

Abstract
Background
Unlike other sports, the relationship between performance deficits and pain/injury in lacrosse players has not been well-investigated.
Purpose
The purposes of this study were to: 1) determine whether age and sex differences exist in dynamic physical function tests and drop jump performance among lacrosse players, and 2) determine whether pre-seasonal physical function scores predict onset of either lower extremity or low back pain over time.
Study Design
Prospective observational study.
Methods
Lacrosse players (N=128) were stratified into three groups: 12-14.9 yrs, 15-18 yrs and >18 yrs. Thomas test (hip flexibility), Ober’s test (iliotibial band tightness), and Ely’s test (rectus femoris tightness) were performed. Landing Error Scoring System (LESS) scores were collected while players performed drop jumps. Sagittal and frontal plane movement from 2D video during single and double legged squats was assessed. Musculoskeletal pain symptoms or injury were tracked for six months. Age bracket, sex and physical function scores were entered into logistic regression models to determine risk factors that predicted onset of lower extremity pain and low back pain onset.
Results
LESS scores and single-leg squat movement quality test scores were lowest in the 12-14.9 yr groups and highest in the >18 yr group (all p<0.05). Single leg squat performance score increased the odds risk (OR) for lower extremity pain (OR=2.62 [95% CI 1.06-6.48], p=.038) and LESS scores elevated risk for low back pain onset over six months (OR = 2.09 [95% CI 1.07- 4.06], p= .031).
Conclusions
LESS scores and single legged squat performance may help identify lacrosse players at risk for musculoskeletal pain or injury onset. Detecting these pertinent biomechanical errors and subsequently developing proper training programs could help prevent lower extremity and low back pain onset.
Level of Evidence
III
Keywords: lacrosse, physical function, landing error scoring system, single leg squat
Introduction
According to participation reports compiled by the NCAA, Lacrosse has been one of the fastest-growing American sports of the 21st century.1 From 2000-01 the number of women’s and men’s teams had nearly doubled to 483 teams with a total of 11,375 athletes in 2015-16. Progressively greater numbers of younger players have participated in the sport and high school program growth has paralleled collegiate trends. In 2001, there were 938 schools with boys’ lacrosse teams across 22 states and 783 schools in 21 states for girls’ teams. In the 2021-22 academic year, the sport expanded into four new states for boys and six new states for girls.2
Epidemiological lacrosse studies indicate that acute injuries commonly occur in the sport, but chronic, non-contact musculoskeletal pain and chronic injuries also manifest.3,4 Depending on the nature of the injury, both types can contribute to time loss.4,5 As many as 28%- 40% of reported injuries do not require time away from the sport.6,7 While pain or chronic injury may not keep a player off the field, the presence of chronic pain may interfere with perceived ability to perform effectively, as also has been found among lacrosse officials.8 Overall, the incidence of chronic and acute injury is greater in high school players compared to youth,3 and greater in males compared to females.9 The lower extremity is the primary area where most injuries occur, with emphasis on ankle, knee and hip/thigh.3,6,7,10 Back/trunk pain prevalence ranges from 2.8%-14.2% of youth through collegiate-level players.3,9 Moreover, the incidence of severity of injuries has changed over time. Bano et al.11 found that the rate of severe injuries among players aged 11-18 years has increased by 85.3% from 2000-2016.
For many sports, the overall prevalence of musculoskeletal injury increases around adolescence for both males and females.12 As such, determination of player characteristics and physical functional deficits that contribute to onset of musculoskeletal pain and injury is important for prevention efforts and sport safety over the long-term. Functional performance deficiencies may contribute to the possible onset of lower body musculoskeletal pains and injuries as has been documented in other well-studied sports like soccer, basketball and volleyball.13–15 Deficits or asymmetries in lower extremity strength, flexibility (quadriceps, hamstring, iliotibial band), and dynamic functional tasks reflect movement competence.13 Since lacrosse incorporates fast speeds, sudden direction changes, rotational movements, and jump landings, functional deficits may contribute to aberrant mechanical loading and onset of pain or chronic injury.16,17 Unlike other sports, the relationship between performance deficits and pain onset in lacrosse players has not been well-investigated.
Therefore, the purposes of this study were to: 1) determine whether age and sex differences exist in dynamic physical function tests and drop jump performance among lacrosse players, and 2) determine whether pre-seasonal physical function scores predict onset of either lower extremity or low back pain over time. First, it was hypothesized that younger players (12-14.9 years) and females would score less favorably on dynamic physical function tests than older players > 15 years and males, respectively. Second, it was hypothesized that worse scores during drop jump tests, single legged squats and double legged squats would be related to a higher odds risk of developing and lower extremity and low back pain over six months.
