

ABSTRACT
Aim
This systematic review was designed to compare the clinical effectiveness of high-viscosity glass ionomer cement (HVGIC) restorations to direct composite resin (CR) restorations in single- or multisurface cavities in primary teeth.
Background
Restorative procedures are typically used to treat caries in primary teeth. Due to their improved preservation of the natural tooth structure and their adhesion to the remaining tooth structure, CR and GIC have drawn attention as the preferred restorative materials. In the literature, over the past 20 years, the term HVGIC has developed. Compared to C-GICs, HVGICs appear to have a higher survival rate. However, isolated studies provide contradictory findings regarding the durability of restorations in primary teeth.
Materials and methods
Major electronic databases were thoroughly searched to find publications from the years 2000 to 2021. Studies included were randomized and nonrandomized clinical trials on children aged 3–13 years, in which restoration of primary teeth using HVGIC and CR was performed.
Results
This systematic review includes four studies [three randomized controlled trials (RCTs) and one nonrandomized controlled trial]. No statistically significant difference between these materials was seen in any of the included studies.
Conclusion
This systematic review of findings supports the assertion that both HVGIC and CR restorations deliver satisfactory outcomes in terms of clinical efficacy and overall survivability. It was found that, for both materials, class I restorations had statistically higher survival rates than class II restorations. Long-term studies are essential to evaluate the clinical efficacy of both restorations.
Clinical significance
This systematic review outlines the application of HVGIC and CR as restorative materials for pediatric dentists to use in their everyday dental practices.
How to cite this article
Krishnakumar K, Kalaskar R, Kalaskar A, et al. Clinical Effectiveness of High-viscosity Glass Ionomer Cement and Composite Resin as a Restorative Material in Primary Teeth: A Systematic Review of Clinical Trials. Int J Clin Pediatr Dent 2024;17(2):221–228.
Keywords: Clinical effectiveness, Composite resin, High-viscosity glass ionomer, Primary teeth, Systematic review
Introduction
Rationale
One of the most common diseases of the oral cavity is dental caries. It has a high incidence due to poor oral hygiene practices and eating foods high in carbohydrates, together with socioeconomic and behavioral variables.1–3 Mainly, restorative procedures are typically used to treat caries in primary teeth.4 Due to their improved preservation of the natural tooth structure and their adhesion to the remaining tooth structure, composite resin (CR) and glass ionomer cement (GIC) has drawn attention as the preferred restorative materials.5 These qualities enable the use of more conservative restorative methods, restricting cavity preparation to the removal of carious lesion in order to protect the healthy tooth structures.6 In fact, deeper carious, fractured, and attrited teeth are thought to be best treated with CR as a restorative material. As a result of composite fillings’ much higher durability compared to their glass ionomer equivalent, this restoration has become a popular choice.7 Based on numerous longitudinal studies and laboratory research, C-GICs were deemed to lack sufficient mechanical properties for widespread use as definitive restorations because they were deemed to be less durable and to fail much more frequently than resin composite when used as posterior occlusal or approximal restorations.5,7 Over the past 20 years, the term “high-viscosity glass ionomer cement (HVGIC)” has developed in the literature. Compared to C-GICs, HVGICs appear to have a higher survival rate, which is equivalent to traditional amalgam restorations. Also, it has a surface hardness that is comparable to fine-particle hybrid composites and its resilience to abrasion is clearly greater than that of conventional GIC.8 However, isolated studies provide contradictory findings regarding the durability of restorations in primary teeth. Hence, systematic reviews, particularly those using meta-analysis, are required to support clinicians in their clinical decision-making.9 Therefore, the purpose of this systematic review is to determine if HVGI restorations indeed have a higher clinical effectiveness than direct resin composite restorations in patients with single and/or multiple surface cavities in primary teeth.
Objectives
To compare the clinical effectiveness of HVGI restorations and direct resin composite restorations in single- or multisurface cavities in primary teeth.
