

Abstract
Introduction
A rectal impalement injury is a rare type of penetrating injury that involves a solid object being forcefully inserted through anal opening. The removal of such injuries should be planned carefully with preparedness to assess and manage associated injuries in the pelvis and peri-anal region.
Case description
An elderly female, around 65 years old, had a history of accidental penetration of an iron rod into her anal orifice. The patient was hemodynamically stable, and the distal end of the penetrated rod was visible in the anal verge on arrival. On evaluation, we found that the object had perforated the posterior wall of the middle 1/3rd of the rectum and had traversed retroperitoneally, bypassing all major vessels and viscera.
Discussion
We performed exploratory laparotomy, and the iron rod was extracted from the anal canal under vision, and a diversion colostomy of the sigmoid colon was performed. The patient had an uneventful recovery, and the reversal of the sigmoid colostomy was done after 3 months.
Conclusion
Rectal impalement injuries are rare and serious. It requires a multidisciplinary approach involving a general surgeon, a vascular surgeon, and a urologist since it is associated with a higher incidence of involving major pelvic organs and vessels. In our case, the penetrating object had bypassed all major vessels, which is a rare occurrence.
Keywords: Impalement injury, Rectal perforation, Trans-anal impalement, Rare presentation, Case report
Highlights
-
•
Rectal impalement injuries are rare and often fatal
-
•
In this case the impaling object had traversed most of its length into the patient’s body bypassing ureter and iliac vessels
-
•
Perianal impalement injuries should be managed with multidisciplinary approach in a tertiary centre
-
•
A diversion must be considered in case of bowel injury when associated with high risk factors
1. Introduction
Rectal impalement injuries are rare and usually associated with accidental falls as well as part of sexual assault or extreme method of torture. It involves entry of a foreign body into the rectum externally through perianal region which results in intra peritoneal or extra peritoneal injury of rectum. The management of such kind of injuries involves major challenges including pre- hospital care, transportation of patient in a safe position with least manipulation of the impaled object and specific surgical approach. Massive penetrating injuries through rectum are complicated and potentially fatal requires multi-disciplinary approach [1]. The treating surgeon must always be prepared to check the nearby structures such as genitourinary organs, major pelvic vessels and other vital structures for associated injuries.
We report one of such case where an elderly woman presented to emergency room with a long iron rod being impaled into her anal canal accidentally. The uniqueness of this case was, despite of the length and the uneven surface of the foreign body the patient narrowly escaped all major vessels and organs, had an uneventful recovery.
2. Case description
This case report has been described corresponding to the SCARE criteria [2]. An elderly female of age around 65 yrs., presented to our emergency room with history of accidental penetration of foreign object into her anal canal which occurred at her home. She reportedly slipped and sat on a projecting iron rod in the field while grazing her cow in the early morning. She received first aid at a local hospital and was shifted to our centre in supine position without disengaging or manipulation of the rod after 2 hours of injury. She was a known hypertensive and had undergone abdominal hysterectomy 10 years ago for fibroid uterus.
On admission patient was conscious, oriented, spontaneously breathing and was hemodynamically stable. Her chief complaints were pain in the abdomen and peri-anal region. On examination abdomen was rigid and tenderness noted in left lumbar and left iliac fossa. The last 10 cm of the iron rod with diameter of 2 cm was visible coming out of her anal orifice (Fig. 1). No injury to external genitalia was present. No other abdominal injuries were noted. A Foley's catheter was inserted, and urine was found clear. Tetanus toxoid injection was given. After primary and secondary survey, assuring her stability she was shifted for CT scan of thorax and abdomen without any manipulation of the impaled object.
Fig. 1.

Clinical picture.
Shows impaling object penetrating the anal orifice, Foleys catheter in-situ.
The CT scan revealed a linear metallic foreign body coursing through the anal canal superiorly through the rectum into the left lumbar region with rectal perforation with the tip lying at the level of L1 vertebra at the under surface of the left kidney. The rod had bypassed the left common iliac vessels and left ureter and found lying posterior to them. The scan showed no evidence of pneumo-peritoneum or pelvic collection (Fig. 2, Fig. 3, Fig. 4).