Materials and Methods
This was a prospective observational study of male and female adolescent through collegiate lacrosse players. This study and its procedures were all approved by the University of Florida Institutional Review Board (IRB). Data were merged from two cohort studies of lacrosse players. Prior to participating in the research, all participants ≥18 years provided written consent, and all participants <18 years provided written assent with parental consent. All procedures on human subjects were conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983.
Players were recruited from various clubs and school teams in the North Florida region, using flyers, web advertisements, and word of mouth. Players were stratified into three age groups from adolescence though young adulthood: 12-14.9 years, 15-18 years and >18 years. Age was self-reported. Height and weight were obtained using a medical-grade scale. Body mass index (BMI) was calculated as: BMI = body weight (kg)/ height (m).2 A study-specific survey was developed to determine key information about the lacrosse playing experience of each participant. The survey included questions about years of experience, current weekly frequency of lacrosse practice sessions or games, and the number of seasons played per year. Positions were categorized into offense (midfield, attack) and defense (including goalie).
A series of physical function exam tests, single leg squat and double leg squat motion tests were performed. The functional tests included the Thomas test to identify hip flexibility limitations, Ober’s test for iliotibial band tightness, and Ely’s test for rectus femoris tightness. A digital goniometer (Wixey® angle gage) was used to record flexibility (bilaterally) for each of the following tests.
Thomas’ Hip Flexor Test. To conduct the test, the participant lay supine on a clinical table, with both knees brought to the chest. While keeping the back flat against the table, the participant dropped one leg into extension, followed by the knee dropping into flexion. The test is considered positive for tightness of the one-joint hip flexors if the hip does not extend to 0 degrees.18 The Thomas test’s intraclass coefficient (ICC) is 0.97 (95% confidence interval of 0.91-0.99).19
Ober’s Iliotibial Band Test. Ober’s test estimates the tightness of the iliotibial band.20 The participant was positioned on their side, and the pelvis was fixed in line with the trunk. The knee was flexed to 90 degrees, and the leg was abducted as far as possible. The tester allowed gravity to pull down on the leg. The goniometer captured this angle, with horizontal as 0 degrees. This was considered a positive test if the hip did not fall into adduction upon release. Using inclinometers, previous investigators have found that healthy athletes’ average hip adduction angle is -10.6 ± 9.6 degrees (where positive tests have an adduction angle of -0.3 ± 7.0 degrees).21 The ICC of this test is 0.9012 and inter-tester agreement is high at 97.6%.21
Ely’s Test. Participants lay prone on the clinical table to perform Ely’s test.22 The participant was instructed to keep the hip stationary against the table and pelvis in a neutral position. One knee at a time was actively flexed, and the heel was brought toward the ipsilateral buttock. The knee joint angle was captured at this position. The test was considered positive for quadricep tightness if the anterior hip of the flexed side flexed and pulled away from the table during the knee flexion.22 The ICC for this test ranges from 0.42-0.52 for pass/fail ratings depending on the tester, and 0.914 for goniometer readings at the final knee flexion position.23
Single and Double Legged Squat Tests. The quality of single and double legged squat performance has been used in clinical and sport settings to identify athletes with good and poor movement patterns. Squat performance is related to higher injury rates in incoming collegiate Division 1 athletes.24 All players wore their habitual shoes and received standard instructions for each test. Movements were captured on video from the frontal and sagittal planes for later analysis. For double legged squat, athletes were instructed to place their feet at shoulder width, hold their arms straight out in front of the body, and act as if sitting in a chair. After four to five practice trials, three trials were captured. For the single legged squat, players stood on one foot and, placed hands on their hips, and looked straight ahead. Participants were then instructed to squat to a comfortable maximum depth and return to standing. Four to five practice trials were permitted, and three were captured on video. Bilateral measures were captured. For both tests, one trained investigator, exercise physiologist with 15 years of functional testing experience, (HKV) scored the squat performance from the videos, using published criteria by Eckard et al.24 Double and single legged squats were scored for 10 and 9 operational definitions, respectively. Errors for double legged squats included foot turnout, flat foot, valgus or varus knee, anterior trunk lean, low back arching or rounding, forward arms, heel lift of or weight shift. Single legged errors included flat foot, valgus or varus knee, trunk or hip shifting, balance loss, knee flexion <60 degrees, low back rounding, trunk flexion/rotation/side bend and hip drop/hike. The asymmetry score for the single legged squat was determined from the absolute difference in scores between limbs.
Drop Jump Tests. The Landing Error Scoring System (LESS) scores, developed by Padua et al.25 were obtained from each participant while performing drop jump maneuvers. The LESS is the sum of the landing technique errors that can be visually observed and documented. High-speed video capture (300 fps) jump tests were viewed in sagittal and anterior planes. Participants performed drop jump landing tasks, which included jumping from a 30-cm high box to a distance of 50% of their height away from the box. After standard instructions were provided, familiarization trials (between three and five were typically needed) were performed to ensure the task was done correctly. Trials were repeated if the participant did not: jump off the box with both feet, jump vertically and forward rather than horizontally to reach the target marked on the floor, land outside the target area on the floor, or produce a fluid jump motion.
