

Abstract
Background
The distal end radius's bony anatomy in relation to three variables—Radial Inclination, Volar tilt, and radial height—has been discussed commonly in the adult population and is not very well defined in the growing skeleton. In children aged 8–16 years old, we measured the osseous distal end radius according to radiography standards. The research comprised 130 patients, 65 males and 65 females aged 8–16. In each child, the norms for radial inclination, volar tilt, and radial epiphyseal height were established. This research defines these radiographic parameters for the paediatric population in India for the first time.
Methods
This research is an Unicentric Cross-sectional observational analytical study. We studied 130 normal wrist posteroanterior and lateral radiographs of the Indian paediatric population aged 8–16 years who reported to our OPD and calculated the three parameters—(1) Radial height, (2) Volar Tilt, and (3) Radial Inclination. Mean measurement values were analysed statistically.
Results
The Mean distal end radius volar tilt is 10.92° ± 1.76° SD with a range from 4° to 15°. The Mean distal end radial inclination is 21.04° ± 2.10° SD with a range from 15° to 25°. The Mean distal end radial height is 11.93 ± 1.44 mm SD with a range from 9.0 to 14.50 mm.
Conclusion
In true Postero-anterior and lateral wrist radiographs of the Indian paediatric population, we have established normal values that may be utilized as a guide for the evaluation and treatment of a variety of traumatic and non-traumatic problems in Indian children.
Keywords: Distal radius, Volar tilt, Epiphysis, Radial inclination
Introduction
Adult diseases affecting the wrist and distal end radius have been treated clinically using the often-discussed factors of volar tilt (additionally known as palmar inclination or palmar tilt), radial height, and radial inclination, linked to the osseous structure of the adult distal end radius [1]. To our knowledge, there has been no study conducted to identify the standard values of volar tilt, radial inclination and radial height in the Indian paediatric population. We looked at the radiographic measures of the typical osseous anatomy of the distal end radius in the paediatric population of India.
Materials and Methods
This research is an Unicentric Cross-sectional observational analytical study. Once our institution's research and ethical committee had given its approval (IEC/42/43), we studied 130 normal wrist posteroanterior and lateral radiographs of the Indian paediatric population aged 8–16 years reporting to our OPD and calculated the three parameters- (1) Radial height, (2) Volar Tilt, and (3) Radial Inclination. Mean measurement values were analysed statistically. The radiographs were taken for different reasons. Routinely in our practice, in the paediatric age group, we prefer doing bilateral forearm radiographs for comparison of the affected side with the normal side in the upper limb (forearm) trauma cases. Forearm radiographs are also routinely performed in cases of children with spinal deformity [2] and coronal plane deformities of the knees to assess the skeletal growth that determines the modality of treatment in these patients. In patients with contralateral non-traumatic pathology, radiographs were also collected for comparison with the unaffected side. We selected 16 as our cut-off age because it is likely that by then both males and females would have attained skeletal maturity [3]. We have chosen the lower limit of age to be 8 years because of several reasons. Firstly, the ossification of the last carpal bone, the Pisiform, typically occurs between the ages of 8 and 12 years. This facilitates the measurement of parameters around the distal radius during this age range. Secondly, according to a study by Gandhi RK et al. [4], most deformities of the distal third of the radius tend to fully correct within 5 years after the fracture. Considering that the distal radial epiphysis may fuse at any time between 15 and 25 years (Caffey, 1956) [5], there is a greater reluctance to accept angular deformities in children over 8–10 years of age. Thirdly, remodelling is proportional to the remaining growth potential and is more pronounced in younger children (< 8 years) [6]. Additionally, remodelling is reduced in the upper extremities compared to lower extremities, probably because the lower extremities are subjected to greater mechanical loads [7]. Based on these considerations, we established a lower limit of 8 years for our study as restoration of the normal anatomy after this age group should have no/less margin of error. Every radiograph was thoroughly examined, and we eliminated any patients who exhibited bilaterally visible signs of acute or chronic damage or deformity at the distal end of the radius. To get our measurements, we employed the Postero-anterior and lateral radiographs. Only true lateral radiographs—defined as having the ulnar head entirely superimposed behind the radius—have been used in the research [8–10]. True PA criteria include the distal radius ulna joint having no or minimum overlap, the metacarpal bases having no or minimal overlap, and the ulnar styloid process beginning from the medial ulnar cortex of the ulna bone [8–10]. On the AGFA Healthcare workstation, the radiographs had to be modified such that the magnification was set to 100% size (true size). We may view the radiographs from this computer workstation and use the computer to draw lines and angles. Instantaneously, the workstation displays the length in millimetres or centimetres and the angle in degrees. Only one observer supplied these length and angle values into the data collecting form.
