

Abstract
Patient: Male, 74-year-old
Final Diagnosis: Abdominal aortic aneurysm (AAA)
Symptoms: Dispnoea • pain in lumbar region • pulsatile mass
Clinical Procedure: Open surgical repair of AAA • spinal anesthesia
Specialty: Anesthesiology • Surgery
Objective:
Unusual or unexpected effect of treatment
Background:
Elderly patients with severe or multiple comorbidities can be at high risk for complications of general anesthesia. This report is of a 74-year-old man with severe comorbidities, including ischemic heart disease (IHD) and chronic obstructive pulmonary disease (COPD), and successful abdominal aortic aneurysm repair with thoracic segmental spinal anesthesia.
Case Report:
The patient, aged 74, had previously been diagnosed with severe COPD and IHD. He was classified as American Society of Anesthesiology (ASA) grade IV, diagnosed with an abdominal aortic aneurysm (AAA) measuring 6 cm in diameter, and had to undergo surgical repair of the aneurysm with the insertion of a synthetic graft. Due to a shortage of beds in the ICU and the desire to avoid the complications associated with general anesthesia, the decision was made to proceed with thoracic spinal regional anesthesia, which is not a customary choice for this type of surgery. Spinal anesthesia was administered at the Th10-11 level, utilizing 8.5 mg of Bupivacaine, 50 mcg of Fentanyl, and 4 mg of Dexason. An epidural catheter was placed at the same level. The surgical procedure lasted 145 min and was successfully completed under regional anesthesia.
Conclusions:
This report has highlighted that developments in spinal thoracic anesthesia mean that this can be a successful alternative to general anesthesia in high-risk patients, even for major emergency surgery.
Keywords: Anesthesia, Spinal; Aorta, Abdominal; Bupivacaine; Thoracic Vertebrae
Introduction
More than 100 years have passed since the seminal introduction of “general spinal anesthesia” by Thomas Jonnesco in 1909, utilized for various types of surgeries. This technique involved puncturing the subarachnoid space between the 1st and 2nd thoracic vertebrae, and between the 10th thoracic and 1st lumbar vertebrae for abdominal surgeries, achieving profound and comprehensive analgesia [1]. Neuraxial anesthesia is used alone or in combination with general anesthesia for most procedures below the neck [2]. Spinal anesthesia performed at the thoracic level of the spine is commonly known as thoracic spinal anesthesia. It is a neuraxial anesthesia technique that has been a subject of considerable debate among anesthesiologists, including the risk of external injury to the spinal cord, cranial distribution of the local anesthetic, and blocking of the sympathetic fibers that innervate the heart, potentially resulting in severe bradycardia and low blood pressure [3–5]. In 2006 and 2007, Van Zundert et al published a case report and subsequently a feasibility study on 20 patients with severe chronic obstructive pulmonary disease (COPD) undergoing surgery, such as laparoscopic cholecystectomy, using combined spinal-epidural anesthesia at the thoracic level of the spine [6,7]. In most patients, either general anesthesia or regional anesthesia can be used without any problems. However, in certain cases, the nature of the surgical intervention or the patient’s comorbid conditions may dictate the choice of anesthesia technique, including the use of thoracic spinal anesthesia. [8–10]. Patients with lung disease facing surgical interventions are at a higher risk of experiencing complications both during and after the procedure. Various complications, such as laryngospasm, bronchospasm, and prolonged mechanical ventilation, pose challenges in managing patients with COPD undergoing abdominal surgery [11]. Regional anesthesia techniques are the method of choice for patients with known cardiopulmonary disorders. In some geriatric centers, this technique is becoming the preferred choice of anesthesia [12]. The literature on major abdominal surgery performed under neur-axial anesthesia techniques is scarce, making it challenging to find relevant studies. With this context in mind, we report the case of a male patient with a known history of COPD, classified as American Society of Anesthesiology (ASA) grade IV, diagnosed with an abdominal aortic aneurysm (AAA), who underwent resection of the aneurysmal segment under thoracic spinal anesthesia [13]. Case reports have been published previously for endovascular or open surgical aortic repair under regional epidural anesthesia [14,15].
