

Abstract
Introduction:
Floating hip and floating knee are high-velocity injuries associated with high mortality and morbidity. The occurrence of both floating hip and floating knee in the same limb is rare and requires proper resuscitation and orthopedic care for the management and for providing a functional limb to the patient.
Case Report:
A 32-year-old male presented with a history of road traffic accident and sustained ipsilateral acetabulum anterior column fracture, sacroiliac joint disruption, double segmental fracture of femur, and segmental fracture of tibia (left side). The patient also sustained head injury and abdominal injuries. The patient underwent a three-staged fixation of the fractures. External fixation of all the fractures was done as an emergency procedure. After the general condition of the patient improved, the acetabular injuries were managed surgically with fixation of the tibia in the same setting. The femur fracture was fixed in the end with a long proximal femur nail. The patient underwent adequate rehabilitation with return to full weight bearing at 4 months. All fractures healed at 6 months. At 18 months, the patient had no limitation of movements and his lower extremity functional score was 73/80 (91.3%).
Conclusion:
Ipsilateral floating hip and floating knee are rare injuries. With early fixation and mobilization, we can ensure fracture union with better functional outcomes.
Keywords: Polytrauma, floating hip, floating knee
Learning Point of the Article:
The key elements in the management of high velocity polytrauma patients with complex fractures are proper staging and good implant choice.
Introduction
Floating hip and floating knee are injuries caused by high-velocity trauma and are commonly seen in younger patients, often due to fall from height or motor vehicle accidents [1]. Either of these occurring individually is not rare, but they rarely occur together. These fractures are usually associated with life-threatening injuries to other systems. Due to the difficulties encountered in reducing these fractures, the complexity of such injuries increases. The paucity of literature on ipsilateral floating hip and floating knee poses a challenge for the treating surgeon as the guidelines are not well established for the management of these patients [2]. We present a rare case of ipsilateral acetabulum fracture, sacroiliac joint disruption, double segmental femoral fracture, and segmental tibia fracture. To the best of our knowledge, only seven case reports of a similar kind have been published and there is no case report published in literature with this combination.
Case Report
A 32-year-old male presented to the emergency room 6 hours after being hit by a lorry while he was driving his car and sustained injuries to his lower abdomen, left hip, left thigh, and left leg. On presentation, the patient was hemodynamically unstable and his Glasgow Coma Scale was 14/15. The patient had diffuse pain in the left hip and the entire left lower limb and was not able to move the limb. The limb was externally rotated and deformed without any open wounds. Perfusion of the limb was also clinically normal. Radiographs (Fig. 1 and 2) revealed a left anterior column fracture of acetabulum, left sacroiliac joint disruption, right comminuted superior pubic rami fracture, double segmental fracture of the left femur, and segmental fracture of the left tibia. In addition to these injuries, he had retroperitoneal hematoma and cerebral edema. Serum lactate and interleukin-6 (IL-6) levels were significantly elevated. The patient was adequately resuscitated in the emergency room and optimization of his general condition was done.
Figure 1.
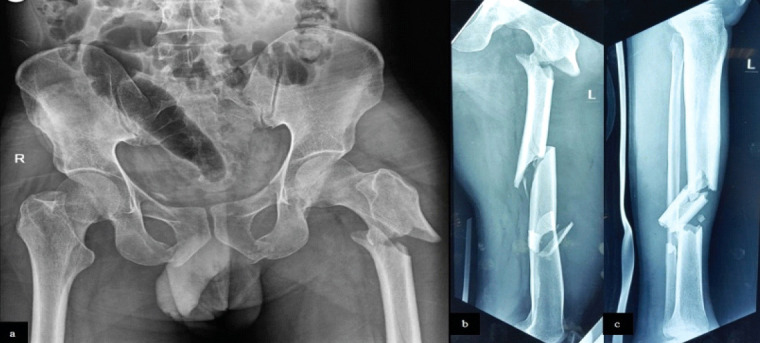
X-rays on presentation (a) pelvis with both hips showing left anterior column fracture of acetabulum, left sacroiliac joint disruption, right comminuted superior pubic rami fracture, (b) left femur double segmental fracture, (c) left tibia segmental fracture.
Figure 2.
