

Abstract
Background
While a high incidence of pickleball-related falls is reported, little is known regarding factors differentiating persons with and without a fall history during play.
Purpose
This study aimed to determine differences between recreational pickleball players who fell while playing and those who did not. Additional aims were to determine reasons for falling and to investigate associations among assessed factors.
Study design
Cross-sectional study.
Methods
Participants completed a survey reporting age, fall history, and reasons for falling during play. Hip abduction strength, single leg squat form, ankle dorsiflexion, and change of direction time using a modified T-test on a pickleball court (i.e. pickleball T-test) were assessed.
Results
Among the 92 individuals participating in the study, 42% reported a fall while playing and 30% reported falling more than once. Leading reasons for reported falls were lunging and moving backward. Participants who reported falling were significantly older (z = -2.60, p = 0.009) and slower on the pickleball T-test (z = -2.10, p = 0.036) than those who did not report falling. Hip abduction strength was not associated with fall history but was associated with faster time on the pickleball T-test (left rs = -.41, p < 0.001, right rs = -.48, p < 0.001). Single leg squat form and dorsiflexion were not related to fall history.
Conclusion
Falls are common among recreational pickleball players, particularly older players. Fall prevention programs for pickleball players should be considered including multi-directional lunging, lower extremity strength and power development, and change of direction training that includes moving backward.
Level of evidence
2
Keywords: racket sports, falls, change of direction, hip abduction strength
INTRODUCTION
Pickleball is the fastest growing sport in the United States with nearly 50 million American adults participating in 2023, a 48% increase from the previous year.1 Played on a smaller version of a tennis court with a plastic, whiffle-type ball and short paddle, pickleball is an easy-to-learn, low-impact sport. Pickleball has been shown to promote social interactions, improve life satisfaction, and reduce depression.2 In addition to the psychosocial benefits of pickleball, both singles and doubles play results in moderate to vigorous intensity exercise,3 which can be an enjoyable way for individuals to meet recommended physical activity guidelines.
Along with the rapid growth of the sport is an alarming number of pickleball-related injuries. Falls accounted for 63% of all pickleball-related injuries seen in United States emergency departments.4 Using data from 2013-2017, players over the age of 50 accounted for more than 90% of pickleball-related injuries.5 Standardized fall assessments such as the 30-second sit-to-stand test and the Timed Up and Go test exist but are unlikely to challenge recreational pickleball players. Additionally, participants in the sport of pickleball are changing rapidly. In 2016, it was estimated that 75% of “core” players (those who played regularly) were 55 years of age or older.6 However, in 2023, the average age of core players dropped to 35 years of age.1 Given this age-related shift and the greater mobility of recreational pickleball players compared to community-dwelling adults, the best assessments to identify those at risk for falling during play is unknown.
Unfortunately, little is known about why pickleball players fall. Muscle weakness is an important risk factor for falls in community-dwelling adults7 and for injury in athletics.8 Specifically, deficits in hip abductor strength are associated with falls, while hip extensor and external rotator strength are not.9 The hip abductors play a key role in frontal plane mechanics10 by helping control the hip and pelvis during activities such as running, side stepping, and lunging. Efficient lunging, a quick step in any direction followed by an immediate return to the start position, is considered key to success in racket sports.11 Given the lateral movement and lunging required during pickleball, hip abductor strength may be an important factor in pickleball performance. The association between falls and hip abductor strength in pickleball players is currently unknown.
Squatting is a fundamental movement that is required for pickleball players to achieve the ready position and a pre-requisite to the lunging and direction changes necessary during play. A single leg squat requires greater stability, neuromuscular control, and balance than a traditional squat. Some studies have shown a relationship between hip abductor weakness and poor single leg squat form,12,13 but this relationship is limited14 and the test should not be used to screen for hip abductor weakness.15 While better single leg squat form is seen in more active individuals,16 the relationship between single leg squat form and fall risk is unknown. Squatting requires at least some weightbearing dorsiflexion range of motion. Limited weightbearing dorsiflexion is correlated with reduced balance17 and increased fall risk18 in older adults. Therefore, examining weightbearing dorsiflexion as a potential risk factor for falls in pickleball players is warranted.
Change of direction training is a recommended component of fall prevention programs in community-dwelling older adults.19 The ability to change direction is also an important determinant of athletic performance.20 The association between change of direction and falls in pickleball players has not been previously investigated. Pickleball play requires movement in a variety of directions to accelerate to the ball and then quickly recover to prepare for the next shot. A standardized change of direction test, the T-test, involves participants running forward 9.14m (30 feet), then side shuffling left 4.57m (15 feet), then side shuffling right 9.14m (30 feet) before running backward 9.14m (30 feet). While the standard T-test is reliable,21 the distance covered is significantly greater than would be required in pickleball given the small court size. Because assessments should match sport-specific demands, a modified version of the T-test that is shorter, but still requires the same motions, may more accurately assess the change of direction required of pickleball players.
