

ABSTRACT
Introduction:
Various tools for measuring health literacy are designed to assess reading comprehension and numeracy in English speakers. There is a need to develop a tool in the vernacular language and estimate health literacy levels in Indian settings. The present study was conducted with the objectives to develop a Marathi version of a 14-item health literacy scale (HLS-14) to test the reliability and validity of its Marathi version and to estimate the health literacy among patients attending the out-patient department at a tertiary care centre.
Methodology:
The present study was conducted among 50 adult patients attending the out-patient department of a tertiary hospital from July 2022 to December 2022. The 14-Item Health Literacy Scale available in English was translated into Marathi and back-translated to English, and the final version was developed. Bilingual study subjects were asked to fill the scales on day 0 and on day 7. Cronbach’s alpha was calculated for internal validity, and the correlation coefficient was calculated for the reliability of the tool and health literacy was estimated.
Results:
When items of the Health Literacy Scale were analysed, all the items barring 2, 6, and 10 gave an r-value of more than 0.70, which shows good reliability of each translated item. The Cronbach’s alpha value found for the current translated Marathi questionnaire is 0.66. Internal consistency is good. The mean total health literacy score was 51.16 ± 6.81.
Conclusions:
A translated Marathi version of HLS-14 is developed, which is valid and reliable. The health literacy among the study participants is marginal.
Keywords: Health literacy scale, Marathi, translation, validity
Introduction
Health literacy (HL) refers, broadly, to the ability of individuals to “gain access to, understand and use information in ways which promote and maintain good health for themselves, their families and their communities.”[1]
Health literacy skills are not limited to compliance with the drug treatment. However, it is needed for exchanging the views between the primary care physicians and the patients or their caretakers. Health literacy includes acclimatisation to health information in various forms like interpreting charts. It is a necessity in making decisions about participating in research studies. Using medical tools like a thermometer or an inhaler pump requires a health-literate individual. The scope of HL also includes calculating the timing or dosage of medicine or voting on health or environmental issues.[2,3]
Don Nutbeam’s (2000) classification of health literacy includes three levels:[4]
Level 1: Functional health literacy: These are the basic skills of reading, writing, and numeracy necessary to function effectively in a health context.
Level 2: Interactive health literacy: This refers to more advanced cognitive literacy skills that with social skills can be used to actively participate in everyday situations, extract information and derive meaning from different forms of communication, and apply this to changing circumstances.
Level 3: Critical health literacy: This is the ability to critically analyse information and use this to exert greater control over life events and situations. HL relies on general literacy skills and has been described as “the bridge between literacy (and other) skills and abilities of the individual and the health context.”
How health literacy and education are different is delineated by the fact that it is sometimes challenging even for people with adequate literacy skills to understand healthcare information. They may not understand medical jargon and the basic concepts of health and medicine.[5]
By improving people’s access to health information and their capacity to use it effectively, health literacy is critical to empowerment.[6] However, it should be noted that health literacy is itself dependent upon the general level of literacy. Poor literacy hampers people’s health by limiting their personal, social, and cultural development as well as hindering the development of health literacy.[7]
A study conducted by Weiss BD et al.[8] highlights that people with limited health literacy are more likely to make medication errors, and they have a worse health status, more hospitalisations, and higher healthcare costs than people with adequate health literacy. The WHO recommends HL as an instrument for achieving several key targets listed in the Sustainable Development Goals.[9]
A low or insufficient health literacy ranging from 14% to 16% has been reported by various researchers across the globe.[4] While most tools are designed to assess reading comprehension and numeracy in English speakers, there is a need to develop a tool in the vernacular language for measuring health literacy in India.[10,11]
The 14-Item Health Literacy Scale (HLS-14) deals with functional, communicative, and critical literacy.[4,10] It was adapted by Suka M[12,13,14] for generic use from the health literacy scale specific to diabetic patients developed by Ishikawa and colleagues. HLS-14 applied the necessary capabilities of obtaining, understanding, and processing health-related information and decision-making in different manners or with different questions. The HLS-14 demonstrated adequate reliability and validity as a generic health literacy measure for Japanese adults.
