

Abstract
Background
Pediatric patients with eating disorders in a multicenter joint study on 11 facilities were enrolled and prospectively investigated to determine whether improvement in body weight, eating attitudes, and psychosocial factors in children with eating disorders would also improve depressive symptoms.
Methods
In this study, 91 patients were enrolled between April 2014 and March 2016. The severity of underweight was assessed using the body mass index-standard deviation score (BMI-SDS), eating behavior was assessed using the children's eating attitude test (ChEAT26), the outcome of childhood eating disorders was assessed using the childhood eating disorder outcome scale, and depressive symptoms were assessed using the Children's Depression Inventory (CDI) score.
Results
After 12 months of treatment, depressive symptoms were evaluated in 62 of the 91 cases where it was evaluated at the initial phase. There was no difference in background characteristics between the included patients and the 29 patients who dropped out. A paired-sample t-test revealed a significant decrease in CDI scores after 12 months of treatment (p < 0.001, 95% CI: 2.401–7.373) and a significant increase in the BMI-SDS (p < 0.001, 95% CI: − 2.41973–1.45321). Multiple regression analysis revealed that BMI-SDS and ChEAT26 scores at the initial phase were beneficial in CDI recovery. In addition, BMI-SDS at the initial phase was useful for predicting BMI-SDS recovery after 12 months of treatment.
Conclusions
Depressive symptoms in children with eating disorders improved with therapeutic intervention on body weight and eating attitudes.
Trial registration
The Clinical Trial Number for this study is UMIN000055004.
Keywords: Eating disorders, Anorexia nervosa, Body mass index-standard deviation score, Eating attitudes, Children’s depression inventory
Background
Eating disorders are chronic illnesses that develop during childhood and adolescence, and they are syndromes that necessitate physical, psychological, and social support. These disorders have a high comorbidity with psychiatric conditions such as depression, anxiety, attention deficit/hyperactivity disorder, obsessive compulsive disorder, and personality disorders [1]. Depression and anxiety are the most common comorbid symptoms of eating disorders [2–5]. Thus, evaluating psychopathology is important when determining the onset, duration, and prognosis of eating disorders. These disorders are poorly understood and often manifest as hyperactivity despite malnutrition, making it challenging to evaluate depression superficially. According to a systematic review, patients with anorexia nervosa (AN) have a higher rate of depression than the general population [6–8]. It is important to understand depression in patients with eating disorders because long-term depression has been linked to suicide [9, 10]. Previous studies have reported eating disorders and depression in adolescents; however, their existence in younger children (pre-pubertal to adolescent) has rarely been reported. Furthermore, although a systematic scoping review revealed that comorbid depression and eating disorder has a negative impact on weight gain [11], another reports suggested that low body weight due to malnutrition does not affect depression [12]. It is important to understand depression at the onset of childhood eating disorders and evaluate treatment options, but it remains unclear whether treatment improves depressive symptoms in children with eating disorders.
In Japan, the prevalence of eating disorders among junior and senior high school students is ~ 0.5%, which is comparable to that in Western societies [13]. Eating disorder subclassifications differ between children and adults, with AN and avoidance/restrictive food intake disorders (ARFID) accounting for > 50% and 22.5% ~ 25.8% of childhood eating disorders, respectively [14, 15]. In other words, many other eating disorders such as ARFID or unspecified feeding exist in children and differ from AN in terms of age of onset, body weight, eating attitude, and extent of anxiety. In a previous study, individuals with ARFID were younger, reported earlier age of onset, and had higher percent median body mass index (BMI) than those with AN [16]. A retrospective study that categorized different eating disorders including AN and ARFID, among younger individuals found that patients with ARFID had higher rates of comorbidities such as anxiety disorders, separation anxiety disorder, pervasive developmental disorders, attention deficit /hyperactivity disorder, and learning disabilities [12, 17]. However, no prospective studies have been conducted on the depressive course of childhood eating disorders.
This study aimed to evaluate body weight, eating attitudes, psychosocial factors, and depression in children with eating disorders at the initial phase and determine whether depressive symptoms improve prospectively with changes in weight and eating behavior after treatment.
Methods
A prospective cohort study of Japanese children and pre-adolescents with eating disorders
This is a prospective multicenter cohort study (J-PED study) that was established in 2014 to develop a new childhood eating disorder outcome scale. Eleven medical institutions from the north to the south of Japan participated in the study. All J-PED members were trained by a child psychiatrist on how to use the Mini-International Neuropsychiatric Interview [18] to assess comorbid psychiatric disorders.
Enrollment and participants
The registration period lasted two years, from April 2014 to March 2016. Patients with eating disorders under the age of 16 were enrolled, and consent was obtained after the study protocol was explained to the patient and their guardians in the research manual. Eating disorders were diagnosed using the Diagnostic and Statistical Manual of Medical Disorders, Fifth Edition (DSM-5) [19]. Eating disorders are not limited to AN but also include other eating disorders. The study included both untreated first-visit patients and patients referred from other hospitals. Patients who did not provide informed consent to participate in this study were excluded.