This study aimed to determine if there were differences between recreational pickleball players who fell while playing and those who did not in terms of age, hip abductor strength, single leg squat form, weightbearing dorsiflexion range of motion, and change of direction time. It was hypothesized that those with a fall history during play would be older, have lower hip abduction strength, poorer single leg squat form, less weightbearing dorsiflexion, and be slower on the change of direction test. Additional aims were to determine reasons for falling and to investigate any associations among assessed factors.
METHODS
Study Design
Cross sectional study.
Participants
Recreational pickleball players from free community centers with indoor pickleball courts and from free outdoor community pickleball courts were recruited to participate in the study. To be included in the study, participants had to be at least 18 years of age and be currently participating in the sport of pickleball without restriction.
Procedures
The study was approved by the Institutional Review Board of University of Tennessee Chatanooga. After being informed of the study, willing participants provided written consent for physical performance testing. Participants were given a link to an online confidential survey with its own online consent. The survey included questions regarding participant name, age, fall history, and reasons for falling during play. A draft of the survey was trialed by 10 individuals familiar with the sport of pickleball and the survey was revised for content, clarity, and brevity. Participants were not required to answer every question. The name of the participant was collected and used to match survey information to physical performance testing.
All assessments were performed on indoor or outdoor pickleball courts. Measurements were performed by one of three assessors. Each assessor practiced in a blinded fashion until they were approved on technique and consistency by the primary investigator. Participants performed a 5-minute dynamic warm-up including jogging forward and backward, side shuffling, and lunging followed by any individual stretching/warm-up as desired. Participants who had played pickleball within 15 minutes of testing could choose to omit this dynamic warm-up and rested for 5-10 minutes prior to any testing while paperwork was being completed. Left and right hip abduction strength was measured with the participant sidelying on a yoga-style mat with the top hip abducted to the horizontal with shoes removed. The assessor resisted the participant’s ability to hold the leg abducted horizontally using a handheld dynamometer (microFET2, Hoggan Scientific LLS; Salt Lake City, UT) placed just proximal to the lateral malleolus. This method has been found to be reliable.22 The force, in kilograms, was recorded to the nearest 0.1 kg. Leg length was measured only on the right leg from the greater trochanter to the lateral malleolus and recorded to the nearest cm. Hip strength was assessed as hip abduction torque (Nm), calculated using the formula: hip abduction force (kg) x leg length (m) x 9.81.
The single leg squat was performed with shoes removed. Visual assessment of single leg squat form has been found to be reliable.23 The participant was first asked to perform a squat to between 45 and 60 degrees of knee flexion while keeping hands on hips. The assessors observed from the side and provided feedback to ensure the squat was performed to the correct depth. Then, the participant was asked to stand on one foot, holding the other out in front. The participant then performed a single squat to the same depth with feedback as needed. The assessor then stood in front of the participant to observe and score the single leg squat on the second attempt. Scoring was adapted from Poulson and James24 as follows: 0 = the patella remains in midline; 1 = the patella moves slightly medial to the foot, 2 = the patella moves significantly medial to the foot, 3 = unable to single leg stand or perform that test. Weightbearing dorsiflexion was also performed with shoes removed. Measuring weightbearing dorsiflexion with an inclinometer has been shown to be reliable.25 The participant performed a lunge moving into maximum dorsiflexion three times. On the third attempt, the assessor placed a digital inclinometer (Acumar, Grayline Medical; Norwalk, CA) on the anterior tibia just distal to the tibial tuberosity to measure the maximal amount of dorsiflexion to the nearest degree.
Change of direction was assessed with the pickleball T-test (Figure 1), a modified version of the T-test, using pickleball court dimensions. The participant wore their typical pickleball shoes to perform the test. With the participant’s feet behind the start line, the recorder gave the commands: “ready, set, go.” The participant (1) ran forward to the non-volley line, (2) side shuffled left to the left side line, (3) side shuffled right to the right sideline, (4) side shuffled left to the center line, then (5) ran backward to the end line. Timing stopped when any portion of the participant’s body crossed the end line. Test time was recorded to the nearest 1/100th of a second using a stopwatch. If a participant did not complete the test correctly (e.g. started early or failed to reach to, or past, the sideline), the test was repeated after resting a minimum of 90 seconds. Rest period was determined based on the time required for the phosphagen system to recover.26 Test order was not strictly controlled although tests performed without footwear were grouped together.
Figure 1. Pickleball T-test.