Prospective Tracking of Musculoskeletal Pain Onset. Pain was collected at baseline, and at months two, four, and six through an initial survey and then with follow-up telephone calls. The operational definition for pain in this study was onset of non-contact musculoskeletal pain or injury in the low back or to the lower extremities that occurred during lacrosse that caused the player to seek medical care. If pain was present, pain severity was captured using the 11-point Numerical Pain Rating scale (NRSpain), with anchors of 0 (no pain) to 10 (worst imaginable pain). The NRSpain scale is a valid, reliable, and responsive outcome measure with established minimum clinically important difference values.26 Pain was rated for the following sites: foot, ankle, leg, knee, thigh, hip and low back. If the participant sought medical attention for the pain and a medical diagnosis was known, this was also recorded.
Statistics: SPSS statistics software version 29.0 (IBM Corp., Armonk, NY, USA) was used for the analyses. Descriptive statistics were obtained to characterize the study groups (means, standard deviations [SD], frequencies). The normality of the data was confirmed before analysis. Ordinal characteristics values and study outcome scores (lacrosse training and experience, other sports played, LESS scores, squat quality ratings) were compared using Kruskal-Wallis tests. Chi-square tests (χ2) were used to determine whether group differences existed for dichotomous variables (positive clinical functional exam tests, pain presence) by age or sex.
Logistic regression was used to determine the risk factors that predicted onset of noncontact lower extremity pain or low back pain. Factors first entered into the model were age bracket and sex, followed by LESS scores, single legged performance scores and double legged squat performance score. As a proxy for model fit, the Nagelkerke R2 are because it is adjusted to achieve a maximum value of 1 and simplifies interpretation.27 A priori alpha levels were established at 0.05 for all statistical tests.
Results
Table 1 displays the characteristics of the study participants across the different age groups (N=128; U12- collegiate). The number of weekly lacrosse sessions and total years playing lacrosse were greater among players 15-18 years and >18 years compared to the youngest group (both p<0.05).
Table 1. Characteristics of lacrosse players of different age brackets. Value are expressed as the number of cases and percent of group, or as means and ± standard deviation (SD).
| Age Bracket (years) | ||||
|---|---|---|---|---|
| 12-14.9 (n=24) | 15-18 (n=53) | >18 (n=51) | p | |
| Age (yr) | 13.8 ± 0.6 | 15.8 ± 0.6 | 21.1 ± 2.7 | <.001 |
| Height (cm) | 165.9 ± 8.9 | 173.5 ± 9.3 | 174.6 ± 9.4 | <.001 |
| Weight (kg) | 56.8 ± 9.2 | 68.1 ± 11.8 | 72.8 ± 11.5 | <.001 |
| Body mass index (kg/m2) | 20.6 ± 2.6 | 22.5 ± 2.8 | 23.8 ± 2.1 | <.001 |
| Female (#, %) | 7 (29.2) | 23 (41.8) | 21 (38.9) | .545 |
| Playing position (#, %) | ||||
| Offense | 19 (79.2) | 39 (73.6) | 44 (86.3) | |
| Defense | 5 (20.8) | 14 (26.4) | 7 (13.7) | .373 |
| Weekly sessions (#) | 2.3 ± 1.4 | 3.7 ± 1.9 | 3.7 ± 2.3 | .008 |
| Years playing lacrosse (#) | 3.4 ± 2.3 | 6.5 ± 2.0 | 10.0 ± 2.8 | <.001 |
| Total sports played in last year (#) | 1.4 ± 1.1 | 1.5 ± 2.0 | 1.3 ± 1.6 | .090 |
Table 2 provides the results of the clinical exam functional tests. None of these clinical test scores (Thomas test, Ober’s test, Ely’s test) differed among the three age groups. When compared by sex, a higher proportion of males had positive Ober’s tests on the left limb than females (χ2 = 4.007; p=0.045).
Table 2. Clinical exam functional test results in lacrosse players by age bracket (2A) and by sex (2B). Value are expressed as the number of cases and percent of group as positive tests.
