

Abstract
Objective
The objective of this study was to explore factors that affect the clearance of imipenem in critically ill patients and to provide a dosing regimen for such patients.
Methods
A prospective open-label study enrolled 51 critically ill patients with sepsis. Patients were between the ages of 18 and 96. Blood samples were collected in duplicate before (0 hour) and at 0.5, 1, 1.5, 2, 3, 4, 6, and 8 hours after imipenem administration. The plasma imipenem concentration was determined by the high-performance liquid chromatography-ultraviolet detection (HPLC-UV) method. A population pharmacokinetic (PPK) model was developed using nonlinear mixed-effects modelling methods to identify covariates. Monte Carlo simulations were performed using the final PPK model to explore the effect of different dosing regimens on the probability of target attainment (PTA).
Results
The imipenem concentration data were best described by a two-compartment model. Creatinine clearance (CrCl, mL/min) was a covariate that affected central clearance (CLc). Patients were divided into four subgroups based on different CrCl rates. Monte Carlo simulations were performed to assess the PTA differences between empirical dosing regimens (0.5 g every 6 hours (q6h), 0.5 g every 8 hours (q8h), 0.5 g every 12 hours (q12h), 1 g every 6 hours (q6h), 1 g every 8 hours (q8h), and 1 g every 12 hours (q12h)) and to determine the target achievement rate covariate.
Conclusion
This study identified covariates for CLc, and the proposed final model can be used to guide clinicians administering imipenem in this particular patient population.
Keywords: clinical medicine; drug monitoring; pharmacy service, hospital; microbiology; medical informatics
WHAT IS ALREADY KNOWN ON THIS TOPIC
The pharmacokinetic characteristics of imipenem in this specific population of critically ill patients can be studied through population pharmacokinetics (PPKs).
WHAT THIS STUDY ADDS
The PPK modelling method described here can be used to explore the pharmacokinetic behaviour of imipenem in critically ill patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings can be used to recommend dosing guidelines when using imipenem in this particular patient population.
Introduction
Imipenem is the most frequently used carbapenem compound in Asia because of its broad antibacterial spectrum and efficacy.1 It plays a huge role in severe infections, such as severe pneumonia, complicated urinary tract infections and intraperitoneal infections.2 However, due to rapidly dynamic physiology, reduced bacterial susceptibility, renal insufficiency and unpredictable pharmacokinetic characteristics, appropriate antibiotic administration remains challenging in critically ill patients.3 The therapeutic drug monitoring (TDM) for β-lactam antibiotics is becoming an increasingly important tool to ensure optimal treatment outcomes in critically ill patients.4
Population pharmacokinetics (PPK) seeks to understand the variability in drug concentrations among individuals in a group of interest (the “population”) receiving clinically relevant doses of a drug. Understanding variability in pharmacokinetics is useful to guide optimal dosing in sub-populations.
Therefore, the pharmacokinetic characteristics of imipenem in this specific population of critically ill patients can be studied through PPK, which can simulate the behaviour of drugs in vivo and identify the influencing factors of drugs in vivo.5 However, there are few studies on the PPK model of imipenem for critically ill patients despite the existence of many established imipenem PPK models in several patient groups.6–9
The purpose of this study was to explore the pharmacokinetic behaviour of imipenem in critically ill patients by using the PPK modelling method. We also explored the effects of different dosing regimens on the probability of target attainment (PTA).
Methods
We conducted a prospective open-label study in which critically ill patients were given imipenem. The plasma imipenem concentration was determined by using the high-performance liquid chromatography-ultraviolet detection (HPLC-UV) method. A PPK model was established to identify covariables using nonlinear mixed-effect modelling. The final PPK model was used to conduct Monte Carlo simulations to explore the effects of different administration regimens on the PTA.
Patient selection
This study was carried out in the intensive care unit (ICU) of Beijing Friendship Hospital, Beijing, China. The inclusion criteria were as follows: (1) ≥18 years old; (2) Patients admitted to the intensive care unit (ICU); (3) Patients met the diagnostic criteria of Sepsis 3.0; and (4) Patients who were treated with imipenem. The exclusion criteria were as follows: (1) Declined informed consent form; (2) Pregnant patient; (3) Estimated survival time is no more than 48 hours.