Materials and Methods
Protocol and Registration
The systematic review protocol was submitted to the International Prospective Register of Systematic Reviews (PROSPERO), National Institute for Health Research) (ID-CRD42021235983). This review is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement from 2009.10
Eligibility Criteria
The inclusion criteria of the studies were defined a priori with the goal of evaluating the clinical effectiveness of HVGIC and CR as restorative materials in primary teeth (Table 1). Randomized controlled trials (RCTs) on children aged 3–13 years in which restorations in primary teeth were included. All eligible trials reported a 12-month or longer follow-up.
Table 1:
Eligibility criteria of the included studies
| Inclusion criteria | Exclusion criteria | |
|---|---|---|
| Participant/population characteristics | Children with carious lesions in primary dentition, Studies conducted the period of on children in age-group of 3–13 years Study conducted on primary teeth with dentinal carious lesions requiring restoration Studies having a clinical follow-up of at least 12 months |
Children with caries in permanent dentition Primary teeth with caries requiring endodontic treatment such as direct pulp capping, indirect pulp capping, pulpotomy, and pulpectomy Studies having clinical follow-ups <12 months |
| Intervention | Studies with primary teeth restored with high-viscosity glass-ionomer restoration Studies with primary teeth restored with viscous glass ionomer restoration |
Studies with type II GIC Cavity restored with silver amalgam, ZnO, ZnPO4 RMGC |
| Comparison/control group | Studies with primary teeth restored with light-cured composite Studies where light curing of composite with incremental technique is done Studies with bulk filling of resin restoration are done |
|
| Outcome | Clinical effectiveness of restoration Fractured restorations, Secondary caries on restoration margins, Partial or total loss of restoration retention, Excessive wear of the restoration material, Caries preventive restoration |
|
| Study design | Randomized controlled trials (RCT) Non-RCTs |
Case reports Case series Laboratory studies Cross-sectional studies Discussions Interviews Editorials Opinions Unpublished studies Review articles Conference abstracts Commentaries Replies to editor/author |
Information Sources
A systematic search of major electronic databases, PubMed, the Cochrane Central Register of Clinical Trials (CENTRAL), and Google Scholar, was conducted to encompass English-language publications from 2000 to 2021.
Search
Two authors independently designed the search keywords and strategy, and the search was carried out. For PubMed, a specific search method was adopted, and the search period was defined from January 2000 to October 2021. The keywords “Clinical survival AND High-viscosity glass ionomer AND CR AND Primary teeth” were used in the search on CENTRAL. A further search was conducted on Google Scholar using the search words “Comparison of HVGI restoration and CR in primary teeth—clinical trials” (Table 2).
Table 2:
Search strategy for PubMed, CENTRAL, and Google Scholar from 2000 to 2021
| PubMed search strategy (since 2000) | ||
|---|---|---|
| Serial number | Category (based on) | Keywords |
| 1 | Population | Primary teeth OR deciduous teeth OR children OR primary dentition OR deciduous dentition OR primary molars OR primary posteriors OR primary posterior teeth OR primary anterior teeth OR pediatric dental population OR pediatric dentistry OR pedodontic* OR pediatric* |
| 2 | Intervention | HVGIC OR high-viscosity glass ionomer OR high-viscosity GIC OR viscous glass ionomer cement OR Ketac Molar |
| 3 | Comparison | CR OR composite OR resin composite OR resin OR posterior CR OR conventional resin OR CR restoration OR resin-based composites OR dental resin composite OR dental composite |
| 4 | Outcome | Clinical efficiency OR clinical effectiveness OR clinical evaluation OR clinical survival OR clinical comparison OR clinical failure OR failure rate OR longevity OR success rate OR durability OR caries prevention OR caries preventive effect |
| 5 | Study design | Clinical trial OR randomized controlled trial OR RCT |
| 6 | #1 AND #2 AND #3 AND #4 AND #5 | |
| Total article | 35 | |
| Cochrane Central Register of Controlled Trials (CENTRAL) search strategy | ||
| Serial number | Category (based on) | Keywords |
| 1 | Population | Primary teeth |
| 2 | Intervention | CR |
| 3 | Comparison | High-viscosity glass ionomer |
| 4 | Outcome | Clinical survival |
| 5 | #1 AND #2 AND #3 AND #4 | |
| Total article | 5 | |
| Google scholar | ||
| Comparison of high-viscosity glass ionomer restoration and CR in primary teeth clinical trial | Total article = 4,410 | |
| Total = 4,450 articles | ||
Study Selection
Two independent authors selected the study and collected the data, and any discrepancies were handled by the third author. Two authors reviewed the title and abstract submissions. Full text was obtained for abstracts that met the inclusion requirements and in cases where abstract information was inconclusive. The full-text papers were subjected to stringent inclusion and exclusion criteria.