| Age Bracket (years) | ||||
| 12-14.9 (n=24) | 15-18 (n=53) | >18 (n=51) | p | |
| A. Age Bracket (years) | ||||
| Thomas test (#, % positive); Hip Flexibility | ||||
| Right | 2 (8.3) | 3 (5.7) | 1 (1.9) | .364 |
| Left | 1 (4.2) | 1 (1.8) | 0 (0) | .368 |
| Ober’s Test (% positive); IT Band tightness | ||||
| Right | 0 (0) | 2 (3.7) | 6 (11.7) | .113 |
| Left | 1 (8.3) | 2 (3.7) | 1 (1.9) | .757 |
| Ely’s Test (% positive); Rectus femoris tightness | ||||
| Right | 0 (0) | 2 (3.8) | 0 (0) | .187 |
| 0 (0) | 0 (0) | 1 (1.8) | 1 (1.9) | .781 |
| Male (n=77) | Female (n=51) | |||
| B. Sex | ||||
| Thomas test (#, % positive); Hip Flexibility | ||||
| Right | 4 (7.8) | 4 (2.0) | .696 | |
| Left | 4 (7.8 | 3 (6.0) | .627 | |
| Ober’s Test (% positive); IT Band tightness | ||||
| Right | 9 (11.7) | 2 (8.3) | .224 | |
| Left | 7 (9.0) | 0 (0) | .045 | |
| Ely’s Test (% positive); Rectus femoris tightness | ||||
| Right | 4 (5.2) | 1 (2.0) | .483 | |
| Left | 4 (5.2) | 2 (8.3) | .951 | |
LESS scores by age bracket are presented in Figure 1. LESS scores were lowest in the >18-year group and highest in the 12-14.9 year bracket (p<0.05). When compared by sex, males scored higher than females, but this was not significantly different (4.2 ± 1.8 points versus 3.8 ± 1.9 points, respectively; p=0.361). The quality scores for single and double legged squat movements are provided in Table 3. Right and left single legged squat quality scores in players aged 12-14.9 years were worse than players in the >18-year age group (both p<0.05). When compared by sex, left leg single legged squat and double legged squat quality scores were worse in males than females (both p<0.05).
Figure 1. Landing error scoring system (LESS) values for lacrosse players across different age brackets. Values are means ± SD. * denotes different from the >18 year group at p<0.05.
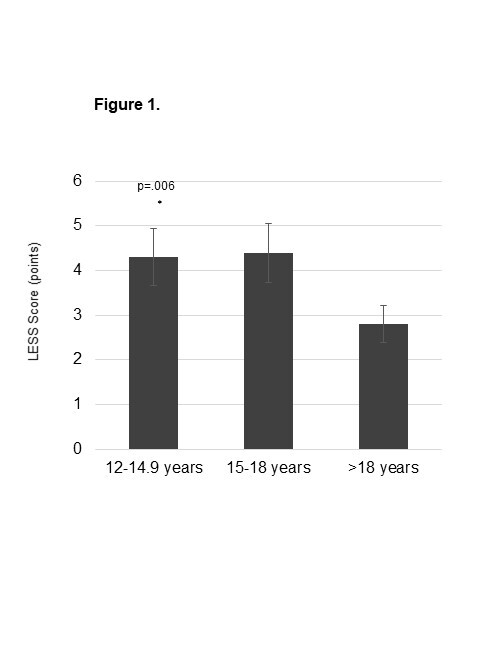
Table 3. Single-leg and double-leg squat movement quality in lacrosse players of different age brackets (3A) and by sex (3B). Values are means ± SD. Higher scores represent a higher number of errors during the task.
| Age Bracket (years) | ||||
| 12-14.9 (n=24) | 15-18 (n=53) | >18 (n=51) | p | |
| A. Age Bracket (years) | ||||
| Single leg squat score (points) | ||||
| Right | 2.2 ± 0.8 * | 2.0 ± 1.1 | 1.7 ± 0.9 | .001 |
| Left | 2.6 ± 1.3 * | 1.9 ± 1.1 | 1.5 ± 0.8 | .016 |
| Interlimb asymmetry (points) | 0.8 ± 0.6 | 0.8 ± 0.7 | 0.5 ± 0.5 | .180 |
| Double leg squat score (points) | 0.9 ± 1.1 | 0.5 ± 0.6 | 0.5 ± 0.6 | .307 |
| Post hoc test: * different than >18 year group | ||||
| Male (n=77) | Female (n=51) | |||
| B. Sex | ||||
| Single leg squat score (points) | ||||
| Right | 2.4 ± 1.2 | 2.0 ± 0.9 | .212 | |
| Left | 2.5 ± 1.2 * | 1.8 ± 1.0 | .006 | |
| Interlimb asymmetry (points) | 0.6 ± 0.6 | 0.7 ± 0.6 | .659 | |
| Double leg squat score (points) | 1.1 ± 0.9 * | 0.5 ± 0.7 | .007 | |
| * different than females by p<.05 | ||||
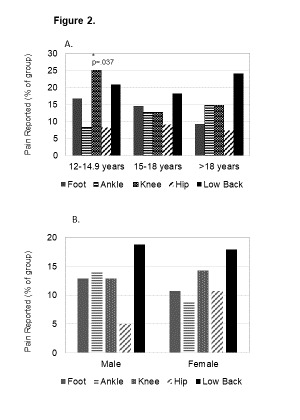
The sites for onset of musculoskeletal pain across player age brackets are reported in Figure 2. Over six months, the two most common sites for pain onset among all players were the knee and low back. The 12-14.9 yr age reported a higher prevalence of knee pain than other age brackets (p<0.05). The pains or reported associated injuries if available were reported. These included metatarsal stress syndrome, patellofemoral pain, Iliotibial band pain, bilateral proximal hamstring pain, Achilles tendon or calf pain, ankle sprain, piriformis syndrome, plantar fasciitis, metatarsal bone and foot pain, quadricep muscle strain, hip impingement syndrome, idiopathic hip pain, sacroiliac joint pain and Sever’s disease flare.
