

Case
Mr. B is a well-educated, nonsmoking, 48-year-old, sedentary businessman with type 2 diabetes mellitus that is well controlled with metformin. He has no renal or other complications of his disease, and his body weight is normal. His lipid profile, however, is abnormal with the low-density lipoprotein (LDL) cholesterol elevated at 4 mmol/L. Although he has no symptoms of coronary artery disease, his diabetes prompted his physician to prescribe an HMG–CoA reductase inhibitor. Mr. B has used the prescription for 2 years and has had a good biochemical response and no side effects. Lately, however, Mr. B has become alarmed by publicity about the risk of serious side effects associated with drugs in the statin class and finds the notion of using natural health products to normalize his blood lipids very appealing. Upon visiting his neighbourhood health food store and surfing the Internet for information on lipid-lowering natural products, he is confronted with a veritable potpourri of herbal and other natural products offered for sale. In addition, on his local grocery shelves, he finds a spread that claims to reduce his LDL cholesterol by up to 15%. Where can Mr. B turn for sound advice, and how can he obtain assurance about the effectiveness of these products?
The nature of the relation between diet and disease is the subject of great controversy. Mixed messages have emerged from the scientific community and from the media concerning the potential benefits of a number of foods and nutrients, including rice bran, vitamins C and E, carotenoids and palm oil, in the treatment and prevention of disease. This confusion, in addition to the wide spectrum of currently marketed products that make questionable health claims, has led health practitioners and consumers to be skeptical and uncertain about the nutritional claims made about new and emerging food products.
There may now be some good news regarding this seeming morass that divides the purported health claims made for foods and the true health benefit realized from their consumption. In many countries including the United States — but not yet in Canada — government regulatory bodies have approved the marketing of foods that carry health claims. These “functional foods” are approved on the basis of scientific evidence. Such products are permitted to carry clear labels describing specific links between a nutrient and disease. However, the level of public awareness of functional foods and their future development remains in question.
Therefore, the first objective of the present review is to provide a definition for functional foods, as well as describe the impetus behind their evolution and identify the stakeholders involved. The second objective is to present specific examples of ongoing and emerging areas of research within the functional foods sector. The third and overarching goal is to consider the future of this sector, examining the positive and negative forces at work that control the scope of the functional foods industry as it enters the 21st century.
What are functional foods?
Functional foods are defined broadly as foods that provide more than simple nutrition; they supply additional physiological benefit to the consumer. Specific definitions are provided in Table 1.1,2 Functional food use reduces risk of disease but is not intended to act as a vehicle for food fortification to address deficiency.1 Similarly, functional foods are not intended for disease treatment or use in palliative care. Definitions arrived at by Health Canada and other agencies require that functional foods contain the bioactive principle mixed within a food. Examples include tomatoes with a high lycopene content or spreads with added plant sterols. These products can be easily incorporated into an individual's everyday diet with little effort. In contrast, nutraceutical products possess bioactive components independent of food matrices, usually in pill, capsular or ampoule form,1 such as capsules containing bioflavonoids or gamma-linoleic acid. In contrast, natural health products are defined as compounds that have been used for a long time and fit into the medicinal foods category. Examples of natural health products include St. John's wort, echinacea and certain herbal teas. Disease treatment is considered possible with natural health products whereas, according to the Health Canada definition, functional foods are used only to reduce the risk of disease.
Table 1

What is motivating the development of functional foods?
The genesis of the functional foods industry has occurred for a number of reasons. First, consumers are aware of the possible positive role diet can play in disease risk management. Despite a lack of consistency in the information that they have recieved, consumers, perhaps because of their advancing average age, are becoming increasingly interested in the relations between food and quality of life. Indeed, a recent poll conducted in the United States found that 95% of the population believed that food possessed the potential to improve health by doing more than just providing nutrients.3 Most of the individuals questioned were also interested in learning more about foods with these functional abilities. Increased education may also be partly responsible, as well as an overall heightening of interest in the general area of preventive health.
Second, regulatory bodies have become increasingly cognizant and supportive of the public health benefits of functional foods. Accordingly, legislative frameworks are now well developed in countries such as Japan that allows more than 200 functional foods to be marketed under existing FOSHU (Foods for Specialized Health Use) legislation4 and the United States where the Food and Drug Administration (FDA) permits health claims to be made for about 15 categories of food.5
Third, governments looking at regulatory issues for functional foods are more aware of the economic potential of these products as part of public health prevention strategies, however, to date the cost savings that might be realized have not been assessed. Processes for the systematic investigation of existing data linking functional foods to physiological mechanisms that affect disease risk have been developed, however, the robustness of the process varies considerably from country to country. The FDA now convenes a group of independent scientists to gather and weigh all the relevant clinical data for each health claim submission. Development of this exhaustive review process has improved the authenticity of health claims, which in itself has led to the birth of the functional food industry.
Examples of functional foods
Many functional foods now exist in various countries. The following examples are provided, because each highlights a particular feature of this growing area. Further information concerning the regulation of functional foods in Canada and the United States can be obtained from the Health Canada (www.hc-sc.gc.ca) and FDA (www .cfsan .fda .gov) Web sites by entering the term “functional food” in the sites' search engines.
