

Abstract
Background:
We evaluated how and whether the pedicular morphometry of the C7 and T1 vertebrae might impact C7/T1 spinal fusions for patients from Argentina.
Methods:
Using computed tomography (CT) scans, we evaluated the pedicular morphology at the C7 and T1 levels.
Results:
Among 102 male and female CT studies, we observed significant differences in the height, width, length, and morphometry of the C7 and T1 pedicles.
Conclusion:
This study of C7/T1 CT scans revealed significant sex-based morphometric differences, particularly in pedicle height, width, and length at C7 and T1. Given the notable variability in vertebral characteristics observed in our study sample, we recommend preoperative planning with CT scans for C7/T1 fusion.
Keywords: Argentine population, Cervicothoracic junction, Computed tomography, Pedicle morphometry, Transpedicular screws

INTRODUCTION
Performing C7/T1 fusions is crucial for treating various spinal pathologies. Notably, the C7 and T1 pedicles are relatively small and typically require pedicle screws.[2] In this study, we analyzed the anatomy and morphology of the C7 and T1 pedicles to minimize the risk of neurological and vascular injuries during surgical fusions at these levels.[6,7]
MATERIALS AND METHODS
A retrospective cross-sectional study analyzing the C7/T1 pedicle morphology in adult computed tomography (CT) scans from male and female patients in Argentina between 2021 and 2022 was performed. The variables studied included age, C7–T1 pedicular laterality, pedicle width (PW), pedicle height (PH), pedicle axis length (PAL), and transverse angle [Table 1 and Figures 1-4]. The statistical tests utilized are summarized in Table 2.
Table 1:
Parameters measured on computed tomography images.

Figure 1:
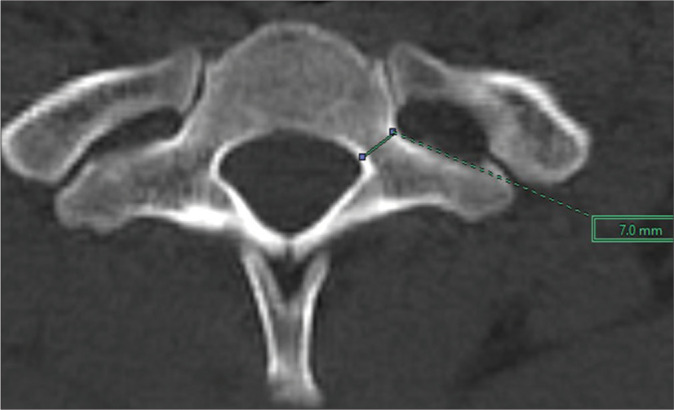
Width of the T1 pedicle in an axial section.
Figure 4:
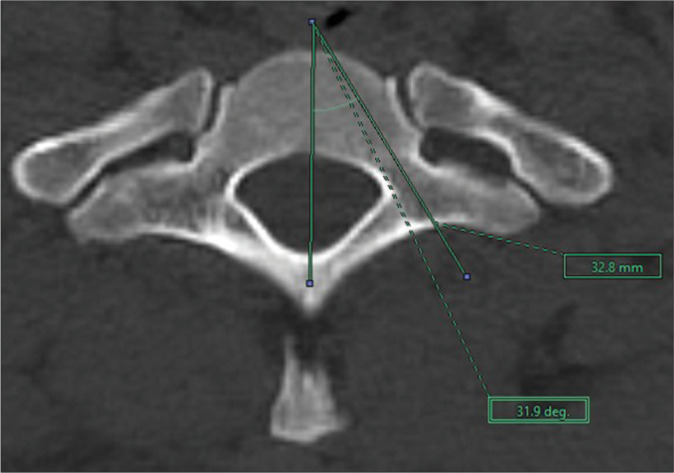
Axial angle of T1 in an axial section.