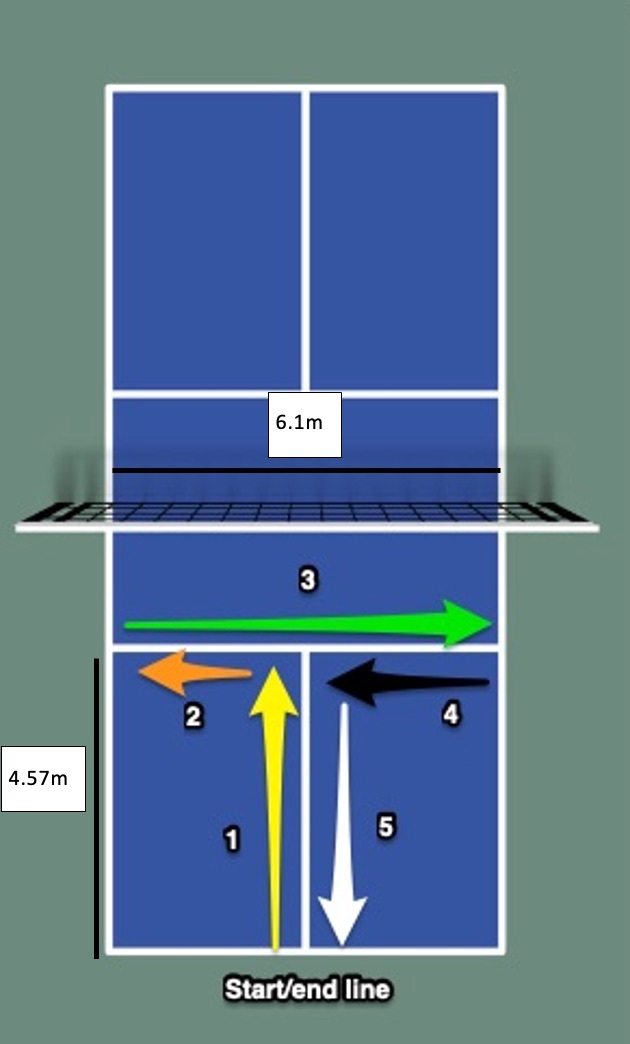
m=meters
Participants who completed the physical performance test were assigned a coded number and test results were entered into an Excel spreadsheet. Survey data were downloaded to a second Excel spreadsheet where participant names were matched with the coded numbers. Participant names were then removed, and the two spreadsheets were merged before being imported into SPSS version 29.0 for analysis.
Statistical Analysis
Frequency data was reported for age and fall history. The Shapiro-Wilk test indicated a non-normal data distribution for the pickleball T-test, hip abduction strength, and weightbearing dorsiflexion; therefore, nonparametric tests were performed, and medians and inner quartile ranges were reported. The Mann-Whitney U test with an alpha level of 0.05 was used to determine the differences in age, hip abduction strength, single leg squat form, dorsiflexion motion, and pickleball T-test between those who reported a fall while playing pickleball and those who did not. Effect sizes (r) were calculated. For this study, the strength of the effect size was defined as follows: r < .30 = small effect, r between .30 and .50 = medium effect, r >.50 = large effect. Correlations between age, hip abduction strength, single leg squat form, weightbearing dorsiflexion, and the pickleball T-test were determined using the Spearman rank correlation coefficient. For this study, correlation strength (rs) was defined as follows: .00-.09: negligible correlation, .10-.39 – weak correlation, .40-.69 = moderate correlation, .70-.89 = strong correlation, .90-1.0 = very strong correlation.
RESULTS
Ninety-two individuals (48 females, 43 males, and one preferred not to answer) completed both the online survey and the physical performance testing. Participant ages ranged from 18 to 79 years of age, with 66% of participants being younger than 55 years of age. The median age range of participants who reported falling was 50-54 years, while the median age range of those who did not report a fall was 30-34 years (Table 1).
Table 1. Participant age range.
| Age | Participants Reporting a Fall While Playing | Participants Not Reporting a Fall While Playing |
|---|---|---|
| 18-24 | 4 | 12 |
| 25-29 | 4 | 12 |
| 30-34 | 2 | 6 |
| 35-39 | 2 | 4 |
| 40-44 | 0 | 1 |
| 45-49 | 5 | 1 |
| 50-54 | 3 | 5 |
| 55-59 | 2 | 5 |
| 60-64 | 4 | 4 |
| 65-69 | 8 | 1 |
| 70-74 | 5 | 1 |
| 75-79 | 0 | 1 |
Table 2 includes results for participants based on reported fall status. Thirty-three percent of participants under the age of 55 reported a fall, whereas 61% of participants 55 years of age or older reported a fall. Definitions of older adulthood vary and cut points for groupings within studies can be rather arbitrary based on age-related changes to individual body systems, to the criterion for participating in the National Senior Games, or when Social Security benefits can be received (in full, or in part). In this study, the cut point for age was based on the societal factor that many individuals begin to retire or reduce their work hours near 55 years of age, thereby allowing them more time to explore recreational activities such as pickleball more consistently. Thirty-nine participants (42%) reported a fall while playing pickleball, with 28 participants (30% of all participants) reporting falling more than once (Figure 2). Table 3 notes the reasons participants reported for falling. The two leading reasons for falls were lunging and moving backward.