The Children's Depression Inventory (CDI) score was obtained from 91 patients with eating disorders at the initial phase. After a 12-month follow-up, 14 patients refused to return to the clinic. Nine patients had missing data. Three patients were referred to psychiatry for suicidal behavior, major depressive symptoms, and other behavioral issues. In addition, three patients had recovered before the 12-month follow-up. Ultimately, 62 patients were able to be evaluated for depression after 12 months (follow-up group; completer), while 29 patients dropped out of enrolment (dropout group) up to 12 months of treatment (Fig. 1). Since the number of dropouts reached up to 30% of the total number of patients at the initial phase, the difference in background characteristics was investigated (Table 1).
Fig. 1.
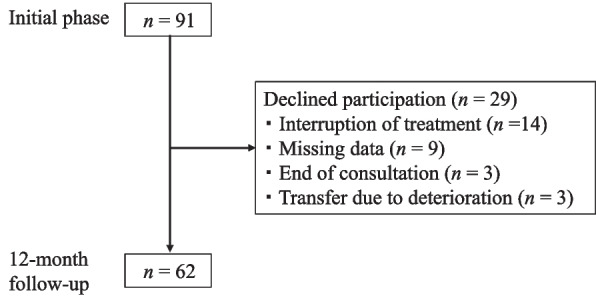
Patient flow diagram for this study
Table 1.
Comparison of background characteristics at the initial visit between patients in12-month-follow-up and dropout groups
| All patients (n = 91) | Follow-up group (n = 62) | Dropout group (n = 29) | P | |
|---|---|---|---|---|
| Age at onset (years) | 12.9 ± 2.1 | 13.0 ± 2.2 | 12.8 ± 2.0 | 1.00 |
| Female (%) | 93.4 | 95.2 | 89.7 | 0.619 |
| BMI (kg/m2) | 13.5 ± 1.6 | 13.5 ± 1.4 | 13.5 ± 2.0 | 1.00 |
| BMI-SDS | − 3.5 ± 1.7 | − 3.5 ± 1.6 | − 3.5 ± 1.9 | 0.981 |
| Free T3(pg/mL) | 1.67 ± 0.84 | 1.63 ± 0.82 | 1.74 ± 0.91 | 0.847 |
| AN, % (n) | 70.3 (64) | 74.2 (46) | 62.1 (18) | 0.503 |
| ASD, % (n) | 12.1 (11) | 12.9 (8) | 10.3 (3) | 0.883 |
| ChEAT26 | 20.7 ± 15.5 | 21.8 ± 15.7 | 18.4 ± 15.1 | 0.729 |
| Outcome scale | 15.7 ± 4.5 | 15.6 ± 4.7 | 16.0 ± 4.1 | 0.923 |
| CDI score (points) | 17.5 ± 8.5 | 17.2 ± 9.0 | 18.2 ± 7.2 | 0.865 |
| Total CDI score above 23/24, % (n) | 24.2 (22) | 22.6 (14) | 27.6 (8) | 0.874 |
Background characteristics at the baseline and 12-month follow-up were compared using independent-sample t-test, whereas chi-squared test was used to compare the groups regarding sex, AN and ASD comorbidities, and CDI positive rate
BMI body mass index, BMI-SDS body mass index standard deviation score, T3 tri-iodothyronine, AN anorexia nervosa, ASD autism spectrum disorder, ChEAT26 Children’s version of the Eating Attitude Test-26 items, outcome scale Childhood eating disorder outcome scale, CDI Children’s Depression Inventory, M ± SD mean ± standard deviation
Study protocol
At the initial phase, age, sex, body mass index-standard deviation score (BMI-SDS), blood test, disease type, neurodevelopmental complications, children's eating attitude test (ChEAT26) score, outcome scale score, and CDI score were obtained. According to the pediatric eating disorder treatment protocol published by the Japanese Society of Psychosomatic Pediatrics [20], they were treated with combined family and individual therapy involving disease education, physical treatment, medical nutrition, medication, supportive psychotherapy, and behavioral therapy according to their needs. Patients were treated as either inpatients or outpatients. Total parenteral nutrition, enteral nutrition via a nasogastric tube, psychotherapy, behavioral therapy, and drug therapy were all recommended, with the attending physician at each institution deciding on the best combinations. Changes in BMI-SD, ChEAT26, outcome scale, and CDI were assessed after 12 months of treatment.
Assessment items
Underweight indicators
In the DSM-5 definition of eating disorders, the BMI is used to designate disease severity as follows: moderate (BMI: 16–16.99 kg/m2), severe (BMI: 15–15.99 kg/m2), and extreme (BMI < 15 kg/m2) [19]. However, BMI is not recommended as a measure of adolescent underweight because development-related variability can bias the results [21, 22]. Therefore, the BMI-SDS [21] standardized by age and sex was used in this study.