Table 2:
Descriptive statistics and normality tests for statistical data

Figure 2:
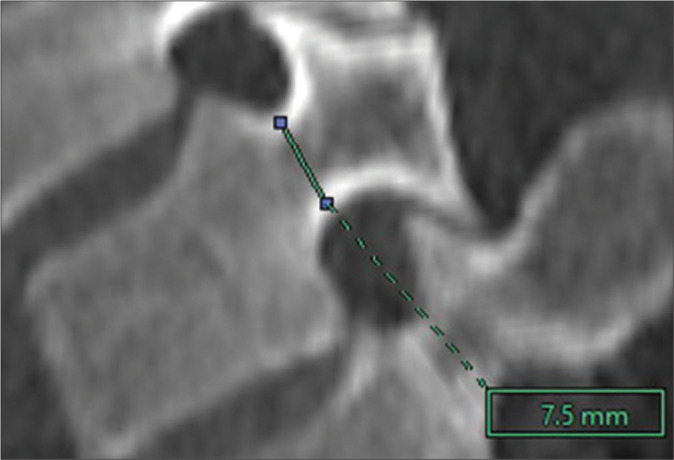
Height of the T1 pedicle in a sagittal section.
Figure 3:
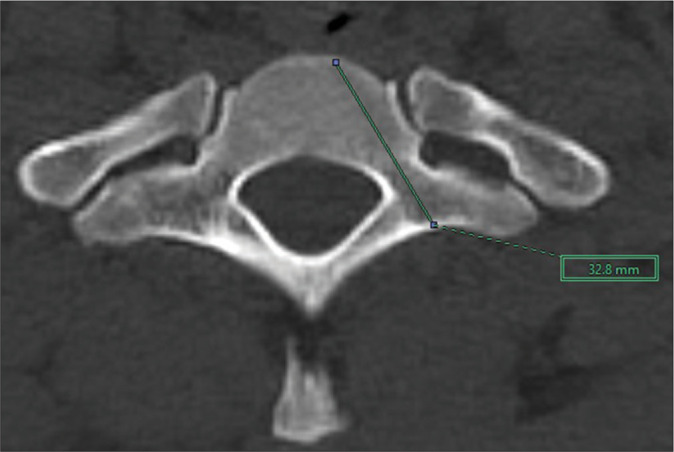
T1 pedicle length in an axial section.
RESULTS
A total of 102 CT scans (60 males and 42 females) were included in this study. Patient ages ranged from 23 to 69 years (mean 52). At both C7 and T1, males had greater PH, PW, and PAL compared to females [Tables 3-5]. At C7, the mean pedicle size for males was 7.5 mm in height, 6.7 mm in width, and 34.2 mm in length. For females, the average pedicle size was 6.7 mm in height, 5.6 mm in width, and 30.4 mm in length. At T1, the mean pedicle measurements for males were 8.5 mm in height, 7.8 mm in width, and 35 mm in length. For females, the measurements were 7.2 mm in height, 6.5 mm in width, and 32 mm in length. For both sexes, age and laterality did not differentially impact C7 or T1 pedicle morphometry [Table 6].
Table 3:
Statistical analysis of the distances analyzed without considering their laterality according to sex.
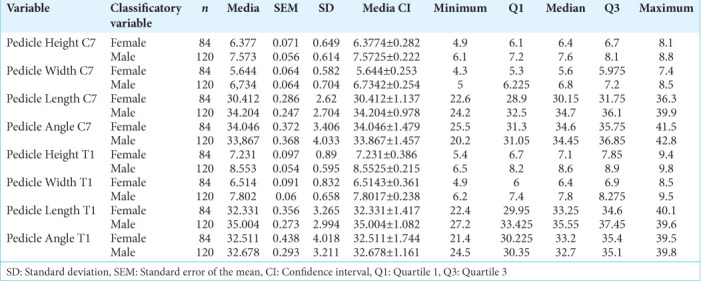
Table 5:
Kruskal-Wallis test results. P-values that are highlighted in red represent comparisons with statistically different means.