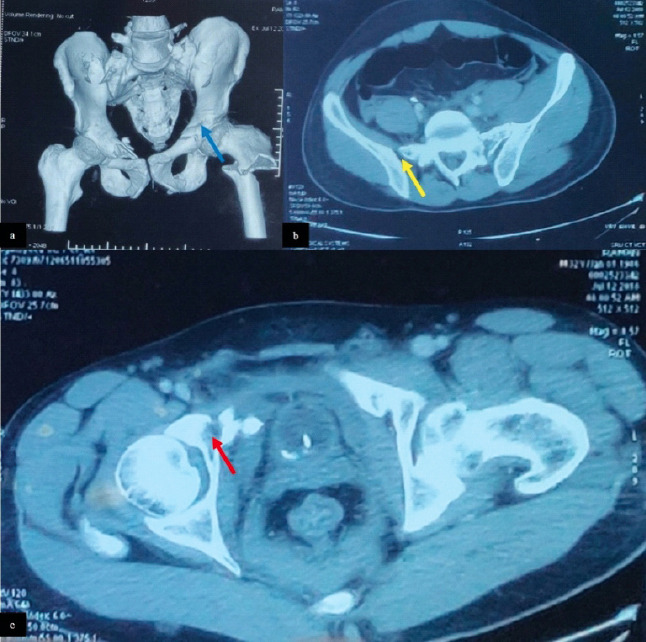
Computed tomography scan of pelvis on presentation, showing left anterior column fracture (a and c) (red arrow and blue arrow), left sacroiliac joint disruption (b) (yellow arrow).
After obtaining fitness from an anesthetist, neurosurgeon, and general surgeon, the patient was taken up for emergency surgery on the same day. Under general anesthesia, the patient in the supine position, external fixation of pelvis, left femur, and left tibia was done (Fig. 3). From the operating room, the patient was shifted to intensive care unit for close monitoring. Specialist opinions were obtained in view of retroperitoneal hematoma and cerebral edema and they were managed conservatively. On post-operative day 4, as the general condition of the patient had improved, he was shifted to ward. Eight days after the external fixator application, the patient was taken up for definitive management of left sacroiliac joint disruption and anterior column fracture, which were fixed percutaneously with cannulated cancellous screws (Fig. 4). In the same setting, left tibia was fixed using an intramedullary interlocking nail, following closed reduction (Fig. 5). Further 4 days later, left double segmental femur fracture was fixed with long proximal femoral nail after fixing the short proximal fragment with 3.5 mm dynamic compression plate (DCP), to counteract the flexion and abduction deformity at that site. Closed reduction at distal fracture sites was achieved using Schanz pins percutaneously (Fig. 6). There were no intraoperative complications.
Figure 3.
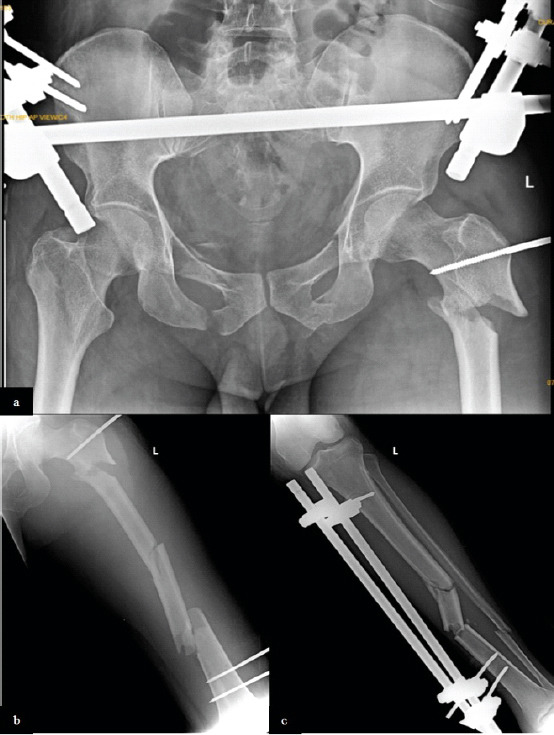
Immediate post-external fixation X-rays, [a] pelvis, [b] femur, and [c] tibia.
Figure 4.
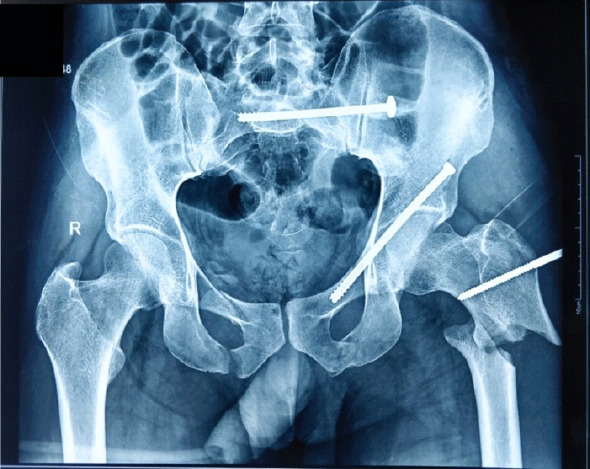
Immediate post-operative X-ray of pelvis.