Table 2. Results for participants based on reported fall status.
| Participants Reporting a Fall While Playing | Participants Not Reporting a Fall While Playing | |
|---|---|---|
| Agea | 18-54 years of age: 20 55 years or older: 19 |
18-54 years of age: 41 55 years or older: 12 |
| Single leg squat score | 0: L 14 / R 13 1: L 14 / R 14 2: L 9 / R 9 3: L 2 / R 3 |
0: L 20 / R 22 1: L 20 / R 20 2: L 11 / R 8 3: L 2 / R 3 |
| Weightbearing dorsiflexionb | L 34° (11) / R 34° (12) | L 36° (9) / R 37° (8) |
| Left hip abduction strengthb | L: 12.45 Nm (9.21)c R: 11.68 Nm (10.51)c |
L: 11.17 Nm (4.64)c R: 11.10 Nm (4.84)c |
| Pickleball T-test | 9.12 sec (2.40)c | 8.16 sec (2.40)c |
a = frequency, b = strength measured as hip abduction torque, c = median (inner quartile range)
Figure 2. Fall frequency.

Table 3. Reason for falls.
| Reason for Fall | Number (%) |
|---|---|
| Lunging | 26 (57%) |
| Moving backward | 11 (24%) |
| Ran into another player | 4 (8%) |
| Ran into the fence | 3 (7%) |
| Ran into the net | 2 (4%) |
| Dizziness | 0 (0%) |
Participants who reported falling were significantly older and slower on the pickleball T-test (Table 4). These differences had small effect sizes. In contrast, hip abduction strength was not significantly different between participants who reported a fall while playing and those who did not report a fall. There were no differences in hip strength, single leg squat form, ankle dorsiflexion, or pickleball T-test between those who fell only once (N = 11) and those who fell more than once (N=28).
Table 4. Between group differences for participants reporting a fall and participants not reporting a fall while playing pickleball.
| Measure | Mann-Whitney U | z-score | p-value | r |
|---|---|---|---|---|
| Age | 764.00 | -2.60 | p = 0.009 | .27 |
| Left hip abduction strength | 847.50 | -1.09 | p = 0.275 | -- |
| Right hip abduction strength | 904.00 | -0.83 | p = 0.407 | -- |
| Pickleball T-test | 746.00 | -2.10 | p =0.036 | .22 |
| Left single leg squat | 992.50 | -.12 | p = 0.90 | -- |
| Right single leg squat | 906.00 | -.86 | p =0 .864 | -- |
| Left dorsiflexion | 808.00 | -1.61 | p = 0.161 | -- |
| Right dorsiflexion | 770.50 | -1.91 | p = 0.057 | -- |
Significant results are bolded, r = effect size
Significant correlations between age, the hip abduction strength, and the pickleball T-test were found (Table 5). Faster times on the pickleball T-test were associated with greater hip abduction strength and younger age. Age was not significantly correlated with hip abduction strength or single leg squat form. Age was inconsistently related to weightbearing dorsiflexion. Hip abduction strength was not correlated with single leg squat form. Right single leg squat form was weakly correlated with right weightbearing dorsiflexion but left was not. Left single leg squat form was weakly correlated with the pickleball T-test, but right was not.
Table 5. Correlations (rs) between variables.
| Age |
Left
abd |
Right
abd |
Left
SLS |
Right
SLS |
Left
DF |
Right
DF |
Pickleball
T-test |
|
|---|---|---|---|---|---|---|---|---|
| Age | 1.00 | -.05, p=.650 |
-.16, p= 0.119 |
.075, p=0.479 | .057, p=0.588 |
-.22,
p=0.038 |
-.185, p=0.079 |
.68,
p <0.001 |
| Left abd | 1.00 | .91, p <0.001 |
-.101, p=0.342 | --- | -.010, p= 0.92 | --- |
-.41,
p<0.001 |
|
| Right abd | 1.00 | --- | .001, p=0.996 | --- | -.078, p=0.462 |
-.48,
p<0.001 |
||
| Left SLS | 1.00 | --- | -.166, p=0.116 | --- | .240, p=0.022 | |||
| Right SLS | 1.00 | --- | -.209, p=0.047 | .142, p=0.178 |
Abd = hip abduction strength; SLS = single leg squat form; DF = weight bearing dorsiflexion range of motion
DISCUSSION
The majority of participants in this study were under 55 years of age making this sample consistent with the shift toward younger players. Nearly half of the participants reported a pickleball-related fall. As hypothesized, persons who reported having fallen during play were significantly older than those who did not report falling. Similar to a study in community-dwelling adults,27 falls in recreational pickleball players were twice as common among older individuals. While some falls are of little consequence, each fall event has a potential for injury, particularly in older individuals, as the number of falls resulting in injuries increases with age.27,28 For senior men and women, the primary mechanism for pickleball-related injury was a slip, trip, fall or dive.4 While pickleball may have positive psychosocial benefits and assist with maintaining an active lifestyle, the sport is not entirely without risk.