The present study was conducted to determine the reliability and validity of HLS-14 translated into the Marathi language and estimate the health literacy of patients attending the out-patient department at a tertiary care centre.
Primary research question
1. Is the translated Marathi version of the HLS-14 scale reliable and valid?
Primary hypothesis
Translated Marathi version of the HLS-14 scale is reliable and valid.
Aim and objectives
To develop a Marathi version of a 14-item health literacy scale (HLS-14)
To test the reliability and validity of the Marathi version of the Health Literacy Scale (HLS- 14)
To estimate the health literacy among patients attending the out-patient department at a tertiary care centre using the 14-item health literacy scale (HLS-14).
Methodology
Study design: Cross-sectional study
Study setting: Shri Vasantrao Naik Government Medical College and Hospital, Yavatmal, Maharashtra.
Study population: The patients attending Anti Rabies Vaccination (ARV) Out Patient Department (OPD).
Sample size: Assuming the minimum expected correlation coefficient to be 0.44 (study by Suka M et al.)[12]
α = 0.05, β = 0.10
By using the formula N = [(zα+ Zβ)/C]2+ 3,
Where C = 0.5 X In [(1 + r)/(1-r)]
N = 50.
Sampling technique: Purposive sampling was done.
Study duration: 6 months (From July 2022 to December 2022).
Selection of study subjects
Inclusion criteria
Adults more than 18 years of age were selected as study participants. Those who understand both English and the Marathi language.
Those who were taking the full course of anti-rabies vaccination at GMCH OPD and therefore were available for follow-up.
Exclusion criteria
Healthcare workers or their family members.
The instrument for data collection: A pre-designed pre-tested questionnaire was used for data collection. It comprised two sections. Demographic characteristics were included in the first section of the questionnaire. The second section comprised the 14-item health literacy scale that was adapted from the health literacy scale specific to diabetes patients developed by Ishikawa and colleagues.
The HLS-14 contains five items about functional HL, five items about communicative HL and four items pertaining to critical HL. The 14 items are the same as those on the original HL scale, while the interrogative sentences have been modified so as not to be specific to diabetic patients.[12]
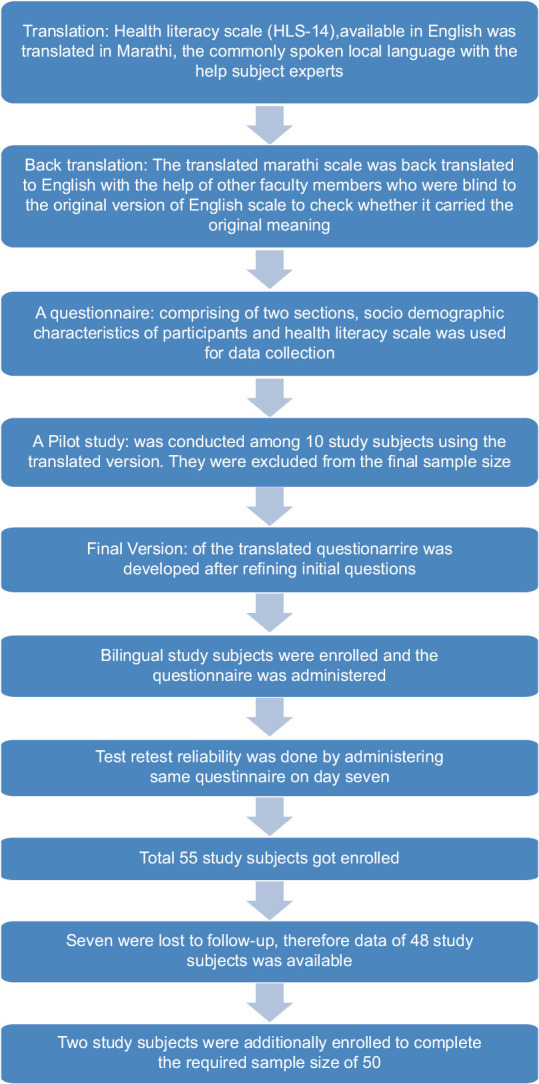
This scale was translated into Marathi, which is the local and most spoken language of Maharashtra. Help from the Marathi subject experts was sought for translation. The translated Marathi scale was back-translated to English with the help of other two faculty members who were blind to the original version of the English scale to check whether it carried the original meaning.