ChEAT26
ChEAT26 was standardized to the Japanese version [23], which is the pediatric version of the eating attitude test modified by Garner and Garfinkle [24]. The ChEAT26 consists of 26 items designed to screen for and assess symptoms and characteristics of eating disorders in children and pre-adolescents. It is appropriate for students in the fourth grade of elementary school to the third grade of junior high school (approximately 10 to 15 years old). The cutoff value was set at 18 points (the sensitivity was 69% and the specificity was 93%).
Childhood eating disorder outcome scale
Members of the J-PED study discussed the outcome scale items and, as a result of factor analysis, the core symptoms of eating disorders (eating attitudes (EA), fear of being fat (FF), body image distortion (BD)), and the biopsychosocial factors, which covered items in physical and psychological areas based on environmental factors specific to children (body weight change, menstruation (ME), perception of physical condition, school attendance (SA), disease recognition of school (RS), family functioning (FA), disease recognition by parent (RP), social adaption (SA), and relationships with friends (RF)). After that, an outcome scale was developed by excluding ME, RS, and RP, which had small loadings as a result of factor analysis [25]. The childhood eating disorder outcome scale has total scores ranging from 0 to 36, with 36 being the worst. There was a significant negative correlation between change in the outcome scale score and change in BMI-SDS (r = − 0.562, p < 0.001).
CDI score
The CDI score was used to evaluate depression. It is the standard depression assessment tool in children and adolescents, developed by Kovacs [26]. The Japanese CDI score was standardized by Ozono et al. in 2019 [27]. The CDI's target age ranges from 6 to 17 years. It consists of 27 items that are based on the child's life, such as questions about school and friendships. Each item has three choices, each worth 0 to 2 points (the worst score is 54 points). The CDI consists of five factors (A: negative mood, B: interpersonal problems, C: ineffectiveness, D: anhedonia, and E: negative self-esteem). The total score cutoff for the detection of depression was set at 24 points [27].
Statistical analysis and ethical statement
The Statistical Package for the Social Sciences (SPSS) software, Version 26.0 (IBM SPSS Statistics for Windows, Armonk, NY, USA: IBM Corp.) was used for data analysis. Descriptive analyses were conducted to assess the distribution of the basic clinical and demographic variables among all participants. As the continuous variables in the groups were non-normally distributed, the Wilcoxon signed-rank test and Mann-Whitney U test were used to compare them. However, categorical variables were compared between groups using Fisher's exact test. Finally, the analysis of covariance (ANCOVA) was used to control for potential confounding variables. A paired t-test was used to analyze changes on a continuous scale, while a multiple regression analysis was used to analyze multiple explanatory variables that affect CDI improvement.
The study's design and procedures for obtaining informed consent were approved by the medical ethics committee of Kurume University School of Medicine (approval no. 13211) after applying to the medical review committees of the participating medical institutions.
Results
Comparison of 12-month-follow-up and dropout patients' characteristics at the initial visit (Table 1)
At the initial visit, the participants of 91 children and adolescents aged 7- 15 years. The average age of the 91 patients with eating disorders was 12.9 years (SD: 2.1). The male-to-female ratio was 8:83, with females accounting for 93.4% of the cohort. The average BMI was 13.5 (SD: 1.6), and the average BMI-SDS was − 3.5 (SD: 1.7). The free T3 levels, which reflect nutritional status, were low at 1.67 pg/mL (SD: 0.84). The prevalence of AN was 70.3% (64/91); the other 29.7% (27/91) were cases of ARFID, and the autism spectrum disorder comorbidity diagnosed based on DSM-5 criteria was 12.1% (11/91). The average ChEAT26 score was 20.7 points (SD: 15.5), and the outcome score was 15.7 points (SD: 4.5). The average CDI score was 17.5 points (SD: 8.5), with 24.2% of the cases exceeding the cutoff value (23/24) for Japanese children. Among the 91 patients with eating disorders who had CDI at the initial visit (all patients), 62 patients who had CDI after 12 months of treatment (the follow-up group), and 29 patients who dropped out during the observation period (the dropout group), there were no significant differences in age at the initial visit, male-to-female ratio, BMI, and BMI-SDS, free T3 levels, the prevalence of AN and autism spectrum disorder comorbidity, the ChEAT26 score, the outcome scale score, and the CDI score.