Contrary to the initial hypothesis, hip abduction strength did not differ based on reported fall status. Given the key role lunging plays in racket sports and that lunging was the most reported reason for falls in this study, it may be important to consider the strength of other key muscle groups in this population. For example, electromyographic studies29–31 have shown quadriceps and gluteus maximus activation to be slightly greater than gluteus medius activation during a forward lunge. Paz et al32 found gluteus medius activation varies based on lunge direction. Therefore, strengthening of the quadriceps and all hip musculature may improve stability while lunging to avoid a fall.
Contrary to the initial hypothesis, single leg squat form and weightbearing dorsiflexion were not different between those who reported falls and those who did not. The single leg squat has been used to identify aberrant motion (dynamic knee valgus) and is a reasonable screening tool for injury prevention.33 However, because this assessment is a pre-planned, single-plane movement pattern with an unchanging base of support, it is not surprising that the single leg squat is not related to falls in individuals participating in a dynamic, multi-directional, and reactive sport, such as pickleball. Therefore, the use of a single leg squat to screen for fall risk is not recommended. Likewise, while limited weightbearing dorsiflexion has been linked to fall risk in older populations,18and to both high-risk positioning34 and injury in an athletic population,35 the relationship between limited dorsiflexion and falls in an athletic population is not apparent.
As hypothesized, participants reporting a fall were significantly slower on the change of direction test than those who did not fall. The pickleball T-test may have been able to distinguish between those reporting a fall and those who did not report a fall because it required participants to move backward at speed. The limits of stability are smaller when moving backward than when moving in other directions. Moving backward challenges balance more than moving in other directions due to the inability to see where one is going. Planned backward movement during testing is predictable and, therefore, less challenging than the reactive backward movement that may occur during play. The inclusion of backward movement during training and testing is suggested related to the observation that about a quarter of reported falls in this study occurred while moving backward.
The pickleball T-test required participants to change direction four times while moving in the straight plane directions of left-right and forward-backward. The point of each direction change is similar to a straight plane lunge in that the participant must stop the momentum of the center of mass from continuing in one direction, then quickly accelerate in the opposite direction. Such movement requires not only strength, but power (the ability to apply force quickly). A study by Simpkins and Yangon,36 found that power was a better predictor of falls than strength. Future studies might consider the use of force plates to measure the relationship between falls and both the amount of force generated and the rate of force development during lunging in various directions in pickleball players.
In this study, there was a moderate to strong correlation between the pickleball T-test and age implying that as age increases so does the time required to complete the change of direction test. While an age-related decline in speed is to be expected, a study by Rodrigues37 found a positive correlation between greater change of direction time and a greater fear of falling in community-dwelling older adults. Therefore, it is possible that older pickleball players may be proactively self-limiting their speed during the change of direction test to ensure safety due to a heightened fear of falling during the test. It is important to consider that such a cautious approach during the change of direction test may not be replicated during game play, where factors such as competitiveness or motivation might influence player movement strategies. A change of direction training program may help build player confidence and reduce change of direction time. This may also allow participants to practice change of direction at speeds that more closely replicate how they participate in the sport of pickleball, ultimately reducing the risk of falls.
There was no relationship between age and hip abduction strength and single leg squat form. Additionally, there was only a weak correlation between age and left weightbearing dorsiflexion. Regular participation in recreational activities has been shown to slow age-related decline in strength, balance/neuromuscular control, and range of motion.38 It appears that pickleball participation could affect these expected age-related changes.
There was a moderate negative correlation between hip abduction strength and change of direction time, with stronger players completing the pickleball T-test faster than their weaker counterparts. This inverse relationship between strength and change of direction aligns with both the Rodrigues study37 of older adults and with studies regarding athletic performance among persons of various ages.39,40 General strength training has been noted to improve change of direction abilities.41 Single leg squat form on the left lower extremity was only weakly correlated with change of direction time, but there was no significant correlation on the right lower extremity. Clinically, it is possible that a holistic strength, neuromuscular control, and power training program for recreational pickleball players, including exercises targeting the hip abductors, may reduce change of direction times, thus both lowering the risk of falls and improving athletic performance. Additional studies are warranted to assess these potential links. In keeping with the previously cited literature, this study did not find a consistent relationship between hip abduction strength, single leg squat form, and ankle dorsiflexion range.