This report is of a 74-year-old man with severe comorbidities, including ischemic heart disease (IHD) and chronic obstructive pulmonary disease (COPD), and successful abdominal aortic aneurysm repair with thoracic segmental spinal anesthesia.
Case Report
A 74-year-old man who was a cigarette smoker was diagnosed with an abdominal aortic aneurysm (AAA) measuring 6 cm in diameter. He was scheduled for open surgery to repair the aneurysmal portion of the AAA, which would involve replacing it with a synthetic vascular graft. General anesthesia is typically the method of choice for such operations due to its ability to ensure hemodynamic stability, control of the airways and ventilation, and provide muscle relaxation during surgery. However, in situations where Intensive Care Unit (ICU) beds for postoperative care are lacking, along with a scarcity of resources for respiratory support in the postoperative period, the complications of general anesthesia in patients with severe respiratory issues necessitate considering alternative methods. This was particularly relevant for this patient, who had severe COPD, heart problems, and was on medications including anticoagulants, beta-blockers, calcium channel blockers, and bronchodilators. There was a contingency plan in case of the need for ICU admission, transferring him to a hospital with ICU beds located very close (2 km) to the hospital where the operation was done.
It was decided to proceed with regional anesthesia, a combination of spinal anesthesia performed at a low thoracic level combined with epidural anesthesia. Spinal anesthesia was administered at the Th10-11 level using a 27-gauge (G) Quincke spinal needle (Figure 1), and an epidural catheter was placed at the Th11-12 level using an 18-G Tuohy needle. The medications used were 8.5 mg of Bupivacaine (1.7 ml of 0.5% heavy Bupivacaine), 50 mcg of Fentanyl, and 4 mg of Dexamethasone, all administered subarachnoidally via the spinal needle. Fifteen min after administration, the sensory block extended from Th6 to L1.
Figure 1.

Performing thoracic spinal anesthesia at Th10-11 with 27-G spinal needle.
Within the first 20 min after the anesthesia was administered, a drop in blood pressure to 80/40 mm Hg was recorded, which was successfully treated with intravenous normal saline 0.9% and bolus doses of 5 mg Ephedrine. Blood pressure returned to normal levels 30 min after initiation of spinal anesthesia. This was the only adverse effect noted during the surgical procedure. The surgery lasted 145 min, and in the final 40 min, epidural anesthesia was initiated with a bolus of 8 ml of 0.375% Bupivacaine.
Very good analgesia was achieved at the end of the operation through the epidural catheter. The catheter was also used for postoperative pain control, administering a combination of 0.125% Bupivacaine with 1 mcg/ml Fentanyl. No drop in blood pressure or other adverse effects were noted during the epidural anesthesia.
The surgery was performed without any complications. The patient underwent graft reconstruction of the AAA under thoracic spinal anesthesia, achieving very good analgesia and without any respiratory compromise (Figures 2, 3). After the surgery, he was transferred to a surgical ward in a very stable condition, awake, with normal vital signs. No neurological sequelae were recorded during the hospital stay. On the 5th postoperative day, he was discharged to home.
Figure 2.
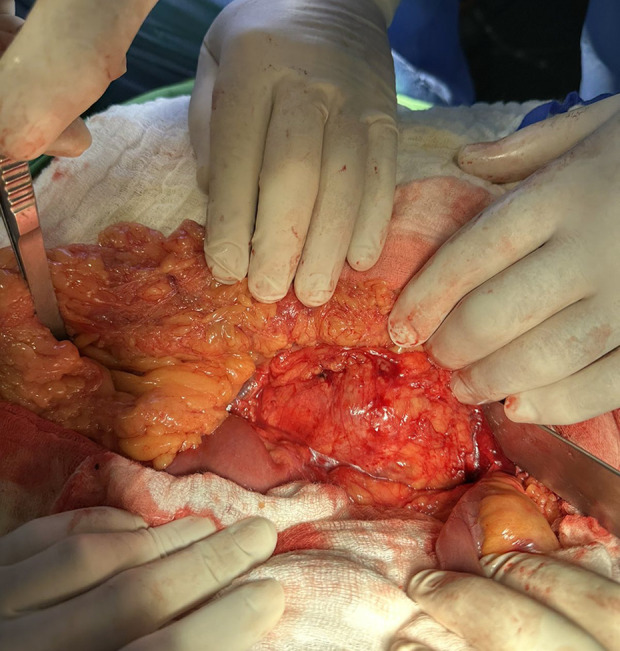
Abdominal aortic aneurysm before removal of the aneurismatic part.
