

Abstract
Pleomorphic adenoma is a benign tumor that can occur in the salivary glands, most commonly in the parotid gland. While it primarily occurs in the major salivary glands, it can sometimes be found in the minor salivary glands. Within the minor salivary glands, it most often originates in the hard palate and soft palate, and less frequently in the upper lips. Due to its location in the minor salivary glands, most pleomorphic adenoma involve and protrude on the mucosa. A 61-year-old man presented with 1.5 cm exophytic mass on the skin of his upper lip. This mass was exophytic on the skin and did not involve or protrude into the inner lip mucosa. The mass was entirely excised, and a subsequent permanent biopsy diagnosed it as a pleomorphic adenoma. In such situations, it can be challenging to suspect pleomorphic adenoma during a physical examination, leading to potential diagnostic confusion. It might also be mistaken for an inclusion cyst or another type of mass, making it tempting to treat without verifying the pathological results.
Keywords: Case reports, Minor salivary gland, Pleomorphic adenoma, Salivary gland tumor
INTRODUCTION
Pleomorphic adenoma is the most common salivary gland tumor, accounting for approximately 60% of all salivary gland tumors [1]. It is most commonly found in the parotid gland or submandibular gland. However, it can also occur, albeit rarely, in the minor salivary glands. Minor salivary glands are small, dispersed glands located throughout the oral cavity lining. They produce around 10% of the total salivary secretion in the oral cavity per day. These glands are primarily located in the hard and soft palate, but can also be found less frequently in the floor of the mouth, tongue, upper gingival sulcus, upper and lower lip, and upper airway. Consequently, most minor salivary gland tumors originate in the palate, and occurrences on the lip are uncommon [2-4]. We encountered a case of pleomorphic adenoma manifesting in the unusual location of the upper lip. Furthermore, what makes this case particularly unique is that the lesion was solely present as an exophytic skin mass, without mucosal involvement. The presence of an exophytic skin mass without any mucosal involvement can be confounding and presents challenges when considering a broad range of differential diagnoses related to the skin and its appendages.
CASE REPORT
A 61-year-old male patient presented to the clinic with a slowly growing exophytic mass on the upper left lip skin, which had been present for the past 4 years. The well-circumscribed mass measured approximately 1 cm and was firm and rubbery upon palpation. However, it was not visible from the intraoral mucosa (Fig. 1). The movement of the lips was normal. There were no other symptoms, such as pain or discharge. The patient had no history of trauma or dental treatment to the upper lip, and there were no underlying medical conditions or medications being taken. On preoperative computed tomography scan, a 1.3 cm protrusion and exophytic mass on the lip skin was observed involving the subcutaneous tissue on the left upper lip, without orbicularis oris and mucosal involvement (Fig. 2). There were no significant findings in the cervical lymph nodes. The initial impression was an inclusion cyst, which is one of the most common benign tumors that can occur on the skin. We planned mass excision via skin incision and a histological examination.
Fig. 1.
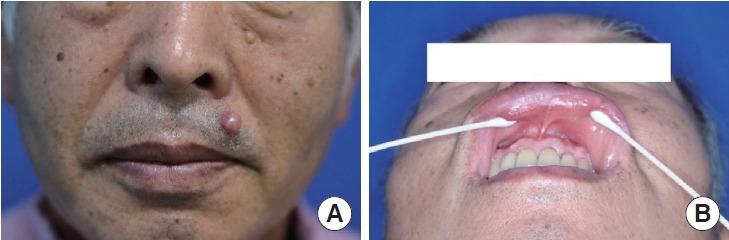
Preoperative photographs. (A) A 61-year-old male patient who presented with a mass on the skin of left upper lip. (B) There was no involvement or protrusion of the inner lip mucosa.
Fig. 2.

Preoperative computed tomography scan.
The surgery was performed through local anesthesia with 2% lidocaine+1:100,000 epinephrine infiltration in the normal skin surrounding the mass. Skin incision parallel to relaxed skin tension line was done and the mass including capsule was gently dissected. The mass was located on the orbicularis oculi muscle, and there was no extension below the muscle. The mass was cleanly excised without muscle injury (Fig. 3). After bleeding control, the subcutaneous tissue was approximated with 5-0 Vicryl and the skin was repaired with 6-0 nylon. A permanent biopsy enabled a diagnosis of pleomorphic adenoma (Fig. 4). The stitches were removed a week later and the wound healed completely without complications. There was no recurrence during 18 months of follow-up (Fig. 5).