A limitation of this study is the retrospective nature of fall reporting. Additionally, participants may have misinterpreted what should be counted as a fall or have been hesitant to report having fallen while playing pickleball. Some participants were tested after playing or during a break in play rather than after performing the specific dynamic warm-up. The order of testing was not strictly controlled. These factors may have influenced performance on the strength and change of direction tests due to fatigue. It is possible that the limited sample size prevented the identification of differences between those who fell and those who did not fall. While increasing the sample size would improve the power of the study, the sample size was sufficient to provide initial direction for future studies. The tests performed in this study were able to be performed courtside. It is possible that more sophisticated testing conducted in a biomechanics laboratory, such as isokinetic or force plate testing, might be able to identify additional factors related to falls in pickleball players.
CONCLUSION
Nearly half of recreational pickleball players reported a pickleball-related fall, with the majority of falls due to lunging and backward movement. Persons reporting a fall were significantly older and slower on the change of direction test. An inverse relationship was found between hip abduction strength and change of direction time. Falls were not related to single leg squat form or weightbearing dorsiflexion. Fall prevention programs for pickleball players should be considered including multi-directional lunging, lower extremity strength and power development, and change of direction training that includes moving backward.
Disclosures
The authors declare they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this study.
Acknowledgments
ACKNOWLEDGEMENTS
The authors wish to acknowledge the valuable contributions made by the recreational pickleball players who participated in this study.
References
- Association of Pickleball Players 2023APP pickleball participation research: Part two - March 2023. :1–5.
- Serious leisure and depression in older adults: A study of pickleball players. Heo J., Ryu J., Yang H., Kim K. M. 2018Leis Stud. 37(2018):561–573. doi: 10.1080/02614367.2018.1477977. doi: 10.1080/02614367.2018.1477977. [DOI] [Google Scholar]
- Physical activity intensity of singles and doubles pickleball in older adults. Webber S.C., Anderson S., Biccum L., Jin S., Khawashki S., Tittlemier B.J. J Aging Phys Act. 2022:1–6. doi: 10.1123/japa.2022-0194. doi: 10.1123/japa.2022-0194. [DOI] [PubMed] [Google Scholar]
- Non-fatal senior pickleball and tennis-related injuries treated in United States emergency departments, 2010-2019. Weiss H., Dougherty J., DiMaggio C. 2021Inj Epidemiol. 8(1):34. doi: 10.1186/s40621-021-00327-9. doi: 10.1186/s40621-021-00327-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pickleball-related injuries treated in emergency departments. Forrester M. B. 2020J Emerg Med. 58(2):275–279. doi: 10.1016/j.jemermed.2019.09.016. doi: 10.1016/j.jemermed.2019.09.016. [DOI] [PubMed] [Google Scholar]
- Pickleball: Injury considerations in an increasingly popular sport. Greiner N. 2019Mo Med. 116(6):488–491. [PMC free article] [PubMed] [Google Scholar]
- Appeadu M. K., Bordini B. Falls and fall prevention in older adults. [2023-12-2]. https://www.ncbi.nlm.nih.gov/books/NBK560761/ [PubMed]
- Exercise-based knee and anterior cruciate ligament injury prevention: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic and Sports Sections of the American Physical Therapy Association. Arundale A. J. H., Bizzini M., Giordano A.., et al. 2023J Orthop Sports Phys Ther. 53(1):CPG1–CPG34. doi: 10.2519/jospt.2023.0301. [DOI] [PubMed] [Google Scholar]
- Hip muscle and hand-grip strength to differentiate between older fallers and non-fallers: A cross-sectional validity study. Gafner S.C., Bastiaenen C.H., Ferrari S.., et al. 2018Clin Interv Aging. 13:1–8. doi: 10.2147/cia.S146834. doi: 10.2147/cia.S146834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Relationship between hip abductor muscle strength and frontal plane kinematics: A cross-sectional study in elite handball athletes. Ceballos-Laita L., Carrasco-Uribarren A., Cabanillas-Barea S.., et al. 2022Applied Sci. 12(19) doi: 10.3390/app121910044. doi: 10.3390/app121910044. [DOI] [Google Scholar]