A pilot study was conducted on ten study subjects from ARV OPD to run the translated version, and the final version was developed after refining the initial questions.
Bilingual study subjects who know English as well as Marathi were selected from Anti Rabies Vaccination, Out Patients Department purposively. They were administered both versions of HLS-14 simultaneously to assess the internal validity of the translated scale. For testing the reliability of the translated tool, study subjects were administered the same tool again on day 7 (third dose of ARV). Data were collected till complete records of the required sample size (50) were obtained. Incomplete records and loss to follow-up were excluded from the study. Figure 1 shows the sequence of the procedure till enrollment of the participants.
Figure 1.
Flow chart for procedure till participant enrollment
Ethical consideration
Approval from the institutional ethics committee was sought before data collection (Vide letter no. O. No./VNGMC/Ethics Committee/190/2022 and date: 14/07/2022).
The participants were assured about the confidentiality of the data. Written informed consent was obtained from each participant prior to data collection.
Statistical analysis
Response options were noted on a 5-point Likert scale that indicates how much the respondent agrees or disagrees with the item (‘strongly disagree’ to ‘strongly agree’). The scores on the items were summed up for each respondent to give the total HL score as well as functional, communicative, and critical HL scores. Higher scores indicate a better HL.
The data were entered in Microsoft Excel and tabulated. Epi Info Version 7.0 was used for the frequency distribution. Cronbach’s alpha was calculated for internal validity, and the correlation coefficient was calculated for the reliability of the tool.
Results
Of the total 50 study subjects, 30 (60%) were male. The mean (SD) age of the study subjects was 33 (±10.58) with a range of 18–62 years. Half of the subjects were graduates, 27 (54%), followed by intermediate/diploma 12 (24%), while 9 (18%) study subjects were professionals. Most of the study subjects, 31 (62%), belonged to socio-economic status class II, followed by class III 13 (26%), while 3 (6%) study subjects belonged to socio-economic status classes I and IV.[15]
Internal consistency was checked via Cronbach’s alpha coefficient, which reflects the extent to which items within an instrument measure various aspects of the same characteristic or construct. It is used to determine whether a collection of items consistently measures the same characteristic. A high value of Cronbach’s alpha indicates that response values for each participant across a set of questions are consistent. Acceptable values range from 0.6 to 0.8. The Cronbach’s alpha value found for the current translated Marathi questionnaire is 0.66. Therefore, it can be concluded that the internal consistency is good.
Item analysis was done for each item. All the items barring 2, 6, and 10 gave an r-value of more than 0.70, which shows good reliability of each translated item [Table 1].
Table 1.
Item-wise correlation coefficients for the Marathi version of HLS-14
| Item | Correlation coefficient |
|---|---|
| I find characters that I cannot read | 0.89 |
| The print is too small for me (Even though I wear glasses) | 0.65 |
| The content is too difficult for me | 0.70 |
| It takes a long time to read them | 0.75 |
| I need someone to help me read them | 0.73 |
| I collect information from various sources | 0.38 |
| I extract the information I want | 0.77 |
| I understand the obtained information | 0.93 |
| I tell my opinion about the illness to my doctor, family, or friends | 0.78 |
| I apply the obtained information to my daily life | 0.42 |
| I consider whether the information is applicable for me | 0.81 |
| I consider whether the information is credible | 0.78 |
| I check whether the information is valid and reliable | 0.76 |
| I collect information to make my healthcare decisions | 0.78 |
The same Marathi version was again administered to the same participants on day 7 to test re-test reliability and correlation coefficient; the r-value was calculated [Table 2].