Oat bran fibre
Fibre is the endogenous component of plant materials in the diet that is resistant to digestion by enzymes produced by humans. Dietary fibre is classified as soluble or insoluble, and specific agents include cellulose, hemicellulose, pectin and lignin.6 Soluble fibres are found in foods such as beans, oats, guar gum, legumes, pectin, psyllium, barley, prunes and guava.7 Use of the soluble fibre oat bran in cardiovascular risk management was the first health claim allowed under the US Dietary Supplement Health Education Act (DSHEA) during the 1990s.8 The claim, written in very general language, is authorized to appear on packaging and contains information supporting the consumption of about 25 g/day of oat-containing foods to reduce the risk of heart disease, which represents a more sophisticated means of delivering the message that has resonated through the households of North America for many decades, namely, “Eat your porridge — it is good for you” (Fig. 1). The claim was approved based on the extensive number of epidemiological and cohort studies that showed that higher daily intakes of fibre (25–50 g) were associated with a modest but significant reduction in risk for cardiovascular disease by lowering total and LDL cholesterol levels.9 For example, according to the findings of Third National Health and Nutrition Examination Survey the mean intake of dietary fibre in men in the United States is only 17g/day,10 however, higher intakes of dietary fibre have been shown in cohorts of Finnish men to be associated with reduced risk of death from coronary artery disease. Men who reported consuming 27 g of fibre per day had a relative risk of dying from coronary artery disease of 0.83 (95% confidence interval [CI] 0.80–0.86) when compared with men in the same cohort whose average daily consumption of fibre was 10 g lower.11

Fig. 1: Product label showing a health claim for soluble fibre.
Consumption of soluble fibre has now been shown to lower LDL cholesterol levels through a series of processes that alter cholesterol and glucose metabolism. The mechanism of action is thought to involve increasing fecal bile acid excretion and interference with bile acid reabsorption.12 Specifically, this effect of fibre may be attributable to its binding and diluting actions on bile acids and lowering of intestinal pH, which inhibits the conversion of primary bile acids to secondary bile acids, thus resulting in a reduction in the absorption of fat and cholesterol.13 The fermentation of fibre in the colon by intestinal microflora leads to the production of short-chain fatty acids and gases. These short-chain fatty acids not only provide fuel for the cells of the colonic mucosa, their production has also been related to lowered serum cholesterol and decreased risk of cancer.14 Undigested fibre also increases fecal wet weight and dry weight and speeds intestinal transit, which decreases the opportunity for both nutrients and fecal mutagens to interact with the intestinal epithelium.13 Additional details concerning the specific agents in fibre responsible for the effect, its mechanism of action and supportive evidence from animal and human trials are obtainable in the FDA position paper supporting the use of this health claim.15
It is likely that bioactive properties will be discovered for other indigestible polysaccharides and oligosaccharides in the management of cholesterol and glucose metabolism. For instance, glucomannan, a complex indigestible carbohydrate found in the konjac plant, has been shown to improve glycemic control and overall lipid profiles in the treatment of the insulin resistance syndrome. In this study, subjects were randomly assigned to take either konjac mannan fibre–enriched test biscuits (0.5 g of glucomannan per 418.4 kJ [100 kcal] of dietary intake or 8–13 g/day) or wheat bran fibre control biscuits for two 3-week treatment periods. They found that total and LDL cholesterol were reduced by 12.4% and 22.0% respectively with the consumption of konjac mannan fibre compared with the wheat bran fibre. Serum fructosamine, an indicator of glycemic control, was also reduced by 5.2%.16
Soy protein
The health claim that the consumption of soy protein is associated with a reduction in the risk of coronary heart disease is permitted to appear on packaging for soy protein products under the DSHEA. The FDA concluded that soy protein that is included in a diet low in saturated fat and cholesterol may reduce the risk of coronary heart disease by lowering blood cholesterol levels.17 This is thought to be at least in part because of its amino acid profile, which differs from those of animal proteins in ways that result in a desirable lowering of circulating LDL cholesterol.18 A meta-analysis of the effects of soy protein intake on serum lipids revealed that, in most of the studies, the intake of energy, fat, saturated fat and cholesterol was similar when the subjects ingested control and soy-containing diets; soy protein intake averaged 47 g per day. Ingestion of soy protein resulted in an average decrease in total and LDL cholesterol and triglycerides of 9.3%, 12.9% and 10.5% respectively compared with the control group. The hypocholesterolemic effect appears to be directly correlated with the patient's cholesterolemia, with minimal or no reductions occurring at a cholesterol level of 6 mmol/L or less, and the most benefit occurring in patients with a cholesterol level that was greater than 7 mmol/L. The method of action by which soy protein is believed to lower cholesterol concentrations is through activation of the LDL receptor pathway.19
Notably, in addition to yielding health effects mediated through its amino acid content, soy also contains a series of estrogen-like compounds termed isoflavonoids (Fig. 2). Evidence suggests that these isoflavonoids, specifically genistein and daidzein, exist as components of soy protein that possess antioxidant properties and are involved both in the regulation of circulating lipid levels20 and cancer risk.21 Studies with soy devoid of isoflavones indicated a loss of effect of the soy protein supplementation, however, an isoflavone-rich extract by itself was also shown to have no hypocholesterolemic activity, therefore, it may be important to consume a soy protein that contains at least a minimal amount of isoflavones.19 In a randomized controlled trial, it was shown that isolated soy protein containing as little as 37 mg of isoflavones lowered LDL cholesterol by 8%, and there was a dose–response effect of increasing amounts of isoflavones on total and LDL cholesterol levels.22
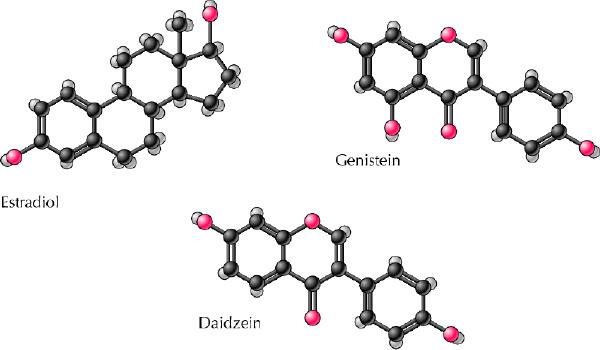
Fig. 2: Structures of dietary isoflavonoids genistein and daidzein compared with estradiol. Photo: Lianne Friesen and Nicholas Woolridge
There is also some suggestion that isoflavones ingested in soy protein undergo biotransformation by intestinal microflora and are absorbed into the circulation where they affect endogenous estrogen levels. These phytoestrogens and their metabolites have several hormonal and nonhormonal activities that may explain some of the biological effects of diets rich in phytoestrogens.23
Mechanisms by which soy isoflavones may inhibit atherosclerotic development independent of lipoprotein effects might include antioxidant effects, antiproliferative and antimigratory effects on smooth muscle cells, effects on thrombus formation and maintenance of normal vascular reactivity.24 It has been speculated that consumption of soy proteins specifically increases circulating levels of genistein, which inhibits the activity of tyrosine kinase, an enzyme associated with plaque development.25 A full description of specific ingredients responsible for the action of soy, its mechanism of action and supporting data from animal and human research can be found in an FDA position document.26 The area of soy foods will undoubtedly be the focus for functional food research activity in the future.