The study protocol was approved by the Research Ethics Committee of Beijing Friendship Hospital (certificate no. 2018-P2-219-01), and all eligible patients or their legal guardians provided written informed consent.
Drug determination
Administration of the medications
Patients enrolled in this study were treated with imipenem-cilastatin (500 mg/500 mg, Merck Sharp & Dohme Corp, USA) as part of their anti-infection therapy. The dosage regimen was determined by attending physicians according to clinical indications and institutional dosing guidelines. Dosages of imipenem at 0.5 g every 6 hours (q6h), 0.5 g every 8 hours (q8h), and 1 g every 6 hours (q8h) were commonly prescribed. Doses of 0.5 g and 1 g were suspended and transferred to 100 mL of an appropriate infusion solution and then administered by an intravenous infusion pump over 1 hour.
Laboratory analysis
All samples were analysed at least 24 hours after imipenem therapy to obtain plasma imipenem concentrations at or near the steady state. Blood samples were scheduled to be collected in duplicate at 0.5, 1, 1.5, 2, 3, 4, 6, and 8 hour (1 g dose every 8 hour) before and after imipenem administration. Blood samples (0.6 mL) were collected and immediately placed into an icebox and processed within 2 hours. Because imipenem hydrolyzes rapidly in plasma through a pH-dependent reaction, morpholino propanesulfonic acid (MOPS), ultra-pure grade (Amresco, USA) buffer (0.126 M, pH 6.8) served as the stabilising solution. Blood samples were centrifuged (3,000×g, 15 min) and mixed in a 1:1 ratio with the stabilising solution. Finally, the samples were stored at −80°C until analysis.
Analysis of imipenem concentrations in plasma and effluent was based on previously validated high-performance liquid chromatography-ultraviolet detection (HPLC-UV) methods,10–13 with a few modifications. Chromatography was performed on a ZORBAX SB-C8 column (5 µm, 4.6×250 mm; Agilent, USA) maintained at 30°C. The ultraviolet detector was set at 298 nm. A gradient elution of ammonium acetate buffer (0.5 M, pH 6.8), and acetonitrile was used as the mobile phase, with a flow rate of 1 mL/min. Imipenem monohydrate (I1K226, 0.932 mg/mg; USP) was used for the preparation of standard solutions, and ceftazidime was used as the internal standard. Two hundred millilitres of stabilised plasma were mixed with 20 µL of 500 µg/mL of ceftazidime.
The lower limit of quantification (LOQ) was 0.3 µg/mL for plasma samples. The linearity of the standard curve was assessed with 1 /x2 weighting over a concentration range of 0.3 to 200.0 µg/mL. The level of accuracy and precision were evaluated with quality control samples at four different concentrations in triplicate. Stability was assessed by storing stabilised quality control samples at −70°C and 20°C for 30 days and 6 hours, respectively. The stability of patients’ samples stored in the ice box (2–8°C) for 2 hours were also evaluated.
Population pharmacokinetics/validation
Base model
Based on the compartment model, the base model was developed using nonlinear mixed-effects modelling methods. All the pharmacokinetic data (concentration-time data sets) were fitted using Phoenix NLME software (Version 8.0; Certara, St. Louis, MO, USA) with the first-order conditional estimation–least squares (FOCE–ELS) approach. An exponential variability model was selected to describe the inter-individual variability (IIV):
| (1) |
This is where Pi and P represent the ith patient’s individual parameter and the typical value of this parameter, respectively. IIV is assumed to follow a log-normal distribution, and the random variable ηi is normally distributed with a mean of zero and variance of ω2. The additive, proportional and mixed error models were tested in order to define the model that best fits the residual error. Finally, the proportional error model was employed to calculate the residual error of the pharmacokinetic model:
| (2) |
This is where Ci and C represent individual observations in the ith patient’s concentration and the model prediction, respectively. The proportional error was characterised using ε, which is distributed with a mean of zero and variances of σ2. Both one- and multiple- compartment models were attempted to fit the pharmacokinetic data. According to the goodness-of-fit and objective function values (OFV), we selected a two-compartmental open model with zero-order infusion and first-order elimination (Eq. 6) describing the pharmacokinetic data:
| (3 |
| (4) |
| (5) |
| (6) |
This is where XC and XP indicate the imipenem amount in the central and peripheral compartments, respectively. Cc and Cp are the drug concentrations in the central compartment (plasma concentration) and peripheral compartment, respectively. Vc and Vp are respectively the central and peripheral volume. K0 represents the administration rate of imipenem into blood. Q is the clearance between central and peripheral compartments, and CL is the clearance.