Figure 3.
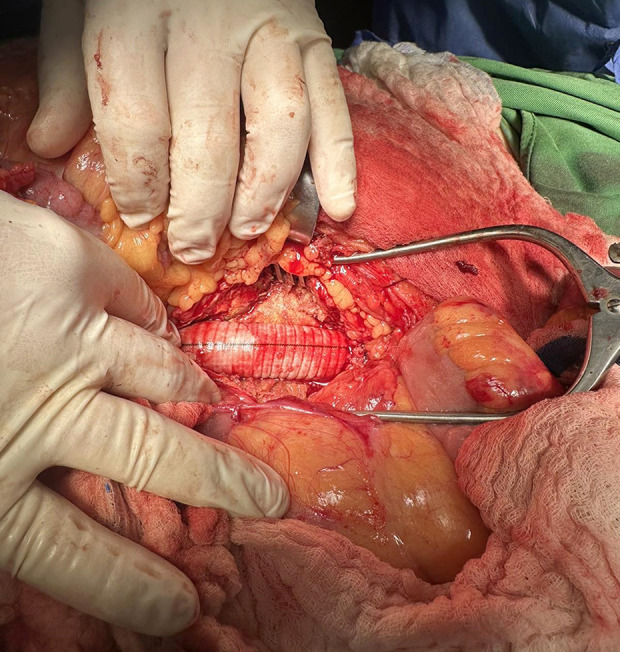
Aorta abdominalis after placement of an aortic vascular graft.
Discussion
This case report shows that spinal thoracic anesthesia as a regional neuraxial technique can be safely used for a major abdominal operation such as AAA. This technique emphasizes that anesthesia and analgesia provided for this patient was sufficient for open surgery, repair the aneurysmal portion of the AAA.
Thoracic spinal anesthesia is not commonly described in anesthesia textbooks, and its use above the L1-L2 level of the lumbar spine is not recommended [16,17]. Several studies using magnetic resonance imaging (MRI) have demonstrated that the posterior distance between the spinal cord and dura mater in the thoracic region, which is widest in the mid-thoracic region [18,19], supports the safety of performing spinal anesthesia in this area.
Although not routinely used, several publications have demonstrated that thoracic spinal anesthesia is a convincing and satisfactory method for various types of surgeries. Imbelloni et al, in a study involving 1406 patients who underwent thoracic spinal anesthesia, concluded that there were no neurological deficits following its use [20]. Our case report supports all these major findings. It was a safe procedure and did not cause a neurologic deficit for our patient.
In certain patients, due to underlying conditions and the nature of the surgical intervention, the risk of perioperative complications, including prolonged ICU stays after general anesthesia, is heightened [21]. In such instances, regional anesthesia may be preferred to minimize complications associated with general anesthesia. In our case, by employing thoracic spinal anesthesia, the patient did not require an ICU bed, resulting in a shorter hospital stay and lower financial costs. Spinal anesthesia, compared to general anesthesia, offers several advantages, such as improved postoperative analgesia, reduced reliance on opioid analgesics, preservation of spontaneous breathing during surgery, and the benefit of remaining conscious throughout the procedure, which in turn can decrease postoperative cognitive dysfunction [22]. It has been reported that, as a result, both ICU and hospital stays are shortened, leading to a reduction in financial costs [23,24]. Compared to all the above, our patient did not require ICU admission, his hospital stay was shorter, there was no cognitive disfunction, and it resulted in lower financial costs due to both regional anesthesia and zero days of ICU stay.