Fish oil fatty acids
Fatty acids found in fish and fish oils have gained interest and publicity for their role in the prevention and management of cardiovascular disease. Another paper in this series by Bruce Holub describes in detail the specific fish oil fatty acids and their use in a variety of clinical trials for the treatment and prevention of atherosclerosis and cardiovascular disease.27 The present paper defines the use of fish oil fatty acids in functional foods that have been shown to be effective in the prevention of several common diseases.
Omega-3 fatty acids, which are found mostly in fish oil, have been recognized for several decades as important in nervous system integrity, particularly during development.27,28 Indeed, fatty acids contained within retinal membrane phospholipids are made up of over 50% omega-3 polyenoic fatty acids, which means that there is a critical demand for these essential fatty acids at certain developmental stages.29 A diet rich in linoleic acid (an omega-6 fatty acid), but low in linolenic acid (an omega-3 fatty acid), was shown to result in episodes of numbness, paresthesia, weakness, inability to walk, pain in the legs and blurred vision in a 6-year-old girl maintained on total parenteral nutrition for 5 months. When linolenic acid was returned to the diet, the child's neurological symptoms disappeared. It was estimated that the requirement for linolenic acid is about 0.54% of energy intake.30
What has only more recently been appreciated is the importance of omega-3 fatty acids in the modulation of risk for a variety of diseases (Table 2).31,32,33,34,35,36,37,38,39 Only within the past few years has the burden of evidence become sufficiently substantial to now claim with reasonable certainty that the intake of omega-3, relative to omega-6 and nonessential, fatty acids can positively reduce the risk of disorders that were until recently not thought linked to fatty acid status. In the United States, health claim status for omega-3 fatty acids with regard to cardiovascular disease has been reviewed, but not at present accepted.40 The FDA concluded that there is not significant scientific agreement for an unqualified claim about the relation between EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) omega-3 fatty acids and reduced risk of coronary heart disease but does permit the use of a qualified claim stating: “The scientific evidence about whether omega-3 fatty acids may reduce the risk of coronary heart disease (CHD) is suggestive, but not conclusive. … It is not known what effect omega-3 fatty acids may or may not have on risk of CHD in the general population.”40 The recommended level of consumption of fish oil fatty acids consistent with health benefits is 2–4 g/day. Omega-3 fatty acids are also available in other foods in addition to fish such as enriched eggs (Fig. 3). Additional research in this area will undoubtedly further clarify and reveal the mechanisms surrounding these diet–disease associations.
Table 2
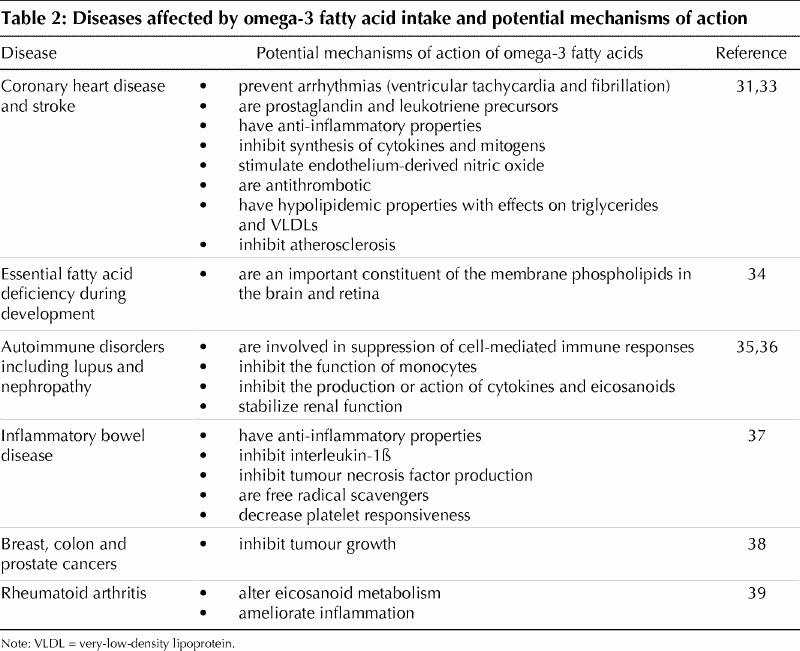
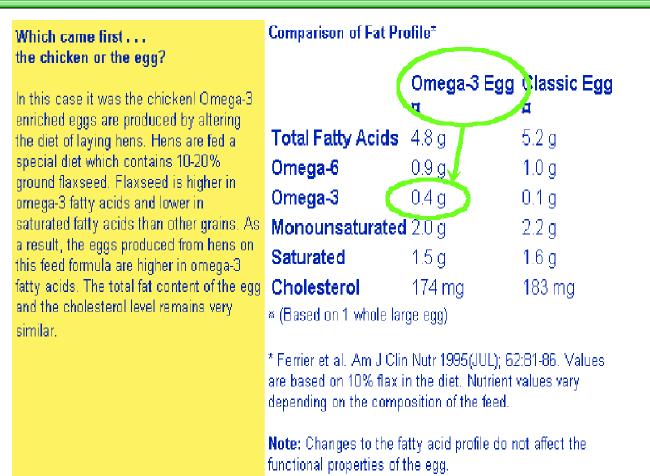
Fig. 3: Product label for omega-3 fatty acid–enriched eggs.