Final model
Based on the base model, the impact of candidate covariates on pharmacokinetic parameters was explored. These candidate covariates included: gender (GNDR), age (AGE), body weight (BW), course, creatinine (Cr), creatinine clearance (CrCl), Sequential Organ Failure Assessment (SOFA) score, Acute Physiology and Chronic Health Evaluation (APACHE) score, sepsis, acute kidney injury (AKI), septic shock and ventilation.14 Categorical covariates, such as GNDR, sepsis, AKI, septic shock and ventilation, were incorporated using indicator variables. Other covariates were continuous and were included in the model in the following way:
| (7) |
In this equation COV and COVMedian represent the covariate and the median value of the covariate, respectively. The coefficient f represents the relationship between COV and Pi .
The impact of covariates was evaluated using the forward inclusion-backward elimination method. The covariates were introduced one by one and retained as significant if a decrease in OFV of at least 3.84 units (p<0.05) was observed (forward inclusion). A backward elimination step after covariates were entered into the model during the forward addition step individually eliminated and identified them in the final population pharmacokinetic model if their removal increased the OFV by >6.6 (p<0.01, df=1).
Model evaluation and validation
The descriptive capability of the final population pharmacokinetic model was demonstrated using goodness-of-fit plots, including scatter plots of observations as well as population prediction versus time after dose, observation versus population prediction, and conditional weighted residuals (CWRESs) against population prediction and time, and quantile-quantile (QQ) plots of CWRESs (constructed by Phoenix NLME software).
Furthermore, the predictive capability of the final model was demonstrated by a visual predictive check (VPC). Simulations of 1000 virtual data sets were performed in the final population pharmacokinetic model, and the observations were overlaid on the median and 90% prediction interval (PI) of simulations. The stability of the final model was assessed using the bootstrap technique. A total of 1000 datasets were generated using the resampling method (using Phoenix NLME software). After obtaining the median and SE of the fixed-effect parameters, the population estimates obtained from the final model were compared with the median and 95% CI of the bootstrap replicates.
Simulation
Imipenem activity is considered to be time-dependent; that is, its antimicrobial activity is associated with the fractional time (ƒT) during which the concentration is above the minimal inhibitory concentration (MIC).15 Monte Carlo simulations were carried out using the final PPK model to investigate the influence of dosage regimens and to identify covariates of PTA at a steady state. We studied the following six dosage regimens: 500 and 1000 mg (1 hour intravenous infusion) with administration q6h or q8h and q12h. For each scenario, 1000 virtual patients were simulated to create imipenem concentration-time profiles. The percentages of ƒT>MIC values against MIC distributions (0.0625–32 mg/L) for pathogens commonly treated with imipenem were determined.
Results
Basic information
A total of 51 patients were enrolled, and the characteristics of the patients are summarised in table 1. Among them, 7 patients provided samples at all time points, and 44 patients provided samples at 3–4 time points. A total of 196 blood samples were collected.
Table 1.