Data Collection Process
A customized data extraction form was used to collect data.
Data Extraction Form
Title of the study.
Name of author.
Publication year.
Institute and country of study.
Study design.
Ethical approval obtained.
Informed consent obtained.
Randomization method used (if any).
Control group (if present).
Comparator specifications.
Age of the patients that participated in the study and the control group.
Inclusion and exclusion criteria in the study group.
Inclusion and exclusion criteria in the control group.
The type of intervention that patients underwent.
Per test and control group.
Type of materials used for restoration.
Type of dentition.
Type of tooth restored.
Type of cavity.
Number of participants and number of teeth included at the commencement of the trial.
Assessment method used.
Assessment criteria followed.
Follow-up period.
Specific for HVGIC group.
Utilization of a rubber dam (yes/no).
Whether material releases fluoride (yes/no).
Specific for CR group.
Utilization of a rubber dam (yes/no).
Beveling of enamel (yes/no).
Type of cavity conditioning.
Type of adhesive system used.
Whether material releases fluoride (yes/no).
Contents
Data Items
Each included the trial's study design, randomization method, population description (including age and gender), sample size, and specific inclusion and exclusion standards for the study and control group were all extracted. The outcome and intervention were used to sort the data. The duration, type of cavity preparation with HVGIC versus composite restoration, the type of curing method, and bulk or incremental technique were all documented in the data that was gathered. The primary outcome was the clinical effectiveness of restoration, which included fractured restorations, secondary caries on restoration margins, partial or total loss of restoration retention, excessive wear of the restoration material, and caries’ preventive effect of the restoration.
Risk of Bias in Individual Studies
Different approaches were employed for RCTs and non-RCTs to assess the risk of bias (RoB) in individual studies. A tool devised by the Cochrane Collaboration was used to evaluate the RoB in the studies in order to establish the validity of the included studies. Using the Cochrane RoB tool, a randomized controlled trial's RoB was evaluated.11 It is part of the review manager 5.4.1 program. The reviewer used this tool to assess the RoB in the chosen studies by looking at the following factors—creation of random sequences, concealment of allocations, participant and personnel blindness, analysis intention (blinding of outcome assessment), incomplete outcome data, selective reporting (selection of the reported results), and other types of bias not previously taken into account (e.g., design bias, contamination bias).A “RoB” table contains one or more particular items for each domain. The first section of the tool is a description of what is alleged to have occurred in the research inside each entry. The tool's second section asks users to rate the likelihood of bias for each entry as either low risk, unclear risk, or high-risk. A single entry for each study addresses the tool's domains of sequence generation, allocation concealment, incomplete outcome data, and selective outcome reporting. For nonrandomized clinical studies, the RoB in Nonrandomized Studies of Interventions (ROBINS-I) tool was used to evaluate the RoB.12
Summary Measures
The primary outcome of this systematic review was to evaluate the clinical effectiveness of CR and HVGIC as restorative materials in primary teeth. To determine clinical effectiveness, various clinical criteria were specified in different studies. Fractured restorations, secondary caries on restoration margins, partial or complete restoration retention loss, excessive wear of the restorative material, and the restoration's ability to prevent caries were all included. As a result, the outcomes for HVGIC and CR restorations were segregated. The measures of effect were calculated from baseline to at least 3 months while taking into account an additional outcome of patient and parental acceptance.
Synthesis of Results
Both the HVGIC and CR restoration show favorable results in terms of clinical efficacy and overall longevity. No statistically significant difference between these materials was seen in any of the included studies.13,16 For both materials, it was shown that class I restorations had statistically higher survival rates than class II restorations.14 Because there were fewer trials included and because of the heterogeneity, there was not enough data to conduct further meta-analysis. Due to the wide range of various outcomes measured across the few numbers of existing trials, there was no room for meta-analysis.