Fig. 3.

Intraoperative photographs. (A) Intraoperative photograph. (B) Excised mass.
Fig. 4.

The permanent biopsy. (A) Histopathological cross-sectional examination (hematoxylin and eosin [H&E], ×1). (B) A pleomorphic adenoma containing ductal epithelial cells (red arrows) and myoepithelial cells with chondromyxoid stromal components (black arrows) (H&E, ×10).
Fig. 5.
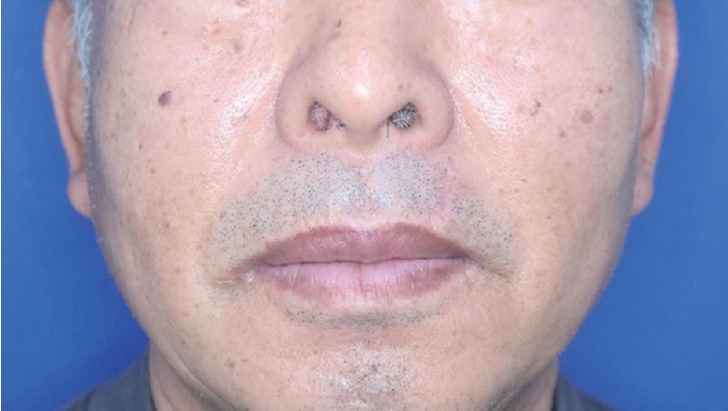
Photograph at 18 months postoperatively.
DISCUSSION
Pleomorphic adenoma is the most prevalent benign tumor found in salivary glands, with the parotid gland (approximately 75%) and submandibular gland (approximately 5%–10%) being the most common sites [5]. Although it is rare for pleomorphic adenoma to occur in minor salivary glands, the hard palate is the most frequent location. The occurrence of pleomorphic adenoma on the lip is even rarer, with previous studies reporting a 6:1 ratio of upper lip to lower lip involvement. This tumor is more prevalent in females, with a female-to-male ratio of 1.9:1, and typically has a peak incidence between the third and fourth decades of life [6]. Pleomorphic adenoma generally appears as an asymptomatic, firm mass that grows slowly over an extended period. However, if it develops secondary to trauma, it may also display clinical symptoms such as ulceration, pain, or bleeding [7]. The etiology of pleomorphic adenoma remains incompletely understood, but cytogenetic and molecular studies suggest an epithelial origin with chromosomal abnormalities at 8q12 and 12q15 [8]. Surgical excision is the preferred treatment for this tumor, and the prognosis is typically favorable [9].
As the name suggests, pleomorphic adenoma exhibits a wide range of histopathological features, consisting of various cellular components and encapsulated growth of ductal and myoepithelial cells, as well as mesenchymal or stromal elements. The myoepithelial cells can display spindle, hyaline, polygonal, or clear morphologies, while the mesenchymal cells may be hyalinized, myxoid/mucoid, or cartilaginous. It is thought that the myoepithelial cells are responsible for producing the myxoid, chondroid, and hyalinized stroma [8].
The minor salivary glands, located on the lips, are distributed throughout the oral mucosa. As a result, pleomorphic adenomas on the lips typically involve the oral mucosa in most cases. However, what is very rare and noteworthy in this case is that the tumor was observed only from the orbicularis oris to the skin of the upper lip without mucosal involvement of the oral mucosa. We thought that this tumor originated from the minor salivary gland within the upper lip and grew outward, presenting an exophytic mass on the upper lip.
The prevalence of pleomorphic adenoma occurring in the upper lip is very low. In a previous review, only 38 cases of pleomorphic adenoma involving the upper lip were reported [10]. Due to this atypical presentation, the initial assumption leaned towards an inclusion cyst, leading to diagnostic confusion. If the specimen had not been submitted for permanent pathology, the condition might have been easily overlooked and misdiagnosed. Additionally, since most pleomorphic adenomas involve the oral mucosa, they can impact dietary habits as they enlarge. Typically, this prompts patients to seek medical attention. However, in our case, the patient did not deem it urgent since there was no involvement of the oral mucosa, which resulted in a delayed diagnosis.