Demographic background and clinical characteristics of enrolled patients for modelling
| Characteristics | Number or mean±SD | Median (range) |
| No. Patients | 51 | – |
| No. Observations | 196 | – |
| Observations per patient | 3.84 | – |
| No. Male/Female | 33/18 | – |
| No. AKI | 20 (39.21%) | – |
| No. Hepatic insufficiency | 26 (50.98%) | – |
| No. Sepsis shock | 18 (35.29%) | – |
| No. Ventilation | 26 (50.98%) | – |
| No. Respiratory infection | 27 (52.94%) | – |
| No. Bloodstream infection | 2 (0.04%) | – |
| No. Other infection | 22 (43.14%) | – |
| Course of treatment (d) | 9.35±3.94 | 9 (3-19) |
| Dose (mg) | 519.61±97.05 | 500 (500–1000) |
| Daily dose (mg) | 2032.26±286.80 | 2000 (1500–3000) |
| Age (year) | 56.45±18.76 | 56 (18–96) |
| Body weight (kg) | 70.21±72.01 | 69 (19.6–311.7) |
| Cr (μmol/L) | 94.35±187.94 | 64.8 (32.8–883) |
| CrCl (mL/min) | 104.59±60.95 | 99.34 (17.80–256.22) |
| APACHE II score | 16.67±6.44 | 15 (8–33) |
| SOFA | 6.78±5.06 | 5 (2-19) |
Hepatic insufficiency: Child-Pugh B&C.
Sepsis shock: Compliance with diagnostic criteria of sepsis 3.0.
By measuring the serum creatinine level, the Cockcroft formula was used to calculate the endogenous creatinine clearance (CrCl), CrCl = [(140-age) × weight (kg)] / [0.818×Cr (μmol / L)]. For women, the calculation result × 0.85.
AKI, Acute Kidney Injury, Compliance with Kidney Disease: Improving Global Outcomes (KDIGO) AKI Guideline 2021; APACHE, Acute Physiology and Chronic Health Evaluation; Cr, Serum Creatinine; CrCl, Serum Creatinine Clearance; SOFA, Sequential Organ Failure Assessment.
Drug determination
The plasma analytical method showed a good linearity over the imipenem concentration range. The mean measured concentrations were between 94.26% and 105.05% of the nominal concentration. The within-day variations were between 1.05% and 3.11%, and the day-to-day variations were between 0.64% and 5.16%. All variations of stability were well within the desired limits of 15%.
Population pharmacokinetics
A two-compartment model with first-order absorption and elimination adequately characterises the in vivo behaviour of imipenem. After forward inclusion-backward elimination of all the candidate covariates, CL was markedly influenced by serum creatinine clearance (CrCl), and the OFV decreased from 776.148 to 734.330. The parameter estimates for the final model are listed in table 2, and a good estimation of all the parameters was obtained (relative standard error (RSE) with a range from 2.283% to 5.181%). The final pharmacokinetic model with one covariate (CrCl) is as follows:
Table 2.
The parameter estimates of final population pharmacokinetic model
| Parameter (unit) | Model estimate | Bootstrap results | |||||
| Estimate | RSE% | 95% CI* | Iiv (CV%) | η-shrinkage | Median | 95% CI† | |
| Vc (L) | 16.378 | 2.283 | 15.641 to 17.116 | 89.853 | 0.466 | 16.460 | 5.110 to 32.423 |
| Vp (L) | 10.904 | 3.951 | 10.054 to 11.754 | 8.319 | 0.450 | 12.505 | 8.434 to 73.773 |
| Q (L/h) | 7.645 | 4.086 | 7.029 to 8.261 | 24.453 | 0.249 | 7.539 | 2.919 to 17.858 |
| CL (L/h) | 11.357 | 3.024 | 10.679 to 12.035 | 35.748 | 0.456 | 11.367 | 9.248 to 14.227 |
| fCrCl | 0.473 | 5.181 | 0.425 to 0.521 | to | to | 0.468 | 0.375 to 0.590 |
| Residual error (proportional error, CV%) | |||||||
| CV% | 30.370 | 5.126 | 27.298 to 33.442 | to | to | 30.537 | 23.936 to 38.133 |
fCrCl is the coefficient representing the relationship between CrCl and CL (Eq. 8), and CL increases as CrCl increases. The IIV decreased from 38.562% (base model) to 35.748% (final model).
*The range was calculated by the equation estimate ±1.96 SE.
†2.5th and 97.5th percentile of the ranked bootstrap parameter estimates.
| (8) |
In this equation the CrCl was calculated by mL/min, and 99.896 is the median value of CrCl; and 0.473 is the coefficient representing the relationship between CrCl and CL. CL increases as CrCl increases.