Results
Study Selection
A total of 4,450 citations were obtained by searching PubMed via Medline, Cochrane, and Google Scholar databases between 2000 and 2021. Large numbers of the citations, especially those from Google Scholar, were irrelevant. A total of 55 items that were relevant were discovered after manually selecting them from each database. A total of 42 were left after removing duplicates. A total of 29 of these studies were disregarded since it was evident from reading the abstracts that these papers did not clearly fit the requirements. A more thorough analysis was done on the remaining 13 citations’ entire texts. Nine further studies were disregarded for an assortment of reasons, including the lack of the study's whole text or the difficulty of translating the article into English, retrospective trials, etc.
The systematic review contained four studies that satisfied the criteria for inclusion.13–16 No unpublished relevant studies were obtained (Flowchart 1).
Flowchart 1:

Flowchart showing identification and selection of studies
Study Characteristics
The results of each of the four studies that were included in this systematic review provide information on their characteristics (Table 3). Three of the four trials that were included were RCTs,13,14,16 and one was a nonrandomized controlled clinical trial.15
Table 3:
Population, intervention, control, outcome, and study design of included studies
| Serial number | Study | Country | Population | Restorative materials used | Follow-up period | Outcome | Study design |
|---|---|---|---|---|---|---|---|
| 1 | Akman and Tosun13 | Turkey | 160 class II carious lesions, 30 patients, primary teeth |
Equia™, Sonicfill™, X-tra fil™, Filtek Z550™ |
12 months | Clinical evaluation scores | RCT |
| 2 | Ersin et al.14 | Turkey | 419 restorations, 219 children, 6–10 years, class I and II primary teeth |
SureFil (packable resin-based composite), Fuji IX GP (HVGIC) |
24 months | Survival rate, marginal discoloration, marginal integrity, marginal caries, anatomical form, surface texture |
RCT |
| 3 | Kupietzky et al.16 | Israel | 87 patients primary teeth |
EQUIA GIC, Filtek™ |
36 months | Clinical parameters- retention of restoration, minor occlusal defects, contact point radiographic parameters- homogeneity of the material, concavity defect of proximal wall (loss of material in the proximal contact region), secondary caries, presence of radiolucent affected dentin layer |
RCT |
| 4 | Pani15 | Saudi Arabia | 87 patients, 258 restorations |
High-viscosity glass-ionomer (KetacFil™) Packable nanocomposite restoration (Filtek™ Z350 XT) |
24 months | Failure rates- secondary caries, failure |
Nonrandomized controlled trial |
All four studies were written and published in English.13–16 The intervention lasted 12 months in the study by Akman and Tosun,13 24 months in each of the studies by Ersin et al.14 and Pani,15 and 36 months in the study by Kupietzky et al.16 The largest study in terms of sample size, Ersin et al.14 study involved 219 children and 419 restorations on both classes I and II primary teeth. The study by Akman and Tosun13 examined one glass ionomer restorative system, two different bulk fill composites, and a nanohybrid composite, whereas all other studies compared one HVGIC and CR.14,15,16 For the purpose of evaluating clinical effectiveness, Ersin et al.14 and Kupietzky et al.16 both placed emphasis on clinical and radiographic criteria. Akman and Tosun13 concentrated on clinical evaluation scores at the same time that Pani15 concentrated on failure rates.8,10
Risk of Bias within Studies
Each study's methodological quality was rated as having low, high, or unclear risks. Only two out of three experiments adequately reported random sequence generation (low risk).13,16 None of the included studies reported any instances of allocation concealment (high-risk).13–16 Since it was impossible to blind the participants and the operator to the interventions due to the nature of the interventions, no studies had indicated blinding of the participants or the researcher carrying out the therapy (high-risk). All of the studies included sufficient mention of the blinding of outcome assessment, as well as the training and calibration of examiners in the evaluation of the relevant outcome.13–16 In two of the three studies, dropout rates and causes were given.14,16 One study included more participants than the intended sample size in order to account for the expected dropout.13 In every study, selective reporting was avoided.13–16 The absence of information on sample size estimation and the lack of reference to baseline demographic factors were also thought to be related to other unspecified types of bias. None of the studies had provided a baseline demographic and clinical table,13–16 and one study did not provide sample size estimation (Fig. 1).15