Although thoracic spinal anesthesia is rarely used for various types of operations, the case report presented here demonstrates its successful application and management even in major surgery. The placement of an aortic graft in a patient with an AAA is considered high-risk surgery, with several possible complications [25].
There are case reports of endovascular repair and open surgical repair of AAA by regional anesthesia solely using epidural anesthesia [14,15], but there are few case reports on using spinal thoracis anesthesia for this kind of surgery. Both epidural and spinal anesthesia were effectively used for this procedure.
Patient and medical personnel satisfaction was high, and the procedure was completed without any complications. This report has highlighted that developments in spinal anesthesia can provide a successful alternative to general anesthesia in high-risk patients, even for major emergency surgery, including abdominal aortic aneurysm repair.
Conclusions
Several studies have shown that thoracic spinal anesthesia, when administered by qualified professionals, is safe and effective for various types of abdominal surgery, most notably for laparoscopic cholecystectomy. However, more data are needed to substantiate its safety advantages compared to current anesthesia techniques.
This report has highlighted that developments in spinal anesthesia can provide a successful alternative to general anesthesia in high-risk patients, even for major emergency surgery, including abdominal aortic aneurysm repair.
Footnotes
Publisher’s note: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher
Declaration of Figures’ Authenticity
All figures submitted have been created by the authors who confirm that the images are original with no duplication and have not been previously published in whole or in part.
References:
- 1.Jonnesco T. Remarks on general spinal analgesia. Br Med J. 1909;2(2550):1396–401. doi: 10.1136/bmj.2.2550.1396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Olawin A, Das J. StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2024. Spinal anesthesia. [Updated 202 June 27] Available from: https://www.ncbi.nlm.nih.gov/books/NBK537299/ [Google Scholar]
- 4.Kowalewski R, Seal D, Tang T, et al. Neuraxial anesthesia for cardiac surgery: Thoracic epidural and high spinal anesthesia – why is it different? HSR Proc Intensive Care Cardiovasc Anesth. 2011;3(1):25–28. [PMC free article] [PubMed] [Google Scholar]
- 4.Shatri G, Singh A. StatPearls [Internet] Treasure Island (FL): StatPearls Publishing; 2024. Thoracic segmental spinal anesthesia. [Updated 2023 Jul 31] Available from: https://www.ncbi.nlm.nih.gov/books/NBK572087/ [PubMed] [Google Scholar]
- 5.Mahmoud AA, Hussein H, Kamal A, et al. The novel use of spinal anesthesia at the mid-thoracic level: A feasibility study. Egypt J Cardiothorac Anesth. 2014;8(1):21–26. [Google Scholar]
- 6.van Zundert AAJ, Stultiens G, Jakimowicz JJ, et al. Segmental spinal anaesthesia for cholecystectomy in a patient with severe lung disease. Br J Anaesth. 2006;96(4):464–66. doi: 10.1093/bja/ael036. [DOI] [PubMed] [Google Scholar]
- 7.van Zundert AAJ, Stultiens G, Jakimowicz JJ, et al. Laparoscopic cholecystectomy under segmental thoracic spinal anaesthesia: A feasibility study. Br J Anaesth. 2007;98(5):682–86. doi: 10.1093/bja/aem058. [DOI] [PubMed] [Google Scholar]
- 8.Ghaffari S, Dehghanpisheh L, Tavakkoli F, Mahmoudi H. The effect of spinal versus general anesthesia on quality of life in women undergoing cesarean delivery on maternal request. Cureus. 2018;10(12):e3715. doi: 10.7759/cureus.3715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Alaali HH, Irwin MG. Anaesthesia for urological surgery. Anaesthesia and Intensive Care Medicine. 2021;22(7):449–53. [Google Scholar]