Table 2.
Test re-test reliability on day 7 follow-up of the Marathi questionnaire
| Item | Correlation coefficient |
|---|---|
| I find characters that I cannot read | 0.24 |
| The print is too small for me (Even though I wear glasses) | 0.28 |
| The content is too difficult for me | 0.22 |
| It takes a long time to read them | 0.41 |
| I need someone to help me read them | 0.75 |
| I collect information from various sources | 0.28 |
| I extract the information I want | 0.50 |
| I understand the obtained information | 0.49 |
| I tell my opinion about the illness to my doctor, family, or friends | 0.36 |
| I apply the obtained information to my daily life | 0.38 |
| I consider whether the information is applicable for me | 0.30 |
| I consider whether the information is credible | 0.35 |
| I check whether the information is valid and reliable | 0.28 |
| I collect information to make my healthcare decisions | 0.53 |
The mean functional health literacy score was found to be 18.20 ± 3.76, the mean communicative health literacy score was 18.10 ± 3.40, the mean critical health literacy score was 14.86 ± 3.00, and the mean total health literacy score was 51.16 ± 6.81. The median score was 51 [Table 3].
Table 3.
Mean health literacy scores
| Health literacy scores | Mean±SD |
|---|---|
| Functional health literacy score (Q1-Q5) | 18.20±3.76 |
| Communicative health literacy score (Q6-Q10) | 18.10±3.40 |
| Critical health literacy score (Q11-Q14) | 14.86±3.00 |
| Total health literacy score (Q1-Q14) | 51.16±6.81 |
Discussion
With technological advancement and widespread Internet access, health information is easily available. For its effective use, adequate health literacy is indispensable.[14] People with limited health literacy are more likely to make medication errors as they have less health knowledge, resulting in worsening their health status.[8] Thus, the estimation of health literacy is an important concern, especially for a primary care physician who might be involved in the continuum of care for the patients.[16]
The present study translated the English version of HLS-14 to Marathi. The translated Marathi version was administered to bilingual study subjects. To assess the reliability of the translated tool, correlation coefficients for all 14 items in HLS-14 were calculated. All the items barring 2, 6, and 10 gave an r-value of more than 0.70, which shows good reliability of each translated item. Azizi N et al.[17] conducted a study to develop and assess the psychometric properties, the Health Literacy Scale for Workers (HELSW). They reported the reliability of a tool using Pearson’s r, which ranged between 0.69 and 0.86. Tavousi M et al.[18] evaluated an instrument for measuring health literacy among adults and found the stability of the scale and its sub-scales as measured by the intra-class correlation coefficient, which ranged from 0.76 to 0.91 and was satisfactory.
The Cronbach’s alpha value was found to be 0.66, in the present study, which indicates good internal consistency. Suka M et al.[12] conducted a questionnaire survey among 1507 eligible respondents to assess the reliability and validity of the HLS-14, in which Cronbach’s alpha indicated satisfactory internal consistency of the functional, communicative, and critical HL scores (0.83, 0.85, and 0.76, respectively). Suto, M et al.[13] conducted a cross-sectional online survey among Japanese men and women aged 16–49 (n = 2000) to develop a health literacy scale in Japanese and found that values of Cronbach’s α for the 13-item knowledge scale were 0.661 (the standard error of measurement was 1.388) and 0.831 for the Cardiff Fertility Knowledge Scale (the standard error of measurement was 1.472). Devi MA et al.[19] conducted a study among 500 college students and reported that the internal consistency reliability was 0.408. Puello SCP et al.[20] estimated the internal consistency of the HLS-14, the Brazilian Portuguese version using Cronbach’s α coefficient as 0.82. For functional literacy, α = 0.66; for communicative literacy, α = 0.90; and for critical literacy, α = 0.81.