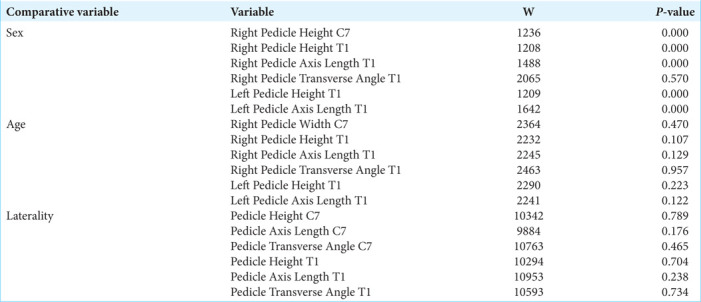
Table 6:
Statistical analysis of the variables studied.
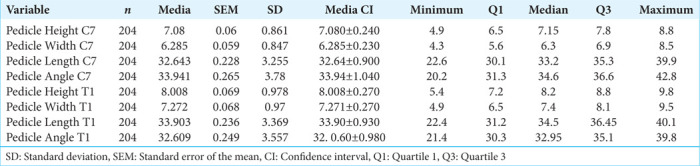
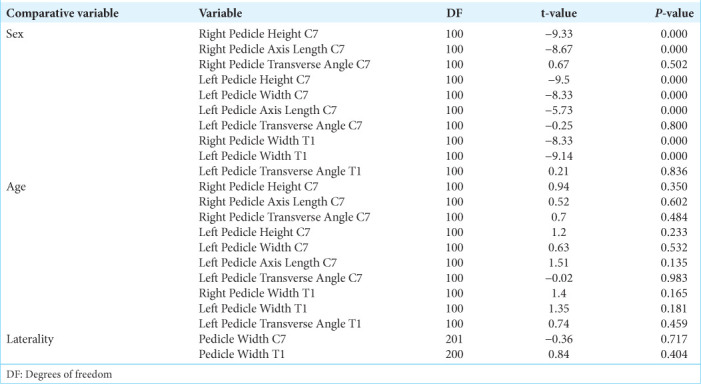
Table 4:
Results of the T-student tests. P-values that are highlighted in red represent comparisons with statistically different means.
DISCUSSION
Many reports have studied the dimensions of C7 and T1 pedicles, which are relatively small and typically require 3.5– 4-mm diameter screws; considering this, larger screws may breach the pedicle wall. Here, we evaluated C7 and T1 PH, PW, and PAL based on 102 CT scans obtained in male and female patients from Argentina.[3,6]
The pedicle dimensions of certain patients in our sample were twice as large as those reported in the previous studies,[3,4,8] suggesting the potential use of larger diameter screws, enhancing construct strength, and significantly decreasing the risk of screw pullout. This finding is crucial as, for fixation involving these vertebrae, it is advisable to measure PH and PW on CT scans and select screws that match these dimensions accurately.
Kotani et al.[5] demonstrated that transpedicular screws might provide greater stability compared to other techniques, especially at the C7/T1 levels. The average axial angle obtained in our study was 33.94° for C7 and 32.60° for T1 [Tables 7 and 8]. The remaining parameters for both C7 and T1 vertebrae were similar to those reported in the previous studies.[1,3,6,9,10] In addition, considerable variation in vertebral characteristics was observed, particularly in angulation and pedicle length [Graphs 1 and 2].
Table 7:
Axial angle of C7 compared with others studies
![]()
Table 8:
Axial angle of T1 compared with others studies
![]()
Graph 1:

Box plots displaying the distribution of the measures under study without classifying variables.
Graph 2:

Histograms showing the distribution of the measurements under study without any classifying variable.
CONCLUSION
This study of C7/T1 CT scans revealed significant sex-based morphometric differences, particularly in PH, PW, and PAL at C7 and T1. Given the notable variability in vertebral characteristics observed in our study sample, we recommend preoperative planning with CT scans for C7/T1 fusion.