Figure 5.
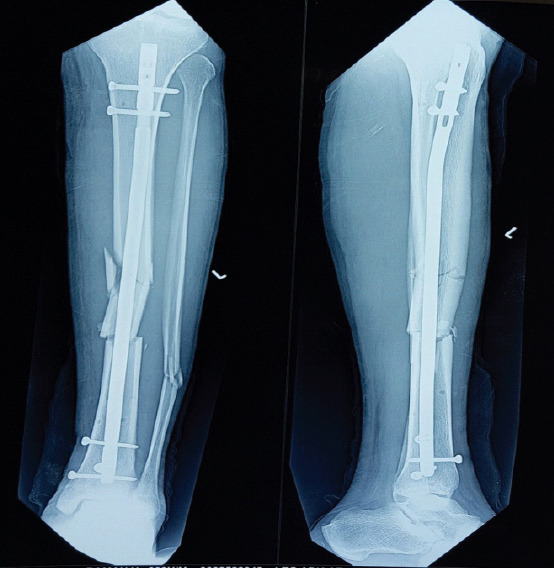
Immediate post-operative X-ray of tibia.
Figure 6.
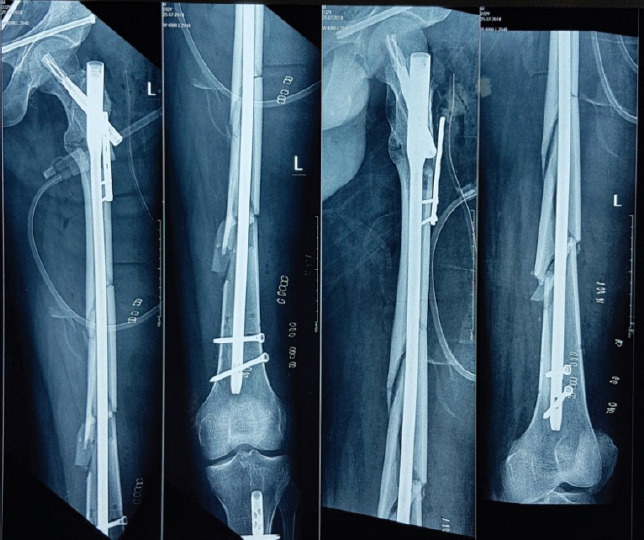
Immediate post-operative X-ray of femur.
Postoperatively, there were no acute complications such as fat embolism or deep vein thrombosis. The patient was started on static exercises of the lower limb and non-weight bearing mobilization for 8 weeks. Partial weight-bearing mobilization was started by 8 weeks and gradually progressed to full weight-bearing by 4 months. All the fractures had healed by 6 months. At the time of last follow-up at 18 months (Fig. 7-9), there was no limitation of hip and knee movements (Fig. 10) and no limb length discrepancy was noted. The patient was functionally evaluated using the lower extremity functionality score and was found to be 73/80 (91.3%). He was able to carry out his activities of daily living without any discomfort. Consent was obtained from the patient for publication of his findings and radiographic images.
Figure 7.

18-month post-operative X-ray of pelvis.
Figure 9.

18-month post-operative X-ray of the left femur.
Figure 10.

Clinical photographs at 18-month follow-up.
Figure 8.

18-month post-operative X-ray of left tibia.
Discussion
While defining musculoskeletal injuries, “Floating” is the term used to refer to bony discontinuity below and above a joint. Floating knee and floating hip injuries are high-velocity injuries, which lead to both the joints being proximally and distally unstable [3].
Liebergall et al., in 1992, introduced the term floating hip for simultaneous fractures in the acetabulum and femur, following their evaluation of 17 patients with such injuries [4]. Most of the literature available on floating hip advocates the surgical fixation of all fractures is the best option, having excellent clinical outcome. However, the sequence of stabilization of these fractures poses the main dilemma for the treating surgeon. While Liebergall et al. suggested toward fixation of femur as the first step, reasoning that it will facilitate the reduction and traction of the acetabulum [4]; Kregor and Templeman advocated for the fixation of acetabular fracture at first [5]. Müller et al., in their case series of 42 cases with floating hip fixed the femur first in 38% of cases [6]. Although there is no consensus on the management of the floating hip, most authors have agreed that the early stabilization of the unstable pelvic injuries is a measure of adequate resuscitation as per the principles of damage control orthopedics [7, 8]. The surgical order, as per our belief, has to be discussed on a case-to-case basis.