Figure 2. Prevalence of musculoskeletal pain reporting at the low back and lower extremity in lacrosse players over six months. Values are percent of the group.
Logistic regression results are shown in Tables 4A-B. After accounting for age bracket and sex, single legged squat quality scores were associated with an elevated OR for developing lower extremity pain over six months (4A; OR = 2.62 [95% CI =1.06, 6.48], Nagelkerke R2 =0.171; p=0.038). The LESS scores were associated with an elevated OR for low back pain (4B; OR = 2.09 [95% CI 1.07, 4.06], Nagelkerke R2 = 0.261; p= 0.031).
Table 4. Regression models to predict onset of lower extremity musculoskeletal pain and low back pain over 6 months (pre-post season).
| A. Lower extremity pain | ||
|---|---|---|
| Predictor | Odds Ratio [95% CI] | p value |
| Age bracket | ||
| 12-14.9 | reference | |
| 15-18 | 1.39 [0.20-9.67] | .738 |
| >18 | 0.97 [0.13 – 7.48] | .968 |
| Sex | ||
| Male | reference | |
| Female | 0.38 [0.11 – 1.35] | .138 |
| LESS Score (points) | 2.09 [1.07 – 4.06] | .031 |
| Single-leg squat test score (points) | 1.20 [0.45 – 3.18] | .727 |
| Two-leg squat quality score (points) | 0.95 [0.32 – 2.79] | .307 |
| B. Low Back Pain | ||
| Predictor | Odds Ratio [95% CI] | p value |
| Age bracket | ||
| 12-14.9 | reference | |
| 15-18 | 0.21 [0.03 – 1.79] | .153 |
| >18 | 2.37 [0.34 – 16.37] | .283 |
| Sex | ||
| Male | reference | |
| Female | 3.68 [0.72 – 8.91] | .118 |
| LESS Score (points) | 2.09 [1.07 – 4.06] | .031 |
| Single-leg squat test score (points) | 1.20 [0.45 – 3.18] | .727 |
| Two-leg squat quality score (points) | 0.95 [0.32 – 2.79] | .922 |
Discussion
The main findings of this study were that the youngest athletes demonstrated the worst performance scores with single-leg squats, and highest LESS scores of the three age groups. Male players in this sample produced worse scores on both single-leg and two-legged squats than females. Over six months, the risks for onset of lower extremity pain and low back pain were higher in players with worse single-leg squat and LESS scores, respectively. These findings suggest that suboptimal neuromuscular control might be a contributing factor to the onset of lacrosse-related musculoskeletal pain.
Directly comparable functional performance data in lacrosse are scarce. Accumulating evidence in other sports provides context to these findings, however. First, younger athletes (or less developmentally mature) may demonstrate more movement variability than older athletes. Among soccer players of varying ages (U14 to U20), younger players have lower postural stability in single-leg stance tasks and demonstrate more sway of the center of pressure.25 Tuck jump landing scores have been reported to be worse among U11 than U18 soccer players.19 Another study showed that pre-teen (<12 years) athletes of varying sport backgrounds demonstrate more kinematic variability during drop jump tests than more mature athletes (≥12 years).28 Among multisport youth and adolescents, single-leg squat performance scores were worst in the youngest and least physically mature athletes.21 Thus, the current findings are comparable to previous work relating younger age with functional performance deficits. Concerning LESS scores, the youngest players produced the highest error scores compared to the older players, and this corresponded with the highest prevalence of new knee pain in this age group. The LESS scores here align with data from collegiate athletes, including lacrosse players, which range from two to nine errors.22 Strong hip and core musculature are essential for stabilizing the lower extremities, especially in lacrosse, which requires high running volumes, direction changes, and jumping. These hip flexor muscles are essential for controlled running, cutting, and landing biomechanics. Poor hip muscle control, especially in hip abduction, extension, and external rotation, predisposes athletes to knee valgus and potential lower-body musculoskeletal injuries, particularly in the knee.23 Excessive knee valgus in athletes is related to a higher risk for knee ligament injury and chronic injuries like patellofemoral pain syndrome.29
Multiple studies have highlighted the differences in sex in regards to LESS scores as well as single and double-legged squats. Meta-analyses of pooled data of a healthy population illustrated that females have higher LESS scores than males.30 Specifically, during the drop jumps females are more prone to errors at initial contact in trunk flexion, medial knee position, medial knee displacement and total joint displacement.31 In regards to single leg squats, previous studies have shown that female athletes are more disposed to increased adduction and internal rotation at the hips.32 Interestingly, the data from this study did not corroborate this as females were shown to have lower error scores with both single and double legged squats (left leg single squat p=0.006, double leg squat p=0.007). Whether this was due to the limited amount of female athletes included in the study remains unclear.
