

Abstract
Transthoracic echocardiography and cardiac magnetic resonance imaging revealed a well-defined globular mass attached to the anterolateral papillary muscle. The mass was hyperintense on T1 and T2 weighted images with suppression of signal on fat saturated and short tau inversion recovery (STIR) images. This imaging established the diagnosis of cardiac lipoma attached to the anterolateral papillary muscle, Papillary muscle is a very rare location of lipoma, which is rarely reported in the literature.
Keywords: cardiac, lipoma, papillary muscle
A 72-year-old hypertensive male presented with occasional shortness of breath (New York Heart Association grade II) of 6-month duration. Transthoracic echocardiography (TTE) revealed a well-defined oval echogenic mass of size 11 × 15 mm seen arising from the lateral myocardial wall of the left ventricle (Figure 1). It was moving normally with the myocardium without paroxysmal movements during the cardiac cycle. The left ventricle had normal dimensions and thickness with preserved functions. To characterize the mass further, cardiac magnetic resonance (CMR) imaging was performed, revealing a well-defined globular mass attached to the anterolateral papillary muscle. The mass was hyperintense on T1 and T2 weighted images with suppression of signal on fat saturated and short tau inversion recovery (STIR) images (Figure 1). No evidence of first pass perfusion or late gadolinium enhancement was seen within the mass. A low-dose computed tomography also confirmed fat attenuation of the mass (Figure 2). These imaging features established the diagnosis of cardiac lipoma attached to the anterolateral papillary muscle. Considering the small dimensions of the mass and the absence of hemodynamic compromise or overt symptoms, surgical excision was not considered. The patient is currently on follow-up with periodic clinical and echocardiographic examination. The follow-up echocardiography did not reveal increased dimensions of the mass.
Figure 1.
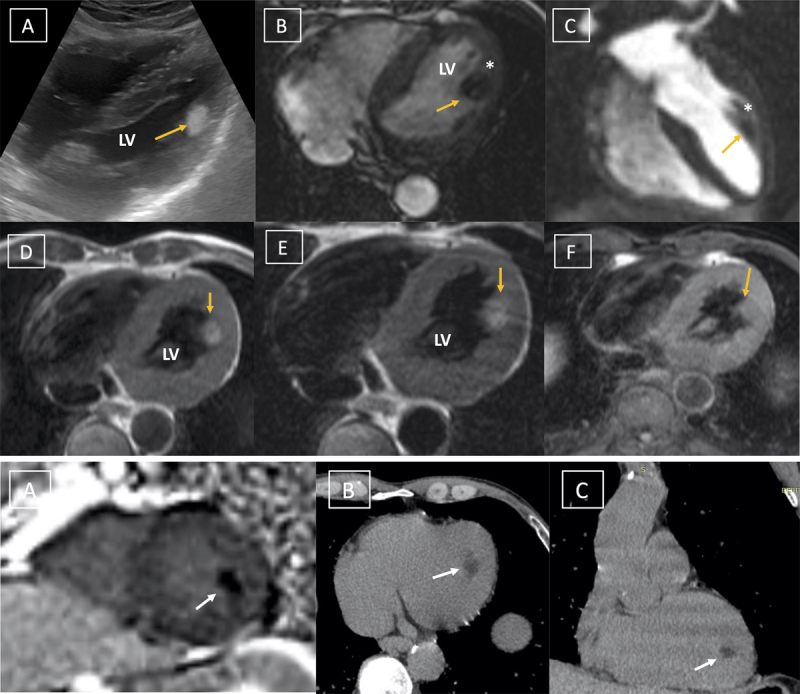
(A) Transthoracic echocardiography reveals echogenic oval mass (depicted with yellow arrow) with regular margins attached to the lateral myocardial wall of the left ventricle. (B) Cine steady state free precession four-chamber image demonstrating oval mass attached to the papillary muscle (white asterisk). (C) Four-chamber image clearly depicting the hypointense mass attached to anterolateral papillary muscle (white asterisk). The mass is hyperintense on (D) T1 and (E) T2 weighted image with suppression on (F) fat saturated sequence suggesting a cardiac lipoma.
Figure 2 (A) Short axis late gadolinium enhanced image demonstrating no enhancement within the mass. (B) Axial and (C) coronal computed tomography image depicts a hypointense mass (white arrow) with fat attenuation suggesting cardiac lipoma.
Primary cardiac tumors are not common. Lipoma is the most common benign tumor after myxoma. Cardiac lipoma can have different locations in the heart with varied clinical presentations. They are usually asymptomatic; occasionally patients can present with palpitations or dyspnea. Rarely, cardiac lipoma may cause arrythmias, hemodynamic abnormalities, and sudden cardiac death due to coronary or valve obstruction.1 Common locations of the occurrence of cardiac lipoma include the epicardial surface of the left ventricle, right atrium, and interventricular septum.1 Papillary muscle is a very rare location of lipoma with few cases reported in the literature.1,2,3 The treatment of choice is surgery with complete excision of the mass. The indications for surgery include presence of symptoms, rapid increase in mass dimensions, and presence of hemodynamic compromise. However, in the absence of overt signs and clinical symptoms, the indications for surgery are less defined, and close follow-up of the patient is recommended.3
Competing Interests
The authors have no competing interests to declare.
References
- 1.Prestipino, F, Cammardella, AG, Chello, M. Unconventional location for a cardiac lipoma: The anterior papillary muscle. J Cardiol Cases. 2016. May 31;14(3):71-73. doi: 10.1016/j.jccase.2016.03.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Koshy, AN, Koshy, G, Hardikar, AA. Intracardiac lipoma arising from the papillary muscle. J Card Surg. 2011. Jan;26(1):65-6. doi: 10.1111/j.1540-8191.2010.01156.x [DOI] [PubMed] [Google Scholar]
- 3.Kim YS, Lee KH, Choi SJ, Baek WK. Cardiac lipoma arising from left ventricular papillary muscle: Resect or not? J Thorac Cardiovasc Surg. 2018. Jul;156(1):244-246. doi: 10.1016/j.jtcvs.2018.01.040 [DOI] [PubMed] [Google Scholar]