Blake and McBride, in 1965, described floating knee injury from their review of 51 patients with fractures of ipsilateral tibia and fibula [9]. Floating knee injuries, being almost always caused by high-velocity trauma, are often associated with other life-threatening injuries. In their report, Ríos et al., observed that 42% of the patients presenting with floating knee had head injuries, 16% had abdominal injuries, and 28% had chest trauma [10]. Moreover, the mortality rate associated with such injuries has been reported to be in the range of 5–10% [11]. Intramedullary nailing of the femur and tibia has been recommended by several authors, reasoning that it allows for prompt mobilization, permits early weight bearing, and may prevent knee stiffness [8, 10, 11].
This case was managed by a three-staged procedure. As the patient was hemodynamically unstable and serum lactate and IL-6 levels were significantly elevated on presentation, the principle of damage control orthopedics was followed. Hence, external fixation of pelvis, femur, and tibia was done as the first procedure. Femur was stabilized using one Schanz pin proximally and two Schanz pins distally and the length was maintained. No Schanz pins were used in the intermediate floating segments to minimize the number of overall pins, thereby decreasing the chances of subsequent pin tract infections. After the hemodynamic status improved and serum lactate and IL-6 levels decreased, we went on to fix the acetabulum, sacroiliac joint, and tibia as the second procedure. Since the pelvic fractures were not displaced much, they were fixed percutaneously using cannulated cancellous screws. Tibia was fixed before femur because it provides an increased lever arm and also facilitates the usage of the fracture table while operating the femur, as was done in our case. While undergoing fixation of the femur, closed reduction was attempted but it failed because the short proximal fragment was flexed. Hence, the proximal most fracture site was opened first and it was reduced using reduction forceps, but the reduction was found to be inadequate. Hence, the short proximal fragment was reduced and fixed using 3.5-mm DCP and unicortical screws, so that the screws do not interfere with the nail entry.
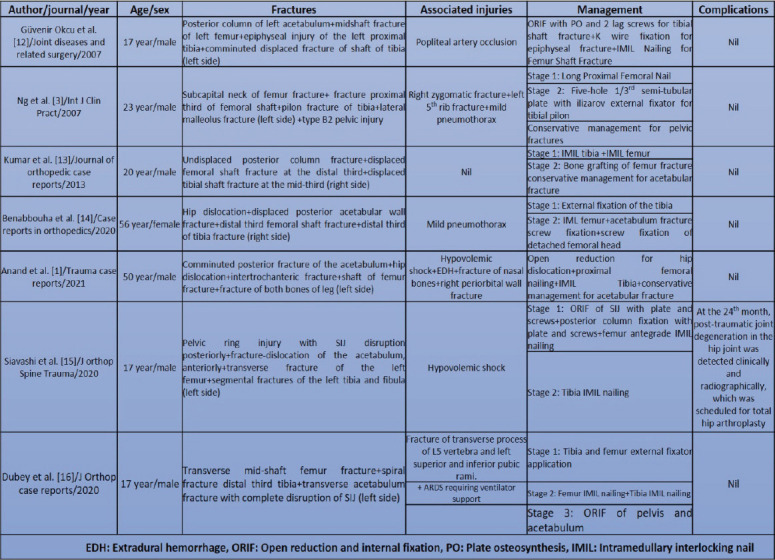
To the best of our knowledge, only seven cases of ipsilateral floating hip and knee have been published so far [1,3,12-16]. Various case reports on ipsilateral floating hip and knee have been tabulated in Table 1.
Table 1.
Various case reports on ipsilateral floating hip and knee injuries.
Conclusion
Ipsilateral floating hip and floating knee are very rare injuries, seen after high-velocity trauma. As very few cases have been reported in the literature, there are no standard guidelines for the treatment of such injuries. The orthopedic management should be performed after the stabilization and resuscitation of the patient. Pelvic and acetabular fractures should be managed by percutaneous fixation whenever possible as it provides a better outcome because of less morbidity. In the case of double segmental femoral fracture, the proximal-most fracture tends to be flexed, which should be reduced adequately to get a correct entry point. Our preferred order of fixing an ipsilateral floating hip and floating knee injury will be to fix the pelvic and acetabular fractures first, followed by fixation of the tibia and then of the femur, either in a single sitting or as a staged procedure. With early fixation and mobilization, we can ensure fracture union with better outcomes.
Clinical Message.