Changes in CDI score, BMI-SDS, ChEAT26 score, and outcome scale from the initial phase to the 12-month follow-up
In 62 patients, the average CDI score was 17.2 points (SD: 9.0) at the initial visit and 12.6 points (SD: 8.3) after 12 months of treatment. A paired t-test revealed that therapeutic intervention significantly reduced the CDI score (p < 0.001, confidence interval (CI): 2.401–7.373; Fig. 2a). In addition, the average BMI-SDS was − 3.5 (SD: 1.6) at the initial visit and − 1.5 (SD: 1.8) after 12 months of treatment, indicating that therapeutic intervention significantly increased BMI-SDS (p < 0.001, CI: − 2.41937– − 1.45321; Fig. 2b). Moreover, the average ChEAT26 score was 21.7 (SD: 15.9) at the initial visit and 8.7 (SD: 9.6) after 12 months of treatment, with the ChEAT26 score decreasing significantly with therapeutic intervention (p < 0.001, CI: 9.284–16.683; Fig. 2c). Furthermore, the average outcome scale scores at the initial visit and after 12 months of treatment were 15.6 (SD: 4.7) and 9.4 (SD: 5.7), respectively, indicating that therapeutic intervention significantly decreased the outcome scale (p < 0.001, CI: 4.472–7.915; Fig. 2d).
Fig. 2.

Changes in assessment items from the initial phase to the 12-month follow-up. a The CDI score was significantly decreased after 12 months of treatment (p < 0.001). b The BMI-SDS was significantly increased after 12 months of treatment (p < 0.001). CDI, Children’s Depression Inventory; BMI-SDS, body mass index-standard deviation score. c The ChEAT26 score was significantly decreased after 12 months of treatment (p < 0.001). d The outcome scale score was significantly increased after 12 months of treatment (p < 0.001). ChEAT26, children’s version of the Eating Attitude Test-26 items
Prognostic factors at the initial visit and their effects on CDI score and BMI-SDS improvement (Tables 2 and 3)
Table 2.
Multiple regression analysis of the effect of prognostic factors on CDI improvement
| Outcome judgment criteria | Prognostic factors | R2 | β | SE | t | P |
|---|---|---|---|---|---|---|
| Differences in CDI score | BMI-SDS | 0.248 | 0.243 | 0.113 | 2.144 | 0.036 |
| ChEAT26 | − 0.429 | 0.113 | − 3.786 | < 0.001 | ||
| Outcome scale | − 0.035 | 0.134 | − 0.262 | 0.795 |
CDI Children’s Depression Inventory, BMI-SDS body mass index standard deviation score, ChEAT26 Children’s version of the Eating Attitude Test-26 items, Outcome scale Childhood eating disorder outcome scale, R2 R Squared, β Beta Coefficient, SE Standard Error, t t-Statistic, P P-Value
Using a model selection procedure, the BMI-SDS and ChEAT26 scores were selected, whereas the outcome scale was excluded. The F value was 10.880, with degrees of freedom (3,58), p < 0.001
Table 3.
Multiple regression analysis of the effect of prognostic factors on BMI-SDS improvement
| Outcome judgment criteria | Prognostic factors | R2 | β | SE | t | P |
|---|---|---|---|---|---|---|
| Differences in BMI-SDS | BMI-SDS | 0.294 | − 0.553 | 0.109 | − 5.094 | < 0.001 |
| ChEAT26 | − 0.105 | 0.124 | − 0.846 | 0.401 | ||
| Outcome score | 0.184 | 0.110 | 1.667 | 0.101 |
BMI-SDS body mass index standard deviation score, ChEAT26 Children’s version of the Eating Attitude Test-26 items, Outcome scale Childhood eating disorder outcome scale, R2 R Squared, β Beta Coefficient, SE Standard Error, t t-Statistic, P P-Value
Using a model selection procedure, the BMI-SDS was selected, whereas ChEAT26 and outcome scores were excluded. The F value was 25.947, with degrees of freedom (3,58), p < 0.001
To identify the factors at the initial visit that influence the prediction of CDI score changes after 12 months of treatment, a multiple regression analysis was performed using each item of the explanatory variables, which were the BMI-SDS as the physical severity score, the ChEAT26 score as the child's eating attitude score, and the outcome scale as the score of eating disorder core symptoms and the biopsychosocial factors. There was a positive correlation with BMI-SDS and a negative correlation with ChEAT26 at the initial visit. On the other hand, to identify the factors at the initial visit that affect the prediction of changes in BMI-SDS, an index of physical improvement, after 12 months of treatment, a multiple regression analysis was performed using each score at the initial visit as an explanatory variable, and only BMI-SDS at the initial visit revealed a negative correlation.
Discussion
In this study, we revealed that children and pre-adolescents with eating disorders showed improvements in CDI scores with therapeutic intervention. Among 91 patients with eating disorders, 22 patients (24.2%) exceeded the depression cutoff value; however, the CDI score significantly decreased after 12 months of treatment (9.7%, n 6/62). In addition, therapeutic intervention promoted weight recovery along with improvement of depressive symptoms. Body weight and ChEAT26 score at the initial visit had an effect on the improvement of depressive symptoms. This suggests that early intervention, before the occurrence of psychophysical deterioration, may enhance outcomes in children and pre-adolescents with eating disorders. Specifically, addressing the factors contributing to nutritional status during the course of treatment may be crucial in improving depression outcomes.