Fig. 1:
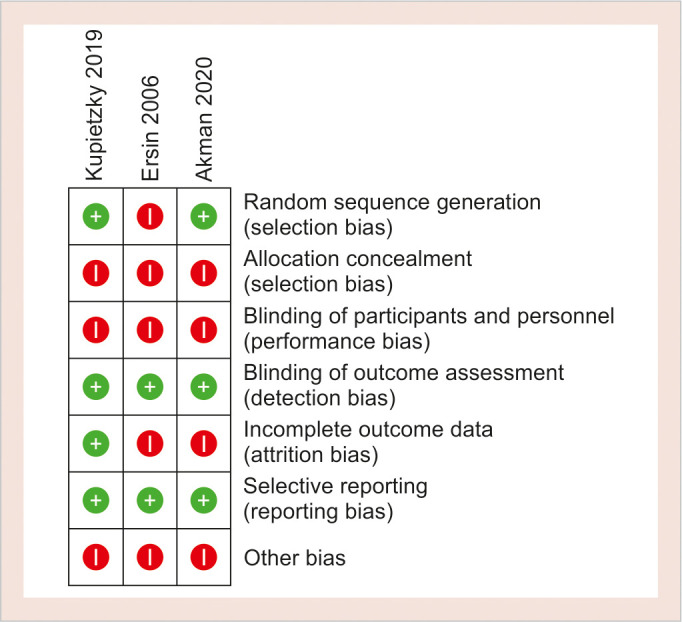
Risk of bias assessment of RCTs
The RoB in ROBINS-I tool was used to evaluate the quality of one of the studies that were included in this review.15 In terms of confounding, participant selection, classification of interventions, protocol deviations, missing data, assessment of the outcome, and reporting of the results, the study was found to have low risk (Table 4).
Table 4:
Risk of bias assessment (ROBINS-I tool)
|
Risk of bias assessment (ROBINS-I tool) Author: Pani, 15 2018 | ||
|---|---|---|
| Domain | Risk | Comment |
| Bias due to confounding | Low risk | No confounding expected |
| Bias in selection of participants into the study | Low risk | Same selection criteria applied through out |
| Bias in classification of interventions | Low risk | Intervention status is well defined |
| Bias due to deviations from intended interventions | Low risk | There were no deviations from the intended interventions |
| Bias due to missing data | Low risk | Data were reasonably complete |
| Bias in measurement of outcomes | Low risk | The methods of outcome assessment were comparable across intervention groups |
| Bias in selection of the reported result | Low risk | There is clear evidence that all reported results correspond to all intended outcomes, analyses and subcohorts |
| Overall judgement | Low risk | – |
Discussion
Summary of Evidence
Resin-based composites are increasingly being used for the treatment of primary molars. They possess superior physical and clinical qualities in comparison to traditional GICs, according to a number of studies. When used for class II restorations, they may have a longer survival time than GIC.17In addition, the atraumatic restorative treatment (ART) approach has grown in popularity in recent years for dental treatment of children using HVGIC, which has superior physical qualities than regular GIC.18,19 A quick turnaround on dental treatment is essential, especially in pediatric dentistry. HVGICs make the restorative treatment more pleasant and comfortable. They offer time-saving qualities and may be applied in bulk rather than technique-sensitive and time-consuming.13 The utilization of them in pediatrics is therefore beneficial. The resin-based composite was found to be satisfactory for class I and II restorations in primary teeth at the 24-month recall examination, according to a study by Ersin et al.14 For Class II restorations, the resin-based composite had a survival rate of 5.9% higher than the HVGIC, but this difference was not statistically significant. Additionally, the study discovered that for both restorative materials, the success rate for class I restorations at 24 months was greater than 90%, which is in line with previous studies and higher than the rate for some prior research. However, compared to class I restorations, the success rates for class II restorations were much lower at 76.1% for the HVGIC and 82% for the packable resin-based composite. Naturally, these findings are in line with prior ART research that demonstrated that multiple surface GIC restorations typically have lower survival rates than single-surface GIC restorations. Additionally, the loss of the restoration was the main cause of failure for class I and II restorations made of both materials. At the margin, caries were hardly ever seen. They also seldom encountered secondary caries, a critical factor in restorative failure. Furthermore, this latter finding was also found in two ART investigations. As a result, the surface texture, anatomical shape, marginal discoloration, and integrity of both materials were all satisfactory for all restorations used in this study.14 Additionally, the Equia system (HVGIC) had an α retention rate of 82%, according to the study results by Akman and Tosun.13 This was comparable to the results of the study by Turkun and Kanik,20 who assessed the Equia system in a 6-year randomized prospective