Technique
Volar Tilt: On a lateral radiograph of the wrist, it is calculated as the angle between a line drawn perpendicular to the long axis of the radius and a tangent line drawn along the slope of the dorsal-to-palmar surface of the radius (as shown in Fig. 1). A normal Indian adult Volar tilt is 4°–17° [11].
Fig. 1.

True lateral view showing measurement of volar tilt on AGFA workstation
Radial Inclination: It is calculated on Postero-anterior view as the angle between a line drawn parallel to the radius's long axis and a line drawn along the distal radius's articular surface (as shown in Fig. 2). A normal Indian adult radial inclination is 21°–33° [11].
Fig. 2.
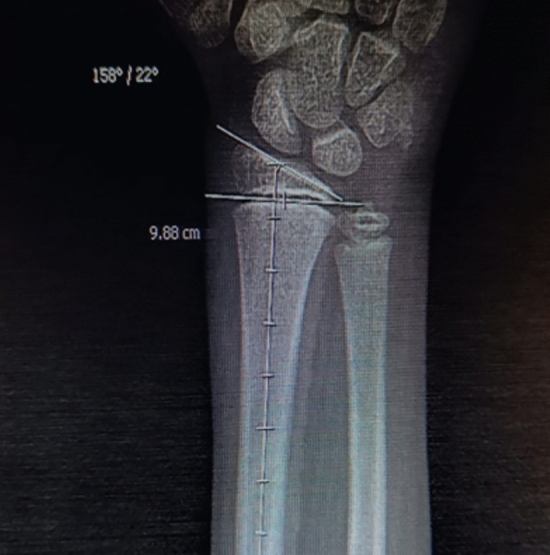
True postero-anterior view of wrist showing measurement of radial inclination angle on AGFA workstation
Radial Height (Distal Radial Epiphyseal Height): Because the distal radius physis hampers the measurement of radial height in children, we have measured the height of the distal end radius physis instead of the radial height (as shown in Fig. 3). A normal Indian adult radial height is 9.1–16.7 mm [11].
Fig. 3.

True postero-anterior view of wrist showing measurement of radial height on AGFA workstation
Results
The research comprised 130 patients, 65 boys and 65 girls, varying in age from 8 to 16 years. For each patient in the aforementioned age range, the normal range of values for radial inclination, volar tilt, and radial epiphyseal height was established. The range of values of radial epiphyseal, volar tilt, and radial inclination height and their variations with gender and age are summarized in Tables 1, 2, 3.
Table 1.
Descriptive statistics of various parameters in the study (N = 130)
| Mean (SD) | Median | Range | |
|---|---|---|---|
| Volar tilt (degrees) | 10.92 (1.76) | 11.00 | 4.0–15.0 |
| Radial inclination (degrees) | 21.04 (2.10) | 21.00 | 15.0–25.0 |
| Radial height (mm) | 11.93 (1.44) | 12.00 | 9.0–15.0 |
Table 2.
Gender and mean (SD) of various parameters in the study
| Volar tilt (degrees) | Radial inclination (degrees) | Radial height (mm) | |
|---|---|---|---|
| Female | 11.20 (1.71) | 21.78 (1.82) | 11.87 (1.52) |
| Male | 10.63 (1.77) | 20.29 (2.11) | 11.99 (1.36) |
| P value | 0.065 | < 0.001 | 0.652 |
Table 3.
Age and mean (SD) of various parameters in the study
| Age (years) | Volar tilt (degrees) | Radial inclination (degrees) | Radial height (mm) |
|---|---|---|---|
| 8–10 (n = 65) | 9.92 (1.66) | 19.62 (1.65) | 10.91 (0.94) |
| 11–13 (n = 41) | 11.34 (0.99) | 21.80 (1.24) | 12.45 (0.86) |
| 14–16 (n = 24) | 12.87 (0.94) | 23.58 (1.01) | 13.80 (0.87) |
| P value | < 0.001* | < 0.001* | < 0.001* |
The mean values and the normal range of the three parameters in the Indian paediatric population aged 8–16 years old are summarised in Table 1. The Mean distal end radial volar tilt is 10.92° ± 1.76° SD with a range from 4° to 15°. The Mean distal end radial inclination is 21.04° ± 2.10° SD with a range from 15° to 25°. The Mean distal end radial height is 11.93 ± 1.44 mm SD with a range from 9.0 to 14.50 mm.
