 2, pp. 306–322, 2019. [Google Scholar]
- [39].Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, and Mokdad H, “The phq-8 as a measure of current depression in the general population,” Journal of affective disorders, vol. 114, no. 1–3, pp. 163–173, 2009. [DOI] [PubMed] [Google Scholar]
- [40].Prinz RJ, Foster S, Kent RN, and O’Leary KD, “Multivariate assessment of conflict in distressed and nondistressed mother-adolescent dyads,” Journal of applied behavior analysis, vol. 12, no. 4, pp. 691–700, 1979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Nelson W, Byrne ML, Sheeber L, and Allen NB, “Does context matter? a multi-method assessment of affect in adolescent depression across multiple affective interaction contexts,” Clinical psychological science, vol. 5, no. 2, pp. 239–258, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].First MB and Gibbon M, “The structured clinical interview for dsm-iv axis i disorders (scid-i) and the structured clinical interview for dsm-iv axis ii disorders (scid-ii).” 2004.
- [43].Kroenke K, Spitzer RL, and Williams JB, “The phq-9: validity of a brief depression severity measure,” Journal of general internal medicine, vol. 16, no. 9, pp. 606–613, 2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Hasan M, Kotov A, Carcone AI, Dong M, Naar S, and Hartlieb KB, “A study of the effectiveness of machine learning methods for classification of clinical interview fragments into a large number of categories,” Journal of biomedical informatics, vol. 62, pp. 21–31, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Lachenbruch PA and Mickey MR, “Estimation of error rates in discriminant analysis,” Technometrics, vol. 10, no. 1, pp. 1–11, 1968. [Google Scholar]
- [46].Lipovetsky S and Conklin M, “Analysis of regression in game theory approach,” Applied Stochastic Models in Business and Industry, vol. 17, no. 4, pp. 319–330, 2001. [Google Scholar]
- [47].Lundberg SM and Lee S-I, “A unified approach to interpreting model predictions,” in Advances in Neural Information Processing Systems 30, Guyon I, Luxburg UV, Bengio S, Wallach H, Fergus R, Vishwanathan S, and Garnett R, Eds. Curran Associates, Inc., 2017, pp. 4765–4774. [Online]. Available: http://papers.nips.cc/paper/7062-a-unified-approach-to-interpreting-model-predictions.pdf [Google Scholar]
- [48].McNemar Q, “Note on the sampling error of the difference between correlated proportions or percentages,” Psychometrika, vol. 12, no. 2, pp. 153–157, 1947. [DOI] [PubMed] [Google Scholar]
- [49].Holtzman NS et al. , “A meta-analysis of correlations between depression and first person singular pronoun use,” Journal of Research in Personality, vol. 68, pp. 63–68, 2017. [Google Scholar]
- [50].Rude S, Gortner E-M, and Pennebaker J, “Language use of depressed and depression-vulnerable college students,” Cognition & Emotion, vol. 18, no. 8, pp. 1121–1133, 2004. [Google Scholar]
- [51].Williams HL, Conway MA, and Cohen G, “Autobiographical memory.” 2008.