Fig. 2.

Abdominal CT scan.
Showing image of abdominal CT scan with metallic foreign body.
Fig. 3.

Abdominal CT scan with reconstruction.
Abdominal CT image with reconstruction showing course of metallic foreign body bypassing ureter.
Fig. 4.

Abdominal CT with reconstruction.
Abdominal CT image with reconstruction showing course of metallic foreign body bypassing left iliac vessels.
3. Therapeutic intervention
Emergency midline laparotomy performed under general anaesthesia. The iron rod was found entering the anal canal and perforated the posterior wall of middle 1/3 rd. of the rectum. It had entered the retroperitoneum by piercing the left psoas muscle passing posterior to the left iliac and left ureter. The impaled object travelled all the way through her abdomen yet did not shear any major vessel. The proximal end of the rod was found in the retroperitoneum in left lumbar region near lower pole of left kidney. Abdomen was explored to look for injuries to other parts of large and small bowel, bladder, left ureter, left kidney and spleen. After assessing thoroughly for all the injuries, we opened the retroperitoneum and visualised the proximal end of the rod (Fig. 5).
Fig. 5.
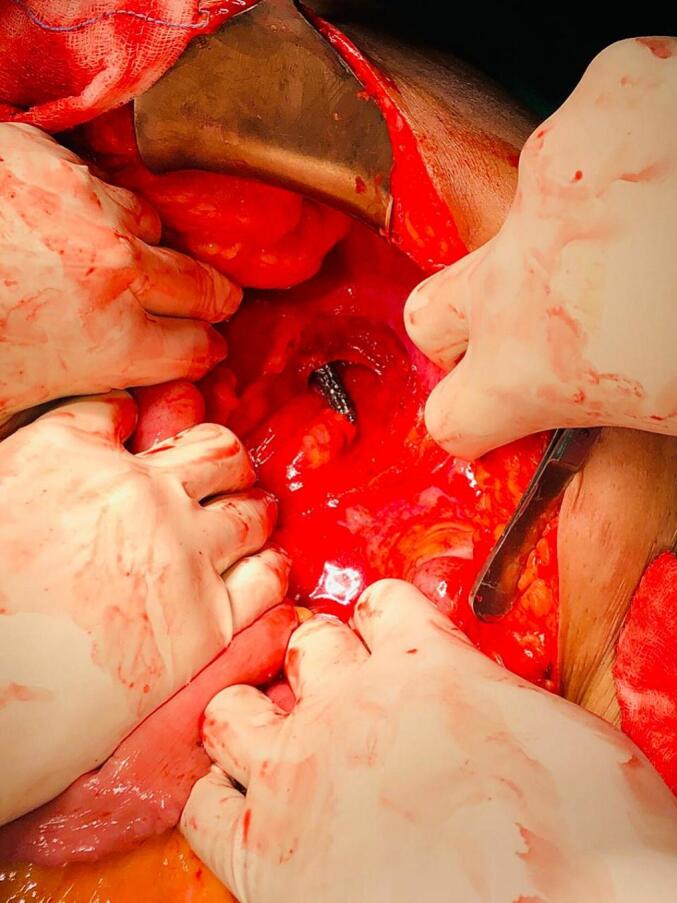
Tip of the iron rod in the retro peritoneum.
Showing upper end of metallic foreign body in the retroperitoneum, lower pole of left kidney.
The rod was lubricated for easy sliding and the distal segment of the rod projecting out of anal canal was pulled out under vision along the track it had entered. The overall length of the rod was 50 cm (Fig. 6). Culture swab was not taken from the iron rod.
Fig. 6.

Full length of the iron rod.
Impaling foreign body after extraction.