In the present study, the mean score (± SD) of HLS–14 was found to be 51.16 ± 6.81. Similar scores (51.2 and 50.7, respectively) were noted by Aoki T et al.[21] and Suka M et al.[22] in a cross-sectional survey, among adult residents of Japan using a 14-item Health Literacy Scale (HLS-14). In a study by Li X et al.[23] in China, a lower score for health literacy was found. The average score was 44. Similarly, a mean total score of 45.16 for the Brazilian Portuguese version of HLS-14 was noted by Puello SCP et al.[20] In the present study, the mean functional health literacy score was found to be 18.20 ± 3.76, the mean communicative health literacy score was 18.10 ± 3.40, and the mean critical health literacy score was 14.86 ± 3.00, which are in congruence with the findings of Suka M et al.[12]
Conclusions
The translated Marathi version of HLS-14 is valid and reliable. The level of health literacy among the study participants is marginal.
Limitations
Test re-test reliability can be better studied after a longer follow-up duration.
Health literacy was seen among the participants who knew English as well as Marathi, which may be a selectively well-educated class. Health Literacy among random samples may be lower than found in the current study.
Institutional ethics committee approval
Taken from IEC SVN Government Medical College, Yavatmal, Maharashtra, India. (Vide letter no. O. No./VNGMC/Ethics Committee/190/2022 and date: 14/07/2022).
Financial support and sponsorship
We are extremely grateful and acknowledge the support and funding under the scheme of Padvidhar Sanshodhan Prakalp Anudan – 2022 of IPHA Maharashtra for conducting this study.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We are grateful to Dr.Gautum Khakse, Head of the Department of Community Medicine, SVNGMC, Yavatmal, for his guidance and support. We extend our gratitude to the faculty members of the Department of Community Medicine, SVNGMC, Yavatmal for their role in translating and back-translating the scale. We are extremely grateful and acknowledge the support and funding under the scheme of Padvidhar Sanshodhan Prakalp Anudan – 2022 of IPHA Maharashtra for conducting this study.
References
- 1.Nutbeam D. Health promotion glossary. Health Promot Int. 1998;13:349–64. [Google Scholar]
- 2.Nielsen-Bohlman L, Panzer AM, Kindig DA. Institute of Medicine (US) Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington (DC): National Academies Press (US); 2004. [[Last accessed on 2022 Dec 26]]. Preface. Available from: https://www.ncbi.nlm.nih.gov/books/NBK216035/ [PubMed] [Google Scholar]
- 3.ECOSOC. “MINISTERIAL DECLARATION –2009 HIGH-LEVEL SEGMENT: Implementing the internationally agreed goals and commitments in regard to global public health.”. 2009. [[Last accessed on 2022 Dec 26]]. Available from: https://www.un.org/en/ecosoc/julyhls/pdf/09%20nvp%20summary%209%20july%20final.pdf .
- 4.Nutbeam D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15:259–67. [Google Scholar]
- 5.Sarbhadhikari SN. How to make healthcare delivery in India more informed. Educ Health (Abingdon) 2010;23:456. [PubMed] [Google Scholar]
- 6.World Health Organization website. Health topics. Health Promotion. [[Last accessed on 2022 Dec 26]]. Available from: https://www.who.int/teams/health-promotion/enhanced-wellbeing/ninth-global-conference/health-literacy .
- 7.Wolf MS, Gazmararian JA, Baker DW. Health literacy and health risk behaviors among older adults. Am J Prev Med. 2007;32:19–24. doi: 10.1016/j.amepre.2006.08.024. [DOI] [PubMed] [Google Scholar]
- 8.Weiss BD, Mays MZ, Martz W, Castro KM, Darren A, Pignone MP, et al. Quick assessment of literacy in primary care: The newest vital sign. Ann Fam Med. 2005;3:514–22. doi: 10.1370/afm.405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.World Health Organization, Programme TUND Policy brief 4: Health literacy. The 9th global conference on health promotion. Shanghai, China. 2017. [[Last accessed on 2022 Dec 03]]. pp. 2–3. Available from: https://www.who.int/teams/health-promotion/enhanced-wellbeing/ninth-global-conference/health-literacy .