Several studies have shown a link between patient body weight and depression in ED, with both positive and negative results. In a study involving 147 patients with AN, Marzola et al. reported that patients with higher depressive and anxious temperament scores had lower lifetime BMI [28]. Furthermore, in a study including 217 ED patients without comorbidity, 32 with comorbid anxiety, 86 with comorbid depression, and 36 with comorbid anxiety and depression, Hughes et al. reported that ED patients with comorbid depression showed complex and severe presentations in weight/shape concerns [29]. Tanaka et al. investigated the relationship between nutritional status and physical and/or mental status at the initial visit in 45 ED patients aged ≥ 18 years and 39 age-matched healthy controls. They found that depression assessed using the Beck’s Depression Inventory (BDI) correlated with harm avoidance and self-directedness assessed using the Temperament and Character Inventory-125 in both groups, but BMI showed no correlation with TCI-125 subscales in either group [30]. Based on these reports, although there is no direct relationship between BMI and BDI, our study on children and pre-adolescents with eating disorders revealed the importance of weight gain for improvement of depressive symptoms.
In a previous study, we demonstrated a significant negative correlation between the outcome scale and BMI-SDS, and changes in outcome scale scores from baseline to 12 months were significantly associated with improvement in BMI-SDS [25]. To the best of our knowledge, this is the first scale that can statistically analyze outcome measure in children with eating disorders. Three outcomes (EA, FF, and BD) based on DSM-5 AN criteria were included as disease-specific factors [19]. Moreover, psychosocial factors (e.g., FA, RF, and SA), which are often considered for the recovery of children with eating disorders, were included. However, statistical analysis revealed that the outcome score at the initial visit cannot predict both CDI and BMI-SDS improvement. As this study's scale did not include psychiatric disorders such as depression, these disorders may have been excluded from the statistical analysis. On the other hand, some patients used medications. Antidepressants were used in 8 out of 62 cases, and antipsychotics were used in 10 out of 62 cases. There was no significant difference in the change in CDI values 12 months after treatment between the groups that used each drug and those that did not (data not shown).
A systematic review that investigated whether neuropsychological impairments in patients with AN are influenced by BMI, anxiety disorders, or depression revealed that none of these factors were associated with altered central coherence (a tendency to focus on details rather than the overall picture when processing information) and set-shifting (cognitive flexibility, refers to the ability to shift thoughts or actions according to situational demands) in individuals with AN in most studies [31]. In other words, in addition to BMI or depression, there are other factors that contribute to AN pathology. According to a study investigating the relationship between body image perception and symptoms of depression and anxiety during outpatient psychotherapy in 242 women with AN aged 18–56 years, body image perceptions were significantly associated with symptoms of depression and anxiety at all treatment stages [32]. Thus, prevention of persistent body image disturbance in AN may have resulted in the recovery of depression and anxiety with treatment. Based on these studies, it is necessary to recover not only the physical state of AN but also the cognitive distortion to achieve mental and physical recovery. Our study's findings indicated that BMI-SDS and ChEAT26 score were factors affecting CDI recovery at the initial visit, indicating the need for comprehensive support for EA.
Several studies have argued regarding the importance of family function in the recovery process of children with AN [33–38]. In a meta-analysis of 19 randomized controlled trials from 8 different countries on the effects of nonpharmacological interventions on BMI, body dissatisfaction, depression, and anxiety among individuals with AN, behavioral family system therapy was found to improve BMI, while conjoint family therapy was more effective in ameliorating depression [39]. This review demonstrated the impact of multidisciplinary family therapy on physical and psychological recovery. Our study patients were treated at multiple facilities in Japan in accordance with the Japanese Society of Psychosomatic Pediatrics guidelines [20], which are based on expert consensus on the importance of a biopsychosocial approach. Our study treatment involved physical therapy provided by a pediatrician and supportive and/or behavioral therapy centered on family support provided by a multidisciplinary team. The J-PED study revealed that the outcome scale can assess the severity of eating disorders, and changes in this score through therapeutic interventions can reflect improvement in BMI-SDS [25]. In this review, therapeutic interventions led to an improvement of eating disorder pathology, resulting in a decrease in CDI scores.