There are various benign tumors that can develop in the skin of the lip without causing any symptoms. These include inclusion cysts, syringomas, clear cell acanthomas, keratoacanthomas, molluscum contagiosum, cylindromas, and tubular adenomas. The malignant tumors that can occur in this area are basal cell carcinoma, squamous cell carcinoma, tubular carcinoma, and adenoid cystic carcinoma [10-12]. The differential diagnosis can be challenging due to the variety of tumors that can develop on the skin. A slow-growing pleomorphic adenoma is prone to long-term neglect and has the potential for recurrence. Furthermore, pleomorphic adenoma can infrequently undergo malignant transformation with rates ranging from 1.9% to 23.3% [13]. Therefore, surgeons should maintain a high level of suspicion, and histological confirmation is essential for an accurate diagnosis and observe whether postoperative occurrence takes place during follow-up.
Footnotes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Ethical approval
The report was approved by the Institutional Review Board of Inha University Hospital (IRB No. 2023-05-008).
Patient consent
The patient provided written informed consent for the publication and use of his images.
Author contributions
Writing - original draft: Jin Myung Yoon, Do Hyuk Chung. Writing - review & editing: Sae Hwi Ki. Resources; Supervision: Sae Hwi Ki. All authors read and approved the final manuscript.
REFERENCES
- 1.Ellis GL, Auclair PL, Gnepp DR. Surgical pathology of the salivary glands. WB Saunders; 1991. [Google Scholar]
- 2.Kim YH, Yoon HW, Kim J, Kim SW. Ectopic pleomorphic adenoma on subcutaneous plane of the cheek. Arch Craniofac Surg. 2019;20:55–7. doi: 10.7181/acfs.2018.01949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Taiwo AO, Akinshipo A, Braimah RO, Ibikunle AA. Pleomorphic adenoma of the upper lip: a case report. Saudi J Med Med Sci. 2018;6:32–5. doi: 10.4103/sjmms.sjmms_109_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Park SY, Han KT, Kim MC, Lim JS. Recurrent pleomorphic adenoma of the parotid gland. Arch Craniofac Surg. 2016;17:90–2. doi: 10.7181/acfs.2016.17.2.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eveson JW, Cawson RA. Salivary gland tumours: a review of 2410 cases with particular reference to histological types, site, age and sex distribution. J Pathol. 1985;146:51–8. doi: 10.1002/path.1711460106. [DOI] [PubMed] [Google Scholar]
- 6.Kataria SP, Tanwar P, Sethi D, Garg M. Pleomorphic adenoma of the upper lip. J Cutan Aesthet Surg. 2011;4:217–9. doi: 10.4103/0974-2077.91260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bentz BG, Hughes CA, Ludemann JP, Maddalozzo J. Masses of the salivary gland region in children. Arch Otolaryngol Head Neck Surg. 2000;126:1435–9. doi: 10.1001/archotol.126.12.1435. [DOI] [PubMed] [Google Scholar]
- 8.Eveson JW, Kusafuka K, Stenman G, Nagao T. In: Pathology and genetics of head and neck tumours. 3rd ed. Barnes L, Eveson JW, Reichart P, Sidransky D, editors. IARC Press; 2005. Pleomorphic adenoma; pp. 254–8. [Google Scholar]
- 9.Sengul I, Sengul D. Pleomorphic adenoma of the lower lip: a review. N Am J Med Sci. 2011;3:536–9. doi: 10.4297/najms.2011.3536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gelidan AG, Arab K. Rare upper lip pleomorphic adenoma presents as cutaneous skin lesion: case report. Int J Surg Case Rep. 2021;85:106142. doi: 10.1016/j.ijscr.2021.106142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Umemori K, Ono K, Kanemoto H, Obata K, Kawai H, Nakamura T, et al. Lip pleomorphic adenomas: case series and literature review. Gland Surg. 2022;11:1730–40. doi: 10.21037/gs-22-308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Suka N, Magoshi S, Ogasawara Y, Takizawa S, Inoue K, Oku Y, et al. Pleomorphic adenoma in the upper lip: a case report and literature review. J Meikai Dent Med. 2021;50:59–65. [Google Scholar]
- 13.Tzermpos F, Chatzichalepli C, Cocos A, Kleftogiannis M, Zarakas M, Chrysomali E. Atypical presentation of an upper lip pleomorphic adenoma: case report. Acta Stomatol Croat. 2014;48:48–53. doi: 10.15644/asc48/1/6. [DOI] [PMC free article] [PubMed] [Google Scholar]