There was no hemo-peritoneum. Thorough rectal wash was given, and repair of the perforation was done after mobilisation. Distal end of sigmoid colon was brought out as diversion colostomy to avoid risk of anastomotic leak considering the patients age and contamination. Drain was placed and abdomen was closed. The entire operative time was 2 h which involved two senior general surgeons, one senior resident and one junior resident.
4. Follow up and outcome
Post operatively patient was managed with broad spectrum IV antibiotics (Inj. Meropenem 1 g IV) for 7 days and physiotherapy. She was mobilised on post op day 1, and oral intake was initiated on post op day 2. Drain was removed on post op day 5. The stoma was functional, and midline wound healed well. She was discharged on day 10 and was on regular monthly follow-up. After 3 months sigmoidoscopy was performed to make sure that the repair done on rectum had healed completely before reversal. Anal continence was check clinically and colostomy reversal was done.
5. Discussion
Impalement injuries are a type of penetrating trauma caused when a long solid object enters the body through anatomical orifices and remains inside the body. In the history many examples of impalement injuries have been documented and to name the most famous method of torture used by the military governor, or prince of Walachia (present day Romania) Vlad Basarab, nickname Dracula the Impaler [3]. The method was used by him was to prolong the duration of suffering of the victim by inserting elongated solid objects through the natural orifices in the very precise direction so that the death doesn't happen quickly. In the recent times the most reported cases are associated with accidental injuries by falling on the objects, sexual related activity or associated with psychiatric conducts where cases were presented with rectal perforation [4]. In our case the mode of injury was an accidental fall on a projecting iron rod, which had penetrated her body through anal orifice.
The impalement injuries are known for through and through kind of penetration. They are frequently involved with multiple organ injury depending on the entry site, the direction and the nature of the penetrating object [5]. Impalement injuries involving rectum usually are due to stab or gunshot injury and as a part of collision during accident but less commonly from trans anal penetration [6]. Challenges associated with anorectal impalement injuries include delay in seeking medical attention, hiding the history in case of sexual activity or when there is suspicion of child abuse. In such cases a detailed history and a careful examination is necessary [7].
While examining the patient if the penetrating object is not visible or associated with an unclear history, a differential diagnosis of hidden object inside body must always kept in mind. Many of the times the patient may disengage the object from the site of injury by himself and present to hospital. In such cases the extent of the injury may get missed at the time of initial assessment or the patient may conceal the actual injury history from the treating surgeon. In such cases the treatment may get delayed and hidden object may get revealed after detailed examination and investigations [5,8]. Evaluation of penetrating injury must include a thorough examination along with imaging techniques to rule out combined thoraco-abdominal injuries. Special attention must be paid since the diaphragmatic injuries quite common with penetration injuries and may get missed out [9,10].
X ray is a good imaging modality when the impaling object is metallic but not helpful in finding the extent of organ injury also not useful when the object is radio lucent. CT abdomen is the investigation of choice since all the details of injury can be interpreted with added advantage of CECT with Angiogram when vascular injury is suspected. MRI is not a preferred mode of imaging since most of the implement injuries are associated with metal-based objects.
There have been few reported cases of impalement injuries where the traversing objecting did not cause major abdominal and vessel injury such as transpelvic and transabdominal impalement injury. This was due to the trajectory of the impaling object and the direction of the entry of the object [[11], [12], [13]].
The uniform agreement about managing such injuries is that the piercing object must be kept in-situ and manipulation must be avoided. Extraction should be done in the operation theatre under the guidance of experienced surgeons and always under vision. Multidisciplinary surgical approach involving trauma surgeon, vascular and thoracic surgeons are necessary for effective management when complex thoraco-abdominal injuries are suspected [13,14]. In situations where complex thoraco-abdominal injuries are suspected, the chances of multi-organ injuries especially cardiac and major vessel injuries are quite common. Hence a thoracotomy with exploratory laparotomy should be planned for wide exposure [13].