The variations of these values with gender are summarised in Table 2 and Fig. 4. Mean distal end radial Volar Tilt is 11.20° (± 1.71°) in females which is more than that in males at 10.63° (± 1.77°). Mean distal end Radial Inclination is 21.78° (± 1.82°) which is more than that in males at 20.29° (± 2.11°). Mean distal end radial height is 11.99 mm (± 1.36 mm) in males which is more than that in females at 11.87 mm (± 1.52 mm).
Fig. 4.
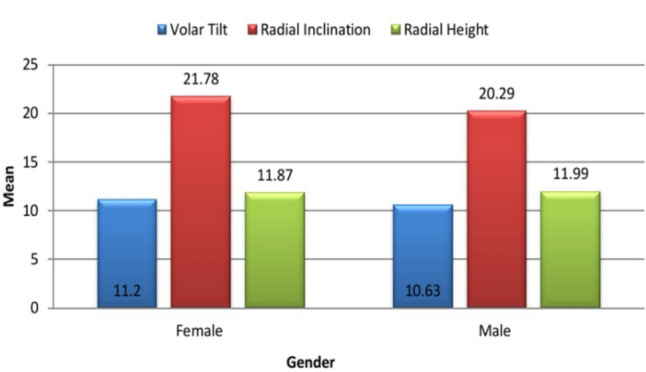
Variations of parameters with gender
The variations of these parameters with increasing age are summarised in Table 3; Figs. 5, 6. All these values demonstrated an increasing trend with an increase in age. This shows that the radiographic anatomy of the distal end radius in children changes with age.
Fig. 5.

Variations of parameters with age
Fig. 6.

Variations of parameters with age
Discussion
Due to the metaphyseal development spurt, “the distal end of the radius is among the most often fractured locations in children aged 8–16 years. These fractures typically occur following a fall onto an extended hand. It is diagnosed by wrist radiographs and is majorly managed by closed reduction and casting [12, 13]. Significantly displaced or angulated fractures in patients who are nearing skeletal maturity need surgery [14]. Despite being a fairly frequent injury (fractures of the distal forearm constitute 35–45% of all pediatric long bone fractures) [15], the distal radius anatomy in the Indian paediatric population has never been studied radiographically.
In adolescents and children, a number of non-traumatic diseases, including congenital abnormalities, may impede the growth as well as development of the distal radius, carpus, and ulna. As normal wrist geometry and development are vital contributing factors to maintaining proper wrist growth and function as well as conducting proper wrist motions, restoring distal end radius parameters in paediatric fractures and non-traumatic diseases affecting the wrist is crucial. Since there is still growth potential left in this age group, restoration of the distal end radius normal anatomy can prevent long-term issues like growth plate disruption, deformities, and impaired wrist function. The steady rise in both the distal radial size and slope with aging is explained by the growth of the radial height and inclination. Loss of radial height is a practical indicator of a worse prognosis in distal radial fractures [16]. Both the paediatric and adult populations basically agree on this [17]. In physeal distal radius fractures, loss of radial height results from either overlap (bayonet apposition) or metaphyseal comminution [16]. Growth will result in an increase in the strain across the lunate due to loss of radial inclination [17].
Three values that are routinely used to ascertain the need for surgery and the acceptability of correction in adults are (1) radial height, (2) radial inclination, and (3) volar tilt. For adults, the average values of these 3 measures are known; however, for the Indian paediatric population, they are not. Our study identified the normal range of three radiographic parameters—(1) Radial height, (2) Radial inclination, and (3) Volar tilt” in the Indian paediatric population aged 8–16 years on Postero-anterior and Lateral view of the wrist radiograph. Less bone overlap may be seen in the Postero-anterior view, making it simpler to calculate these parameters. Also, two different studies: One by Johnson [16] and another by Pennock et al. [17] demonstrate that the apparent morphometric measures at the distal end of the radius are considerably increased when the forearm is supinated.
