

Abstract
A chemoport is widely used in paediatric oncology population. Removal is a relatively easy procedure, but difficulty can be encountered in case the catheter is densely adherent to the vascular wall. It is a rare complication and is associated with long indwelling duration and acute lymphoblastic leukaemia (ALL). Forceful traction can lead to vascular injury and high morbidity. Herein, we report a 7-year-old girl with precursor B ALL who had delayed chemoport removal due to the coronavirus disease (COVID-19) pandemic. The removal process was difficult, as the catheter was adherent to the right innominate vein. Out of panic, the surgeon pulled it out forcefully. Fortunately, the catheter and its fragment were successfully retrieved completely and the child was discharged the next day. The management strategy varies and ranges from minimally invasive to open surgery. Leaving a stuck chemoport catheter in situ can be a bailout method or part of conservative management.
Keywords: Chemoport, leukaemia, paediatric oncology
INTRODUCTION
A chemoport plays a crucial role amongst the paediatric oncology population for long-term chemotherapy, as it avoids multiple venipuncture procedures. The chemoport should be removed soon after completion of the scheduled treatment, remission of the disease, infection or dysfunction.[1] The removal procedure is relatively simple, but difficulty can be encountered in case the chemoport catheter is densely adherent to the vascular wall, also known as a stuck chemoport catheter. It is a rare complication with an incidence of around 0.4%–4% amongst the paediatric population.[2,3] It may represent an unprecedented challenge to inexperienced surgeons, which can lead to significant morbidity. The long indwelling time is an important risk factor for difficult chemoport removal.[2,4,5] A stuck chemoport catheter may become more evident in the post-COVID-19 era, as plenty of elective surgeries have been commonly postponed during the COVID-19 pandemic[6] which can lead to longer chemoport indwelling time. Herein, we report a case of difficult chemoport removal, which was delayed for 2 years due to the COVID-19 pandemic. In our case, the removal was exceedingly difficult, as the catheter had adhered to the right innominate vein. The perioperative clinical events, associated risk factors and management strategies after a detailed literature review are discussed in the current report.
CASE REPORT
A 7-year-old girl was diagnosed with precursor B acute lymphoblastic leukaemia (ALL) in 2018. A chemoport was inserted through right external jugular vein approach without complication for scheduled chemotherapy [Figure 1a]. She completed her chemotherapy and has been in remission since 2020. She was arranged for chemoport removal but it was delayed for 2 years due to the COVID-19 pandemic. Under general anaesthesia, a skin incision was made over the pocket of the port on the right chest. After adequate dissection around the port and subcutaneous tunnel track, significant resistance was felt upon pulling out the catheter. Another incision was made at the neck to expose the catheter insertion site of the right external jugular vein. There was still difficulty in pulling the catheter out. Subsequently, venotomy on the right external jugular vein was performed, but the catheter was still unable to be removed. The catheter was stuck to the right innominate vein. The surgeon pulled out the catheter forcefully out of panic. After two forceful attempts, the catheter was successfully removed. The distal end of the catheter was enclosed with a fibrin sheath with single fragmentation where it had been adherent [Figure 2]. Fortunately, there were no intraoperative or post-operative complications. A chest x-ray post-operatively showed no residual catheter [Figure 1b]. She made an uneventful recovery and was discharged the next day.
Figure 1.

(a) Chest X-ray post-chemoport insertion. (b) Chest X-ray revealed complete removal of the chemoport
Figure 2.
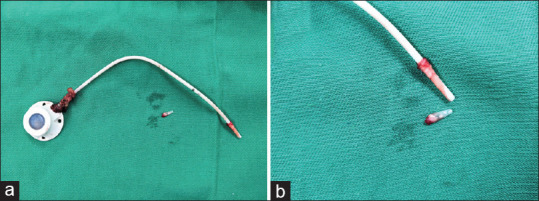
(a) The removed chemoport with fragmentation. (b) Distal end of the catheter was enclosed with a fibrin shealth with single fragmentation
DISCUSSION
The occurrence of stuck chemoport catheter is likely due to fibrin sheath formation and calcification around the catheter.[4] The degree of difficulty during removal has been graded from no difficulty (grade 0), significant traction required (grade 1), venous access incision opened with further dissection and traction (grade 2), venotomy done to mobilise the catheter (grade 3) and part of catheter remained in situ (grade 4).[4]
The common risk factors are ALL and long indwelling time (>20 months).[2,4,5] All the risk factors above were identified in our case as well. The association of ALL and stuck catheter is probably due to the chemotherapy regimen.[3,4,5] The long indwelling duration in our case (about 4 years) is attributed to the COVID-19 pandemic, whereby most elective surgery was delayed to a later date. The chemoport catheter can be stuck to the heart or the major blood vessels.[7] Forceful and aggressive traction during removal can lead to vascular injuries or fragmentation of the catheter, which leads to higher mortality and morbidity.[7] Hence, pulling out the catheter forcefully is extremely dangerous, which we would like to highlight in our case. Fortunately, there was no massive vascular bleeding from the forceful traction, and a single fragmentation of the catheter was successfully retrieved.