Our case was unique due to peculiarity of the mode of injury, the object perforated the rectum and directly entered the retroperitoneum, due to which all the major viscera and vascular structures were unharmed. Although the iron rod was rusted, covered with mud and cow dung, we were able to manage with antibiotic coverage as well as immunisation with tetanus toxoid due to which patient did not have any signs of sepsis post operatively including tetanus or clostridia infection.
6. Conclusion
Rectal impalement is uncommon, and it is crucially important for the treating surgeon to identify associated injuries. Management in tertiary centre with suitable intensive care, early diagnostics and appropriate surgical interventions by multidisciplinary team play a very important role to maximise recovery and minimise mortality.
6.1. Patient perspective
I usually wake up at around 6 am and take my cows for grazing every day. We have a wide field near our house, and we plant these iron rods on the ground to support the creepers. That day when I went out, it was still dark and raining. I took my cow out for grazing, and I had wrapped the rope around my wrist. I don't know why that cow got agitated and it started pulling me with force. Me being an old lady, I lost my balance and sat on my buttocks right on top of one of those rods. It happened all of sudden, and It didn't give me time to realise. I was in a lot of pain, and I started screaming. I slowly got up by myself, but I couldn't walk. My family heard my screams, and they came running. They couldn't believe what had happened. All were in shock and confused. Later my neighbour came with his vehicle and took me to our nearby hospital. There the duty doctor saw me and gave me a pain killer and one antibiotic injection. He told us not to touch the rod and immediately arranged an ambulance to transport me to this hospital.
In this hospital they took me for scan immediately and shifted me for operation. Doctors came and spoke to me before surgery and explained to my family as well. I was very scared when they said I need an immediate major surgery to remove that rod and they told me that I may have a stoma. I was very shocked and disturbed when they said that my faecal matter will come out through my tummy. Once they explained to me that it will be a temporary thing to save my life and made me realise that the operation was necessary.
After surgery I was having a bit of pain and nausea, but it got better. They made me walk on the next day, and slowly I could drink water and eat small portions. They taught me how to take care of my stoma area. I went home after 10 days. I came for admission again after 3 months. After the reversal surgery now, I feel much better. I am grateful to all the doctors and nurses who took such good care of me.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Declaration
This study was performed in accordance with the ethical standards of the institution and the research committee complying with the 1964 Helsinki declaration and its later amendments.
Ethical Approval – Ethical approval was received from the Institutional Ethics Committee of Kasturba Medical College, Mangalore (Reg. no. ECR/541/Inst/KA/2014/RR-17).
Ethical approval
Ethical approval was received from the Institutional Ethics Committee.
Funding
None.
Author contribution
Dr. Deepika CA: Data collection, data analysis or interpretation, study concept, writing the paper.
Dr. Manohar Pai: Reviewing and Editing the article, Surgical operation
Dr. Jagadish Rao P.P: Reviewing and Editing the article, Study concept
Dr. Alfred J Augustine: Study concept, writing, reviewing and Editing the article, Surgical operation
Guarantor
Dr. Alfred J Augustine.
Research registration
N/A.
Conflict of interest statement
None.
Contributor Information
Deepika C.A., Email: drdeepikanayaka.ca@gmail.com.
Manohar V. Pai, Email: mv.pai@manipal.edu.
Jagadish Rao P.P., Email: ppj.rao@manipal.edu.
Alfred J Augustine, Email: alfred_augustine@aimsrchittoor.edu.in.
References
- 1.Rectal impalement injury: from cruelty to salvage endeavour - PubMed. [cited 2022 Jul 6]; Available from: https://pubmed.ncbi.nlm.nih.gov/25800318. [PubMed]
- 2.Sohrabi C., Mathew G., Maria N., Kerwan A., Franchi T., Agha R.A. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. Lond. Engl. 2023;109(5):1136. doi: 10.1097/JS9.0000000000000373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dracula: A Biography of Vlad the Impaler 1431–1476 by Radu R. Florescu [Internet]. [cited 2022 Jul 6]. Available from: https://www.goodreads.com/book/show/532989. Dracula.