Probiotics and prebiotics
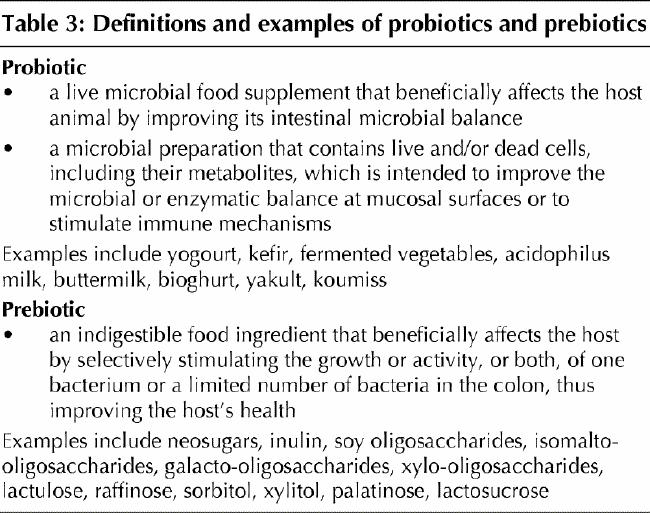
Probiotics are bacteria-containing foods, such as milk and milk solids, yogourt and kefir, that may favourably alter the floral composition of the gut through competition of one type of culture with another. The gastrointestinal tract is inhabited by a multitude of different micro-organisms, the blend of which varies depending on the type of bacteria consumed.41,42,43,44,45 Conversely, prebiotics alter the bacterial composition of the gut, not by adding bacteria, but by changing the type of substrate provided to the existing mixture.41 Specific definitions are provided in Table 3. An area of ongoing and future research regarding probiotics and prebiotics concerns the way in which positive health benefits, including cholesterol level reduction,46 protection from gastrointestinal diseases,42 and improved immunomodulation and resistance to disease,43,47 are achieved.
Table 3
Fermented milk has been shown to cause an increase in human intestinal bacterial content. These bacteria, once resident in the large intestine, are believed to ferment food- derived indigestible carbohydrates. Such fermentation causes increased production of short-chain fatty acids, which decreases circulatory cholesterol concentrations either by inhibiting hepatic cholesterol synthesis or by redistributing cholesterol from plasma to the liver. Furthermore, increased bacterial activity in the large intestine results in enhanced bile acid deconjugation. Deconjugated bile acids are not well absorbed by the mucosa of the gut and are excreted. Consequently, cholesterol, being a precursor of bile acids, is used to a greater extent for de novo bile acid synthesis. It has been suggested that these actions combined are contributing mechanisms to the association of fermented milk consumption with decreased circulating cholesterol concentrations.46
Several strains of bacteria have been studied as probiotics. Lactobacillus and Bifidobacterium, which are commonly found in yogourts, are the most frequently used bacteria to treat gastrointestinal diseases by improving the ability of the gut to prevent invasion by pathogens. The health and immunity of the gut largely depend on the presence of microflora. Probiotic therapy is believed to promote the gut defence barrier by normalization of intestinal permeability and altered gut microecology. Such therapy also strengthens the intestinal immunological barrier, particularly through intestinal immunoglobulin A and inflammatory responses.47 Additional work has also shown that some probiotics may decrease fecal concentrations of enzymes, mutagens and secondary bile salts that are potentially involved in colon carcinogenesis.48
Short-chain fatty acids, such as acetate, propionate and butyrate, produced during gut fermentation may also have promising uses in the treatment of colon cancer. Increased production of short-chain fatty acids has been shown to decrease the pH of the contents of the colon49 and enhance cell proliferation in normal cells, while suppressing proliferation in transformed cells,50 which in turn has been associated with a reduced incidence of colon cancer in various populations. A case–control study of black and white South Africans showed that there was a significant inverse correlation between fecal pH value and total fecal short-chain fatty acid concentration (r = 0.704, p = 0.001). The authors concluded that the high concentrations of fecal short-chain fatty acids in the study group could provide protection against chronic bowel diseases (Fig. 4).49
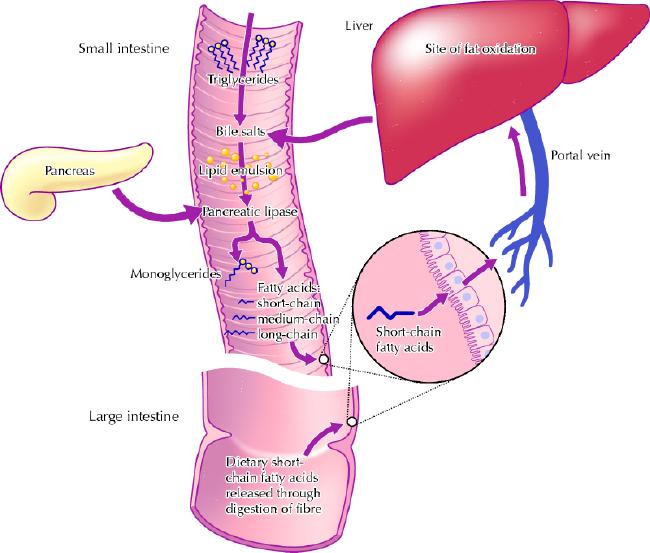
Fig. 4: Relative metabolic pathways of long-chain, medium-chain and short-chain fatty acids. Photo: Lianne Friesen and Nicholas Woolridge
Although traditional thinking has been that the presence of one form of bacteria rather than another in the gut is sufficient to produce such actions, more recent evidence suggests that the secondary products produced by the flora are responsible for the bioactivity that leads to health benefits. These secondary products include short-chain fatty acids, as well as short bioactive peptides resulting from cleavage from milk or other proteins in the gut.42,44,45 This change in thinking will probably stimulate active research in exploring mechanisms that might explain the health benefits of probiotic and prebiotic materials.