- Badminton injuries in elite athletes: A review of epidemiology and biomechanics. Pardiwala D. N., Subbiah K., Rao N., Modi R. 2020Indian J Orthop. 54(3):237–245. doi: 10.1007/s43465-020-00054-1. doi: 10.1007/s43465-020-00054-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Performance on the single-leg squat task indicates hip abductor muscle function. Crossley K., Zhang W., Schache A., Bryant A., Cowan S. 2011Am J Sports Med. 39(4):866–873. doi: 10.1177/0363546510395456. [DOI] [PubMed] [Google Scholar]
- Relationship between hip and core strength and frontal plane alignment during a single leg squat. Stickler L., Finley M., Gulgin H. 2015Phys Ther Sport. 16(1):66–71. doi: 10.1016/j.ptsp.2014.05.002. doi: 10.1016/j.ptsp.2014.05.002. [DOI] [PubMed] [Google Scholar]
- The relationship between hip muscle strength and dynamic knee valgus in asymptomatic females: A systematic review. Dix J., Marsh S., Dingenen B., Malliaras P. May;2019 Phys Ther Sport. 37:197–209. doi: 10.1016/j.ptsp.2018.05.015. doi: 10.1016/j.ptsp.2018.05.015. [DOI] [PubMed] [Google Scholar]
- What are the validity of the single-leg-squat test and its relationship to hip-abduction strength? DiMattia M. A., Livengood A. L., Uhl T. L., Mattacola C. G., Malone T. R. 2005J Sport Rehabil. 14(2):108–123. doi: 10.1123/jsr.14.2.108. doi: 10.1123/jsr.14.2.108. [DOI] [Google Scholar]
- Single leg squat performance in physically and non-physically active individuals: A cross-sectional study. Gianola S., Castellini G., Stucovitz E., Nardo A., Banfi G. 2017BMC Musculoskelet Disord. 18:1–10. doi: 10.1186/s12891-017-1660-8. doi: 10.1186/s12891-017-1660-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balance and ankle range of motion in community-dwelling women aged 64 to 87 years: A correlational study. Mecagni C., Smith J. P., Roberts K. E., O'Sullivan S. B. 2000Phys Ther. 80(10):1004–1011. doi: 10.1093/ptj/80.10.1004. doi: 10.1093/ptj/80.10.1004. [DOI] [PubMed] [Google Scholar]
- Relationship between balance and ankle range of motion in adults aged 60 years and above. Metange D. P., Kulkarni V., Kapoor D. 2013Rom J Phys Ther. 19(32):15–25. [Google Scholar]
- Exercise-based fall prevention in the elderly: What about agility? Donath L., van Dieën J., Faude O. 2016Sports Med. 46(2):143–9. doi: 10.1007/s40279-015-0389-5. doi: 10.1007/s40279-015-0389-5. [DOI] [PubMed] [Google Scholar]
- The effect of angle and velocity on change of direction biomechanics: An angle-velocity trade-off. Dos'Santos T., Thomas C., Comfort P., Jones P. A. 2018Sports Med. 48(10):2235–2253. doi: 10.1007/s40279-018-0968-3. doi: 10.1007/s40279-018-0968-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reliability and factorial validity of non-specific and tennis-specific pre-planned agility tests; preliminary analysis. Sekulic D., Uljevic O., Peric M., Spasic M., Kondric M. 2017J Hum Kinet. 55:107–116. doi: 10.1515/hukin-2017-0010. doi: 10.1515/hukin-2017-0010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clinical assessment of hip strength using a hand-held dynamometer is reliable. Thorborg K., Petersen J., Magnusson S. P., Hölmich P. Jun;2010 Scand J Med Sci Sports. 20(3):493–501. doi: 10.1111/j.1600-0838.2009.00958.x. doi: 10.1111/j.1600-0838.2009.00958.x. [DOI] [PubMed] [Google Scholar]
- Validity and inter-rater reliability of medio-lateral knee motion observed during a single-limb mini squat. Ageberg E., Bennell K. L., Hunt M. A., Simic M., Roos E. M., Creaby M. W. 2010BMC Musculoskelet Disord. 11:265. doi: 10.1186/1471-2474-11-265. doi: 10.1186/1471-2474-11-265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Concurrent validity and reliability of clinical evaluation of the single leg squat. Poulsen D.R., James C.R. 2011Physiother Theory Pract. 27(8):586–94. doi: 10.3109/09593985.2011.552539. doi: 10.3109/09593985.2011.552539. [DOI] [PubMed] [Google Scholar]
- Reliability of three measures of ankle dorsiflexion range of motion. Konor M. M., Morton S., Eckerson J. M., Grindstaff T. L. 2012Int J Sports Phys Ther. 7(3):279–287. [PMC free article] [PubMed] [Google Scholar]
- Haff C., Triplett N. Essentials of Strength Training and Conditioning. Human Kinetics; Chicago: [Google Scholar]