Performing jump landing tests and specific functional tests in lacrosse players could help identify athletes who may benefit from injury prevention strategies. Educating coaching staff, players, and care teams about safe mechanics of jump landings, strengthening core and hip musculature, and improving dynamic stability has the potential to prevent a variety of lower body injuries and knee ligament injury. Training programs can be implemented to address these biomechanical deficiencies, therefore, potentially decreasing their future risk of injury. USA Lacrosse, with MedStar Health, offers LaxFit, a standardized program that reduces these high-risk injuries, promotes athlete development, and improves performance.33 Multicomponent preventative training programs that include plyometrics, strength, agility, flexibility, and balance can reduce injury rates, even for severe injury like rupture of the anterior cruciate ligament, as much as 75% upon completion of the 15-20 minute program two to three times per week.34 Plyometric drop jump training has improved several performance metrics of on-field performance across youth and adolescent athletes.35 The challenge of this initiative is widespread adoption and implementation of injury prevention programs across geographic areas.
There were limitations identified in this study. Cross-sectional design does not allow for cause and effect of these biomechanical deficiencies on injury onset. Future studies could use prospective data collection and injury surveillance over years of play to determine predictive relationships to the onset of new injury over the course of an athletic career. The physical function metrics are but a small sample of potential neuromuscular tests that can be used to screen athletes prior to the preseason. Future work could consider use of additional field screening tools or motion sensors that could produce better pain and injury prediction models. Dynamic tools may include the Star excursion or Y-Balance tests, time to stabilization after drops or hops, single leg jumps and hops, tuck jumps and asymmetry between limbs on relevant tests – any of which may has potential to improve injury prediction capacity,36 particularly if the athlete holds a cross in their hands. This is an area of strong need to help advance the field of injury predictions in lacrosse similar to that of other sports. The included population consisted of relatively fewer younger female participants, a demographic subgroup in need of additional research. A more robust documentation of previous training exposure/ experience would have provided insight into our measures’ performance differences. Finally, previous concussion history was not considered, which may have affected physical function performance.
Conclusion
The results of this study indicate that jump landing LESS scores, single legged and double legged tests performed in developing lacrosse players show potential for identification of those at risk for future lower extremity and back pain.
Conflicts of Interest
None to declare.
Acknowledgments
Acknowledgments
This project was supported by USA Lacrosse. The authors wish to thank USA Lacrosse for the grant funding for this project. The authors would like to sincerely thank the teams and families who participated in this project. The authors declare that the study procedures complied with the current laws of the United States.
References
- Irick E. Student-athlete participation 198182 - 2015-2016. [2023-7-20]. http://www.ncaapublications.com/productdownloads/PR1516.pdf
- National Federation of State High School Associations Gudiance for opening up high school athletics and activities. [2021-11-8]. https://www.nfhs.org/sports-resource-content/nfhs-sports-medicine-position-statements-and-guidelines/
- Injury incidence in youth, high school, and NCAA men’s lacrosse. Kerr Z. Y., Roos K. G., Lincoln A. E.., et al. 2019Pediatrics. 143(6):e20183482. doi: 10.1542/peds.2018-3482. doi: 10.1542/peds.2018-3482. [DOI] [PubMed] [Google Scholar]
- A comparison of high school boys’ and girls’ lacrosse injuries: academic years 2008-2009 through 2015-2016. Warner K., Savage J., Kuenze C. M., Erkenbeck A., Comstock R. D., Covassin T. 2018J Athl Train. 53(11):1049–1055. doi: 10.4085/1062-6050-312-17. doi: 10.4085/1062-6050-312-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Descriptive epidemiology of collegiate women’s lacrosse injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. Dick R., Lincoln A.E., Agel J., Carter E.A., Marshall S.W., Hinton R.Y. 2007J Athl Train. 42(2):262–269. [PMC free article] [PubMed] [Google Scholar]