Plant sterols and stanols
Plant sterols and stanols, and their esters, represent another functional food that has been the object of increasing interest. These materials are chemically not dissimilar from cholesterol but are not found in any significant abundance in eukaryotic cells (Fig. 5). Plant sterols and their derivatives act in the small bowel by competitively inhibiting intestinal absorption of cholesterol.51,52,53 Data now show sterols and stanols to be equally effective, with or without a fatty acid ester attached to the sterol ring, in their ability to lower LDL cholesterol.54,55 A meta-analysis of 18 clinical trials supporting the efficacy of action of spreads containing plant sterols and stanols suggests that regular consumption of 2 g per day (weight of unesterified sterols and stanols) of these materials, compared with margarine alone, lowers LDL cholesterol concentrations by at least 0.5 mmol/L (95% CI 0.46–0.63) for individuals aged 50–59 years and 0.4 mmol/L (95% CI 0.37–0.47) for individuals aged 40–49 years. At this level of LDL lowering, a reduction in heart disease risk of 25% would be expected in the population.55 Sterols and stanols are presently found in functional foods including spreads and yoghourts in Europe, the United States and Australia and have over the past 2–3 years been approved to bear health claims in those jurisdictions. In Canada, sterol esters have been very recently launched onto the food market despite the absence of health claim legislation and warnings about their use in a bulletin issued by Health Canada.56 Sterols and their derivatives have a unique property compared with other functional foods in that chemical modification of the bioactive principle is carried out rendering the final constituent distinct from the form normally found in foods.
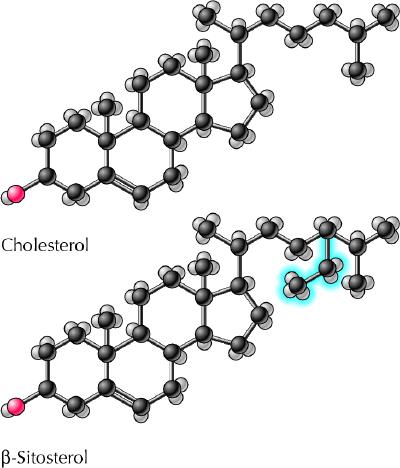
Fig. 5: Structure of plant sterol β-sitosterol compared with cholesterol. Photo: Lianne Friesen and Nicholas Woolridge
Future areas of research regarding plant sterols include possible inverse links between β-sitosterol consumption and cancer risk. Compared with a cholesterol control, β-sitosterol provided to LNCaP cells, a human prostate cancer cell line, retarded cell growth rate by 24%.57 Dietary phytosterols may also exert protective effects on proliferation of colonocyte growth,58 inhibiting the growth of HT-29 cells, a human colon cancer cell line,59,60 compared with control treatments. Moreover, in the treatment of males with benign prostatic hyperplasia, β-sitosterol was shown to improve urological symptoms and flow measures.61,62 Because prostate cancer occurs worldwide and is the second main cause of cancer-related death in men,63 future work will undoubtedly be focused in this area.
Conclusion
The future viability and success of functional foods in the marketplace depend on several elements. The key issue is consumer acceptance of such products. For consumers to agree to pay the premium associated with functional foods, they must be convinced that their health claim messages are clear, truthful and unambiguous. In order for these messages to be such, a more robust working partnership is needed among the 3 key stakeholders in the functional foods dynamic. Industry must avoid the temptation to market food without rigorously validating health claims made on labels. Regulatory agencies must provide a just and efficient regulatory framework within which products bearing authenticated claims can be positioned, with the pace of claim approval occurring at a reasonable speed in order not to overly delay product launches. And the research and academic sector must participate in the process of authenticating and evaluating the science behind individual health claims fairly and impartially.