- 4.Witz M., Shpitz B., Zager M., Eliashiv A., Dinbar A. Anal erotic instrumentation. Dis. Colon Rectum 1984 275 [Internet] May 1984;27(5):331–332. doi: 10.1007/BF02555649. https://link.springer.com/article/10.1007/BF02555649 Available from: (cited 2022 Jul 6) [DOI] [PubMed] [Google Scholar]
- 5.Kasapas K., Daskalaki A., Kaimasidis G., Chalkiadakis G. Successful management of a combined abdominal and thoracic trauma with rectal impalement: report of a case. Case Rep. Surg. [Internet] 2013;2013:1–3. doi: 10.1155/2013/816089. https://pubmed.ncbi.nlm.nih.gov/23844309/ Available from: (cited 2022 Jul 6) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.The Injured Colon: Annals of Surgery [Internet]. [cited 2022 Jul 6]. Available from: https://journals.lww.com/annalsofsurgery/citation/1986/06000/the_injured_colon.16.aspx.
- 7.Jona J.Z. Accidental anorectal impalement in children. Pediatr. Emerg. Care [Internet] 1997;13(1):40–43. doi: 10.1097/00006565-199702000-00013. https://pubmed.ncbi.nlm.nih.gov/9061736/ Available from: (cited 2022 Jul 6) [DOI] [PubMed] [Google Scholar]
- 8.Deen S., Manek R., Mittal A., Garg K.M. Rectal impalement with bladder perforation: an unusual injury. IOSR J. Dent. Med. Sci. e-ISSN [Internet] 2015;14(3):77–79. www.iosrjournals.org Available from: (cited 2022 Jul 6) [Google Scholar]
- 9.Lear G.H., De K.R., Birt S.J. Impalement injury by a tree branch from rectum to right nipple. Injury [Internet] 1981;12(6):495–498. doi: 10.1016/0020-1383(81)90172-8. https://pubmed.ncbi.nlm.nih.gov/7275296/ Available from: (cited 2022 Jul 6) [DOI] [PubMed] [Google Scholar]
- 10.Prognostic factors and outcome of traumatic diaphragmatic rupture - PubMed [Internet]. [cited 2022 Jul 6]. Available from: https://pubmed.ncbi.nlm.nih.gov/20517745/.
- 11.Alani M., Mahmood S., El-Menyar A., Atique S., Al-Thani H., Peralta R. An unusual case of transpelvic impalement injury: a case-report. Int. J. Surg. Case Rep. 2017;41:26–29. doi: 10.1016/j.ijscr.2017.08.068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abdullahi A., Salahi R., Foroutan A., Banani S.A., Abbasi H.R., Paydar S., et al. Nonfatal perineal impalement injury traversing pelvic, abdominal, and thoracic cavities. Am. Surg. [Internet] Nov 2011;77(11) https://pubmed.ncbi.nlm.nih.gov/22196633/ Available from: (cited 2022 Jul 6) [PubMed] [Google Scholar]
- 13.Mohan R., Ram D.U., Baba Y.S., Shetty A., Bhandary S. Transabdominal impalement: absence of visceral or vascular injury a rare possibility. J. Emerg. Med. [Internet] Nov 2011;41(5):495–498. doi: 10.1016/j.jemermed.2008.03.033. https://pubmed.ncbi.nlm.nih.gov/18829207/ Available from: (cited 2022 Jul 6) [DOI] [PubMed] [Google Scholar]
- 14.Sawhney C., D’souza N., Mishra B., Gupta B., Das S. Management of a massive thoracoabdominal impalement: a case report. Scand. J. Trauma Resusc. Emerg. Med. [Internet] Oct 7, 2009;17(1) doi: 10.1186/1757-7241-17-50. https://pubmed.ncbi.nlm.nih.gov/19811644/ Available from: (cited 2022 Jul 6) [DOI] [PMC free article] [PubMed] [Google Scholar]