trial of permanent teeth. When it came to the retention criteria at the conclusion of a 12-month clinical review, their study found that the Equia system received an α score in 88% of the cases. The increased translucency of the material, the presence of tiny glass particles, and newly created resin-based coating materials gave the HVGICs a better color matching with the surrounding tooth structures.20 The composite restorations used in this study by Akman and Tosun13 showed comparable levels of wear resistance to adjacent tooth structures and maintained their anatomical form throughout the study. The study came to the conclusion that Equia had a successful anatomical form and that the use of Gc Coat Plus improved the material's clinical performance. The experience and technique of the practitioner, the characteristics of the dental materials, the usage of rubber dams, and pediatric patient-dependent factors, such as behavior, high-caries risk, and age, all affect how long a restoration lasts. The retention of restorations is also influenced by occlusal variables, including clenching and bruxism, as well as the location and size of the restoration. The degree of marginal discoloration; however, was clinically acceptable (Bravo) for Equia despite the fact that it was only observed in a small number of instances throughout the course of the 1-year trial. At the same time, marginal discoloration was considerable, and some composite restorations received Bravo ratings. No restoration failed as a result of secondary caries, as determined by the radiographic examination data. This can be as a result of the patients’ good dental hygiene. Additionally, they claimed that the acid/base resistant layer or the release of fluoride ions from Equia could be responsible for the absence of any secondary caries in the Equia group.13 The clinical effectiveness of heat-cured HVGI class II restorations and CR restorations were also compared by Kupietzky et al.16 The findings of this study raised serious concerns about the long-term restorative efficacy of heat-cured GI for proximal lesions in primary molars. In contrast, a patient population from a private clinic with CR restorations showed a very high success rate of 95% after 3 years. The failure rate of the GI was nearly three times that of the CR, demonstrating the superiority of the CR over the HVGIC.Although both types of restorations in this study functioned effectively, more than a third of the GI restorations had concavity defects on the proximal wall of the box cervical to the contact point. However, in this study, there were no cases of caries in any of the GI restorations, as opposed to two cases in the CR group. A high success rate of 95% for CR was reported, with significant differences between the clinical performance of heat-cured HVGI and CR restorations in primary teeth over 3 years. The study also showed that 83% of the heat-cured, HVGI restorations survived for up to 36 months, making them a potential intermediate-lasting restoration for proximal lesions in primary molars.16In the restoration of teeth while under general anesthesia, Pani15 compared the survivability of HVGICs and CR. Despite the type of restoration used, the study's findings revealed that failure occurred in >70% of the anterior teeth within the 1st year. Overall, there was no discernible difference in the survival rates of composite and glass ionomers. Interestingly, survival rates for posterior teeth were nearly identical, while anterior teeth showed an earlier failure for glass ionomers when compared to composites. Given the constrained time available for surgeries under general anesthesia, it might be claimed that HVGIC restorations might be more efficient from a time of placement standpoint. On the contrary, when compared to composites in the anterior teeth, HVGIC restorations were noticeably worse from a structural aspect. It can be claimed that neither material is efficient in the absence of efficient disease management, given the secondary caries rates of both materials were greater than 40%.15However, because there is currently inadequate clinical evidence on this subject, Mickenautsch and Yengopal, in their systematic review on permanent posterior teeth, were unable to support the superiority claims regarding the failure rates of direct hybrid resin composite restorations over those of conventional HVGI restorations.