- 10.Paria R, Surroy S, Majumder M, et al. Spinal at T10 [10th Thoracic] IOSR J Dent Med Sci. 2014;13(8):28–32. [Google Scholar]
- 11.Park S, Eun Jung O, Han S, et al. Intraoperative anesthetic management of patients with chronic obstructive pulmonary disease to decrease the risk of postoperative pulmonary complications after abdominal surgery. J Clin Med. 2020;9(1):150. doi: 10.3390/jcm9010150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Spannella F, Giulietti F, Damiani E, et al. Thoracic continuous spinal anesthesia for high-risk comorbid older patients undergoing major abdominal surgery: One-year experience of an italian geriatric hospital. Minerva Anestesiol. 2020;86(3):261–69. doi: 10.23736/S0375-9393.19.13896-5. [DOI] [PubMed] [Google Scholar]
- 13.Horvath B, Kloesel B, Todd MM, et al. The evolution and future of the american society of anesthesiologists physical status classification system. Anesthesiology. 2021;135(5):904–19. doi: 10.1097/ALN.0000000000003947. [DOI] [PubMed] [Google Scholar]
- 14.Cheruku S, Huang N, Meinhardt K, Aguirre M. Anesthetic management for endovascular repair of the thoracic aorta. Anesthesiol Clin. 2019;37(4):593–607. doi: 10.1016/j.anclin.2019.07.001. [DOI] [PubMed] [Google Scholar]
- 15.Yu S, Park S, Hong Y, Lee G. Surgical repair of abdominal aortic aneurysm under epidural anesthesia in patient with chronic obstructive pulmonary disease a case report. Korean J Thorac Cardiovasc Surg. 2006;39(10):782–85. [Google Scholar]
- 16.Rosenblatt WH SW. Barash clinical anesthesia. Clinical Anesthesia. 2013 [Google Scholar]
- 17.DiLorenzo AN, Schell RM. Morgan & Mikhail’s clinical anesthesiology. 5th Edition. Anesth Analg; 2014. [Google Scholar]
- 18.Park JW, Bae SK, Huh J. Distance from Dura mater to spinal cord at the thoracic vertebral level: An introductory study on local subdural geometry for thoracic epidural block. J Int Med Res. 2016;44(4):950–56. doi: 10.1177/0300060516652751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lee RA, Van Zundert AAJ, Botha CP, et al. The anatomy of the thoracic spinal canal in different postures: A magnetic resonance imaging investigation. Reg Anesth Pain Med. 2010;35(4):364–69. doi: 10.1097/aap.0b013e3181e8a344. [DOI] [PubMed] [Google Scholar]
- 20.Luiz Eduardo I, Marcos F, Raphael S, et al. Thoracic spinal anesthesia is safe and without neurological sequelae: Study with 1,406 patients. Int J Anesth Anesthesiol. 2022;9(2):148. [Google Scholar]
- 21.Gavali H, Mani K, Tegler G, et al. Editor’s choice – Prolonged ICU length of stay after AAA repair: Analysis of time trends and long-term outcome. Eur J Vasc Endovasc Surg. 2017;54(2):157–63. doi: 10.1016/j.ejvs.2017.05.014. [DOI] [PubMed] [Google Scholar]
- 22.Cottrell JE, Hartung J. Anesthesia and cognitive outcome in elderly patients: A narrative viewpoint. J Neurosurg Anesthesiol. 2020;32(1):9–17. doi: 10.1097/ANA.0000000000000640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yousef G, Lasheen A. General anesthesia versus segmental thoracic or conventional lumbar spinal anesthesia for patients undergoing laparoscopic cholecystectomy. Anesth Essays Res. 2012;6(2):167–73. doi: 10.4103/0259-1162.108302. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 24.Imbelloni L. Spinal anesthesia for laparoscopic cholecystectomy: Thoracic vs. lumbar technique. Saudi J Anaesth. 2014;8(4):477–83. doi: 10.4103/1658-354X.140853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kumar A, Persaud P, Leite AF, et al. Aortic aneurysm: Clinical findings, diagnostic and treatment. IntechOpen; 2021. Available at: https://www.intechopen.com/chapters/76514. [Google Scholar]