Our study has its limitations. Children have significant cartilaginous epiphyseal components periarticularly which makes them very different from adults. Only the ossified anatomy that is evident on simple radiographs has been the subject of our investigation. MR imaging is not cost-effective, despite the fact that it would have increased visibility of this cartilaginous component. Hence it becomes impractical as the study includes a large volume of patients. Another limitation of the study is the lack of ethnicity of the subjects. The study was performed at a large teaching hospital in Mumbai. Although the ethnicity of each patient was not noted for this study, results of the latest census done in 2011 [19] reveal that in the state of Maharashtra, particularly Mumbai, the population consisted of 60.7% Hindu, 25.1% Muslims, 5.4% Jain. 0.49% Sikhs, 4.4% Buddhist, 2.7% Christians 0.40% Sikh. Based on the population, we expect our study results to mostly represent normal values in Hindu population.
The difference between our study and the Western literature is compared in Table 4. In our study, the range of distal end radial inclination is 15°–25° which is in the reference range of Hosseinzadeh and Olson [1], 2018 (19.66°–24.79°) and of Sallam et al. [18], 2020 (10.5°–33.5°). The range of volar tilt in our study is 4°–15° and the lower/upper limit does not fall in the reference range of volar tilt in a study by Hosseinzadeh and Olson [1], 2018 (9.96°–13.57°) but it falls in the reference range of Sallam et al. [18] (0°–16°). The range of distal end radial height in our study is 9.0–14.50 mm which is not significantly different from the reference range of Hosseinzadeh and Olson [1], 2018 (8.73–14.01 mm). It also falls in the reference range of Sallam et al. [18], 2020 (6.6–15.4 mm). Our findings may be utilized therapeutically to create a template of normal values that doctors treating children with fractures and wrist pathologies may utilize as a reference.
Table 4.
Comparison of our study to western literature on the paediatric population
| Our study (n = 130) Age: 8–16 indian population |
Hosseinzadeh P and Olson D1, 2018 (n = 372) Age: 8–16 Caucasians |
Sallam AA, Briffa N12, 2020 (n = 896) |
|
|---|---|---|---|
| Radial inclination | 15.0–25.0 | 19.66–24.79 | 10.5–33.5 |
| Volar tilt | 4.0–15.0 | 9.96–13.57 | 0–16 |
| Radial height | 9.0–14.50 | 8.73–14.01 | 6.6–15.4 |
Conclusion
In true Postero-anterior and lateral wrist radiographs of the Indian paediatric population, we have established normal values that may be utilized as a guide for the evaluation and treatment of a variety of traumatic and non-traumatic problems in Indian children.
Acknowledgements
We would like to express our gratitude to all those who contributed to this research project in various ways. We are grateful to LTMMC and GH, Sion for providing the data necessary for our study and appreciate the support from the institute in facilitating the research process. We would like to thank the Institutional Ethics Committee in LTMMC and GH for their expertise in research methodology and for scrutinizing the protocol of our study, which significantly contributed to the methodology of this study. We acknowledge their guidance and oversight to ensure compliance with ethical standards. We acknowledge the invaluable technical assistance (AGFA WORKSTATION) provided by the Department of Radiology in LTMMC and GH Hospital, Sion. We express our gratitude to the patients who participated in the study, without whom this research would not have been possible. We thank Dr Prashantha Bettappa for his expert statistical advice, which was crucial in the analysis of our data and we also acknowledge his contributions in designing tables and graphs for this study. We would like to acknowledge and thank any other individuals or entities that have made significant contributions to this work.
Funding
None.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable requests.