Limitations of Existing Studies and Future Perspective
Only three trials documented the use of an appropriate randomization technique.13,14,16 Due to the obvious differences in clinical appearance between the compared materials, successful blinding or masking appeared to have been impossible in all trials from the start. Patients and operators could, therefore, see their allocation to either therapy group. Additionally, it was not possible to completely eliminate the risks of heterogeneity between the datasets that were available in terms of the control intervention, the type of restored cavity, the assessment method, and the duration of the follow-up period. There were multiple trials comparing HVGIC to amalgam and resin composite to amalgam restorations; however, there was a lack of trials directly comparing HVGIC to CR restorations. Therefore, large-sized, parallel-group, randomized control trials comparing HVGIC with CR restorations are necessary to support the existing evidence. Future trials of this type should reduce the risk of attrition bias through low loss-to-follow-up, investigate the influence of performance/detection bias on methodology, and test for selection bias risk using the Berger–Exner test to measure the degree of adherence to the assigned random sequence over the course of the trial. A 12-month follow-up period may not be long enough to offer comprehensive information regarding the clinical success rates of restorative materials, making long-term follow-up studies more useful for assessing the long-term clinical success rates of restorative materials. According to this systematic review, both HVGIC and CR restoration show positive outcomes in terms of clinical efficacy and overall survivability. No statistically significant difference between these materials was seen in any of the included studies. For both materials, it was shown that class I restorations had statistically higher survival rates than class II restorations. The research has raised significant concerns about the use of heat-cured glass ionomer as a long-term restorative for proximal lesions in primary molars; therefore, heat-cured HVGI restorations may be thought of as an intermediate-lasting restorative option. It was also discovered that there is no discernible difference in the frequency of secondary caries under either restoration, despite the fact that HVGIC restorations for anterior teeth have inferior structural survivability when compared to resin composites. Longer-term studies are needed to track the therapeutic efficacy of both restorations, though. Any clinically significant judgment must be supported by direct head-to-head comparisons through clinically adequate large-sized parallel group randomized control trials with good internal validity.
Strengths and Limitations
The strict adherence to the 2009 PRISMA statement characterizes the strength of this systematic review.10 In this study, which evaluated the clinical efficacy of HVGIC and CR, only prospective clinical trials were taken into account. The restricted number of database searches and the small amount of published research are the key drawbacks of this systematic review. Due to the wide range of various outcomes measured across the few numbers of existing trials, there was no room for meta-analysis.
Clinical Significance
Why this paper is important to pediatric dentists?
Isolated studies provide contradictory findings regarding the durability of restorations in primary teeth. Therefore, a systematic review of the effectiveness of HVGIC and CR in primary teeth is essential. The population of this systematic review was composed strictly of pediatric patients.
This systematic review outlines the application of HVGIC and CR as restorative materials for pediatric dentists to use in their everyday dental practices.
This study provides pediatric dentists with a comprehensive understanding of HVGIC, CR, atraumatic restorative procedures, and minimally invasive dentistry, all of which are crucial in a pediatric setting.
Orcid
Karthika KK https://orcid.org/0000-0002-6011-7337
Ritesh Kalaskar https://orcid.org/0000-0001-7403-3364
Suyash Joshi https://orcid.org/0000-0002-1976-2676
Footnotes
Source of support: Nil
Conflict of interest: Dr Ritesh Kalaskar is associated as the National Editorial Board member of this journal and this manuscript was subjected to this journal's standard review procedures, with this peer review handled independently of this editorial board member and his research group.