Global acceptance of functional foods is mixed. On the positive side, several countries have provided legislation permitting health claim use and regulation, although this process has not yet resulted in permission for the use of such claims here in Canada. As of April 2002, health claims on foods continue to be disallowed, despite a consultative process for establishing a regulatory framework that has been ongoing for 5 years. On the less positive side, there are at least 2 telltale harbingers of slower growth for the functional foods industry. First, the marketplace is recording a number of casualties for functional food items and categories. Two major suites of functional food products launched by multinational firms have been discontinued over the past 5 years in various countries. In the United States, sales of the most recently launched major functional food item, plant sterols in spreads and other foods, have been more disappointing than anticipated. However, heightened consumer awareness, the move toward health claims approval and the accumulating food–disease scientific database all predict growth in the functional foods sector in the short-to-medium term.
The case revisited
For an effective, alternative, nonpharmacological approach to the management of his hypercholesterolemia, Mr. B should look for foods labelled with health claims concerning cholesterol management. Such foods include oat-containing cereals, foods rich in soy protein, fish oils, probiotics and spreads containing plant sterols and their derivatives. Through the authenticated health claims found on the labels of these products, Mr. B can be assured that there exists sound validity to the nutrient–disease relation and, thus, that he is consuming an effective and safe product in the management of his cholesterol levels and reduction of his risk of heart disease.
Articles to date in this series .
Hoffer LJ. Clinical nutrition: 1. Protein–energy malnutrition in the inpatient. CMAJ 2001;165(10):1345-9.
Atkinson SA, Ward WE. Clinical nutrition: 2. The role of nutrition in the prevention and treatment of adult osteoporosis. CMAJ 2001;165(11):1511-4.
Young SN. Clinical nutrition: 3. The fuzzy boundary between nutrition and psychopharmacology. CMAJ 2002; 166(2):205-9.
Holub BJ. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. CMAJ 2002;166(5):608-15.
Birmingham CL, Jones PJ. Clinical nutrition: 5. How much should Canadians eat? CMAJ 2002;166(6):767-70.
Jeejeebhoy KN. Clinical nutrition: 6. Management of nutritional problems of patients with Crohn's disease. CMAJ 2002;166(7):913-8.
Footnotes
This series is supported, in part, by an unrestricted educational grant from the Danone Institute of Canada.
This article has been peer reviewed.
Competing interests: Dr. Jones has been a paid consultant to Forbes Medi-Tech (plant sterols) and has received travel assistance from Unilever/Lipton Canada (plant sterols).
Correspondence to: Dr. Peter J. Jones, School of Dietetics and Human Nutrition, Macdonald Campus, McGill University, 21111 Lakeshore Rd., Ste Anne de Bellevue QC H9X 3V9; fax 514 398-7739; jonesp@macdonald.mcgill.ca
References
- 1.Therapeutic Products Programme and the Food Directorate of the Health Protection Branch, Health Canada. Nutraceuticals/functional foods and health claims on foods. 1998. Available: www.hc-sc.gc.ca/hpb-dgps/therapeut/zfiles/english/ffn/nutra_pol_e.html (accessed 2002 May 3).
- 2.Sloan AE. The top ten functional food trends. Food Technol 2000;54(4):33-62. Available: www.ift.org/publications/docshop/ft_shop/04-00/04_00_pdfs/04-00-sloan.pdf (accessed 2002 May 7).
- 3.International Food Information Council Foundation. Background on functional foods. March 2000. Available: http://ific.org/proactive/newsroom/release.vtml?id=18801 (accessed 2002 May 3).
- 4.International Association of Consumer Food Organizations. Japan — the inventor of functional foods. Center for Science in the Public Interest report. 1998. Available: www.cspinet.org/reports/functional_foods/japan_recmnd.html (accessed 2002 May 3).
- 5.Department of Health and Human Services, Food and Drug Administration. Food labelling: use on dietary supplements of health claims based on authoritative statements. 1999 Jan 21. Available: www.cfsan.fda.gov/~lrd/fr990121.html (accessed 2002 May 2).
- 6.LSRO (Life Sciences Research Office). Physiological effects and health consequences of dietary fiber. Bethesda (MD): Federation of American Societies for Experimental Biology; 1987. p. 236.
- 7.Dwyer J. Overview: dietary approaches for reducing cardiovascular disease risks. J Nutr 1995;125:656s-65s. [DOI] [PubMed]
- 8.Brown L, Rosner B, Willett WW, Sacks FM. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr 1999;69:30-42. [DOI] [PubMed]
- 9.Kushi LH, Meyer KA, Jacobs DR Jr. Cereals, legumes, and chronic disease risk reduction: evidence from epidemiologic studies. Am J Clin Nutr 1999;70 : 451S-8S. [DOI] [PubMed]
- 10.Alaimo K, McDowell MA, Briefel RR. Dietary intake of vitamins, minerals, and fiber of persons ages 2 months and over in the United States: the Third National Health and Nutrition Examination Survey, Phase 1, 1988–1991. Adv Data 1994;258:1-26. [PubMed]
- 11.Pietinen P, Rimm EB, Korhonen P, Hartman AM, Willett WC, Albanes D, et al. Intake of dietary fiber and risk of coronary heart disease in a cohort of Finnish men. The Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Circulation 1996;94(11):2720-7. [DOI] [PubMed]
- 12.Marlett JA. Sites and mechanisms for the hypocholesterolemic actions of soluble dietary fiber sources. Adv Exp Med Biol 1997;427:109-21. [DOI] [PubMed]
- 13.McIntyre A, Gibson PR, Young GP. Butyrate production from dietary fibre and protection against large bowel cancer in a rat model. Gut 1993;34:386-91. [DOI] [PMC free article] [PubMed]
- 14.Cummings J, Bingham S, Heaton K, Eastwood M. Fecal weight, colon cancer risk and dietary intake of nonstarch polysaccharide (dietary fiber). Gastroenterology 1992;103:1783-7. [DOI] [PubMed]
- 15.Food and Drug Administration, U.S. Department of Health and Human Services. FDA proposes health claims for oatmeal and oat bran. 1996 Jan 11. Available: www.cfsan.fda.gov/~lrd/tpoatbrn.html (accessed 2002 May 2).