Due to its rarity and unpredictable nature, a stuck chemoport catheter will always pose a significant challenge for surgeons. Various management strategies have been described to aid in the removal of grade 3 stuck chemoport catheters. The management of grade 3 stuck chemoport catheters remains controversial and needs to be individualised. It should be started with simple manoeuvres to invasive procedures. After failed venotomy removal of the catheter, the simplest method is to insert a guide wire into the catheter, followed by ‘push in’ force, which helps detach the catheter from the vessel wall.[8] If this fails, a same-size peel-away sheath can be advanced over the stuck catheter into the major vein.[9] The sheath aids in the mechanical detachment of the catheter, but the primary drawback would be that the peel-away sheath may not be readily available.[9] Furthermore, endoluminal balloon dilatation under fluoroscopy[10] or the application of a laser sheath[11] may be helpful. Surgical approaches such as sternotomy, thoracotomy or resection of the clavicle play a role in the removal of a stuck catheter.[3,4,5] These approaches should be as last resort, given their highly invasive and complex nature amongst the paediatric population. Otherwise, as a bailout method, the catheter can safely be left in situ without causing thromboembolism or local infection.[2,4,5,7] If it feels insecure, a few anchoring stitches or clips can be placed.[7] This method gives ample time for referral to a specific speciality centre for further management. Leaving a chemoport in situ could be part of conservative management as well.
CONCLUSION
A stuck chemoport catheter is a rare complication. The management of such complications should be individualised and started with the least invasive manoeuvre. Aggressive forceful traction may result in uncontrolled bleeding, which may lead to high mortality and morbidity. Leaving a stuck chemoport catheter in situ can be a bailout method or part of conservative management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors would like to thank all the staffs involved in the care of this patient.
REFERENCES
- 1.Chuah JS, Wong WL, Bakin S, Lim RZ, Lee EP, Tan JH. Pinch-off syndrome from a chemoport catheter successfully managed with endovascular retrieval. Ann Med Surg (Lond) 2021;65:102294. doi: 10.1016/j.amsu.2021.102294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Patel PA, Parra DA, Bath R, Amaral JG, Temple MJ, John PR, et al. IR approaches to difficult removals of totally implanted venous access port catheters in children: A single-center experience. J Vasc Interv Radiol. 2016;27:876–81. doi: 10.1016/j.jvir.2016.02.021. [DOI] [PubMed] [Google Scholar]
- 3.Maizlin I, Carpentier H, Bliss D. Difficult extraction of long-term central venous catheters in children –Case report. J Pediatr Surg. 2010;45:1720–3. doi: 10.1016/j.jpedsurg.2010.05.026. [DOI] [PubMed] [Google Scholar]
- 4.Wilson GJ, van Noesel MM, Hop WC, van de Ven C. The catheter is stuck: Complications experienced during removal of a totally implantable venous access device. A single-center study in 200 children. J Pediatr Surg. 2006;41:1694–8. doi: 10.1016/j.jpedsurg.2006.05.065. [DOI] [PubMed] [Google Scholar]
- 5.Jung H, Cho JY, Seok Y, Lee Y. Stuck fragment of totally implantable central venous access ports during removal: Risk factor analysis in children. BMC Surg. 2021;21:276. doi: 10.1186/s12893-021-01271-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Qureshi SS, Ramraj D, Chinnaswamy G, Parambil BC, Prasad M, Amin N, et al. Assessment of outcomes of elective cancer surgeries in children during coronavirus disease 2019 pandemic: Retrospective cohort study from a tertiary cancer center in India. Medicine (Baltimore) 2021;100:e26752. doi: 10.1097/MD.0000000000026752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mehra D, Brummund D, Sinyor B, Gulec S. Complicated surgical removal of an adherent port-a-cath after 11 years of implantation. Cureus. 2020;12:e7301. doi: 10.7759/cureus.7301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Huang SC, Tsai MS, Lai HS. A new technique to remove a “stuck” totally implantable venous access catheter. J Pediatr Surg. 2009;44:1465–7. doi: 10.1016/j.jpedsurg.2009.03.033. [DOI] [PubMed] [Google Scholar]
- 9.Katrancioglu N, Serhatlioglu F, Katrancioglu O. An easy way to remove a stuck hemodialysis catheter. Hemodial Int. 2021;25:E18–21. doi: 10.1111/hdi.12896. [DOI] [PubMed] [Google Scholar]
- 10.Hong JH. A breakthrough technique for the removal of a hemodialysis catheter stuck in the central vein: Endoluminal balloon dilatation of the stuck catheter. J Vasc Access. 2011;12:381–4. doi: 10.5301/JVA.2011.8415. [DOI] [PubMed] [Google Scholar]
- 11.Carrillo RG, Garisto JD, Salman L, Merrill D, Asif A. A novel technique for tethered dialysis catheter removal using the laser sheath. Semin Dial. 2009;22:688–91. doi: 10.1111/j.1525-139X.2009.00646.x. [DOI] [PubMed] [Google Scholar]