This study had some limitations. First, one-third of the 91 patients at the initial visit had dropped out during the 12 months leading up to the analysis. The dropout analysis revealed that there were no significant differences in background characteristics of patients among the three groups (91 patients at the initial visit, 62 patients after 12 months of treatment, and 29 patients who dropped out) and that dropout patients had no distinguishing characteristics. Furthermore, while the 12-month follow-up period enabled the evaluation of medium-term outcomes, it may not sufficiently capture long-term recovery and sustainability of treatment effects. Future research should consider extending the follow-up duration to better assess the long-term stability of the therapeutic benefits. It is necessary to examine these dropout cases in the future. Second, despite the presence of psychiatric comorbidities (autism spectrum disorder, depression, and obsessive compulsive disorder) among the study patients were not included as weighting factors in the outcome score. The severity of comorbidities may vary between diseases or patients, and the presence of comorbidities was not included in our outcome scale. Finally, the use of antidepressants and antipsychotics was not subject to specific criteria and was left to the discretion of the attending physician. Because these conditions were not included in the outcome scale, I think this explains why the coefficients of determination (R2) were low. These comorbidities are believed to have a significant negative impact on the prognosis of eating disorders and may be evaluated as prognostic factors in future studies.
Conclusions
In our study, the therapeutic intervention improved CDI score and BMI-SDS after 12 months of treatment. Furthermore, patient body weight and eating attitudes were useful for predicting improvement of depressive symptoms.
Acknowledgements
We would like to thank all participants and their families who participated in the study.
Abbreviations
- AN
Anorexia nervosa
- ARFID
Avoidance/restrictive food intake disorders
- DSM-5
The Diagnostic and Statistical Manual of Medical Disorders, Fifth Edition
- CDI
The Children's Depression Inventory
- BMI-SDS
Body mass index-standard deviation score
- ChEAT26
Children's eating attitude test
- Outcome Scale
Childhood eating disorder outcome scale
- EA
Eating attitudes
- FF
Fear of being fat
- BD
Body image distortion
- ME
Menstruation
- SA
School attendance
- RS
Disease recognition of school
- FA
Family functioning
- RP
Disease recognition by parent
- SA
Social adaption
- RF
Relationships with friends
- SPSS
The Statistical Package for the Social Sciences
Authors’ contributions
All authors reviewed the manuscript, approved it in its current form, and approved the authorship order. All authors (Yuichi Suzuki, Shinichiro Nagamitsu, Takeshi Inoue, Ryoko Otani, Ryoichi Sakuta, Toshiyuki Iguchi, Soh Uchida, Ayumi Okada, Shinji Kikayama, Kenshi Koyanagi, Yuki Suzuki, Yoshino Sumi, Shizuo Takamiya, Chikako Fujii, and Yoshimitsu Fukai) except Nobuoki Eshima collected patient data. Yuichi Suzuki and Shinichiro Nagamitsu compiled the manuscript. Shinichiro Nagamitsu, Yoshimitsu Fukai, and Soh Uchida participated in the design of this study. Nobuoki Eshima conducted the statistical analyses and supervised the preparation of the manuscript.
Authors’ information
Yuichi Suzuki. Lecturer in Pediatrics, Fukushima Medical University; specialist in pediatrics, pediatric neurology, and child mental health; board member of the Japanese Society of Psychosomatic Pediatrics; and a representative of the Eating Disorders Working Group, Japanese Society of Psychosomatic Pediatrics.
Funding
This work was supported by the Ministry of Health, Labour and Welfare under Grant (#H28Sukoyaka-001 and H29Sukoyaka-005 #29040501) provided research materials.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval was granted by the medical ethics committee of Kurume University School of Medicine, reference number 13211. Informed consent was obtained from all individual participants included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article. Informed consent was obtained from the parents or legal guardians of all participants under the age of 16.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Arija Val V, Santi Cano MJ, Novalbos Ruiz JP, Canals J, Rodríguez MA. Characterization, epidemiology and trends of eating disorders. Nutr Hosp. 2022;39(2):8–15. [DOI] [PubMed] [Google Scholar]
- 2.Godart N, Radon L, Curt F, Duclos J, Perdereau F, Lang F, et al. Mood disorders in eating disorder patients: prevalence and chronology of ONSET. J Affect Disord. 2015;185:115–22. 10.1016/j.jad.2015.06.039 [DOI] [PubMed] [Google Scholar]