Model evaluation and validation
Goodness-of-fit plots were employed to display the descriptive capability of both the base and final models (figure 1). These plots did not show systematic bias for either the base or final model predictions. Compared with the base model, the final model clearly improved data fitting. The plots of the ETA of CL against covariates (Cr and CrCl) in the base model clearly showed their relationship (figure 2). After the incorporation of the covariate, the relationships disappeared in the final model, indicating that CrCl was appropriately incorporated in the final model.
Figure 1.

The goodness-of-fit plots of basic (left) and final (right) population pharmacokinetic models.
Figure 2.
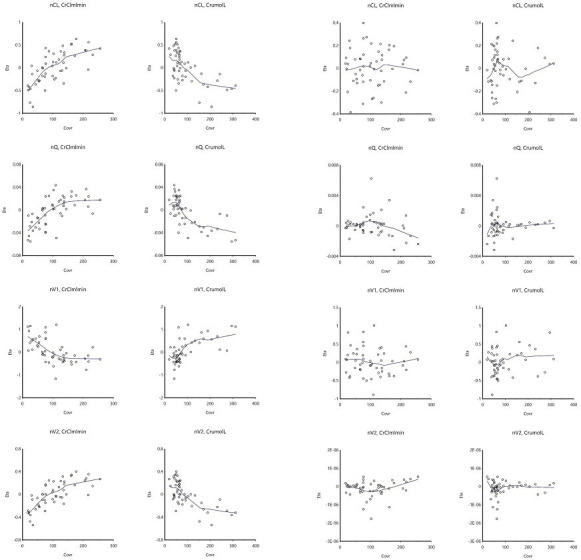
Scatter plots of the ETA of parameters vs Cr or CrCl in the base (left) and final (right) models.
One thousand bootstrap datasets were generated, and the final results are listed in table 2. The median value and its 95% CI of the bootstrap values was similar to the final model parameter estimate, suggesting that the final model was robust. The VPC result is displayed in figure 3, and approximately 90% of the observations were located within the 90% PI, indicating an acceptable prediction ability of the final model.
Figure 3.
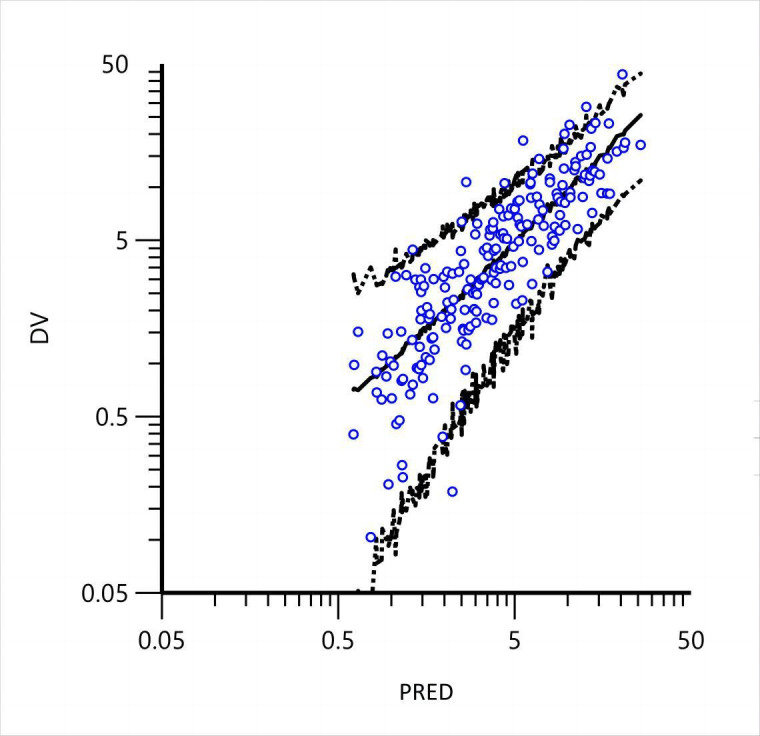
The VPC plots from the final PPK model. DV: dependent value (observation); PRED: prediction. The dots are the original observations. The solid lines represent 50% quantiles from the simulated observations, and the dashed lines represent the 5% and 95% quantiles.