- Epidemiology of injuries in National Collegiate Athletic Association women’s lacrosse: 2014-2015 through 2018-2019. Bretzin A. C., D’Alonzo B. A., Chandran A.., et al. 2021J Athl Train. 56(7):750–757. doi: 10.4085/1062-6050-613-20. doi: 10.4085/1062-6050-613-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epidemiology of injuries in National Collegiate Athletic Association men’s lacrosse: 2014-2015 through 2018-2019. D’Alonzo B. A., Bretzin A. C., Chandran A.., et al. 2021J Athl Train. 56(7):758–765. doi: 10.4085/1062-6050-612-20. doi: 10.4085/1062-6050-612-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musculoskeletal pain in lacrosse officials impacts function on the field. Vincent H. K., Bruner M., Obermayer C., Griffin B., Vincent K. R. 2021Res Sports Med Print. 29(5):486–497. doi: 10.1080/15438627.2020.1860046. doi: 10.1080/15438627.2020.1860046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epidemiology of lacrosse injuries in high school-aged girls and boys: a 3-year prospective study. Hinton R. Y., Lincoln A. E., Almquist J. L., Douoguih W. A., Sharma K. M. 2005Am J Sports Med. 33(9):1305–1314. doi: 10.1177/0363546504274148. doi: 10.1177/0363546504274148. [DOI] [PubMed] [Google Scholar]
- The first decade of web-based sports injury surveillance: descriptive epidemiology of injuries in US high school boys’ lacrosse (2008-2009 through 2013-2014) and National Collegiate Athletic Association men’s lacrosse (2004-2005 through 2013-2014) Pierpoint L. A., Lincoln A. E., Walker N.., et al. 2019J Athl Train. 54(1):30–41. doi: 10.4085/1062-6050-200-17. doi: 10.4085/1062-6050-200-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lacrosse-related injuries in boys and girls treated in U.S. emergency departments, 2000-2016. Bano J.M., McAdams R.J., Roberts K.J., Yang J., McKenzie L.B. 2023J Sport Health Sci. 12(3):414–422. doi: 10.1016/j.jshs.2020.08.006. doi: 10.1016/j.jshs.2020.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Use of an inclinometer to measure flexibility of the iliotibial band using the Ober test and the modified Ober test: differences in magnitude and reliability of measurements. Reese N. B., Bandy W. D. 2003J Orthop Sports Phys Ther. 33(6):326–330. doi: 10.2519/jospt.2003.33.6.326. doi: 10.2519/jospt.2003.33.6.326. [DOI] [PubMed] [Google Scholar]
- Musculoskeletal screening and functional testing: considerations for basketball athletes. Bird S.P., Markwick W.J. 2016Int J Sports Phys Ther. 11(5):784–802. [PMC free article] [PubMed] [Google Scholar]
- Preseason functional performance test measures are associated with injury in female college volleyball players. Brumitt J., Mattocks A., Loew J., Lentz P. 2020J Sport Rehabil. 29(3):320–325. doi: 10.1123/jsr.2018-0179. doi: 10.1123/jsr.2018-0179. [DOI] [PubMed] [Google Scholar]
- Hip muscle strength, range of motion, and functional performance in young elite male australian football players. Girdwood M., Mentiplay B. F., Scholes M. J.., et al. 2023J Sport Rehabil. 32(8):910–919. doi: 10.1123/jsr.2022-0450. doi: 10.1123/jsr.2022-0450. [DOI] [PubMed] [Google Scholar]
- Core and back rehabilitation for high-speed rotation sports: Highlight on lacrosse. Vincent H. K., Vincent K. R. 2018Curr Sports Med Rep. 17(6):208–214. doi: 10.1249/JSR.0000000000000493. doi: 10.1249/JSR.0000000000000493. [DOI] [PubMed] [Google Scholar]
- Rehabilitation and prehabilitation for upper extremity in throwing sports: Emphasis on lacrosse. Vincent H.K., Vincent K.R. 2019Curr Sports Med Rep. 18(6):229–238. doi: 10.1249/JSR.0000000000000606. doi: 10.1249/JSR.0000000000000606. [DOI] [PubMed] [Google Scholar]
- Reliability of the modified Thomas test using a lumbo-plevic stabilization. Kim G. M., Ha S. M. 2015J Phys Ther Sci. 27(2):447–449. doi: 10.1589/jpts.27.447. doi: 10.1589/jpts.27.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landing kinematics in elite male youth soccer players of different chronologic ages and stages of maturation. Read P. J., Oliver J. L., De Ste Croix M. B. A., Myer G. D., Lloyd R. S. 2018J Athl Train. 53(4):372–378. doi: 10.4085/1062-6050-493-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reliability of the Ely’s test for assessing rectus femoris muscle flexibility and joint range of motion. Peeler J., Anderson J. E. 2008J Orthop Res. 26(6) doi: 10.1002/jor.20556. doi: 10.1002/jor.20556. [DOI] [PubMed] [Google Scholar]