- 3.Carrot B, Radon L, Hubert T, Vibert S, Duclos J, Curt F, et al. Are lifetime affective disorders predictive of long-term outcome in severe adolescent anorexia nervosa? Eur Child Adolesc Psychiatry. 2017;26:969–78. 10.1007/s00787-017-0963-5 [DOI] [PubMed] [Google Scholar]
- 4.Lloyd EC, Haase AM, Foster CE, Verplanken B. A systematic review of studies probing longitudinal associations between anxiety and anorexia nervosa. Psychiatry Res. 2019;276:175–85. 10.1016/j.psychres.2019.05.010 [DOI] [PubMed] [Google Scholar]
- 5.Pearson CM, Miller J, Ackard DM, Loth KA, Wall MM, Haynos AF, et al. Stability and change in patterns of eating disorder symptoms from adolescence to young adulthood. Int J Eat Disord. 2017;50:748–57. 10.1002/eat.22692 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Berkman ND, Lohr KN, Bulik CM. Outcomes of eating disorders: a systematic review of the literature. Int J Eat Disord. 2007;40:293–309. 10.1002/eat.20369 [DOI] [PubMed] [Google Scholar]
- 7.Miranda-Mendizabal A, Castellví P, Parés-Badell O, Alayo I, Almenara J, Alonso I, et al. Gender differences in suicidal behavior in adolescents and young adults: systematic review and meta-analysis of longitudinal studies. Int J Public Health. 2019;64:265–83. 10.1007/s00038-018-1196-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carretier E, Blanchet C, Moro MR, Lachal J. Comorbid major depressive disorder of anorexia nervosa in adolescence: a scoping review of treatment strategies. Encephale. 2021;47(1):72–8. 10.1016/j.encep.2020.05.017 [DOI] [PubMed] [Google Scholar]
- 9.Amiri S, Khan MA. Prevalence of non-suicidal self-injury, suicidal ideation, suicide attempts, suicide mortality in eating disorders: a systematic review and meta-analysis. Eat Disord. 2023;31(5):487–525. 10.1080/10640266.2023.2196492 [DOI] [PubMed] [Google Scholar]
- 10.Valentine AZ, Hall SS, Sayal K, Hall CL. Waiting-list interventions for children and young people using child and adolescent mental health services: a systematic review. BMJ Ment Health. 2024;27(1):e300844. 10.1136/bmjment-2023-300844 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eskild-Jensen M, Støving RK, Flindt CF, Sjogren M. Comorbid depression as a negative predictor of weight gain during treatment of anorexia nervosa: a systematic scoping review. Eur Eat Disord Rev. 2020;28:605–19. 10.1002/erv.2787 [DOI] [PubMed] [Google Scholar]
- 12.Mattar L, Huas C, Duclos J, Apfel A, Godart N. Relationship between malnutrition and depression or anxiety in anorexia nervosa: a critical review of the literature. J Affect Disord. 2011;132:311–8. 10.1016/j.jad.2010.09.014 [DOI] [PubMed] [Google Scholar]
- 13.Hotta M, Horikawa R, Mabe H, Yokoyama S, Sugiyama E, Yonekawa T, et al. Epidemiology of anorexia nervosa in Japanese adolescents. Biopsychosoc Med. 2015;9:17. 10.1186/s13030-015-0044-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nicely TA, Lane-Loney S, Masciulli E, Hollenbeak CS, Ornstein RM. Prevalence and characteristics of avoidant/restrictive food intake disorder in a cohort of young patients in day treatment for eating disorders. J Eat Disord. 2014;2:21. 10.1186/s40337-014-0021-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Takeshi Inoue, Ryoko Otani, Toshiyuki Iguchi, Ryuta Ishii, Soh Uchida, Ayumi Okada, et al. Prevalence of autism spectrum disorder and autistic traits in children with anorexia nervosa and avoidant/restrictive food intake disorder. Biopsychosoc Med. 2021. PMID: 34001197 [DOI] [PMC free article] [PubMed]
- 16.Becker KR, Keshishian AC, Liebman RE, Coniglio KA, Wang SB, Franko DL, et al. Impact of expanded diagnostic criteria for avoidant/restrictive food intake disorder on clinical comparisons with anorexia nervosa. Int J Eat Disord. 2019;52:230–8. 10.1002/eat.22988 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zanna V, Criscuolo M, Mereu A, Cinelli G, Marchetto C, Pasqualetti P, et al. Restrictive eating disorders in children and adolescents: a comparison between clinical and psychopathological profiles. Eat Weight Disord. 2021;26:1491–501. 10.1007/s40519-020-00962-z [DOI] [PubMed] [Google Scholar]
- 18.Otsubo T, Tanaka K, Koda R, Shinoda J, Sano N, Tanaka S, et al. Reliability and validity of Japanese version of the mini-international neuropsychiatric interview. Psychiatry Clin Neurosci. 2005;59:517–26. 10.1111/j.1440-1819.2005.01408.x [DOI] [PubMed] [Google Scholar]
- 19.American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- 20.Japanese Society of Psychosomatic Pediatrics. Guideline for childhood eating disorders. 2nd ed. Tokyo: Nankoudo (Japanese); 2015.