Simulation
The covariate CrCl was incorporated into the final model. Patients were categorised into four subgroups based on different CrCl rates (17.80–30; 30–60; 60–90; 90–256.22 mL/min). The range of CrCl is the key point for the simulation in our patients, and the range of CrCl is from 17.80 to 256.22 mL/min. The predication model can only be used within the range (17.80–256.22 mL/min). We performed Monte Carlo simulations of six dosage regimens in patients with different CrCl rates. The percentage of patients with at least 100% ƒT>MIC against MIC distributions for pathogens commonly treated with imipenem was determined. A PTA of >80% was considered acceptable, and a PTA of >90% was considered desirable. Figure 4 shows the PTA percentages for specific MIC values ranging from 0.0625 to 32 mg/L for each dosage regimen.
Figure 4.

PTA values of different dosage regimens for patients with different CrCl rates.
Discussion
In the present study, we reported the imipenem PPK in 51 critically ill patients using a population approach. Imipenem concentrations were best described by a two-compartment model, and CrCl had a significant effect on CLc.
Compared with previous studies, the results of this study have similarities and differences. For CLc, in our study, the result was 11.357 ± 3.024 L/h, which was in line with the conclusions of Couffignal6 and Sakka8 (13.0 L/h and 12.3 L/h) but differed greatly from the results of Li9 (6.11 L/h). We reason that this is probably because the cases included in Li’s study were not only critically ill patients but also those who were receiving continuous renal replacement therapy (CRRT) treatment. In our study, the Vc result was 16.378 ± 2.283 L, which was between the results of Couffignal6 and Sakka. Slightly lower results than Couffignal’s (22.4 L), possibly because their subjects were heavier than those in our study (77 kg vs 70.21 kg).
During the modelling process, we found that the covariates age (AGE), Cr, CrCl, and BW were related to the individual variation in the parameters (online supplemental figure 1). We therefore analysed the correlations of the covariates (online supplemental figure 2). When CrCl was introduced into CLc, the OFV had the largest decrease (>30), and other covariates had smaller effects than CrCl. This correlation was not visible, indicating that CrCl is a covariate that actually affects CLc (online supplemental figure 1).
ejhpharm-2022-003403supp001.pdf (605.6KB, pdf)
ejhpharm-2022-003403supp002.pdf (253.4KB, pdf)
For β-lactam antibiotics, the pharmacodynamic predictor of clinical efficacy and risk of developing microbial resistance to imipenem are commonly indicated by the percentage of free drug concentrations remaining above the MIC of the pathogen (ƒT>MIC), and a target of at least 40% is recommended.16–19 For critically ill patients, the pharmacodynamic predictor of β-lactams were considered to be 100% ƒT>MIC.20 It was indicated that ƒT>4–5× MIC maximised the likelihood of clinical cure in patients with severe infections,4 21 and a target of at least 60% has been suggested for bolus infusion.20
According to the simulation results, PTA was relatively similar when CrCl >30 mL/h (figure 4B–D). If the MIC=1, to achieve a target of 100% ƒT >MIC or ƒT >4–5 × MIC, we administered a dosage schedule of 0.5 g q6h, 1 g q8h or 1 g q6h. Once CrCl was less than 30 mL/h, the PTA of imipenem changed greatly, and all six simulated dosing regimens achieved the general therapeutic target (figure 4A). We can use the simulation results to select the imipenem dosing regimen for severe patients with different CrCl rates to obtain optimal clinical efficacy and avoid drug resistance. However, if a pathogen with a higher MIC (MIC 4–8 g/mL) is present, a dose of 2 g/d (imipenem) or more may be needed to adequately treat and prevent infection. In addition, Augmented renal clearance (ARC) is another important problem faced by severely ill patients, which leads to significantly reduced effective exposure to antimicrobial agents metabolised via the kidney. To avoid this, there are two approaches: daily measurement of CLCR (as opposed to the use of estimates) so as to accurately identify high-risk patients, and regular TDM.22 Of course, with the regimen potential central nervous system toxicity and other risks should be considered and closely monitored.23
Our study had some limitations. (1) The sample size of this study was small, and additional clinical studies are needed to verify these results. (2) Creatinine clearance was calculated using the Cockroft-Gault equation, which is an imperfect equation for patients with sepsis and can lead to an underestimation or overestimation of GFR. (3) Some data were missing (many covariates had not been measured), affecting the selection of covariates. (4) The universality of the model needs to be verified with external data. 5) Data on the concentration in urine was not available, and material balance and drug accumulation could not be calculated.