REFERENCES
- 1.Anil S, Anand PS. Early childhood caries: prevalence, risk factors, and prevention. Front Pediatr. 2017;18(5):157. doi: 10.3389/fped.2017.00157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mobley C, Marshall TA, Milgrom P, et al. The contribution of dietary factors to dental caries and disparities in caries. Acad Pediatr. 2009;9(6):410–414. doi: 10.1016/j.acap.2009.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Peres MA, Sheiham A, Liu P, et al. Sugar consumption and changes in dental caries from childhood to adolescence. J Dent Res. 2016;95(4):388–394. doi: 10.1177/0022034515625907. [DOI] [PubMed] [Google Scholar]
- 4.Santamaria RM, Innes NP, Machiulskiene V, et al. Caries management strategies for primary molars: 1-yr randomized control trial results. J Dent Res. 2014;93(11):1062–1069. doi: 10.1177/0022034514550717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Francisconi LF, Scaffa PM, de Barros VR, et al. Glass ionomer cements and their role in the restoration of non-carious cervical lesions. J Appl Oral Sci. 2009;17(5):364–369. doi: 10.1590/s1678-77572009000500003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Frencken JE, Peters MC, Manton DJ, et al. Minimal intervention dentistry for managing dental caries - a review: report of a FDI task group. Int Dent J. 2012;62(5):223–243. doi: 10.1111/idj.12007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chan KH, Mai Y, Kim H, et al. Review: resin composite filling. Materials. 2010;3(2):1228–1243. doi: 10.3390/ma3021228. [DOI] [Google Scholar]
- 8.Hilgert LA, de Amorim RG, Leal SC, et al. Is high-viscosity glass-ionomer-cement a successor to amalgam for treating primary molars? Dent Mater. 2014;30(10):1172–1178. doi: 10.1016/j.dental.2014.07.010. [DOI] [PubMed] [Google Scholar]
- 9.Chisini LA, Collares K, Cademartori MG, et al. Restorations in primary teeth: a systematic review on survival and reasons for failures. Int J Paediatr Dent. 2018;28(2):123–139. doi: 10.1111/ipd.12346. [DOI] [PubMed] [Google Scholar]
- 10.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–e34. doi: 10.1016/j.jclinepi.2009.06.006. [DOI] [PubMed] [Google Scholar]
- 11.Higgins JPT, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomized trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ. 2016;355:i4919. doi: 10.1136/bmj.i4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Akman H, Tosun G. Clinical evaluation of bulk-fill resins and glass ionomer restorative materials: a 1-year follow-up randomized clinical trial in children. Niger J Clin Pract. 2020;23(4):489–497. doi: 10.4103/njcp.njcp_519_19. [DOI] [PubMed] [Google Scholar]
- 14.Ersin NK, Candan U, Aykut A, et al. A clinical evaluation of resin-based composite and glass ionomer cement restorations placed in primary teeth using the ART approach: results at 24 months. J Am Dent Assoc. 2006;137(11):1529–1536. doi: 10.14219/jada.archive.2006.0087. [DOI] [PubMed] [Google Scholar]
- 15.Pani SC. Comparison of high viscosity glass ionomer cement to composite restorations placed in primary teeth under general anesthesia. Pediatr Dent J. 2018;28(3):154–159. doi: 10.1016/j.pdj.2018.08.001. [DOI] [Google Scholar]
- 16.Kupietzky A, Atia Joachim D, Tal E, et al. Long-term clinical performance of heat-cured high-viscosity glass ionomer class II restorations versus resin-based composites in primary molars: a randomized comparison trial. Eur Arch Paediatr Dent. 2019;20(5):451–456. doi: 10.1007/s40368-019-00423-x. [DOI] [PubMed] [Google Scholar]
- 17.Bezerra IM, Brito ACM, de Sousa SA, et al. Glass ionomer cements compared with composite resin in restoration of noncarious cervical lesions: a systematic review and meta-analysis. Heliyon. 2020;6(5):e03969. doi: 10.1016/j.heliyon.2020.e03969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dorri M, Martinez-Zapata MJ, Walsh T, et al. Atraumatic restorative treatment versus conventional restorative treatment for managing dental caries. Cochrane Database Syst Rev. 2017;12(12):CD008072. doi: 10.1002/14651858.CD008072.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Turkun L, Kanik O. A prospective six-year clinical study evaluating reinforced glass ionomer cements with resin coating on posterior teeth: quo vadis? Oper Dent. 2016;41(6):587–598. doi: 10.2341/15-331-C. [DOI] [PubMed] [Google Scholar]
- 20.Mickenautsch S, Yengopal V. Failure rate of direct high-viscosity glass-ionomer versus hybrid resin composite restorations in posterior permanent teeth - a systematic review. Open Dent J. 2015;9:438–448. doi: 10.2174/1874210601509010438. [DOI] [PMC free article] [PubMed] [Google Scholar]