Although ipsilateral floating hip and knee fractures are rare, the management depends on the general condition of the patient, comorbid status, and the pattern of the fractures. The key to survival of a polytrauma patient with multiple fractures is the optimum golden hour treatment and measures to prevent fat embolism and pulmonary embolism. This may include early temporary stabilization of fractures and strict monitoring of biochemical and hemodynamic indicators. The surgical expertise of the trauma team should guide the definitive treatment and its sequence.
Biography



Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that informed consent was obtained from the patient for publication of this case report
References
- 1.Anand V, Deviprasad, Praba K, Babar S, Babu M. Ipsilateral floating hip and knee, or floating lower limb - a rare case report. Trauma Case Rep. 2021;31:100390. doi: 10.1016/j.tcr.2020.100390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brainard BJ, Slauterbeck J, Benjamin JB. Fracture patterns and mechanisms in pedestrian motor-vehicle trauma:The ipsilateral dyad. J Orthop Trauma. 1992;6:279–82. doi: 10.1097/00005131-199209000-00002. [DOI] [PubMed] [Google Scholar]
- 3.Ng AB, Soong VK, Maguire MP, Hopgood P, Shepard GJ. Concomitant ipsilateral floating hip and floating knee injuries:A unique injury and review of the literature. Int J Clin Pract. 2007;61:1585–7. doi: 10.1111/j.1742-1241.2006.00868.x. [DOI] [PubMed] [Google Scholar]
- 4.Liebergall M, Mosheiff R, Safran O, Peyser A, Segal D. The floating hip injury:Patterns of injury. Injury. 2002;33:717–22. doi: 10.1016/s0020-1383(01)00204-2. [DOI] [PubMed] [Google Scholar]
- 5.Kregor PJ, Templeman D. Associated injuries complicating the management of acetabular fractures:Review and case studies. Orthop Clin N Am. 2002;33:73–95. doi: 10.1016/s0030-5898(03)00073-7. [DOI] [PubMed] [Google Scholar]
- 6.Müller EJ, Siebenrock K, Ekkernkamp A, Ganz R, Muhr G. Ipsilateral fractures of the pelvis and the femur- floating hip?A retrospective analysis of 42 cases. Arch Orthop Trauma Surg. 1999;119:179–82. doi: 10.1007/s004020050385. [DOI] [PubMed] [Google Scholar]
- 7.Sen RK, Jha L. Floating hip. J Clin Orthop. 2017;2:43–8. [Google Scholar]
- 8.Mohamed SO, Ju W, Qin Y, Qi B. The term floating used in traumatic orthopedics. Medicine. 2019;98:e14497. doi: 10.1097/MD.0000000000014497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Blake R, McBryde A., Jr The floating knee:Ipsilateral fractures of the tibia and femur. South Med J. 1995;68:13–6. [PubMed] [Google Scholar]
- 10.Ríos JA, Ho-Fung V, Ramírez N, Hernández RA. Floating knee injuries treated with single-incision technique versus traditional antegrade femur fixation:A comparative study. Am J Orthop. 2004;33:468–72. [PubMed] [Google Scholar]
- 11.Oh CW, Oh JK, Min WK, Jeon IH, Kyung HS, Ahn HS, et al. Management of ipsilateral femoral and tibial fractures. Int Orthop. 2005;29:245–50. doi: 10.1007/s00264-005-0661-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Güvenir Okcu MD, Hüseyin S, Yercan MD. A case of ipsilateral floating hip and knee with concomitant arterial injury. Joint Dis Rel Surg. 2007;18:134–8. [Google Scholar]
- 13.Kumar Y, Nalini KB, Nagaraj P, Jawali A. Ipsilateral floating hip and floating knee, a rare entity. J Orthop Case Rep. 2013;3:3–6. doi: 10.13107/jocr.2250-0685.105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Benabbouha A, Boussouga M, Fjouji S, Lamkhanter A, Jaafar A. Simultaneous Ipsilateral floating hip and knee:A complex combination and difficult surgical challenge. Case Rep Orthop. 2020;2020:9197872. doi: 10.1155/2020/9197872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Siavashi B, Shafiei SH, Mahdavi F, Baghbani S, Golbakhsh MR. A case report of simultaneous ipsilateral floating knee and hip. J Orthop Spine Trauma. 2021;6:72–4. [Google Scholar]
- 16.Dubey S, Azam Q, Sarkar B, Agrahari H. A rare case of ipsilateral ”floating ileum“with floating hip and floating knee. J Orthop Case Rep. 2020;10:33–6. doi: 10.13107/jocr.2020.v10.i08.1848. [DOI] [PMC free article] [PubMed] [Google Scholar]