Conclusion
Our study determined the plasma imipenem concentration in critically ill patients, and a PPK model was developed. It was concluded that CrCl has a significant effect on CLc. Simulation analysis was also performed to recommend dosing regimens when using imipenem in different CrCl patient populations. Clinicians can use the simulation results to select imipenem administration regimens for different patients to obtain the best clinical efficacy, especially for patients with a high CrCl rate and MIC, which require larger doses or more frequent administration.
Footnotes
JB and AW contributed equally.
XL and MD contributed equally.
Contributors: Guarantor: MD, XL; Conception and design: MD, AW and XL; sample collection and analysis: ZL, AW and JB; Modelling and simulation: XL; Writing the manuscript: JB, XL and ZL.
Funding: This study was funded by Beijing Municipal Natural Science Foundation (No. 7192060).
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
The study protocol was approved by the Research Ethics Committee of Beijing Friendship Hospital (certificate no. 2018-P2-219-01) Participants gave informed consent to participate in the study before taking part.
References
- 1. Hellinger WC, Brewer NS. Carbapenems and monobactams: imipenem, meropenem, and aztreonam. Mayo Clin Proc 1999;74:420–34. 10.4065/74.4.420 [DOI] [PubMed] [Google Scholar]
- 2. Shiber S, Yahav D, Avni T, et al. Β-Lactam/Β-Lactamase inhibitors versus carbapenems for the treatment of sepsis: systematic review and meta-analysis of randomized controlled trials. J Antimicrob Chemother 2015;70:41–7. 10.1093/jac/dku351 [DOI] [PubMed] [Google Scholar]
- 3. Ulldemolins M, Vaquer S, Llauradó-Serra M, et al. Beta-Lactam dosing in critically ill patients with septic shock and continuous renal replacement therapy. Crit Care 2014;18:227. 10.1186/cc13938 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Roberts JA, Hope WW, Lipman J. Therapeutic drug monitoring of beta-lactams for critically ill patients: unwarranted or essential? Int J Antimicrob Agents 2010;35:419–20. 10.1016/j.ijantimicag.2010.01.022 [DOI] [PubMed] [Google Scholar]
- 5. Bellanti F, Della Pasqua O. Modelling and simulation as research tools in paediatric drug development. Eur J Clin Pharmacol 2011;67 Suppl 1:75–86. 10.1007/s00228-010-0974-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Couffignal C, Pajot O, Laouénan C, et al. Population pharmacokinetics of imipenem in critically ill patients with suspected ventilator-associated pneumonia and evaluation of dosage regimens. Br J Clin Pharmacol 2014;78:1022–34. 10.1111/bcp.12435 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. de Velde F, de Winter BCM, Neely MN, et al. Population pharmacokinetics of imipenem in critically ill patients: a parametric and nonparametric model converge on CKD-EPI estimated glomerular filtration rate as an impactful covariate. Clin Pharmacokinet 2020;59:885–98. 10.1007/s40262-020-00859-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sakka SG, Glauner AK, Bulitta JB, et al. Population pharmacokinetics and pharmacodynamics of continuous versus short-term infusion of imipenem-cilastatin in critically ill patients in a randomized, controlled trial. Antimicrob Agents Chemother 2007;51:3304–10. 10.1128/AAC.01318-06 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Li S, Xie F. Population pharmacokinetics and simulations of imipenem in critically ill patients undergoing continuous renal replacement therapy. Int J Antimicrob Agents 2019;53:98–105. 10.1016/j.ijantimicag.2018.10.006 [DOI] [PubMed] [Google Scholar]