Declarations
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Institutional Ethics Committee Human research, LTMMC AND GH, SION + Ref: IEC/42/43) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Hosseinzadeh, P., Olson, D., Eads, R., Jaglowicz, A., Goldfarb, C. A., & Riley, S. A. (2018). Radiologic evaluation of the distal radius indices in early and late childhood. The Iowa Orthopaedic Journal,38, 137. [PMC free article] [PubMed] [Google Scholar]
- 2.Luk, K. D., Saw, L. B., Grozman, S., Cheung, K. M., & Samartzis, D. (2014). Assessment of skeletal maturity in scoliosis patients to determine clinical management: A new classification scheme using distal radius and ulna radiographs. The Spine Journal,14(2), 315–325. 10.1016/j.spinee.2013.10.045 [DOI] [PubMed] [Google Scholar]
- 3.Kirmani, S., Christen, D., Van Lenthe, G. H., Fischer, P. R., Bouxsein, M. L., McCready, L. K., Melton, L. J., III., Riggs, B. L., Amin, S., Müller, R., & Khosla, S. (2009). Bone structure at the distal radius during adolescent growth. Journal of Bone and Mineral Research,24(6), 1033–1042. 10.1359/jbmr.081255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gandhi, R. K., Wilson, P., Mason Brown, J. J., & Macleod, W. (1962). Spontaneous correction of deformity following fractures of the forearm in children. Journal of British Surgery,50(219), 5–10. 10.1002/bjs.18005021903 [DOI] [PubMed] [Google Scholar]
- 5.Caffey, J. (1956). Pediatric X-ray Diagnosis (3rd ed., p. 691). Chicago: The Year Book Publishers. [Google Scholar]
- 6.Stilli, S., Magnani, M., Lampasi, M., Antonioli, D., Bettuzzi, C., & Donzelli, O. (2008). Remodelling and overgrowth after conservative treatment for femoral and tibial shaft fractures in children. La Chirurgia degli Organi di Movimento,91, 13–19. 10.1007/s12306-007-0003-6 [DOI] [PubMed] [Google Scholar]
- 7.Naik, P. (2021). Remodelling in children’s fractures and limits of acceptability. Indian Journal of Orthopaedics,55(3), 549–559. 10.1007/s43465-020-00320-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Freiberg, K. S. (1979). Remodeling after distal forearm fractures in children. I. The effect of residual angulation on the spatial orientation of the epiphyseal plates. Acta Orthopaedica Scandinavica,50, 537–546. 10.3109/17453677908989801 [DOI] [PubMed] [Google Scholar]
- 9.Friberg, K. S. (1979). Remodelling after distal forearm fractures in children II: The final orientation of the distal and proximal epiphyseal plates of the radius. Acta Orthopaedica Scandinavica,50(6), 731–739. 10.3109/17453677908991303 [DOI] [PubMed] [Google Scholar]
- 10.Friberg, K. S. (1979). Remodelling after distal forearm fractures in children III: Correction of residual angulation in fractures of the radius. Acta Orthopaedica Scandinavica,50(6), 741–749. 10.3109/17453677908991304 [DOI] [PubMed] [Google Scholar]
- 11.Tambe, D., Goregaonkar, A., Sheth, B., & Pawar, J. (2018). Research article Orthopaedics. International Journal of Orthopaedics,4(1), 147–152. [Google Scholar]
- 12.Pershad, J., Williams, S., Wan, J., & Sawyer, J. R. (2009). Pediatric distal radial fractures treated by emergency physicians. The Journal of emergency medicine,37(3), 341–344. 10.1016/j.jemermed.2008.08.030 [DOI] [PubMed] [Google Scholar]
- 13.Jones, K., & Weiner, D. S. (1999). The management of forearm fractures in children: A plea for conservatism. Journal of pediatric orthopaedics,19(6), 811. 10.1097/01241398-199911000-00021 [DOI] [PubMed] [Google Scholar]
- 14.Miller, J. D., & Riley, S. A. (2012). Current concepts in pediatric distal radial fractures. Current Orthopaedic Practice,35, 409–413. 10.1097/BCO.0b013e318266f09f [DOI] [Google Scholar]
- 15.Noonan, K. J., & Price, C. T. (1998). Forearm and distal radius fractures in children. JAAOS-Journal of the American Academy of Orthopaedic Surgeons,6(3), 146–156. 10.5435/00124635-199805000-00002 [DOI] [PubMed] [Google Scholar]
- 16.Johnson, P. G., & Szabo, R. M. (1993). Angle measurements of the distal radius: A cadaver study. Skeletal Radiology,22, 243–246. 10.1007/BF00197667 [DOI] [PubMed] [Google Scholar]
- 17.Pennock, A. T., Phillips, C. S., Matzon, J. L., & Daley, E. (2005). The effects of forearm rotation on three wrist measurements: Radial inclination, radial height and palmar tilt. Hand Surgery,10(01), 17–22. 10.1142/S0218810405002528 [DOI] [PubMed] [Google Scholar]
- 18.Sallam, A. A., Briffa, N., Mahmoud, S. S., & Imam, M. A. (2020). Normal wrist development in children and adolescents: A geometrical observational analysis based on plain radiographs. Journal of Pediatric Orthopaedics,40(9), e860–e872. 10.1097/BPO.0000000000001584 [DOI] [PubMed] [Google Scholar]
- 19.Census of India. (2011). Maharashtra Series 28 Part XII-A. Mumbai: District Census Handbook. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable requests.