- 21.Brannsether B, Eide GE, Roelants M, Bjerknes R, Júlíusson PB. BMI and BMI SDS in childhood: annual increments and conditional change. Ann Hum Biol. 2017;44:28–33. 10.3109/03014460.2016.1151933 [DOI] [PubMed] [Google Scholar]
- 22.Freeman RK, Walker MK, Ben-Tovim DI. Low levels of interrater reliability in a standard measure of outcome in eating disorders (the modified Morgan-Russell assessment schedule). Int J Eat Disord. 1996;20:51–6. [DOI] [PubMed] [Google Scholar]
- 23.Chiba H, Nagamitsu S, Sakurai R, Mukai T, Shintou H, Koyanagi K, et al. Children’s eating attitudes test: reliability and validation in Japanese adolescents. Eat Behav. 2016;23:120–5. 10.1016/j.eatbeh.2016.09.001 [DOI] [PubMed] [Google Scholar]
- 24.Garner DM, Garfinkel PE. The eating attitudes test: an index of the symptoms of anorexia nervosa. Psychol Med. 1979;9:273–9. 10.1017/S0033291700030762 [DOI] [PubMed] [Google Scholar]
- 25.Nagamitsu S, Fukai Y, Uchida S, Matsuoka M, Iguchi T, Okada A, et al. Validation of a childhood eating disorder outcome scale. Biopsychosoc Med. 2019;13:21. 10.1186/s13030-019-0162-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kovacs M. Children’s depression inventory CDI manual. North Tonawanda, NY: Multi-Health Systems, Inc; 1992. [Google Scholar]
- 27.Ozono S, Nagamitsu S, Matsuishi T, Yamashita Y, Ogata A, Suzuki S, et al. Reliability and validity of the children’s depression inventory-Japanese version. Pediatr Int. 2019;61:1159–67. 10.1111/ped.13984 [DOI] [PubMed] [Google Scholar]
- 28.Marzola E, Porliod A, Panero M, De-Bacco C, Abbate-Daga G. Affective temperaments and eating psychopathology in anorexia nervosa: which role for anxious and depressive traits? J Affect Disord. 2020;266:374–80. 10.1016/j.jad.2020.01.142 [DOI] [PubMed] [Google Scholar]
- 29.Hughes EK, Goldschmidt AB, Labuschagne Z, Loeb KL, Sawyer SM, Le Grange D. Eating disorders with and without comorbid depression and anxiety: similarities and differences in a clinical sample of children and adolescents. Eur Eat Disord Rev. 2013;21:386–94. 10.1002/erv.2234 [DOI] [PubMed] [Google Scholar]
- 30.Tanaka S, Yoshida K, Katayama H, Kohmura K, Kawano N, Imaeda M, et al. Association of beck depression inventory score and temperament and character Inventory-125 in patients with eating disorders and severe malnutrition. J Eat Disord. 2015;3:36. 10.1186/s40337-015-0077-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fuglset TS. Is set-shifting and central coherence in anorexia nervosa influenced by body mass index, anxiety or depression? A systematic review. BMC Psychiatry. 2021;21:137. 10.1186/s12888-021-03120-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Junne F, Zipfel S, Wild B, Martus P, Giel K, Resmark G, et al. The relationship of body image with symptoms of depression and anxiety in patients with anorexia nervosa during outpatient psychotherapy: results of the ANTOP study. Psychotherapy (Chic). 2016;53:141–51. 10.1037/pst0000064 [DOI] [PubMed] [Google Scholar]
- 33.Balottin L, Mannarini S, Mensi MM, Chiappedi M, Balottin U. Are family relations connected to the quality of the outcome in adolescent anorexia nervosa? An observational study with the Lausanne trilogue Play. Clin Psychol Psychother. 2018;25:785–96. 10.1002/cpp.2314 [DOI] [PubMed] [Google Scholar]
- 34.Duclos J, Dorard G, Cook-Darzens S, Curt F, Faucher S, Berthoz S, et al. Predictive factors for outcome in adolescents with anorexia nervosa: to what extent does parental expressed emotion play a role? PLoS ONE. 2018;13:e0196820. 10.1371/journal.pone.0196820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Holtom-Viesel A, Allan S. A systematic review of the literature on family functioning across all eating disorder diagnoses in comparison to control families. Clin Psychol Rev. 2014;34:29–43. 10.1016/j.cpr.2013.10.005 [DOI] [PubMed] [Google Scholar]
- 36.Moskovich AA, Timko CA, Honeycutt LK, Zucker NL, Merwin RM. Change in expressed emotion and treatment outcome in adolescent anorexia nervosa. Eat Disord. 2017;25:80–91. 10.1080/10640266.2016.1255111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sim LA, Homme JH, Lteif AN, Vande Voort JL, Schak KM, Ellingson J. Family functioning and maternal distress in adolescent girls with anorexia nervosa. Int J Eat Disord. 2009;42:531–9. 10.1002/eat.20654 [DOI] [PubMed] [Google Scholar]
- 38.Steinhausen HC, Gavez S, Winkler MC. Psychosocial correlates, outcome, and stability of abnormal adolescent eating behavior in community samples of young people. Int J Eat Disord. 2005;37:119–26. 10.1002/eat.20077 [DOI] [PubMed] [Google Scholar]
- 39.Gan JKE, Wu VX, Chow G, Chan JKY, Klainin-Yobas P. Effectiveness of non-pharmacological interventions on individuals with anorexia nervosa: a systematic review and meta-analysis. Patient Educ Couns Patient Ed. 2022;105:44–55. 10.1016/j.pec.2021.05.031 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.