- 10. Krausse R, Ullmann U. Determination of imipenem and cilastatin in serum and tissue by high-pressure liquid chromatography. Infection 1986;14:243–5. 10.1007/BF01644271 [DOI] [PubMed] [Google Scholar]
- 11. López KJV, Bertoluci DF, Vicente KM, et al. Simultaneous determination of cefepime, vancomycin and imipenem in human plasma of burn patients by high-performance liquid chromatography. J Chromatogr B Analyt Technol Biomed Life Sci 2007;860:241–5. 10.1016/j.jchromb.2007.10.041 [DOI] [PubMed] [Google Scholar]
- 12. Legrand T, Chhun S, Rey E, et al. Simultaneous determination of three carbapenem antibiotics in plasma by HPLC with ultraviolet detection. J Chromatogr B Analyt Technol Biomed Life Sci 2008;875:551–6. 10.1016/j.jchromb.2008.09.020 [DOI] [PubMed] [Google Scholar]
- 13. Wen A, Li Z, Yu J, et al. Clinical validation of therapeutic drug monitoring of imipenem in spent effluent in critically ill patients receiving continuous renal replacement therapy: a pilot study. PLoS One 2016;11:e0153927. 10.1371/journal.pone.0153927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Li Z, Bai J, Wen A, et al. Pharmacokinetic and pharmacodynamic analysis of critically ill patients undergoing continuous renal replacement therapy with imipenem. Clin Ther 2020;42:1564–77. 10.1016/j.clinthera.2020.06.010 [DOI] [PubMed] [Google Scholar]
- 15. Jaruratanasirikul S, Wongpoowarak W, Jullangkoon M, et al. Population pharmacokinetics and dosing simulations of imipenem in serious bacteraemia in immunocompromised patients with febrile neutropenia. J Pharmacol Sci 2015;127:164–9. 10.1016/j.jphs.2014.12.003 [DOI] [PubMed] [Google Scholar]
- 16. Rodloff AC, Goldstein EJC, Torres A. Two decades of imipenem therapy. J Antimicrob Chemother 2006;58:916–29. 10.1093/jac/dkl354 [DOI] [PubMed] [Google Scholar]
- 17. Sime FB, Roberts MS, Peake SL, et al. Does beta-lactam pharmacokinetic variability in critically ill patients justify therapeutic drug monitoring? A systematic review. Ann Intensive Care 2012;2:35. 10.1186/2110-5820-2-35 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis 1998;26:1–10. 10.1086/516284 [DOI] [PubMed] [Google Scholar]
- 19. Craig WA. Basic pharmacodynamics of antibacterials with clinical applications to the use of beta-lactams, glycopeptides, and linezolid. Infect Dis Clin North Am 2003;17:479–501. 10.1016/s0891-5520(03)00065-5 [DOI] [PubMed] [Google Scholar]
- 20. Sinnollareddy MG, Roberts MS, Lipman J, et al. β-lactam pharmacokinetics and pharmacodynamics in critically ill patients and strategies for dose optimization: a structured review. Clin Exp Pharmacol Physiol 2012;39:489–96. 10.1111/j.1440-1681.2012.05715.x [DOI] [PubMed] [Google Scholar]
- 21. Roberts JA, Norris R, Paterson DL, et al. Therapeutic drug monitoring of antimicrobials. Br J Clin Pharmacol 2012;73:27–36. 10.1111/j.1365-2125.2011.04080.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Baptista JP, Roberts JA, Udy AA. Augmented renal clearance: a real phenomenon with an uncertain cause. Anaesth Crit Care Pain Med 2019;38:335–6. 10.1016/j.accpm.2019.03.002 [DOI] [PubMed] [Google Scholar]
- 23. Fish DN, Teitelbaum I, Abraham E. Pharmacokinetics and pharmacodynamics of imipenem during continuous renal replacement therapy in critically ill patients. Antimicrob Agents Chemother 2005;49:2421–8. 10.1128/AAC.49.6.2421-2428.2005 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
ejhpharm-2022-003403supp001.pdf (605.6KB, pdf)
ejhpharm-2022-003403supp002.pdf (253.4KB, pdf)
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplementary information.