Footnotes
How to cite this article: Devoto PR, Minghinelli FE, Mezzadri JJ, Pipolo DO, Lacsi MF, Jalon PG. Pedicle morphometry of the C7 and T1 vertebrae in an argentine population. Surg Neurol Int. 2024;15:295. doi: 10.25259/SNI_356_2024
Contributor Information
Pablo Raul Devoto, Email: pablodevoto7892@gmail.com.
Federico Eduardo Minghinelli, Email: minghinelli.f@gmai.com.
Juan José Mezzadri, Email: jjmezzadri@gmail.com.
Derek Orlando Pipolo, Email: dpipolo@stanford.edu.
Matias Facundo Lacsi, Email: lacsifacundo1994@gmail.com.
Pablo Gustavo Jalon, Email: pablojalon@yahoo.com.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
REFERENCES
- 1.Cho W, Eid AS, Chang UK. The use of pedicle screw-rod system for the posterior fixation in cervico-thoracic junction. J Korean Neurosurg Soc. 2010;48:46–52. doi: 10.3340/jkns.2010.48.1.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Demiroz S, Erdem S. Computed tomography-based morphometric analysis of thoracic pedicles: An analysis of 1512 pedicles and their correlation with sex, age, weight and height. Turk Neurosurg. 2020;30:206–16. doi: 10.5137/1019-5149.JTN.26848-19.2. [DOI] [PubMed] [Google Scholar]
- 3.Faghih-Jouibari M, Moazzeni K, Amini-Navai A, Hanaei S, Abdollahzadeh S, Khanmohammadi R. Anatomical considerations for insertion of pedicular screw in cervicothoracic junction. Iran J Neurol. 2016;15:228–31. [PMC free article] [PubMed] [Google Scholar]
- 4.Herrero CF, Luis Do Nascimento A, Maranho DA, Ferreira-Filho NM, Nogueira CP, Nogueira-Barbosa MH, et al. Cervical pedicle morphometry in a Latin American population. Medicine (United States) 2016;95:e3947. doi: 10.1097/MD.0000000000003947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kotani Y, Cunningham BW, Abumi K, McAfee PC. Biomechanical analysis of cervical stabilization systems. An assessment of transpedicular screw fixation in the cervical spine. Spine. 1994;19:2529–39. doi: 10.1097/00007632-199411001-00007. [DOI] [PubMed] [Google Scholar]
- 6.Lee DH, Lee SW, Kang SJ, Hwang CJ, Kim NH, Bae JY, et al. Optimal entry points and trajectories for cervical pedicle screw placement into subaxial cervical vertebrae. Eur Spine J. 2011;20:905–11. doi: 10.1007/s00586-010-1655-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liau KM, Yusof MI, Abdullah MS, Abdullah S, Yusof AH. Computed tomographic morphometry of thoracic pedicles: Safety margin of transpedicular screw fixation in Malaysian Malay population. Spine. 2006;31:E545–50. doi: 10.1097/01.brs.0000225978.97652.e0. [DOI] [PubMed] [Google Scholar]
- 8.Morita K, Ohashi H, Kawamura D, Tani S, Karagiozov K, Murayama Y. Thoracic and lumbar spine pedicle morphology in Japanese patients. Surg Radiol Anat. 2021;43:833–42. doi: 10.1007/s00276-021-02707-8. [DOI] [PubMed] [Google Scholar]
- 9.Munusamy T, Thien A, Anthony MG, Bakthavachalam R, Dinesh SK. Computed tomographic morphometric analysis of cervical pedicles in a multi-ethnic Asian population and relevance to subaxial cervical pedicle screw fixation. Eur Spine J. 2015;24:120–6. doi: 10.1007/s00586-014-3526-1. [DOI] [PubMed] [Google Scholar]
- 10.Onibokun A, Khoo LT, Bistazzoni S, Chen NF, Sassi M. Anatomical considerations for cervical pedicle screw insertion: The use of multiplanar computerized tomography measurements in 122 consecutive clinical cases. Spine J. 2009;9:729–34. doi: 10.1016/j.spinee.2009.04.021. [DOI] [PubMed] [Google Scholar]