- 16.Vuksan V, Sievenpiper JL, Owen R, Swilley JA, Spadafora P, Jenkins DJ, et al. Beneficial effects of viscous dietary fiber from Konjac-mannan in subjects with the insulin resistance syndrome: results of a controlled metabolic trial. Diabetes Care 2000;23:9-14. [DOI] [PubMed]
- 17.Food labeling: health claims; soy protein and coronary heart disease. Food and Drug Administration, HHS. Final rule. Fed Regist 1999;64:57700-33. [PubMed]
- 18.Costa RL, Summa MA. Soy protein in the management of hyperlipidemia. Ann Pharm 2000;34:931-5. [DOI] [PubMed]
- 19.Sirtori CR, Lovati MR. Soy proteins and cardiovascular disease. Curr Atheroscler Rep 2001;3:47-53. [DOI] [PubMed]
- 20.van der Schouw YT, de Kleijn MJ, Peeters PH, Grobbee DE. Phyto-oestrogens and cardiovascular disease risk. Nutr Metab Cardiovasc Dis 2000;10:154-67. [PubMed]
- 21.Lamartiniere CA. Protection against breast cancer with genistein: a component of soy. Am J Clin Nutr 2000;71:1705S-7S. [DOI] [PubMed]
- 22.Crouse JR III, Morgan T, Terry JG, Ellis J, Vitolins M, Burke GL. A randomized trial comparing the effect of casein with that of soy protein containing varying amounts of isoflavones on plasma concentrations of lipids and lipoproteins. Arch Intern Med 1999;159:2070-6. [DOI] [PubMed]
- 23.Setchell KD. Phytoestrogens: the biochemistry, physiology, and implications for human health of soy isoflavones. Am J Clin Nutr 1998;68:1333S-46S. [DOI] [PubMed]
- 24.Anthony MS, Clarkson TB, Williams JK. Effects of soy isoflavones on atherosclerosis: potential mechanisms. Am J Clin Nutr 1998;68:1390S-3S. [DOI] [PubMed]
- 25.Wilcox JN, Blumenthal BF. Thrombotic mechanisms in atherosclerosis: potential impact of soy proteins. J Nutr 1995;125:631S-38S. [DOI] [PubMed]
- 26.Department of Health and Human Services, Food and Drug Administration. Food labeling: health claims; soy protein and coronary heart disease. 1999 Oct 26. Available: http://vm.cfsan.fda.gov/~lrd/fr991026.html (accessed 2002 May 2).
- 27.Holub BJ. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. CMAJ 2002;166(5):608-15. Available: www.cmaj.ca/cgi/content/full/166/5/608 [PMC free article] [PubMed]
- 28.Uauy R, Peirano P, Hoffman D, Mena P, Birch D, Birch E. Role of essential fatty acids in the function of the developing nervous system. Lipids 1996; 31:S167-76. [DOI] [PubMed]
- 29.Gibson RA, Makrides M. n-3 polyunsaturated fatty acid requirements of term infants. Am J Clin Nutr 2000;71:251S-5S. [DOI] [PubMed]
- 30.Holman RT, Johnson SB, Hatch TF. A case of human linolenic acid deficiency involving neurological abnormalities. Am J Clin Nutr 1982;35:617-23. [DOI] [PubMed]
- 31.Connor WE. Importance of n-3 fatty acids in health and disease. Am J Clin Nutr 2000;71:171S-5S. [DOI] [PubMed]
- 32.Jones PJH, Papamandjaris A. Lipids: cellular metabolism: In: Bowman BA, Russell R, editors. Present knowledge in nutrition. 8th ed. Washington: ILSI Foundation; 2001.
- 33.Connor WE. n-3 Fatty acids and heart disease. In: Kritchevsky D, Carroll KK, editors. Nutrition and disease update: heart disease. Champaign (IL): American Oil Chemists' Society, 1994. p. 7-42.
- 34.Al MDM, van Houwelingen AC, Hornstra G. Long-chain polyunsaturated fatty acids, pregnancy, and pregnancy outcome. Am J Clin Nutr 2000;71: 285S-91S. [DOI] [PubMed]
- 35.Hughes DA, Pinder AC. n-3 Polyunsaturated fatty acids inhibit the antigen-presenting function of human monocytes. Am J Clin Nutr 2000;71:357S-60S. [DOI] [PubMed]
- 36.Donadio JV Jr. Use of fish oil to treat patients with immunoglobulin A nephropathy. Am J Clin Nutr 2000;71:373S-75S. [DOI] [PubMed]
- 37.Belluzzi A, Boschi S, Brignola C, Munarini A, Cariani G, Miglio F. Polyunsaturated fatty acids and inflammatory bowel disease. Am J Clin Nutr 2000; 71:339S-42S. [DOI] [PubMed]
- 38.Sauer LA, Dauchy RT, Blask DE. Mechanism for the antitumor and anticachectic effects of n-3 fatty acids. Cancer Res 2000;60:5289-95. [PubMed]
- 39.Kremer JM. n-3 Fatty acid supplements in rheumatoid arthritis. Am J Clin Nutr 2000;71:349S-51S. [DOI] [PubMed]
- 40.U.S. Food and Drug Administration, Center for Food Safety and Applied Nutrition, Office of Nutritional Products, Labeling, and Dietary Supplements. Letter regarding dietary supplement health claim for omega-3 fatty acids and coronary heart disease. 2000 Oct 31. Available: http://vm.cfsan.fda.gov/~dms/ds-ltr11.html (accessed 2002 May 2).