- Single-leg squat performance in active adolescents aged 8-17 years. Agresta C., Church C., Henley J., Duer T., OʼBrien K. 2017J Strength Cond Res. 31(5):1187–1191. doi: 10.1519/JSC.0000000000001617. doi: 10.1519/JSC.0000000000001617. [DOI] [PubMed] [Google Scholar]
- The relationship between Landing Error Scoring System performance and injury in female collegiate athletes. Lisman P., Wilder J. N., Berenbach J., Jiao E., Hansberger B. 2021Int J Sports Phys Ther. 16(6):1415–1425. doi: 10.26603/001c.29873. doi: 10.26603/001c.29873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hip external rotator strength is associated with better dynamic control of the lower extremity during landing tasks. Malloy P. J., Morgan A. M., Meinerz C. M., Geiser C. F., Kipp K. 2016J Strength Cond Res. 30(1):282–291. doi: 10.1519/JSC.0000000000001069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Association between double-leg squat and single-leg squat performance and injury incidence among incoming NCAA Division I athletes: A prospective cohort study. Eckard T., Padua D., Mauntel T.., et al. 2018Phys Ther Sport. 34:192–200. doi: 10.1016/j.ptsp.2018.10.009. doi: 10.1016/j.ptsp.2018.10.009. [DOI] [PubMed] [Google Scholar]
- Changes in postural control between 13- and 19-year-old soccer players: is there a need for a specific therapy? Bieć E., Giemza C., Kuczyński M. 2015J Phys Ther Sci. 27(8):2555–2557. doi: 10.1589/jpts.27.2555. doi: 10.1589/jpts.27.2555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clinical assessment of low-back-pain treatment outcomes in athletes. Vela L. I., Haladay D. E., Denegar C. 2011J Sport Rehabil. 20(1):74–88. doi: 10.1123/jsr.20.1.74. doi: 10.1123/jsr.20.1.74. [DOI] [PubMed] [Google Scholar]
- Statistics review 14: Logistic regression. Bewick V., Cheek L., Ball J. 2005Crit Care Lond Engl. 9(1):112–118. doi: 10.1186/cc3045. doi: 10.1186/cc3045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Movement variability in pre-teen and teenage athletes performing sports related tasks. Wren T. A. L., O’Callahan B., Katzel M. J.., et al. 2020Gait Posture. 80:228–233. doi: 10.1016/j.gaitpost.2020.06.003. doi: 10.1016/j.gaitpost.2020.06.003. [DOI] [PubMed] [Google Scholar]
- Muscle activity and flexibility in individuals with medial knee displacement during the overhead squat. Bell D.R., Vesci B., Distefano L.J., Guskiewicz K.M., Hirth C., Padua D.A. 2012Athl Train Sports Health Care. 4(3):117–125. doi: 10.3928/19425864-20110817-03. [DOI] [Google Scholar]
- Factors influencing the Landing Error Scoring System: Systematic review with meta-analysis. Hanzlíková I., Athens J., Hébert-Losier K. 2021J Sci Med Sport. 24(3):269–280. doi: 10.1016/j.jsams.2020.08.013. [DOI] [PubMed] [Google Scholar]
- Sex differences on the Landing Error Scoring System among individuals with anterior cruciate ligament reconstruction. Kuenze C. M., Trigsted S., Lisee C., Post E., Bell D. R. 2018J Athl Train. 53(9):837–843. doi: 10.4085/1062-6050-459-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sex-dependent differences in single-leg squat kinematics and their relationship to squat depth in physically active individuals. Zawadka M., Smolka J., Skublewska-Paszkowska M.., et al. 2020Sci Rep. 10(1):19601. doi: 10.1038/s41598-020-76674-2. doi: 10.1038/s41598-020-76674-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- USA Lacrosse LaxFit Program. [2023-9-29]. https://www.usalacrosse.com/laxfit-program
- National Athletic Trainers’ Association Position Statement: Prevention of Anterior Cruciate Ligament Injury. Padua D.A., DiStefano L.J., Hewett T.E.., et al. 2018J Athl Train. 53(1):5–19. doi: 10.4085/1062-6050-99-16. doi: 10.4085/1062-6050-99-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Effects of maturation on physical fitness adaptations to plyometric drop jump training in male youth soccer players. Vera-Assaoka T., Ramirez-Campillo R., Alvarez C.., et al. 2020J Strength Cond Res. 34(10):2760–2768. doi: 10.1519/JSC.0000000000003151. doi: 10.1519/JSC.0000000000003151. [DOI] [PubMed] [Google Scholar]
- A review of field-based assessments of neuromuscular control and their utility in male youth soccer players. Read P.J., Oliver J.L., De Ste Croix M.B.A., Myer G.D., Lloyd R.S. 2019J Strength Cond Res. 33(1):283–299. doi: 10.1519/JSC.0000000000002069. doi: 10.1519/JSC.0000000000002069. [DOI] [PMC free article] [PubMed] [Google Scholar]