

Abstract
Bone deficiency in the posterior maxillary bone can be associated with a large sinus cavity and this dilemma can limit implant placement for dental rehabilitation in this area. The maxillary sinus lifting technique can be the solution for many clinical situations with minimal bone height, allowing the placement of longer implants. Autogenous bone graft is a safe and reliable material for reconstructive surgery. In this article, a case of an elderly male patient with inadequate maxillary bone height is presented. Simultaneous maxillary sinus elevation and implant placement with autogenous parietal bone graft were performed.
Keywords: Bone graft, dental implants, oral rehabilitation, sinus floor elevation
Introduction
The sinus floor elevation technique aims to augment the maxillary sinus in cases where inadequate alveolar bone height hinders clinicians from reconstructing the maxilla with dental implants. The sinus can be lifted in a lateral[1] or crestal approach[2] and earlier reports have shown that sinus floor lifting is a predictable procedure to provide adequate bone height for the insertion of dental implants.[3] Autogenous bone grafts are a safe and reliable material for reconstructive surgery. Among the donor sites used in oral and maxillofacial surgery, the cranium has been favored by many surgeons.[4]
Case Report
A 63-year-old man with a nonsignificant medical history presented with a chief complaint of unsatisfactory conventional treatment with her upper denture, asking if dental implants can be placed for a better quality of life.
Comprehensive clinical and radiological assessments were carried out perioperatively to rule out the presence of sinusitis. No history of systemic or local disease was found to contraindicate sinus or implant surgery. A thorough presurgical plan was prepared with the fabrication of a glass template as a guide for the location and angulation of the intended dental implants.
The linear measurements of the posterior maxillary ridge height at the implant’s site are shown in Table 1.
Table 1.
The maxillary ridge height at the site of implantation
| RR3 (mm) | RR2 (mm) | RR1 (mm) | RL1 (mm) | RL2 (mm) | RL3 (mm) |
|---|---|---|---|---|---|
| 6 | 5 | 8 | 3 | 2 | 8.5 |
RR1: Ridge height at the site of the right first premolar; RR2: Ridge height at the site of the right second premolar; RR3: Ridge height at the site of the right first molar; RL1: Ridge height at the site of the left first premolar; RL2: Ridge height at the site of the left second premolar, RL3: Ridge height at the site of the left first molar
The patient was prepared for the operation under general anesthesia. A crestal incision was made on the alveolar crest that continued into the vestibule through vertical releasing incisions and the flap was carefully elevated and extended labially to expose the bone. The lateral procedure of the maxillary sinus elevation was performed in a standard way and extra care was applied when lifting the sinus membrane. The floor, lateral wall, and posterior wall of the membrane were carefully detached and pushed upward to deliver the needed space for implant placement [Figure 1].
Figure 1.
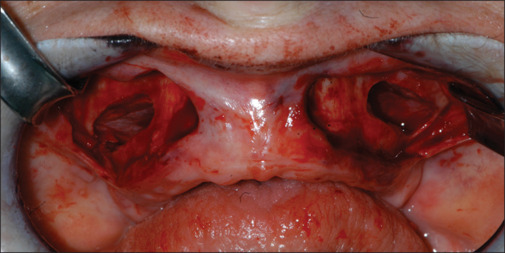
Lifted sinuses on both sides of the maxilla
Two-stage implant system was used where six implants (ITI Straumann, Basel, Switzerland) measuring diameter Ø =4.1 mm and length L = 2 mm × 14 mm and 4 mm × 12 mm were inserted.
A parietal bone graft was harvested according to a standard technique published in full detail in 2011.[4] The skull radiographs were thoroughly assessed to determine the thickness and density of the vault, which is vital to avoid exposure or tearing of the dura. The graft would consist of two major blocks and several bony chips [Figure 2a and b]. The graft’s lamellar bone was then milled using a bone mill (MONDEAL Medical Systems GmbH, Germany) that would produce two bony layers together with granules. Each layer would cover the lifted mucosa on one side. The planned implants were straightforwardly placed before the setting of the grafts. Adequate bone granules were packed on both sides of the maxilla so that the hollow space around the implants was filled with the granules increasing the bone height to more than 15 mm below the lifted mucosa. This was followed by the application of a Bio-Gide membrane. Single and continuous sutures were used for the closure of the intraoral wounds. Pre- and postsurgical radiographs are shown in Figures 3 and 4.
Figure 2.
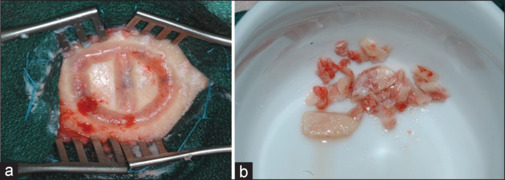
(a and b) The prepared parietal bone and the harvested graft that consisted of two major blocks and several bony chips
Figure 3.

Maxillary sinuses: Presurgery
Figure 4.
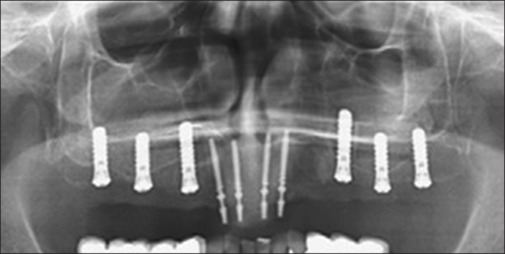
Maxillary sinuses: Postimplant surgery with lifting and grafting
The patient was discharged with full postoperative instructions and needed medications. Follow-up appointments were given before exposure and further prosthetic procedures commenced 9 months after grafting. Transgingival healing abutments were then applied and left for 6 weeks to allow soft tissue to heal [Figure 5]. Later, elastomer material was injected around the impression posts and impression tray after open-tray impression posts were attached to the implants. A bar-retained overdenture was fabricated to support the lips and cheeks and provide fullness and shape to the face [Figure 6].
Figure 5.
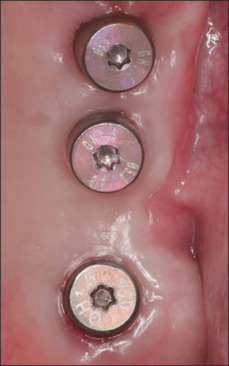
Soft-tissue healing after 6 weeks after implant exposure
Figure 6.