- Falls in young, middle-aged and older community dwelling adults: Perceived cause, environmental factors and injury. Talbot L. A., Musiol R. J., Witham E. K., Metter E. J. 2005BMC Public Health. 5(1):86. doi: 10.1186/1471-2458-5-86. doi: 10.1186/1471-2458-5-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Falls and fall-related injuries among community-dwelling adults in the united states. Verma S.K., Willetts J.L., Corns H.L., Marucci-Wellman H.R., Lombardi D.A., Courtney T.K. 2016PLoS One. 11(3):e0150939. doi: 10.1371/journal.pone.0150939. doi: 10.1371/journal.pone.0150939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hip-muscle activation during the lunge, single-leg squat, and step-up-and-over exercises. Boudreau S. N., Dwyer M. K., Mattacola C. G., Lattermann C., Uhl T. L., McKeon J. M. 2009J Sport Rehabil. 18(1):91–103. doi: 10.1123/jsr.18.1.91. doi: 10.1123/jsr.18.1.91. [DOI] [PubMed] [Google Scholar]
- Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. Ekstrom R., Donatelli R., Soderberg G. 2003J Orthop Sport Phys Ther. 33:247–258. doi: 10.2519/jospt.2003.33.5.247. [DOI] [PubMed] [Google Scholar]
- Differences in gluteal and quadriceps muscle activation during weight-bearing exercises between female subjects with and without patellofemoral pain. Glaviano N. R., Saliba S. 2022J Strength Cond Res. 36(1):55–62. doi: 10.1519/JSC.0000000000003392. [DOI] [PubMed] [Google Scholar]
- Myoelectric responses of lower-body muscles performing squat and lunge exercise variations adopting visual feedback with a laser sensor. Paz G. A., Almeida L., Ruiz L.., et al. 2020J Sport Rehabil. 29(8):1159–1165. doi: 10.1123/jsr.2019-0194. doi: 10.1123/jsr.2019-0194. [DOI] [PubMed] [Google Scholar]
- Single leg squat test and its relationship to dynamic knee valgus and injury risk screening. Ugalde V., Brockman C., Bailowitz Z., Pollard C.D. 2015PM & R: Journal of Injury, Function, and Rehabilitation. 7(3):229–235. doi: 10.1016/j.pmrj.2014.08.361. doi: 10.1016/j.pmrj.2014.08.361. [DOI] [PubMed] [Google Scholar]
- Hip and ankle strength and range of motion in female soccer players with dynamic knee valgus. Jo Y. J., Kim Y. K. 2022Isokinet Exerc Sci. 30(1):47–52. doi: 10.3233/IES-200260. doi: 10.3233/IES-200260. [DOI] [Google Scholar]
- Ankle stability and movement coordination impairments: Lateral ankle ligament sprain revision 2021: Clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of orthopaedic physical therapy of the american physical therapy association. Martin R, Davenport T E, Fraser J J., et al. 2021J Orthop Sport Phys Ther. 51(4):CPG1–CPG80. doi: 10.2519/jospt.2021.0302. [DOI] [PubMed] [Google Scholar]
- Muscle power is more important than strength in preventing falls in community-dwelling older adults. Simpkins C., Yang F. Mar 1;2022 J Biomech. 134:111018. doi: 10.1016/j.jbiomech.2022.111018. doi: 10.1016/j.jbiomech.2022.111018. [DOI] [PubMed] [Google Scholar]
- Effects of muscle strength, agility, and fear of falling on risk of falling in older adults. Rodrigues F., Monteiro A. M., Forte P., Morouço P. 2023Int J Environ Res Public Health. doi: 10.3390/ijerph20064945. doi: 10.3390/ijerph20064945. [DOI] [PMC free article] [PubMed]
- Leisure engagement in older age is related to objective and subjective experiences of aging. Bone J. K., Bu F., Sonke J. K., Fancourt D. Feb 19;2024 Nat Commun. 15(1):1499. doi: 10.1038/s41467-024-45877-w. doi: 10.1038/s41467-024-45877-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The relationship between lower limb maximal and explosive strength and change of direction ability: Comparison of basketball and tennis players, and long-distance runners. Kozinc Ž., Smajla D., Šarabon N. 2021PLoS One. 16(8):e0256347. doi: 10.1371/journal.pone.0256347. doi: 10.1371/journal.pone.0256347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agility and change-of-direction speed are two different abilities also during the execution of repeated trials and in fatigued conditions. Ciocca G. T A, Tschan H. 2022PLoS One. 17(6):40. doi: 10.1371/journal.pone.0269810. doi: 10.1371/journal.pone.0269810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Effects of combined plyometric, strength and running technique training program on change-of-direction and countermovement jump: A two-armed parallel study design on young soccer players. Martín-Moya R., Silva A. F., Clemente F. M., González-Fernández F. T. 2023Gait Posture. 105:27–34. doi: 10.1016/j.gaitpost.2023.06.025. doi: 10.1016/j.gaitpost.2023.06.025. [DOI] [PubMed] [Google Scholar]