- 41.Roberfroid MB. Prebiotics and probiotics: Are they functional foods? Am J Clin Nutr 2000;71:1682S-7S. [DOI] [PubMed]
- 42.Marteau PR, de Vrese M, Cellier CJ, Schrezenmeir J. Protection from gastrointestinal diseases with the use of probiotics. Am J Clin Nutr 2001;73: 430S-6S. [DOI] [PubMed]
- 43.Golden BR, Gorbach SL. Probiotics for humans. In: Fuller R, editor. Probiotics. The scientific basis. London: Chapman & Hall; 1992. p. 366.
- 44.Conway PL, Gorbach SL, Golden BR. Survival of lactic acid bacteria in the human stomach and adhesion to intestinal cells. J Dairy Sci 1987;70:1-12. [DOI] [PubMed]
- 45.Robins-Brown RM, Levine M. The fate of ingested lactobacilli in the proximal small intestine. Am J Clin Nutr 1981;34:514-9. [DOI] [PubMed]
- 46.St-Onge M, Farnworth T, Jones PJH. Consumption of fermented and nonfermented dairy products: effects on cholesterol concentrations and metabolism. Am J Clin Nutr 2000;71:674-81. [DOI] [PubMed]
- 47.Isolauri E, Sütas Y, Kankaanpää P, Arvilommi H, Salminen S. Probiotics: effects on immunity. Am J Clin Nutr 2001;73:444S-50S. [DOI] [PubMed]
- 48.Wollowski I, Rechkemmer G, Pool-Zobel BL. Protective role of probiotics and prebiotics in colon cancer. Am J Clin Nutr 2001;73:451S–5S. [DOI] [PubMed]
- 49.Segal I, Hassan H, Walker ARP, Becker P, Braganza J. Fecal short chain fatty acids in South African urban Africans and whites. Dis Colon Rectum 1995; 38:732–4. [DOI] [PubMed]
- 50.Hague A, Elder DJE, Hicks DJ, Pareskeva C. Apoptosis in colorectal tumour cells: induction by the short chain fatty acids butyrate, propionate and acetate and by the bile salt deoxycholate. Int J Cancer 1995;60:400–6. [DOI] [PubMed]
- 51.Miettinen TA, Vuoristo M, Nissinen M, Jarvinen HJ, Gylling H. Serum, biliary, and fecal cholesterol and plant sterols in cholectomized patients before and during consumption of stanol ester margarine. Am J Clin Nutr 2000; 71 (5): 1095-102. [DOI] [PubMed]
- 52.Jones PJ, Raeini-Sarjaz M, Ntanios FV, Vanstone CA, Feng JY, Parsons WE. Modulation of plasma lipid levels and cholesterol kinetics by phytosterol versus phytostanol esters. J Lipid Res 2000;41(5):697-705. [PubMed]
- 53.Ostlund RE, Spilburg CA, Stenson WF. Sitostanol administered in lecithin micelles potently reduces cholesterol absorption in humans. Am J Clin Nutr 1999; 70:826-31. [DOI] [PubMed]
- 54.Jones PJH, Raeini-Sarjaz M. Plant sterols and their derivatives; the current spread of results. Nutr Rev 2001;59:21-4. [DOI] [PubMed]
- 55.Law M. Plant sterol and stanol margarines and health. BMJ 2000;320:861-4. [DOI] [PMC free article] [PubMed]
- 56.Health Canada advises that BecelTM Pro-ActivTM not approved for sale [advisory]. Ottawa: Health Canada; 2001. Available: www.hc-sc.gc.ca/english/protection/warnings/2001/2001_106e.htm (accessed 2002 May 9).
- 57.von Holtz RH, Fink CS, Awad AB. Beta-sitosterol activates the sphingomyelin cycle and induces apoptosis in LNCaP human prostate cancer cells. Nutr Cancer 1998;32(1):8-12. [DOI] [PubMed]
- 58.Awad AB, Hernandez AY, Fink CS, Mendel SL. Effect of dietary phytosterols on cell proliferation and protein kinase C activity in rat colonic mucosa. Nutr Cancer 1997;27(2):210-5. [DOI] [PubMed]
- 59.Awad AB, Chen YC, Fink CS, Hennessey T. β-Sitosterol inhibits HT-29 human colon cancer cell growth and alters membrane lipids. Anticancer Res 1996; 16(5A):2797-804. [PubMed]
- 60.Awad AB, von Holtz RH, Cone JP, Fink CS, Chen YC. β-Sitosterol inhibits the growth of HT-29 human colon cancer cells by activating the sphingomyelin cycle. Anticancer Res 1998;18(1A):471-3. [PubMed]
- 61.Wilt TJ, Macdonald R, Ishani A. β-Sitosterol for treatment of benign prostate hyperplasia: a systematic review. BJU Int 1999;83:976-83. [DOI] [PubMed]
- 62.Berges RR, Windeler J, Trampisch HJ, Senge T. Randomised placebo-controlled, double-blind clinical trial of beta-sitosterol in patients with benign prostatic hyperplasia. Lancet 1995;345(8964):1529-32. [DOI] [PubMed]
- 63.Boring C, Squires T, Montgomery S. Cancer statistics. Cancer J Clin 1994; 44:7-26. [DOI] [PubMed]