The final overdenture at 1-year follow-up
Discussion
It is very important to preserve the Schneiderian membrane during the sinus floor elevation procedure when determining to perform such surgery.
Dental implants can be placed instantaneously with or without bone grafting after the lateral sinus elevation approach[5] or postponed for several months allowing the grafts to heal.[6]
Studies have shown that the boundary between the new bone and the recipient bed was indiscernible when examining bone specimens several months after sinus grafting with cranial bone.[7] Furthermore, a meta-analysis reported survival rates of approximately 90% from 6 to 60 months for implants in the grafted maxillary sinus.[8] On the other hand, a variety of clinical studies disagree regarding the minimum bone height of the posterior atrophic maxilla needed for sinus elevation with or without sinus grafting.[9,10]
The deficient alveolar ridge in this study was treated by placing immediate implants after sinus lifting and grafting with autogenous parietal bone and the graft’s position under the lifted mucosa ensured a simple uncomplicated placement of implants. The pain was well controlled and minimum doses of opioids were taken. Postoperative nausea was reported because of patient-controlled analgesia. No antiemetics were required.
Neither implant mobility nor peri-implant bone loss was clinically observed on initiation of loading from the prosthetic components from 9 months after surgery to a minimum of a 1-year follow-up.
Simultaneous augmentation after sinus floor elevation can be a difficult procedure needing a large volume of bone, especially bilateral augmentation. Mobilizing adequate soft tissues to cover the whole grafted area can be a challenge that the surgeon must primarily consider and understanding the local anatomy is essential for expected excellent results in this type of surgery.
Conclusion
This presented case suggests that the reconstruction of the sinus floor and the resorbed alveolar ridge using an autogenous parietal bone graft are reliable giving the surgeon the ability to immediately place implants in patients with deficient maxillary alveolar bone height.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The author would like to thank Prince Sattam Bin Abdulaziz University and the Deanship of Scientific Research for their continuous support.
References
- 1.Tatum H., Jr Maxillary and sinus implant reconstructions. Dent Clin North Am. 1986;30:207–29. [PubMed] [Google Scholar]
- 2.Draenert GF, Eisenmenger W. A new technique for the transcrestal sinus floor elevation and alveolar ridge augmentation with press-fit bone cylinders: A technical note. J Craniomaxillofac Surg. 2007;35:201–6. doi: 10.1016/j.jcms.2007.02.005. [DOI] [PubMed] [Google Scholar]
- 3.Chiapasco M, Ronchi P. Sinus lift and endosseous implants – Preliminary surgical and prosthetic results. Eur J Prosthodont Restor Dent. 1994;3:15–21. [PubMed] [Google Scholar]
- 4.Sakka S, Krenkel C. Simultaneous maxillary sinus lifting and implant placement with autogenous parietal bone graft: Outcome of 17 cases. J Craniomaxillofac Surg. 2011;39:187–91. doi: 10.1016/j.jcms.2010.04.007. [DOI] [PubMed] [Google Scholar]
- 5.Ferrigno N, Laureti M, Fanali S. Dental implants placement in conjunction with osteotome sinus floor elevation: A 12-year life-table analysis from a prospective study on 588 ITI implants. Clin Oral Implants Res. 2006;17:194–205. doi: 10.1111/j.1600-0501.2005.01192.x. [DOI] [PubMed] [Google Scholar]
- 6.Fugazzotto PA. Maxillary sinus grafting with and without simultaneous implant placement: Technical considerations and case reports. Int J Periodontics Restorative Dent. 1994;14:544–51. [PubMed] [Google Scholar]
- 7.Le Lorc’h-Bukiet I, Tulasne JF, Llorens A, Lesclous P. Parietal bone as graft material for maxillary sinus floor elevation: Structure and remodeling of the donor and of recipient sites. Clin Oral Implants Res. 2005;16:244–9. doi: 10.1111/j.1600-0501.2004.01102.x. [DOI] [PubMed] [Google Scholar]
- 8.Tong DC, Rioux K, Drangsholt M, Beirne OR. A review of survival rates for implants placed in grafted maxillary sinuses using meta-analysis. Int J Oral Maxillofac Implants. 1998;13:175–82. [PubMed] [Google Scholar]
- 9.Chen TW, Chang HS, Leung KW, Lai YL, Kao SY. Implant placement immediately after the lateral approach of the trap door window procedure to create a maxillary sinus lift without bone grafting: A 2-year retrospective evaluation of 47 implants in 33 patients. J Oral Maxillofac Surg. 2007;65:2324–8. doi: 10.1016/j.joms.2007.06.649. [DOI] [PubMed] [Google Scholar]
- 10.Sbordone L, Levin L, Guidetti F, Sbordone C, Glikman A, Schwartz-Arad D. Apical and marginal bone alterations around implants in maxillary sinus augmentation grafted with autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. Clin Oral Implants Res. 2011;22:485–91. doi: 10.1111/j.1600-0501.2010.02030.x. [DOI] [PubMed] [Google Scholar]