- 10.Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care. 2008;31:874–9. doi: 10.2337/dc07-1932. [DOI] [PubMed] [Google Scholar]
- 11.Jordan JE, Osborne RH, Buchbinder R. Critical appraisal of health literacy indices revealed variable underlying constructs, narrow content and psychometric weaknesses. J Clin Epidemiol. 2011;64:366–79. doi: 10.1016/j.jclinepi.2010.04.005. [DOI] [PubMed] [Google Scholar]
- 12.Suka M, Odajima T, Kasai M, Igarashi A, Ishikawa H, Kusama M, et al. The 14-item health literacy scale for Japanese adults (HLS-14) Environ Health Prev Med. 2013;18:407–15. doi: 10.1007/s12199-013-0340-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Suto M, Mitsunaga H, Honda Y, Maeda E, Ota E, Arata N, et al. Development of a health literacy scale for preconception care: A study of the reproductive age population in Japan. BMC Public Health. 2021;21:2057. doi: 10.1186/s12889-021-12081-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liu H, Zeng H, Shen Y, Zhang F, Sharma M, Lai W, et al. Assessment tools for health literacy among the general population: A systematic review. Int J Environ Res Public Health. 2018;15:1711. doi: 10.3390/ijerph15081711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gunjan K, Dash P, Patnaik J, Pany G. Socioeconomic status scale-Modified Kuppuswamy Scale for the year 2022. Int J Comm Dent. 2022;10:1–6. [Google Scholar]
- 16.Dowse R. The limitations of current health literacy measures for use in developing countries. J Commun Healthc. 2016;9:4–6. [Google Scholar]
- 17.Azizi N, Karimy M, Abedini R, Armoon B, Montazeri A. Development and validation of the health literacy scale for workers. Int J Occup Environ Med. 2019;10:30–9. doi: 10.15171/ijoem.2019.1498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tavousi M, Haeri-Mehrizi A, Rakhshani F, Rafiefar S, Soleymanian A, Sarbandi F, et al. Development and validation of a short and easy-to-use instrument for measuring health literacy: The Health Literacy Instrument for Adults (HELIA) BMC Public Health. 2020;20:655. doi: 10.1186/s12889-020-08787-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Devi MA, Soni S, Radha G, Kadanakuppe S, Nagashree SR, Pallavi SK. Reliability and validity of a questionnaire to assess oral health literacy among college students in Bangalore City. J Contemp Dent. 2011;2:43–7. [Google Scholar]
- 20.Puello SCP, Silva-Junior MF, de Sousa MLR, Batista MJ. Criterion validity of 14 item health literacy scale (HLS-14) questionnaire among Brazilian adults and older people. Health Promot Int. 2022;37:daac142. doi: 10.1093/heapro/daac142. [DOI] [PubMed] [Google Scholar]
- 21.Aoki T, Inoue M. Association between health literacy and patient experience of primary care attributes: A cross-sectional study in Japan. PLoS One. 2017;12:e0184565. doi: 10.1371/journal.pone.0184565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Suka M, Odajima T, Okamoto M, Sumitani M, Igarashi A, Ishikawa H, et al. Relationship between health literacy, health information access, health behavior, and health status in Japanese people. Patient Educ Couns. 2015;98:660–8. doi: 10.1016/j.pec.2015.02.013. [DOI] [PubMed] [Google Scholar]
- 23.Li X, Duan T, Lai Y, Wang X, Yang L, Su X, et al. Status of medication literacy and its related factors among undergraduate students in Shanxi Province, China: A cross-sectional study. J Clin Pharm Ther. 2022;47:1201–11. doi: 10.1111/jcpt.13655. [DOI] [PubMed] [Google Scholar]